
Abstract
Background:
The sedentary aspects of many U.S. occupations and the amount of time American workers spend in the workplace make it an ideal location to implement health promotion programs.
Methods:
This study assessed the effectiveness of a free smartphone app with a goal-setting feature to increase physical activity (PA) and impact anthropometric, body mass (BM), and body composition (BC) changes among overweight and obese women within a community health workforce. Eighteen overweight and obese (body mass index [BMI] = 32.18 ± 4.48 kg/m2), adult (50.73 ± 8.76 years), female volunteers, tracked daily steps with a free smartphone app (StridekickTM) over an 8-week period. Pre- and post-program body composition (BC) measurements included: relative (%) body fat (BF), fat mass (FM), fat-free mass (FFM), and lean mass (LM), using dual X-ray absorptiometry (DEXA scan), and five anthropometric measurements (biceps, waist, abdomen, hips, and thigh).
Findings:
Pre- to post-program average daily steps resulted in significant anthropometric changes for biceps, hips, and thigh measures, with encouraging changes in FFM, LM, and relative (%) BF. The goal-setting feature of the app did not result in significant differences between the experimental and control groups. No differences were noted in FM, BMI, waist, and abdomen or step goals compared with steps completed.
Conclusions:
An occupational PA health promotion intervention program that tracked daily steps through the StridekickTM smartphone app resulted in anthropometric, BM, and BC changes.
Application to Practice:
The workplace is an ideal location to affect change in health behaviors via a free smartphone app to increase PA and improve health.
Background
The World Health Organization (2023) estimates approximately 3.2 million deaths each year are attributed to physical inactivity, of which about 2.8 million people die annually due to excess weight gain. Curbing excessive weight gain is key to improving health and reducing associated comorbidities. The sedentary aspects of many U.S. occupations have been associated with increased health risks, such as obesity, type II diabetes, and heart disease (Alòs et al., 2022; Pate, 2019). The amount of time American workers spend at work makes the workplace an ideal setting to impact health. Women often cite “lack of time” as a primary barrier to exercise, and the incorporation of a physical activity (PA) intervention in the workplace might be a way to overcome this barrier (Peng et al., 2023). Comprehensive workplace occupational programs that are health-focused and employee-centered have the potential to positively impact workers’ health and quality of life, and therefore, are ideal for impacting health behaviors (Fetherman & Cebrick-Grossman, 2023; Fetherman et al., 2020; Metcalfe et al., 2020). Workplaces that offer PA programs as part of employee health promotion programs through prevention and intervention behoove the employer to improve health (Office of Disease Prevention and Health Promotion, U.S. Department of Health and Human Services, n.d.). The effectiveness of interventions to reduce sedentary time and increase PA during the workday has been investigated with encouraging health outcomes (Bailey, 2021).
Despite the continued emphasis on the benefits of regular PA to reduce chronic disease, less than 30% of adults engage in sufficient PA (Liguori, 2021; Piercy et al., 2018). Sedentary behavior is defined as awake activity in a sitting or a reclining posture with an energy expenditure less than 1.5 metabolic equivalents (METs), with resting expenditure equal to an MET level of 1.0 (Liguori, 2021). METs are a standardized way to determine absolute intensity of different PAs and depending upon the activity, MET levels vary. For example, a MET level between 2.0 and 2.9 is considered light intensity like walking around an office or standing and performing light office work. A MET level between 3.0 and 5.9 is moderate activity, such as brisk walking or raking leaves, whereas a MET level of at least 6.0 is vigorous activity, for example, running at 7.0 mph or carrying heavy loads such as bricks (Liguori, 2021).
Walking, the most common form of PA has been supported for overweight and obese women to improve health, resulting in increased aerobic capacity, weight management, weight loss, and body mass (BM) changes to reduce obesity-related risk factors (Batrakoulis et al., 2018; Cebrick-Grossman & Payne, 2016; Grossman et al., 2018). Evidence also supported walking via accelerometer technology to record steps and increase PA in middle-aged overweight women to reduce cardiovascular disease risks (Arigo et al., 2020; Grossman et al., 2018). In addition, a systematic review supported a smartphone app in the workplace as an effective and feasible means to promote PA, although more work is suggested to determine reasons for attrition (Buckingham et al., 2019).
