
Abstract
Background:
Prior pandemic research has focused on physicians and nurses who provide direct patient care. Literature on the experiences of nonnurse/physician clinicians and nonclinical health care professionals is sparse.
Methods:
An observational, cross-sectional study was conducted over threetime points to examine the impact of COVID-19 on clinical and nonclinical healthcare professionals (n = 464).
Findings:
There were no significant differences in distress across survey waves, except for anger (p = .046). No significant differences in distress scores were found between job types. Multiple linear regression results varied. Both the threat and interrupted plans scores were significant predictors of distress. Resources available to healthcare providers (HCPs) were underutilized in all three waves.
Conclusions:
Healthcare professionals’ distress increases with exposure. Integrating self-care resources for staff may mitigate the impact and maintain a healthy work environment.
Application to practice:
Occupational health providers should incorporate these findings when developing opportunities to address the needs of health care professionals in the workplace.
Coronavirus disease (COVID-19) first appeared in Wuhan, Hubei Province in China in December 2019 (Zhu et al., 2020). On January 20, 2020, the first case of coronavirus in the United States was reported (Holshue et al., 2020). This highly contagious and deadly disease was declared a public health emergency on January 30, 2020, and a global pandemic on March 11, 2020 (Ji et al., 2017; Lehmann et al., 2015; World Health Organization [WHO], 2024).
Prior pandemics from the Spanish flu, severe acute respiratory syndrome (SARS), H1N1, through Ebola demonstrated adverse physical and mental health impacts on clinical health care providers (HCPs; Brooks et al., 2018; Gordon et al., 2020; Goulia et al., 2010; Ji et al., 2017). By early 2021, research on COVID-19’s impact on HCPs was limited and did not include nonclinical HCPs. Two non-U.S. meta-analyses revealed that psychological and mental impacts on HCPs, patients, and the public were prevalent. Luo et al. (2020) found anxiety and depression occurred in about one-quarter of the health care workers, 26% and 25%, respectively. Krishnamoorthy et al. (2020) observed poor sleep quality (43%), stress (33%), psychological distress (41%), insomnia (37%), posttraumatic stress symptoms (13%), anxiety (24%), and depression (25%) among health care workers.
Early in the pandemic, Aiyer et al. (2020) researched the mental health impacts of COVID-19 on HCPs in the United States using a web-based survey assessing stress and depression among physicians and nurses. Approximately 42% of HCPs screened positive for a mood disorder, and 49% had an elevated stress level. Evanoff et al. (2020) assessed the mental well-being among faculty and staff at an academic medical center during COVID-19. Among all workers, anxiety, depression, and high work exhaustion were independently associated with community or clinical exposure to COVID-19. A rapid systematic review of the mental impact of COVID-19 on HCPs included three studies from the United States out of the 59 included reviewed (Muller et al., 2020). Exposure to COVID-19 was the most reported correlate of mental health problems, followed by female gender, worry about infection, or about infecting others. HCPs in the high-stress group were female (69%) compared to male (29%) and significantly higher scores on anxiety, depression, and stress were found in registered nurses (RNs) compared to medical doctors (MDs). In a random sample of American households, McGinty et al. (2020) found 13% experienced persistent psychological stress. A gap remains in the literature determining the prevalence of psychological distress among clinical and nonclinical HCPs. Understanding is critical for the future health of the workforce. The purpose of this study was to explore the impact of COVID-19 on clinical and nonclinical HCPs over time at a large (1273 bed) midwestern, academic, quaternary hospital.
Methods
Study Design and Recruitment
This study used an observational, cross-sectional design consisting of three independent timepoints (initial, 6 months, and 12 months) at which an anonymous survey was collected from HCPs. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline was used. Recruitment posters and fliers were placed at hospital entrances and employee work areas. An embedded QR code on the posters and fliers directed the HCP to the study information sheet in REDCap. An institutional newsletter was also used for recruitment during the second and third surveys. Posters, fliers, and the newsletter included details about the study and inclusion criteria. Informed consent was obtained by clicking a link to begin the survey. Posters and fliers were visible throughout the data collection period. Institutional Review Board (IRB) approval was obtained from the Washington University Human Research Protection Office (IRB202101139).
Recruitment and data collection began a year after the start of the pandemic; February to April 2021, the second, August to October 2021, and third, January to March 2022. A convenience sample of clinical (nurses, respiratory therapists, pharmacists, nutritionists, physical therapists, occupational therapists, and social workers) and nonclinical or “other” (spiritual care, housekeeping, public safety, and clerical staff) staff over the age of 18 and English speaking were invited to participate. To test differences in the survey scores across the three independent time points, sample size estimation was conducted for an analysis of variance (ANOVA) with a medium effect size, alpha = 0.05, and power = 0.80. The required minimum sample size estimated for the study was 159 participants across all 3 time points, or 53 participants at each time. To maximize the available sample size for the analyses, if a participant did not complete a full subscale, they were excluded from the analysis for the specific subscale that was not completed.
