
Abstract
Background: Early childhood education (ECE) working environments often contribute to poor health outcomes. The purpose of this study was to describe healthy eating–related and physical activity–related awareness and adoption of behavior change of ECE providers after participating in a workplace wellness (WW) program and to explore facilitators and barriers to ECE provider participation in WW program. Methods: The WW program offered healthy eating and physical activity challenges to promote ECE provider health and well-being. Approximately 1,000 ECE providers in Colorado from 35 ECE settings were invited to participate. After the intervention, ECE providers completed two surveys: (a) a provider postsurvey and (b) a WW challenge survey. Multivariable logistic regression modeling was used to examine factors associated with percent agreement that participation in the WW program increased awareness and adoption of health behaviors. Findings: A total of 250 (25%) ECE providers participated in WW program from 2015 to 2017. After participation, approximately 84% of respondents agreed they were more aware of the importance of eating fruits and vegetables and of being physically active, while 81% reported eating more fruits and vegetables, and 80% reported being more physically active in the workplace. Logistic regression models found that the length of time teaching in ECE settings was positively and significantly associated (odds ratio [OR] = 1.10, 95% confidence interval [CI] = [1.00, 1.21]) with the odds of providers agreeing that participation in the WW program increased their awareness of health behaviors. Conclusion/Application to Practice: The design and implementation of WW programs that emphasize facilitators, such as intrinsic and extrinsic motivation, as well as reduce barriers, such as time constraints and unachievable goal setting, may increase the awareness and adoptions of healthy eating–related and physical activity–related behaviors among ECE work settings.
Introduction
Early childhood education (ECE) providers play an important role in the well-being of the children they serve. With over a million providers nationwide, they are a large sector of the U.S. workforce (Bureau of Labor Statistics, 2016). This workforce faces unique job-related challenges that contribute to overall physical and mental health. Recent research shows associations between ECE providers’ well-being and the quality of the learning environment they create for their students (Jennings, 2015). Despite the importance of the health and well-being of those responsible for providing safe, stable, and nurturing environments for young children, there exists a lack of resources and working environments often lead to significant physical and mental health disparities (Linnan et al., 2017).
A review of literature found that challenging work conditions in ECE centers, such as long hours, low job control, and high job demands, are related to a higher risk for injuries and other occupational hazards, as well as adverse effects on workers’ psychological, emotional, and physical health (Bloechliger & Bauer, 2016; Cumming, 2017; Jeon, Buettner, & Grant, 2018). In addition, a 2017 study on working conditions of ECE providers found the average annual income of providers was US$21,000, with 42% of respondents living at or below federal poverty level (Linnan et al., 2017).
ECE providers have been found to have low physical activity levels (Hibbs-Shipp, Milholland, & Bellows, 2015; Linnan et al., 2017; Sharma, Upadhyaya, Schober, & Byrd-Williams, 2014). Schools are typically a sedentary environment, with ECE providers reporting average sedentary behavior for 8 hours a day (Linnan et al., 2017; Sharma et al., 2014). A recent needs assessment conducted in eight Colorado Head Start programs indicated that teacher access to physical activity may be limited due to job-related factors, including time, fatigue, and money (Hibbs-Shipp et al., 2015). A study of Head Start teachers in Texas focused on nutrition knowledge and behaviors found only 9% of teachers reporting their nutrition habits were healthy; over one-fourth had not consumed fruits or vegetables the day before (Sharma et al., 2013). With 54% agreeing that they did not know which nutrition information to believe, this study showed the lack of access Head Start or preschool providers had to supportive nutrition information.
Job-related challenges and minimal opportunities for healthy eating or being physically active may contribute to ECE providers being disproportionately impacted by chronic mental and physical health conditions. For example, the rates of depression of ECE providers are 3 times the national average (36% vs. 12% clinically depressed) (Linnan et al., 2017) and ECE providers have a higher prevalence of being obese, as well as having heart disease and diabetes compared with the general population (Linnan et al., 2017; Sharma et al., 2013; Whitaker, Becker, Herman, & Gooze, 2013). These studies highlight the need for environmental supports that promote ECE provider’s health and well-being.