The popularity of smartphone apps offers accessible ways to easily track PA. In young adults, significant increases in PA (walking) with a mobile phone app were identified, along with the importance of goal setting and self-monitoring, important for program compliance and adherence (Walsh et al., 2016). Romeo et al. (2019) conducted a meta-analysis from 2007 to 2018 specific to the influence of smartphone apps and PA in adults. The results showed a modest effect in increased PA with the greatest impact for short-term duration programs less than 3 months in length. In addition, a systematic review and meta-analysis reported the effects of mobile health app interventions and the potential of reducing sedentary time, and increasing PA fitness levels in older populations, between 3 and 6 months in duration (Yerrakalva et al., 2019). More recent work has supported the long-term effectiveness (12 months) of a multi-component mobile health intervention, combining a smartphone app and an activity tracker wristband, on weight loss, BC, PA, and caloric intake in overweight and obese sedentary adults (Lugones-Sanchez et al., 2022). This 8-week short duration study aimed to assess (a) the effectiveness of a free smartphone app in increasing PA, (b) whether or not the use of the goal-setting feature of the app increased PA levels, and (c) how increased PA impacted changes in anthropometric, BM, and BC among overweight and obese women within a community health workforce.
Methods
Overview
This study was based within a community-based participatory research approach, a partnership between university faculty and a non-profit, community health care, and multifaceted service social assistance provider, for special needs individuals with approximately 500 employees, of whom 87% were females. Community-based participatory research partnerships among researchers and workplaces address concerns which translate research into useful and practical workplace interventions. The workplace selected the free smartphone app, StridekickTM (Matchup, Chicago, IL, USA) designed to track employees’ daily steps to increase PA and determine the effectiveness of the goal-setting app feature, while impacting anthropometric, BM, and BC measures for improved health. The project was based within the parameters of the employees’ job requirements and organizational policies. The university institutional review board (IRB) and the workplace administrative wellness committee approved this study.
Program Description
A pre-test, post-test, randomized, time × group mixed-design compared daily steps over an 8-week period with participants assigned via block randomization to the experimental group (n = 9; goal-setting group) or control group (n = 9; non–goal-setting group). Both the experimental and control groups used the StridekickTM smartphone app (iPhone or Android) to record their PA, daily steps through the “friends” feature of the app. This feature also permitted data sharing used by a research assistant (student) who tracked all data and at the conclusion of each week, downloaded and recorded the completed daily steps for both groups. Baseline steps were determined (week 0) for all participants. The experimental group only used the goal-setting component of the smartphone app known as the “streak” feature which allowed participants to set a daily step goal and create a PA weekly “streak,,” meant to encourage PA and the continuation of their “streak,” that is, or steps. The use of the “streak” feature also enabled the experimental group to monitor their step goals throughout the study period. The control group did not use the “streak” feature, instead, their step goals were initially set after the orientation session and recorded on their demographic questionnaire, baseline (week 0). The control group then determined their daily step goals at the start of each week without the support of the StridekickTM “steak” feature that supported step goals and monitoring throughout the week.
Study Population
Participants were recruited at the workplace, a community health care and multifaceted service social assistance provider for special needs individuals through publicized informational flyers and electronic newsletters designed to increase PA among employees. Study criteria included: a body mass index (BMI) either in the overweight or obese category between 25.0 and 29.9 or 30.0 and 35.9 kg/m2, respectively (Liguori, 2021), a sedentary lifestyle with no structured exercise outside of activities of daily living (with the ability to engage in daily PA), non-smoker, possession of a smartphone (iPhone or Android) for the wearable technology app, fluency in English, and no self-reported medical concerns. Ineligible criteria included: participating in another PA intervention, a medical contraindication for engaging in increased PA, and enrollment in any weight loss program, such as Weight WatchersTM or Jenny CraigTM.