Instruments
Questions included demographic and behavioral characteristics such as occupation (17 response options listed in Table 1) and direct contact with COVID-19 patients, 1 = “Not at all,” 2 = “A little bit (25% or less),” 3 = Moderate (26%–50%),” 4 = “A lot (51%–75%),” and 5 = “Very much so (greater than 75%).” The How People React Coronavirus (HPRC) survey was utilized (Marjanovic et al., 2007; Sterling et al., 2020). The HPRC survey was first used with nurses in 2004 during the SARS outbreak in Canada and again in 2020 at the beginning of the COVID-19 pandemic. The survey was found to predict symptoms of burnout in nurses (Marjanovic et al., 2007; Sterling et al., 2020). The alpha score for the survey is 0.96 for exhaustion, .92 for state anxiety, .80 for avoidance behavior, .85 for vigor, .89 for organizational support, and .60 for trust. The authors received permission to modify and use the HPRC survey with nonclinicians in this study. To the authors’ knowledge, this is the first time the HPRC survey was used with nonnurse clinicians and nonclinical HCPs.
Sociodemographic Characteristics of Clinical and Nonclinical Healthcare Professionals (N = 464)
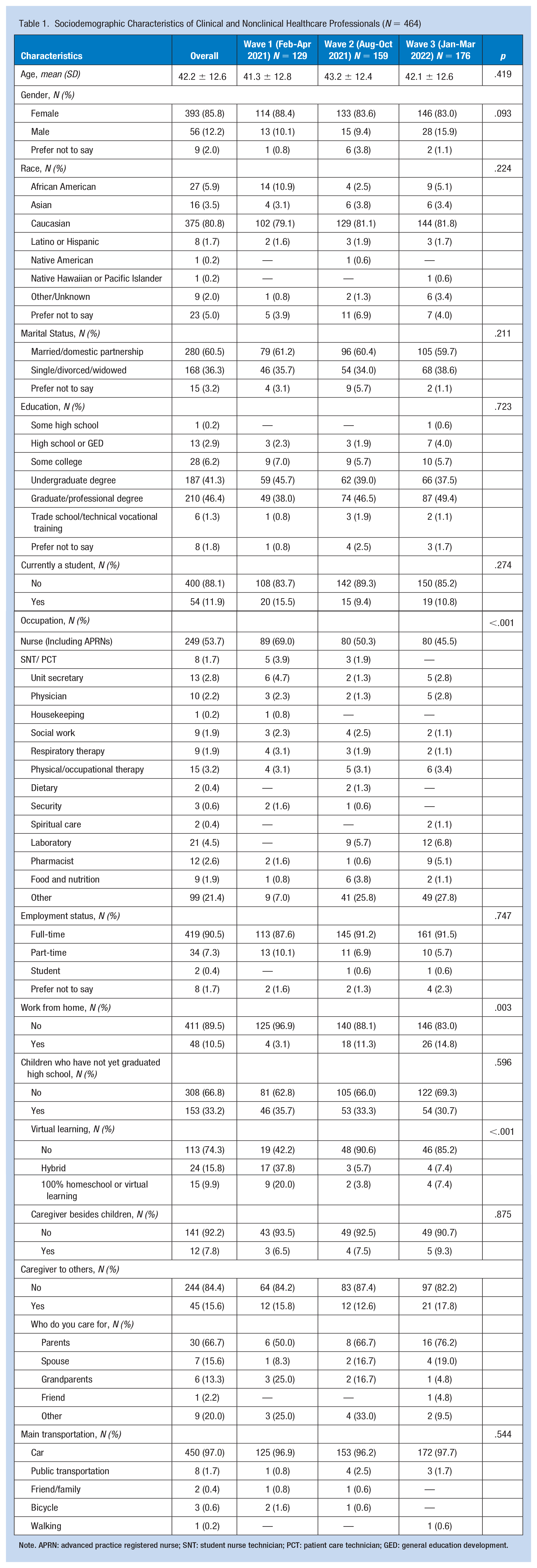
Note. APRN: advanced practice registered nurse; SNT: student nurse technician; PCT: patient care technician; GED: general education development.
Distress was measured utilizing the Profile of Mood States; anxiety, depression, anger, and fatigue subscales (Shacham, 1983). Distress contains 26 items with a 5-point Likert-type scale response from 1 (“not at all”) to 5 (“extremely”). Distress encompasses six anxiety items (on edge and uneasy), eight depression items (sad and miserable), seven anger items (annoyed and peeved), and four items related to fatigue (worn out and weary). The scale statements are prefaced with “Using the scale below, indicate your recent feelings about coronavirus by selecting the number that corresponds best to your feelings.” Summative scores for overall distress and each of the four subscales were used for analysis. The possible range of scores for overall distress is 26 to 130 with higher scores indicating higher overall distress. The possible range of scores for the anxiety subscale is 6 to 30 with higher scores indicating increased anxiety. The possible range of scores for the depression subscale is 8 to 40 with higher scores indicating increased depression. The possible range of scores for the anger subscale is 7 to 35 with higher scores indicating increased anger. The possible range of scores for the fatigue subscale is 4 to 20 with higher scores indicating increased fatigue.