The literature on healthy eating and physical activity interventions in ECE settings primarily focuses on improving outcomes in children, with few interventions focusing on improved outcomes of ECE providers. In elementary school settings, the implementation of workplace wellness (WW) programs has been associated with positive outcomes. For example, a comprehensive 2-year WW program in a large public school district significantly improved several health outcomes in staff, including increased days and minutes of physical activity, fruit and vegetable consumption, and restful sleep (LeCheminant, Merrill, & Masterson, 2017). This study suggests that WW programs can be successful in school-based settings, which are likely to translate to preschool centers. The purpose of this study was to present findings from a healthy eating–focused and physical activity–focused WW program implemented in ECE centers. This WW program was one component of a larger obesity prevention program implemented in diverse ECE centers.
Method
The Culture of Wellness in Preschools (COWP) program is an early childhood obesity prevention research program that aims to increase healthy eating and physical activity in 3 to 5 year-olds (more information can be found at www.cowpprogram.com). The program has five components including (a) classroom-based nutrition education; (b) child-focused physical activity education; (c) parent wellness workshops; (d) policy, system, and environment changes; and (e) WW. Although many interventions cited in the literature focus on child health outcomes, the WW component of the COWP program provides a program to support the health and wellness of ECE providers.
The goal of the WW component was to promote ECE provider health and well-being in the workplace. The purpose of this evaluation study was to (a) describe healthy eating–related and physical activity–related awareness and adoption of behavior change of ECE providers after participating in COWP WW program; (b) analyze demographic factors related to healthy eating and physical activity awareness, and physical activity and healthy eating behavior change; and (c) explore facilitators and barriers related to ECE provider participation in COWP WW program.
Participants
COWP WW program was implemented from 2015 to 2017 at 35 delegate agencies which included 69 physical ECE centers (delegate agencies can include more than one ECE center). The sample consisted of Head Start (n = 9), community-based (n = 21), and school-based (n = 5) preschools located in six counties throughout Colorado, including Denver, Jefferson, Adams, Arapahoe, El Paso, and Pueblo. All ECE centers participating in the COWP WW program served low-income families. Within these preschools, all ECE providers (n = ~1,000) were invited to participate in the COWP WW program. Approval for the evaluation study was obtained from Colorado Multiple Institutional Review Board (protocol #12-0902).
Procedures
The WW program focused on the well-being of ECE providers by offering health and wellness challenges that fostered goal setting and accountability among coworkers. Workplace wellness challenges (e.g., walking challenges, fruit and vegetable consumption challenges) were offered as part of COWP WW program by four University-hired Research Assistants (RAs) to all ECE providers at ECE centers who were participating in COWP. A director or wellness champion at each center selected to help promote and participate in the WW challenges. Culture of wellness in preschool RAs attended a kick-off event, such as a Toss it Together Salad lunch, and asked ECE providers to sign up for the challenge. Research Assistants distributed WW challenge materials including healthy eating or physical activity–related tracking logs. Challenges varied in length and ranged from 1 week to 6 weeks, depending on the preference of the center. Culture of wellness in preschool RAs also sent Monday motivational e-mails once a week to all participating ECE providers to remind them of the challenge and provide healthy eating and/or physical activity tips. Early childhood education providers chose to compete against themselves or coworkers. Samples of COWP WW challenges are available electronically (cowpprogram.com).
Measures
After the intervention, RAs administered two surveys to evaluate the impact of the intervention: (a) a provider postsurvey in the spring of 2016 and spring of 2017 and (b) a WW challenge survey that was sent out immediately after the completion of every WW challenge. Both surveys were administered electronically and in-person to increase response rates. Data from the provider postsurvey and WW challenge survey were collected and managed using REDCap (Research Electronic Data Capture). The average time for completion of the provider postsurvey was approximately 15 minutes, and the average time for the completion of the WW challenge survey was 5 minutes.