A self-selected convenience sample of 29 female employees volunteered for the intervention. The full sample consisted of 18 overweight and obese (BMI = 32.18 ± 4.48 kg/m2) women (50.73 ± 8.76 years): nurses, nursing assistants, and administrative office workers. Four of the 29 participants who completed the study were not included in the data analysis as their BMI was normal (18.5–24.9 kg/m2; Liguori, 2021). An additional seven participants (three from the experimental group and four from the control group) dropped out of the study for various reasons, such as sickness and inability to complete data collection. To ensure confidentiality, each participant was assigned a number for identification, and was randomly assigned into either the experimental group (experimental [n = 9; BMI = 31.47 ± 4.21 kg/m2; 51.93 ± 6.05 years]) or control group (control [n = 9; BMI = 33.77 ± 5.53 kg/m2; 51.63 ± 12.59 years]). Interested individuals were invited to attend orientation sessions at the workplace with convenient dates and times for employees. Participant eligibility was established and confirmed through self-reported demographic information and a PA readiness questionnaire (PAR-Q; Thomas et al., 1992) after which an informed consent was completed during the orientation sessions.
Intervention
This 8-week study assessed the effectiveness of a free smartphone app in increasing PA, whether or not use of the app goal-setting feature increased PA levels, and how increased PA impacted changes in anthropometric, BM, and BC among overweight and obese women. The PA intervention was increased daily steps, tracked throughout the study period. Both the experimental and control groups used the free smartphone app (StridekickTM) to track their PA (steps). During the orientation sessions, all participants received instructions for increasing steps safely, with steps tracked during weeks 1 to 8 and end-program measures collected between weeks 9 and 10. The PA intervention progression was as follows: for weeks 1 to 3, an increase of no more than 20% above baseline, for weeks 4 to 5, an increase of no more than 20% above their individual average daily recorded steps during weeks 1 to 3, and, for weeks 6 to 8, an increase of no more than 20% above their individual average daily steps during weeks 4 to 5. This PA increase is consistent with exercise progression guidelines, to allow for intervention impact, that is, increased PA through daily step counts (Liguori, 2021). Initially (week 0), each participant set a daily step goal after which the groups differed in the use of the goal-setting smartphone app. The experimental group (goal setting) was directed to use the “streak” feature, wherein, participants set a daily step goal that created a PA weekly “streak” or step challenge, meant to encourage PA continuation of their “streak,” that is, steps. This feature also allowed participants to monitor their daily and weekly step goal(s). The control group did not use the “streak” feature of the StridekickTM app for goal setting. Instead, their daily steps were increased based upon the advice and direction provided during the orientation sessions when participants learned about the impact of PA and health and a safe progression of increased daily steps. After completion of the orientation sessions, all participants set an end-program (week 8) daily step goal with hopes to achieve it.
Data Collection
Participants were guided in downloading the StridekickTM app to their mobile phones and instructed on PA frequency (how often or daily), intensity (effort put forth), type (mode of exercise—walking), time (duration), and progression of exercise (how the body adapts). All participants were also instructed on the benefits and recommendations of daily PA, risks of a sedentary lifestyle, goal setting, and ways to reduce occupational sitting. In addition, they were directed to carry their smartphones during waking hours (workplace and home) and encouraged to continue their normal PA levels, and to track their daily steps without any increase. Activities of daily living were encouraged to remain unchanged, with no additional structured exercise program, outside of that indicated for this study. Baseline steps were determined during week 0 (pre-program). At the outset of each week (Sunday evening), all participants received a reminder text message to charge their phones and synchronize their steps with the StridekickTM app. Synchronizing ensured accuracy of the participants’ recorded daily step totals. In addition, the experimental group was reminded each week, to enter their daily step goal into the “streak” feature for their weekly streak challenge. Dietary behaviors were instructed to remain unchanged, to not confound study results, as the study intervention was PA and not caloric restriction and/or any dietary changes.
An exercise physiologist and registered dietitian, certified and trained in dual X-ray absorptiometry (DEXA) scan (General Electric, Madison, WI, USA) completed all anthropometric, BM, BC, and blood pressure measurements in a university BC laboratory. The anthropometric measurements included: weight and height for BMI calculation, along with five anthropometric circumference measures (in inches): waist, abdomen, hips, biceps, and thigh, with the latter two measured on the right side of the body for universal consistency (Liguori, 2021). The total inches lost per participant were determined from the reduction or differences in the girth measurement from pre-program (week 0) to the end-program measures (weeks 9–10). The BC and BM measurements included: relative percent body fat (BF), fat mass (FM), fat-free mass (FFM), and lean mass (LM). During the anthropometric, BM, and BC assessments, each participant received feedback of their pre-program (week 0) measures. After the end-program assessments (weeks 9 and 10), all participants received a written comprehensive report of their pre- and end-program data along with an explanation of the results. Inter-rater reliability was not performed.