Remaining calm was 1 item with a 4-point Likert-type scale response from 1 (“not at all true”) to 4 (“exactly true”). The scale statement preface includes, “I can remain calm when facing this difficulty because I can rely on my coping abilities.” For this analysis, the item was recoded to create a dichotomous variable. Remaining calm was recoded as 0 = “not at all true/hardly true” and 1 = “moderately true/exactly true.”
Worry was 1 item with a 5-point Likert-type scale response from 1 (“not at all true”) to 5 (“exactly true”). The scale statement asks, “In general, would you say you are a worrier, that is do you worry all the time?” For this analysis, the item was recoded to create a categorical variable. Worry was recoded as 1 = “not at all true/a little bit”, 2 = “moderately,” and 3 = “quite a bit/extremely.”
Coronavirus threat and interrupted plans each had five items, each with a 5-point Likert-type scale response from 1 (“not at all”) to 5 (“a great deal”). The scale statement for threat asks, “Indicate how you feel about the COVID-19 virus” with items such as uncertain, at risk, and threatened. The scale statement for interrupted plans asks, “Indicate the extent to which your plans have been affected . . .” with items including travel, social events, and significant life events, that is, a graduation party. Summative scores for threat and interrupted plans were used for analysis. The possible range of scores for threat and interrupted plans is 5 to 25 with higher scores indicating more threat and interrupted plans.
Resource utilization refers to sources of support that were in place at the study site to address the psychological and emotional needs of the HCPs. Participants were asked “Which of the following support resources have you utilized? Check all that apply.” Resource utilization contains eight response items, each with two options (yes/no), including (a) Your Well-Being (offers employees resources for taking care of themselves, their team and family), (b) Show Me Hope hotline (Missouri’s crisis counseling program in response to COVID-19), (c) Employee Assistance Program (to help maximize employees physical and emotional well-being), (d) Talk With Us (national disaster distress helpline) (Substance Abuse and Mental Health Services Administration [SAMHSA], 2022, p. 5) WeCare (study site teams that provide care and support to employees “in the moment” and when adverse events occur), (e) Thrive (internal website with holistic focus on employee well-being; seeks to help team members thrive physically, emotionally and socially), (f) the study site resilience website (provides resources to help learn about building and strengthening resilience), and (g) none.
Data Analysis
Sociodemographic and health behavior information were analyzed using descriptive statistics. Continuous variables are reported as means and standard deviations. Categorical variables are reported as frequencies and percentages. Participants’ direct exposure to COVID-19 patients was defined as 1 = “No direct contact with COVID-19 patients,” 2 = “≤50% direct contact with COVID-19 patients,” 3 = “>50% direct contact with COVID-19 patients.” Differences in overall distress and the separate distress subscale scores (anxiety, anger, depression, and fatigue) across the three survey time points were first examined separately using ANOVA. Bivariate associations between overall distress, anxiety, depression, anger, fatigue, threat score, and interrupted plans score were examined using Pearson’s correlation coefficient. Bivariate associations between overall distress, anxiety, depression, anger, fatigue, direct exposure to COVID-19 patients, job type, remaining calm, and worry were examined using ANOVA. Multiple linear regression was used to examine the relationship between distress scores (overall, anxiety, depression, anger, and fatigue) and survey wave, direct exposure to COVID-19 patients, job type, remaining calm, worrier, threat score, and interrupted plans score. Data were analyzed using IBM SPSS Statistics (Version 25) and StataCorp Stata 18 Basic Edition. Statistical significance was set at 0.05.
Results
Participants
A total of 464 surveys were returned across the three time points with descriptive and behavioral characteristics presented in Table 1. The mean age of participants was 42.2 ± 12.6. 375 (81%) self-identified as Caucasian with most participants identifying as female (n = 393, 86%). Two hundred eighty (61%) of the participants were married. Two hundred forty-nine (54%) participants described their occupation as being a nurse (including advanced practice registered nurses [APRNs]) with an additional 8 (2%) stating their roles as student nurses or patient care technicians. Fifty-four (12%) of the participants were enrolled in an academic program. Overall, 419 (91%) were employed full-time, of which 411 (90%) stated they were not working from home. Although 153 (33%) of the participants had children who had not yet graduated from high school, only 15 (10%) were home-schooled or learning virtually. Some of the participants were caregivers to others, such as parents (n = 30, 67%) and spouses (n = 7, 16%). Four-hundred fifty (97%) participants noted that a car was the main source of transportation to get to work from one of the 69 unique neighboring zip codes.