Provider postsurvey
This survey contained 25 items, including several pertaining to participant demographic characteristics, such as their ethnicity (Hispanic, Latino, or Spanish origin; coded as yes/no) and highest grade or year of school they completed (some high school, high school graduate, some college or technical school, and college graduate) which was dichotomized for the analysis (0 = less than a college degree, 1 = college degree or greater). Early childhood education providers were asked how many years they had been teaching in ECE settings (continuous variable = 1-43 years), and the number of years they had been participating in the COWP program (continuous variable = 1-7 years). This survey also asked about healthy eating–related and physical activity–related awareness and adoption of behavior changes after participating in COWP WW program. For example, providers were asked to rate the extent of their agreement with the following statements about their awareness of fruit and vegetable consumption and physical activity. On a 5-point Likert-type scale (i.e., strongly disagree, disagree, neutral, agree, strongly agree), they answered the following questions: “After participating in the COWP WW program, I am more aware of the importance of eating fruits and vegetables” and “After participating in the COWP WW program, I am more aware of the importance of being physically active,” which were collapsed to a dichotomous response (strongly disagreed, disagreed, or neutral versus agreed or strongly agreed). Providers were also asked about their adoption of fruit and vegetable consumption and physical activity behaviors via the following questions: “After participating in the COWP WW program, I eat more fruits and vegetables at work” and “After participating in the COWP WW program, I am more physically active at work.” Participants rated this on the same 5-point scale, which was also dichotomized in the analysis.