Results
Descriptive and inferential statistical analyses examined data using SPSS Statistics (Version 24). Statistical tests of kurtosis, skewness, median, and mean confirmed normality of the data set. Dependent sample t-tests determined pre-/post-test anthropometric statistical significance for the full sample (n = 18) for thigh and biceps (p ≤ .01) measurements, along with an increase in lean BM (p ≤ .05). Reductions in inches of hips and abdomen, relative percent BF, and an increase in FFM in pounds were also noted, though not statistically significant (Table 1).
Changes in Key Outcomes, Full Sample, (n = 18)
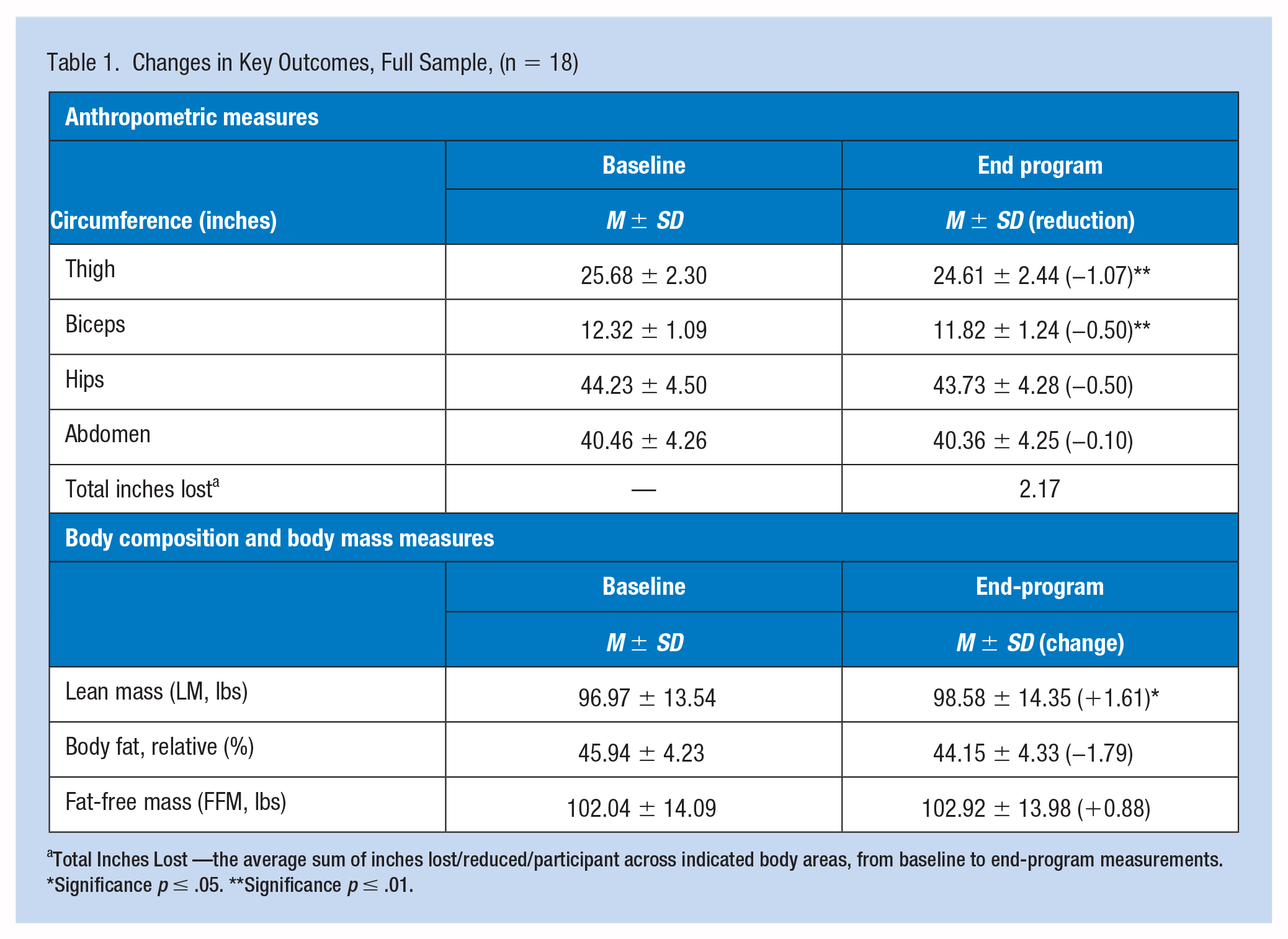
Total Inches Lost —the average sum of inches lost/reduced/participant across indicated body areas, from baseline to end-program measurements.