Mean overall distress, anxiety, depression, and fatigue scores were not significantly different across survey time points. However, the mean anger score was significantly different across survey time point (15.5 ± 7.7 vs. 17.5 ± 7.0 vs. 16.3 ± 6.9, p = .046). There were no significant differences in mean overall distress, anxiety, depression, anger, or fatigue between nurses/physicians and nonnurses/physicians. Mean overall distress, anxiety, depression, and fatigue scores were significantly different across “remain calm” and “worrier”. Mean overall distress, depression, and anger scores were significantly different across direct contact with COVID-19 patients (p = .018, 0.001, and 0.031, respectively). In each survey wave, threat score and interrupted plans score were significantly correlated with overall distress, anxiety, depression, anger, and fatigue scores (results of bivariate analysis not displayed).
Multiple Linear Regression
To examine the relationship between distress and survey wave, direct exposure to COVID-19 patients, job type, remaining calm, worrier, threat score, and interrupted plans score, multiple linear regression was used for each score separately.
Table 2 summarizes the multiple linear regression model with the overall distress score as the dependent variable. The model was statistically significant (p < .001) and explained 42.6% of the variation in overall distress score. On average, overall distress score was significantly higher for those who had >50% direct contact with COVID-19 patients compared to those who had no direct contact (B = 6.46, p = .018), those who were “extremely/quite a bit” a worrier compared to “a little bit/not at all” (B = 9.66, p < .001), and significantly lower among those who reported “moderately true/exactly true” remaining calm compared to “hardly true/not at all true” (B = −11.34, p = .001). For every 1-point increase in threat score, the overall distress score increased by 1.97 (p < .001) on average. For every 1-point increase in the interrupted plans score, the overall distress score increased by 1.24 (p < .001).
Summary of Multiple Regression Model for Overall Distress Score
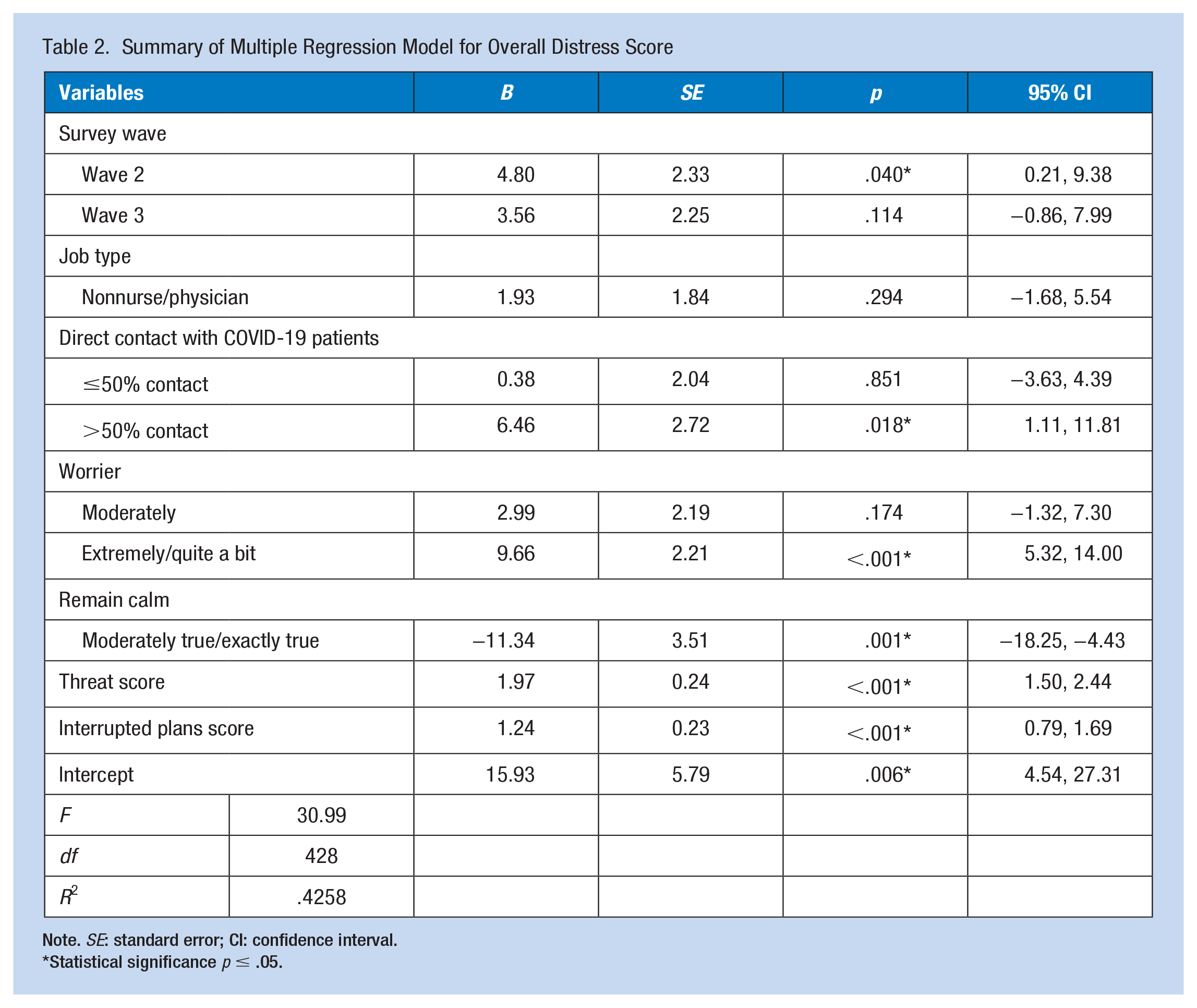
Note. SE: standard error; CI: confidence interval.