WW challenge survey
This survey contained seven open-ended questions and was administered electronically after participation in a WW challenge. These open-ended survey questions assessed goals participants set during the challenges, as well as facilitators and barriers to participating in the WW challenges, such as “What were the barriers to completing your goal/s?” Responses were collected via an e-mailed survey link.
Data Analysis
Descriptive statistics were employed for the provider postsurvey. Next, two multivariable logistic regression models using odds ratios (ORs) and 95% confidence intervals (CIs) were analyzed to calculate the strength and significance of the associations between demographic factors, years teaching in ECE settings, years of participation in the COWP program and percent agreement (e.g., agree or strongly agree) that participation in the COWP WW program increased awareness of health behaviors (Model 1) and adoption of health behaviors (Model 2). All predictor variables were added simultaneously to each model. All quantitative analyses were performed in SPSS (IBM SPSS Inc., 2012) and a p-value of <.05 was considered significant.
To analyze qualitative data from the WW challenge survey, open-ended survey responses were analyzed by trained RAs using open-coding to identify themes related to facilitators and barriers to participation in the COWP WW program. Structural coding, coding that finds relationships, similarities, or differences when analyzing the survey responses was utilized (Saldana, 2013).
Results
Demographics for the participants of the COWP WW program are included in Table 1. In total, 250 providers (response rate: 25%) completed the postsurvey. Of them, 96% of providers were female and one third (33%) were Hispanic or Latino. More than half (62%) of the providers were college educated and 28% completed 1 to 3 years of college. The average years of working in the ECE setting was 13 years, and 1.5 years for participating with the COWP program.
Demographics of Early Childhood Education Providers (n = 250)
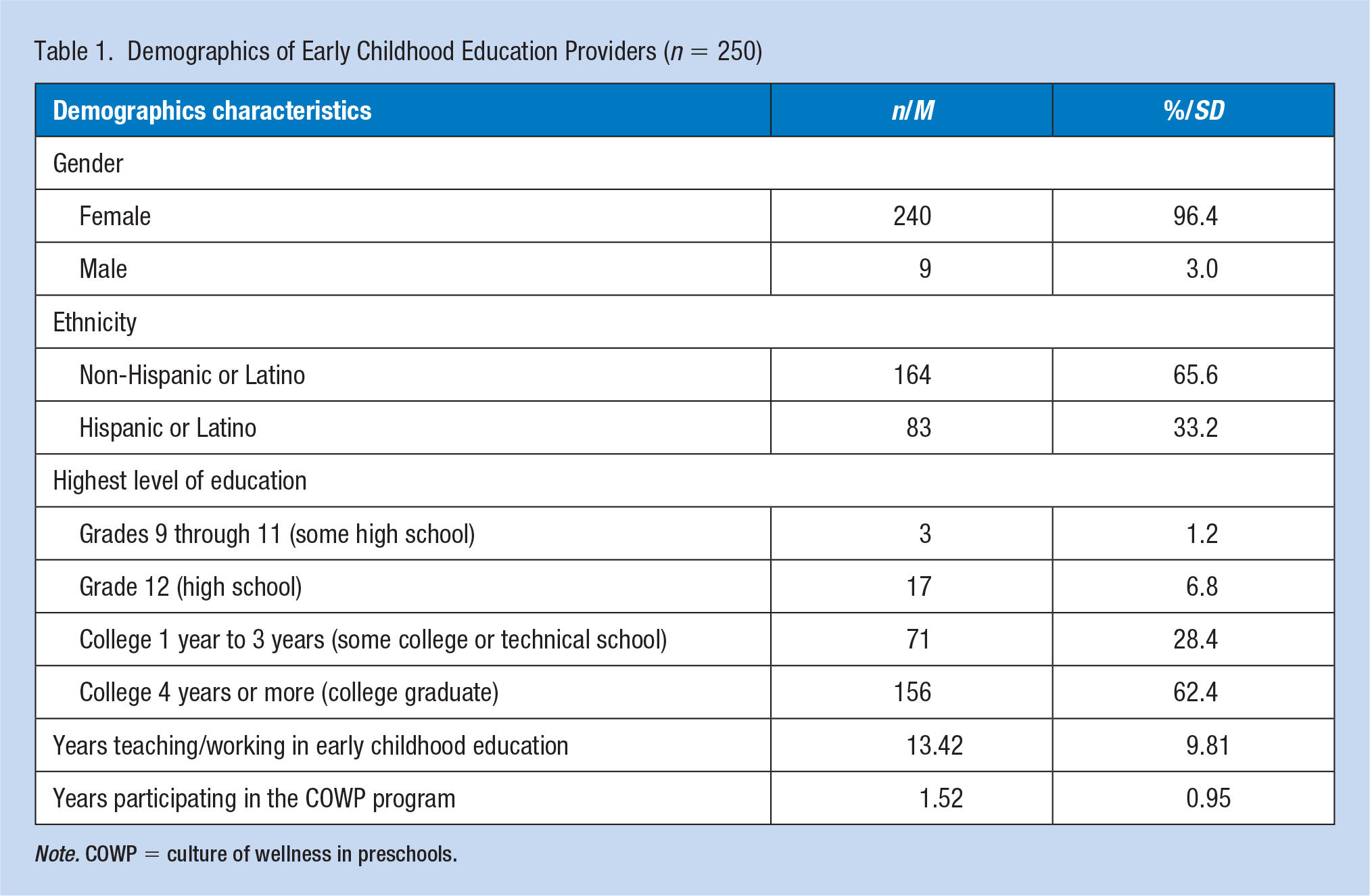
Note. COWP = culture of wellness in preschools.
Most providers agreed that they were more aware of the importance of eating fruits and vegetables (84%) and of being physically active (84%) after participating in the WW program (Table 2). Eighty-one percent of providers reported eating more fruits and vegetables and 80% reported being more physically active in the workplace after participation. At home, 77% of providers agreed that they ate more fruits and vegetables and 76% agreed that they were more physically active after participating in the WW program.
Healthy Eating–Related and Physical Activity–Related Awareness and Behavior Change After Participation in the COWP WW Program (n = 250)
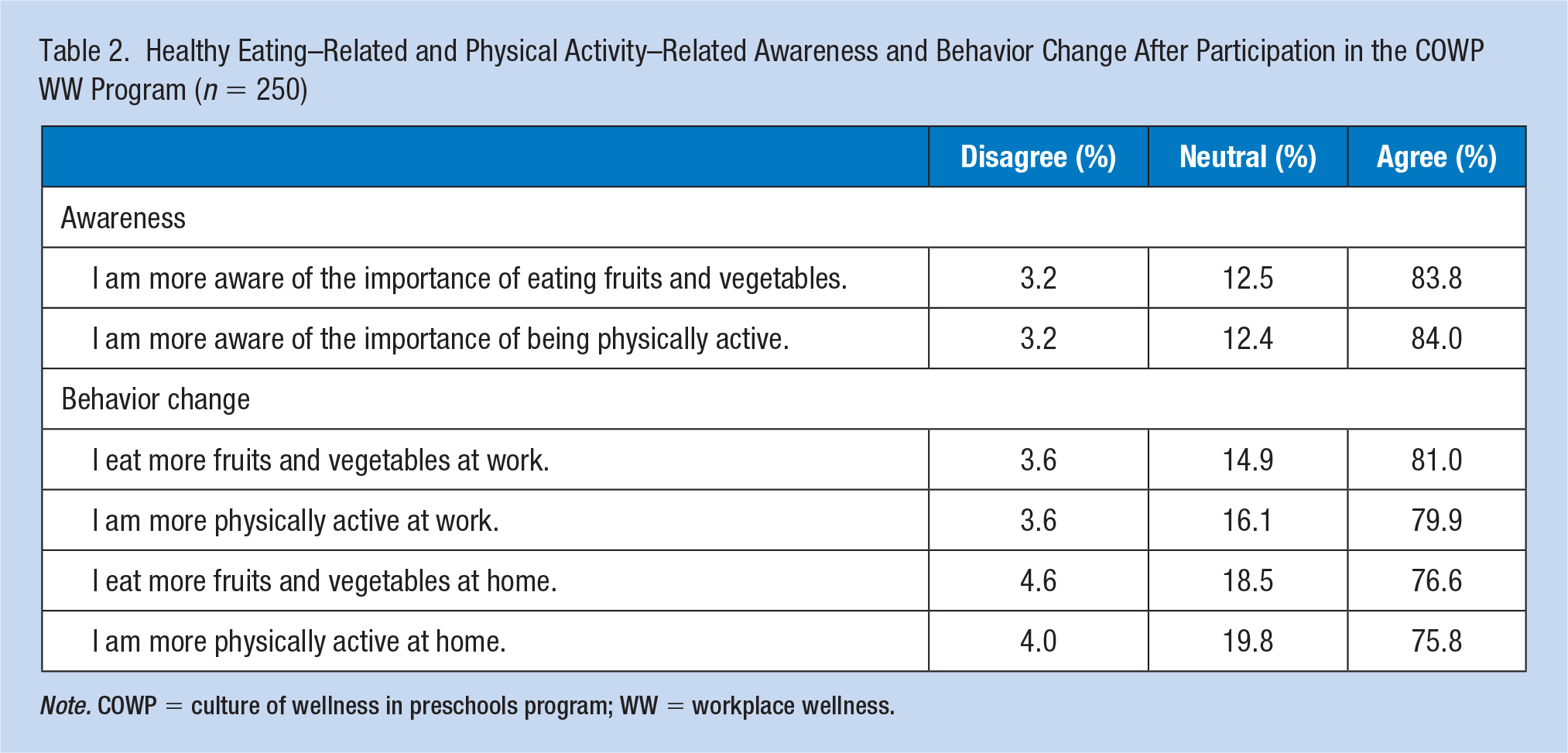
Note. COWP = culture of wellness in preschools program; WW = workplace wellness.
We found a statistically significant association for every 1-year increase in teaching in ECE centers, the odds of awareness of health behaviors increased by a factor of 1.10 (OR = 1.10; 95% CI = [1.00, 1.21]) (Table 3). No other predictors were significant. For the second model, there were no significant differences in the odds of agreement related to the adoption of health behaviors by ethnicity, education, years teaching in ECE centers, or years participating in the COWP program.