Significance p ≤ .05. **Significance p ≤ .01.
As shown in Table 2, dependent t-tests identified significant anthropometric differences within the experimental group (n = 9) for thigh circumference measurements (p < .05) and within the control group (n = 9) for thigh and biceps circumference measurements (p ≤ .01). Hip measurements were reduced for both groups, as were biceps within the experimental group, although not statistically different.
Change in Key Outcomes by Intervention
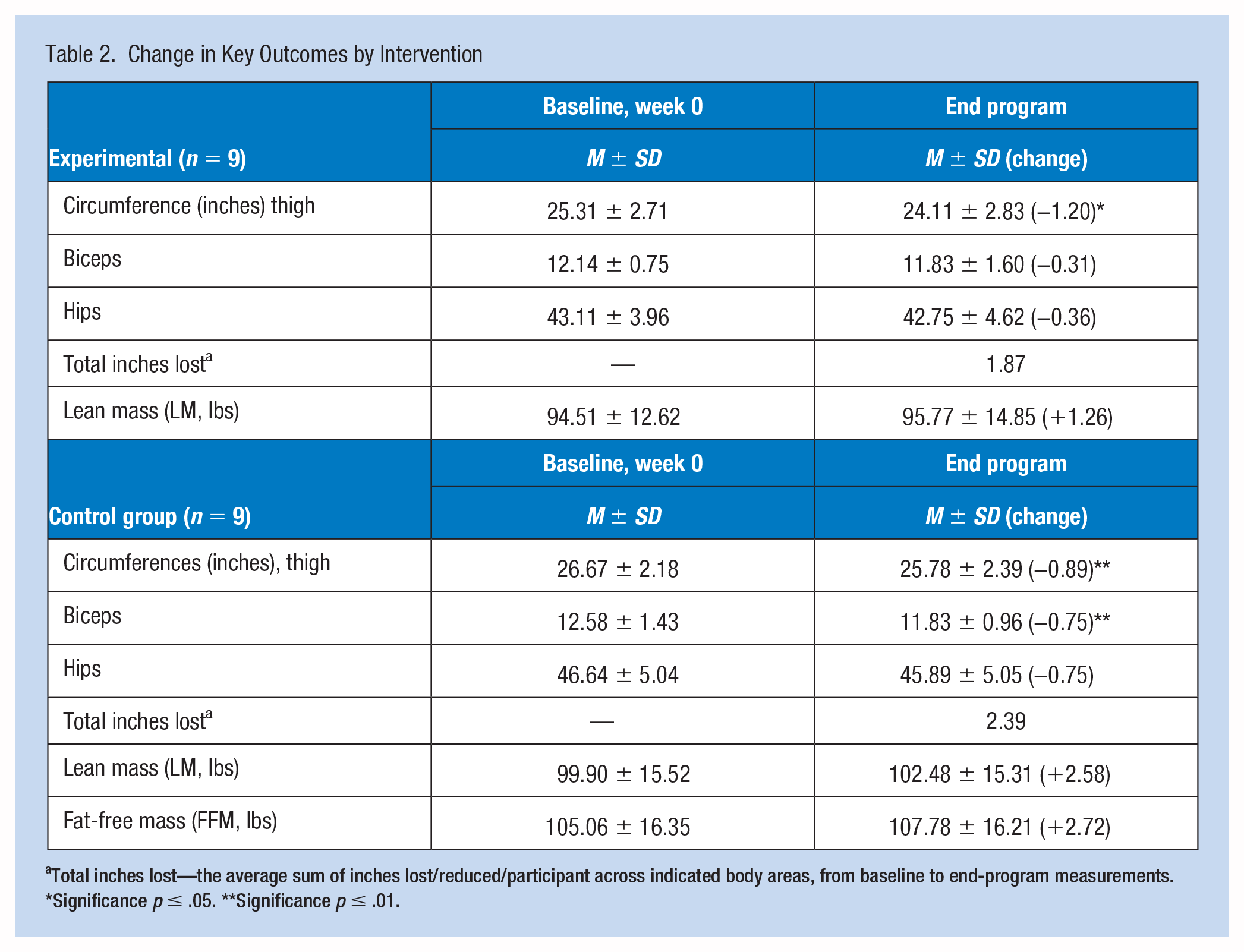
Total inches lost—the average sum of inches lost/reduced/participant across indicated body areas, from baseline to end-program measurements.