Statistical significance p ≤ .05.
Table 3 displays the multiple linear regression model with anxiety subscale score as the dependent variable. The model was statistically significant (p < .001) and explained 49.1% of the variation in anxiety score. The mean anxiety score was significantly higher for those who were “extremely/quite a bit” a worrier compared to “a little bit/not at all” (B = 2.44, p < .001), and significantly lower among those who reported “moderately true/exactly true” remaining calm compared to “hardly true/not at all true” (B = −2.82, p = .003). For every 1-point increase in threat score, anxiety score increased by 0.75 (p < .001) on average. For every 1-point increase in the interrupted plans score, the anxiety score increased by 0.31 (p < .001).
Summary of Multiple Regression Model for Anxiety Subscale Score
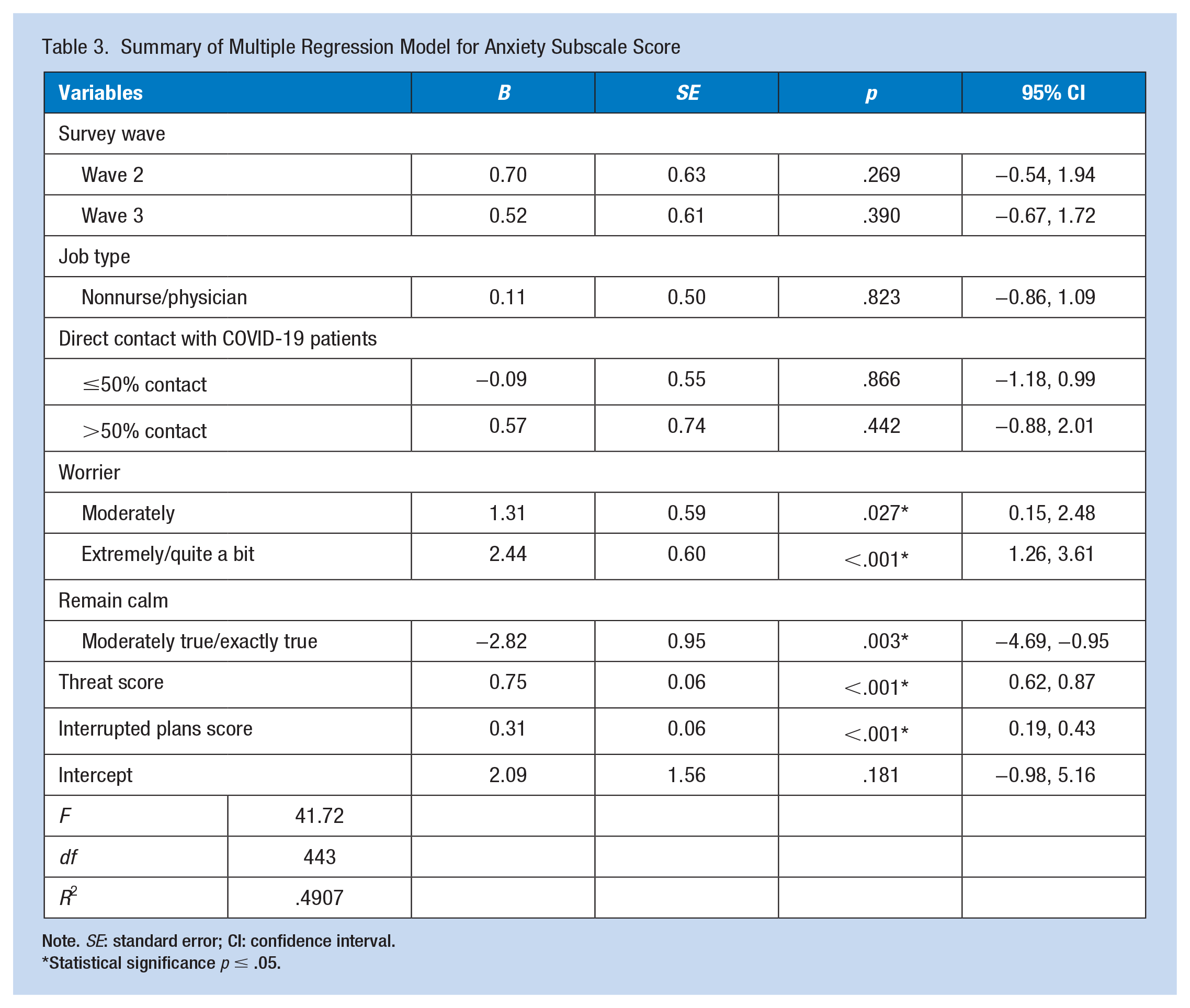
Note. SE: standard error; CI: confidence interval.