ECE Provider Awareness and Adoption of Health Behaviors After Participating in the COWP WW Program (n = 250)
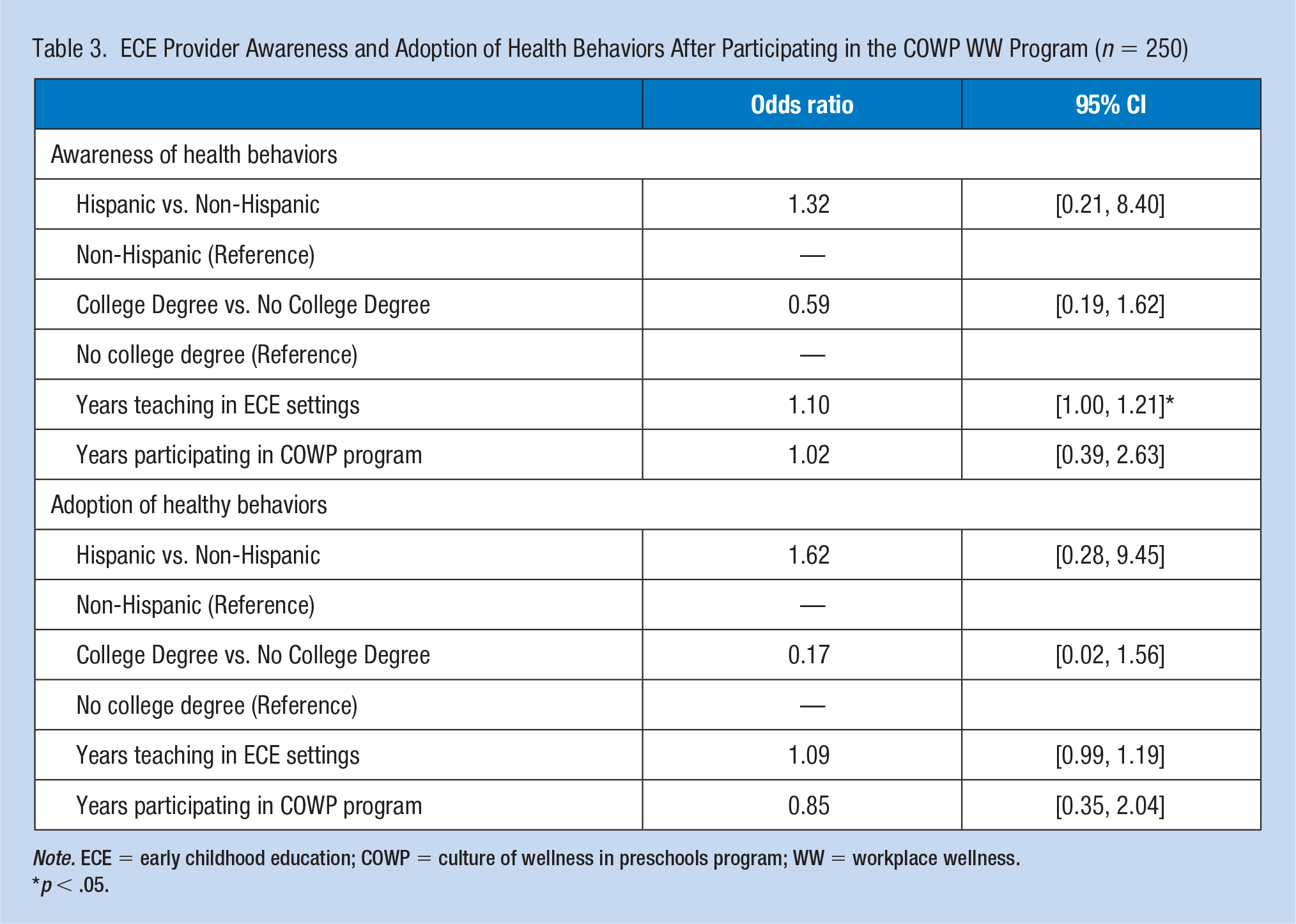
Note. ECE = early childhood education; COWP = culture of wellness in preschools program; WW = workplace wellness.
p < .05.
Qualitative
A total of 108 ECE providers responded to the WW challenge survey that asked open-ended questions about participation in the WW program. The three most commonly reported facilitators to participating in the WW program were (a) internal and external motivation, (b) awareness of current habits, and (c) teamwork with coworkers. Internal and external motivation was the most common response with over one fourth of participants reporting personal goals and accountability as facilitators related to motivation and participation. Participants expressed that setting their own personal goal and/or having coworkers hold them accountable to their goals helped them participate in the challenge. One provider said, “It kept us better focused towards meeting our goal just by setting one.” Another said, “When colder weather comes and things get busy at work, I tend to forget about drinking water. It makes a huge difference in how I feel. This challenge helped me get back on track.” A final provider shared, “I like them because I already drink a lot of water and it held me more accountable for a healthy lifestyle change.”
The second theme that emerged was increasing awareness of current habits, which consisted of providers realizing which health behaviors they currently were or were not utilizing while participating in challenges. One provider said, “I like that the program that supports our students, supports us as teachers to be more active and be more aware of what we are consuming,” and another responded, “Made me think about my water consumption and how it was so low.” Another provider shared that it “Made me more aware of what my goal was and I worked harder to keep it.” Providers also reported teamwork with coworkers as a factor that supported participation in the COWP WW program. Early childhood education providers found ways to incorporate group activities in their individual goals. One provider responded, “It was a lot of fun doing Zumba with coworkers,” and another said, “I like doing something as a team.”