Significance p ≤ .05. **Significance p ≤ .01.
For BC measures, no significant differences were noted within both groups. However, BM differences were identified with increases in LM for both groups along with an increase in FFM for the control group (Table 2). Independent samples t-tests and multivariate analysis of variance (ANOVA) probed for anthropometric, BM, and BC differences between groups with no significant differences determined.
For the PA intervention, (pre–post) daily steps for the full sample (n = 18), (3,128 ± 143; 5,967 ± 837) significantly increased (p ≤ .05). Although the post-program daily steps completed, increased significantly from baseline, they were less than the average daily step goals set by all participants at baseline (week 0; 7,916 ± 1,909). Independent t-tests probed for differences between groups for daily step goals and daily steps completed and tracked by the smartphone app, with no significant differences identified for the experimental group (n = 9) ([7,756 ± 2,679]; [5,957 ± 698]) and the control group (n = 9) ([8,143 ± 2,056]; [5,897 ± 743]). Daily step goals created at the outset of the study for both groups exceeded daily steps completed at program end (week 8).
Discussion
The workplace is an ideal location to incorporate daily PA since “lack of time” is a primary exercise barrier for women (Peng et al., 2023). A workplace intervention program that incorporates steps, the most common form of PA, to reduce sedentary behaviors and impact health and reduce obesity-related chronic disease risk simply makes sense. This study demonstrated a realistic approach of incorporating an occupational PA intervention program into the workday through the use of a free smartphone app, StridekickTM.
Body mass changes are instrumental in improving health, such that, as lean BM increases, so does metabolic activity, in favor of increased energy expenditure, enhancing weight loss (Bellicha et al., 2021). A reduction in relative percent BF with increases in LM and FFM are key to weight control. Fat-free mass consists of all body components except fat. Lean mass has a small amount of essential fat from bone marrow and internal organs and is more metabolically active than FM (Bellicha et al., 2021). Most important, LM, such as skeletal muscle mass, burns about 13 kcals/kg of body weight/day for muscle and 5 kcals/kg of body weight/day for fat with approximately 80% of the difference in energy expenditure explained by BC and the remainder, due to genetics, age, and gender (DeNino, 2022). A workplace health promotion intervention program that increases PA, wherein BC is significantly changed with FM reduced, and FFM and LM increased, should be encouraged for improved health to reduce obesity-related chronic disease risks.
Regardless of group, use of the smartphone app helped participants increase PA and impacted anthropometric, BM, and BC measures positively. Use of the “streak” feature which allowed the experimental group to set and monitor their daily and weekly streak goals did not significantly increase the experimental group PA levels relative to the control group PA levels. Tracking PA via StridekickTM created a level of accountability for both groups, necessary for participant compliance particularly since this industry has a greater prevalence of obesity (Ross et al., 2019) with limited studies specific to PA interventions and improving health behaviors (Ito-Masui et al., 2021). This work is especially important for this population, as female nurses who represent the largest professional group of health care workers, are sedentary for about 50% to 60% of their workday (Reed & Prince, 2018). A recent web-based cross-sectional survey specific to PA and sedentary behaviors among nurses of whom more than 55% were obese/overweight, self-reported that they do not engage in PA with about 80% reported as sedentary (3 or more hours of sitting/week; Ross et al., 2019). Workplace PA interventions that reduce sedentary behavior and increase even low levels of PA are important in combating obesity and serious illnesses; yet few interventions have targeted nurses (Reed & Prince, 2018).