Statistical significance p ≤ .05.
Table 4 summarizes the multiple linear regression model with depression subscale score as the dependent variable. The model was statistically significant (p < .001) and explained 37.6% of the variation in depression score. Mean depression score was significantly higher for those who had >50% direct contact with COVID-19 patients compared to those who had no direct contact (B = 2.69, p = .004), who were “extremely/quite a bit” a worrier compared to “a little bit/not at all” (B = 3.11, p < .001), and significantly lower among those who reported “moderately true/exactly true” remaining calm compared to “hardly true/not at all true” (B = −3.52, p = .004). For every 1-point increase in threat score, depression score increased by 0.65 (p < .001) on average. For every 1-point increase in the interrupted plans score, depression score increased by 0.34 (p < .001).
Summary of Multiple Regression Model for Depression Subscale Score
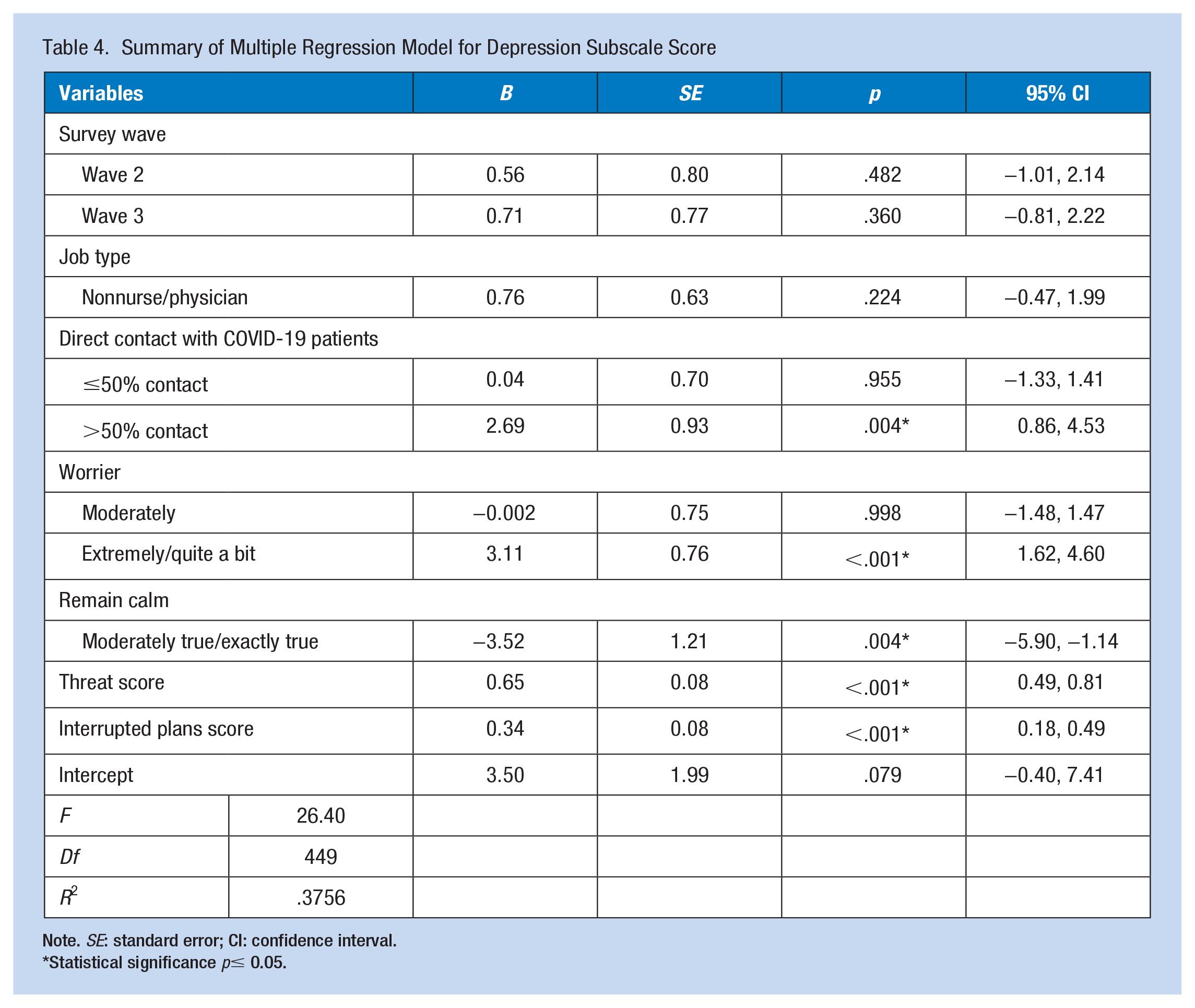
Note. SE: standard error; CI: confidence interval.