Themes related to barriers to participating in the COWP WW program included (a) time constraints, (b) setting a challenging goal, and (c) difficulty tracking goals and activity. Time was by far the largest barrier to participation, with providers commenting they didn’t have enough time to prepare or participate in WW challenges. Comments such as “Time is always a challenge,” “working 2 jobs,” and “having to fill up a water bottle when I was running behind” are all examples of how participants struggled to participate in the WW programs due to time constraints. The second theme related to barriers for participants was difficulty meeting the challenging goal they set for themselves. Setting too challenging of a goal left some providers commenting that they didn’t feel capable of meeting that goal. Several providers mentioned setting a goal of drinking less soda with one provider saying, “cutting out soda from meals” was a barrier to completing their goal. Difficulty tracking goals and activities was the third most common barrier identified. Some participants struggled with remembering to complete daily activities or track those activities. One provider said, “I would forget to fill out the calendar and at times I would forget about the challenge. It’s self-reminders to myself that I need to be more on top of.” Another provider said, “There was one morning that I simply forgot to drink 8 oz first thing in the morning. It was a busy morning and one when my typical routine was disrupted. That leads to me getting off track.”
Discussion
This evaluation study aimed to understand the impact of COWP WW program on ECE provider awareness and adoption of healthy eating–related and physical activity–related behaviors. Demographic factors related to ECE providers’ awareness and behavior changes, as well as facilitators and barriers to participation in a WW program in ECE settings, were explored.
We found an increase in awareness related to healthy eating and physical activity. After participating in the COWP WW program, providers agreed they were more aware of the importance of eating fruits and vegetables and being physically active. This finding differs from some existing literature. Although some WW interventions aim to increase awareness of health and wellness to initiate behavior change (LeCheminant et al., 2017), few studies measure or report on change in awareness levels. A 5-year WW intervention outside of ECE settings that aimed to improve the health and well-being of employees found no significant improvement in knowledge/awareness around physical activity and diet (Blake, Zhou, & Batt, 2013).
This evaluation study also measured self-reported behavior change after participation in the COWP WW program. Providers reported that participation increased their consumption of fruits and vegetables at work and activity levels at work. Providers reported more behavior change at work compared with in the home. The COWP WW program targets behaviors in the workplace, which explains the larger impact in the workplace compared with the home environment. These findings also fit within the Transtheoretical Model (Stages of Change Model) explaining an individual’s readiness to change a particular behavior (Glanz, Rimer, & Viswanath, 2014). Early childhood education providers may report increases in awareness; however, some providers may not be ready to make a change, and therefore, they are less likely to report an increase in behavior change. A study on a WW intervention in ECEs in California found similar results of no significant differences in provider personal health behaviors, but significance in provider’s comfort level in discussing nutrition information with preschool parents and an increase in fruits and vegetables served to children after the intervention (Gosliner et al., 2010). These findings highlight the potential for WW programs to increase the adoption of healthy behaviors in ECE settings.
Minimal significant differences were found between awareness or behavior change and demographic characteristics of ECE providers. However, the odds of reporting an increase in the awareness of eating fruits and vegetables and being physically active increased as years working in ECE settings increased. This finding may be confounded by provider age, which was not collected in the staff survey. Years working in ECE settings is likely associated with age of employees; those having worked in ECE longer likely being older. Older employees may notice a deterioration in their physical health, and therefore, be ready to make health and wellness changes. This hypothesis aligns with existing research that found that as age increases, so does knowledge gain related to various health behaviors (Abell & Main, 2016).