Conclusion
The StridekickTM app was deemed useful in tracking and recording daily steps regardless of groups as all participants PA increased throughout the 8-week study period. Physical activity increased significantly from baseline to end-program in both groups, as evidenced through the StridekickTM app “friends” feature that tracked and recorded approximately 6,000 steps per participant each day. This increased PA resulted in significant anthropometric, BM and BC changes for improved health for the full sample. However, for both the control and experimental groups, the participants’ challenge daily step goals set at baseline were greater than the average daily steps completed and tracked via the app, not unusual ambition for novice exercisers (Gjestvang et al., 2021). The “streak” feature of the StridekickTM app, used only by the experimental group, designed to encourage participants to set goals, continue their PA “streak” and monitor daily step goal progress, did not appear as impactful as anticipated, as evidenced by a greater increase in PA in the control group. Best practices in goal setting have begun to explore the importance of differentiating between performance and learning goals (Swann et al., 2021). The ability of the control group to monitor their daily steps via the StridekickTM app was enough to help them increase their PA levels without the use of the “streak” feature. This was evidenced through the study outcomes, as the control group surpassed the experimental group in both circumference measures (thigh, biceps, and hips) and in BM measures (LM and FFM). No significant differences were noted between groups, most likely a result of the small group sample sizes.
Limitations
The primary limitation of this work was the small group sample sizes which restricted significant statistical analyses between groups. Other limitations included an 8-week timeline and the need to continuously carry a smartphone throughout the day for PA tracking. Future work could include larger group sizes and longer intervention timelines with different populations, such as those of normal body weight, men, and participant companions for support. Additional work could investigate and explore the intersect between a smartphone app, an accelerometer, caloric intake/restriction, and/or stress levels, to further impact health behaviors.
Implications for Occupational Health Practice
Approximately, three of four Americans over the age of 20 are either overweight or obese (National Institutes of Health, National Heart Lung and Blood Institute, 2022). As obesity rates rise, so do serious illnesses, such as cardiovascular disease and diabetes (National Institutes of Health, National Heart Lung and Blood Institute, 2022). One way to combat the current obesity epidemic in the United States is with PA opportunities in the workplace where millions of Americans spend hours each day (Alòs et al., 2022). These study findings are relevant as participants increased PA through the use of a free smartphone app, (StridekickTM), which tracked daily steps and increased PA levels with positive health outcomes of anthropometric, BM, and BC changes in favor of improved health. In this study, the goal-setting feature did not result in significant increases in PA levels among the experimental group. Oftentimes, the goal-setting feature of free smartphone apps is only accessible with additional cost to the employer. Overall, the integration of such a health promotion program that improves health and reduces obesity-related chronic disease risks should be welcomed into the workplace.
Applications to Professional Practice
This workplace occupational health promotion program demonstrated a practical application of a free smartphone app, goal setting, and increased PA for a non-profit community health care and social assistance provider. The smartphone app was instrumental in increasing employee PA, although the goal-setting feature of the smartphone app used by the experimental group did not result in significant outcomes. However, PA was significantly increased and positively impacted anthropometric measures along with favorable changes in body mass and body composition measurements for improved health and reduction in obesity-related chronic disease. This community-based participatory (translational) research gives credence to the implementation of a partnership between academia and the workplace, as a useful approach to develop, implement, and evaluate health promotion programs.
Footnotes
Author Contributions
J.A.C.-G. along with D.L.F. conceptualized and designed the study, worked with the community-based partner, and completed the statistical analyses. J.A.C.-G. interpreted the data and wrote the intellectual content.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human Subjects Review
Human Subjects Review CITI Certification—The University of Scranton. Completion Date: April 13, 2021. Expiration Date: April 12, 2024. Record ID: 30596333.