Statistical significance p≤ 0.05.
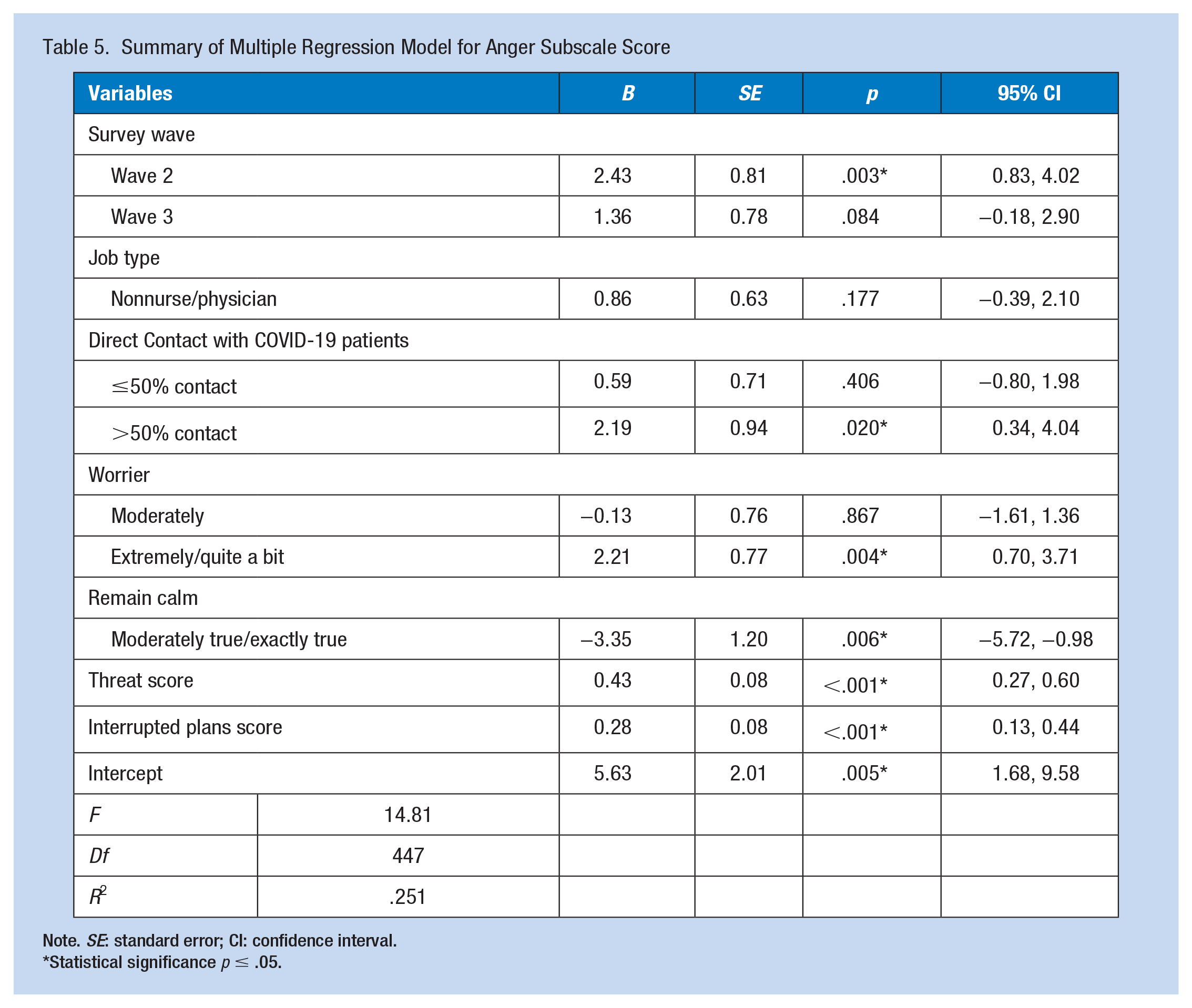
A summary of the multiple linear regression model with anger subscale score as the dependent variable is displayed in Table 5. The model was statistically significant (p < .001) and explained 25.1% of the variation in anger score. Mean anger score was significantly higher for those who had >50% direct contact with COVID-19 patients compared to those who had no direct contact (B = 2.19, p = .020), those who were “extremely/quite a bit” a worrier compared to “a little bit/not at all” (B = 2.21, p = .004), and significantly lower among those who reported “moderately true/exactly true” remaining calm compared to “hardly true/not at all true” (B = −3.35, p = .006). For every 1-point increase in threat score, anger score increased by 0.43 (p < .001) on average. For every 1-point increase in the interrupted plans score, the anger score increased by 0.28 (p < .001).