Internal and external motivation, awareness of current habits, and teamwork were identified as facilitators to COWP WW program participation. Facilitators to WW participation among employees in non-ECE environments align with these findings. The most common themes identified include “personal motivation” and “social supports” (Fletcher, Behrens, & Domina, 2008), as well as “healthy behavior awareness” (Flannery & Resnick, 2014). Flannery and Resnick’s (2014) study shared participants’ quotes focused on healthy behavior awareness. Participants shared that after participation in the WW program, they thought more about the foods they ate and therefore made a conscious effort to read label, stop mindlessly eating, and eat healthier foods, similar to the findings of this study. Early childhood education centers implementing WW programs should consider ways to maximize these facilitators by sharing healthy messages, having participants set realistic and achievable goals, and fostering social support among coworkers.
Barriers related to participation in the WW program included time constraints, difficulty tracking activity, and setting a challenging goal. Several studies also found time to be a common barrier to WW participation (Blake et al., 2013; Flannery & Resnick, 2014). Flannery and Resnick’s study shared that time both inside and outside of work, along with outside-of-work responsibility made it difficult to participate in WW programs. This could be due to family responsibilities outside of work, or a second job due to low wages, making it difficult for ECE providers to prioritize their own health. In an environment where staff turnover is high (Grant, Jeon, & Buettner, 2019), ECE sites are often understaffed and finding the time at work to take active breaks may be difficult for ECE providers, in addition to limited time outside of work. This turnover is related to working conditions and provider well-being (Grant et al., 2019), so finding ways to improve providers’ well-being is important. Future WW programs in ECEs should help providers identify easy goals that can be scaffolded and improved upon over time. Effective WW programs in ECE settings should work to reduce these identified barriers to promote WW participation.
Limitations
Survey data collection from ECE providers at the end of the school year is a challenge. The sample size is not inclusive of all providers who participated in a WW program throughout the year. Questions on the staff post-only survey only collect WW data on providers who participated in the WW program; therefore, the researchers are unable to compare data with providers who did not participate or understand why providers chose not to participate at all. The authors also acknowledge that a post-only design is a limitation, but was a necessity due to provider time and resources. Researchers tied the survey questions to a behavior change theory, the Transtheoretical Model. For example, the precontemplation stage focuses on awareness of a behavior change and the action stage focuses on the adoption of a behavior change. Moving forward, researchers will collect pre- and postdata for WW program. Self-reported awareness and behavior change is an additional limitation of this evaluation study. Finally, age was not collected as a demographic variable and may be a confounding variable.
Conclusion
ECE providers face challenging work conditions that impact their physical and mental health and well-being. There is a need to foster innovative physical health promotion strategies to improve the well-being of the early child care workforce, which, in turn, may improve the job satisfaction and job retention of this critically vital job sector. Having healthy ECE providers also increases the quality and consistency of care of our youngest members of society, which is vitally important since the early childhood years are when children develop the cognitive, language, motor, and socioemotional skills necessary to support a productive and happy life (O’Connor, Blewitt, Nolan, & Skouteris, 2018; Shonkoff, 2010). This evaluation study suggests that WW programs in ECE settings can support provider wellness by increasing their awareness and adoption of health behaviors in the workplace.
Implications for Occupational Health Practice
Findings from this evaluation study suggest the following: (a) WW programs in ECE settings can increase awareness and adoption of healthy eating–related and physical activity–related behaviors among ECE providers, and (b) WW programs implemented in ECE settings should emphasize facilitators and reduce barriers. Occupational health practitioners should identify and assess current health habits of providers and create a space for them to set achievable goals, share those goals with others, and work collaboratively with coworkers to potentially increase participation in WW programs. Occupational health practitioners may also need to consider creating set times for providers to take active breaks, help providers identify attainable goals, and give providers easy ways to track their activities, helping to reduce the barriers to participating in WW program that are identified in this study.
Applying Research to Practice
There is a strong relationship between working conditions in ECE settings and ECE provider health disparities. Early childhood education centers need to adopt WW programs to foster health-promoting environments. The objective of this study was to evaluate the effectiveness of a healthy eating–focused and physical activity–focused WW program in ECE settings. The results from this study revealed that the WW program increased the awareness and adoption of health behaviors among ECE providers in the workplace. These results reinforce the importance of occupational health practitioners promoting WW programs in ECE settings to increase healthy eating and physical activity outcomes.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the funders for supporting this work including the Colorado Health Foundation (CHF-6471 for Dr. J.P.) and Colorado Department of Health and Human Services (CMS#84020 for Dr. J.P.).