Summary of Multiple Regression Model for Anger Subscale Score
Note. SE: standard error; CI: confidence interval.
Statistical significance p ≤ .05.
A summary of the multiple linear regression model with fatigue subscale score as the dependent variable is displayed in Supplemental Table 1. The model was statistically significant (p < .001) and explained 26.3% (R2 = .263) of the variation in fatigue score. Mean fatigue score was significantly higher for participants in Wave 2 (B = 1.51, p = .008) and Wave 3 (B = 1.18, p = .032) compared to Wave 1, those who were “extremely/quite a bit” a worrier compared to “a little bit/not at all” (B = 1.73, p = .001). For every 1-point increase in threat score, the fatigue score increased by 0.27 (p < .001) on average. For every 1-point increase in the interrupted plans score, the fatigue score increased by 0.31 (p < .001).
Resource Utilization
Across survey time points, 42 (32.6%), 69 (43.4%), and 72 (40.9%) of team members, respectively, indicated that they used at least one resource. In Wave 1, the most used resource was Your Well Being (66.7%), followed by the Resilience Website (26.2%). In Wave 2, the most used resource was Your Well Being (76.8%), followed by the Employee Assistance Program (23.2%). In Wave 3, the most used resource was Your Well Being (65.3%), followed by the Employee Assistance Program (29.2%).
Discussion
This study aimed to understand the impact of COVID-19 on clinical and nonclinical HCPs in a Midwestern urban quaternary academic medical health center. RNs represent the largest share of employees in hospitals constituting 30% of all positions as of May 2019 (Bureau of Labor Statistics & U.S. Department of Labor, 2022). In the United States, 65% of RNs are Caucasian and female with an average age of 43 (Zippia, 2022) like the participant demographics of this study. Although this study sought to gain a wider respondent perspective by including nonclinical HCPs, most of the participants in this study were nurses.
The pandemic posed significant challenges to the staff’s occupational health. Social distancing is a way to reduce the staff’s reduce the spread of COVID-19; however, HCPs who provided health care to sick individuals had an increased risk of exposure (Betancourt-Sánchez et al., 2020). This study showed that HCPs with greater exposure to COVID-19 patients had significantly more distress, depression, and anger. Research from prior pandemics and COVID-19 suggests that various exposures related to the pandemic put HCPs at an increased risk of manifesting mental health problems compared to the public (Czepiel et al., 2022). Consistent across the decades, greater exposure to an outbreak or pandemic agent increases HCP distress. During the outbreak of SARS, less contact with SARS predicted lower levels of emotional exhaustion (p = .003) (Marjanovic et al., 2007). In addition, the risk of death and family exposure to SARS were key predictors of emotional distress among HCPs exposed to SARS (Nickell et al., 2004). During the early COVID-19 pandemic, healthcare systems across the United States were still facing unique issues such as lack of equipment and personal protective equipment, unfamiliar staffing patterns, and the fear of exposing friends and family to COVID-19 (Evanoff et al., 2020). The emotional toll and distress persisted for the second and third waves of this study which was 1.5 to 2 years from onset of the pandemic.
Psychological distress is defined as a set of painful mental and physical symptoms that are associated with normal fluctuations of mood in most people (BetterHelp, 2023). In some cases, this distress can be the start of a mental health disorder, such as depression, anxiety, or other mental health conditions (American Psychological Association, 2022). This study assessed these mood states along with anger (a response to distress) and fatigue (a physical symptom related to mental exhaustion) (Cooks-Campbell, 2022). There were no significant differences in distress between job types at each survey time point.
The COVID-19 pandemic created uncertainty and disruption on many levels. A normal healthy stress response can create a level of fear and anxiety. When levels are heightened, humans’ natural tendency is to shut down, tense up, and succumb to the “chaos” (Specialized Therapy, 2023). In this study, HCPs who responded they could remain calm reported significantly lower overall distress, anxiety, depression, and anger across all three waves. However, anger was statistically significant only in wave 2. At the time of the second wave, there was a new spike in COVID-19 cases after a return to the usual hospital activity (Pew Research Center, 2022). This may explain the spike in anger for wave 2. It should be noted that respondents were not asked the reason behind their anger.
Interrupted plans and a sense of threat were significant across all three waves. Both impacted overall distress and the components of anxiety, depression, anger, and fatigue. Life in the United States was interrupted by the arrival and threat of the COVID-19 pandemic. Social connection protects and promotes mental health, being an important clinical tool for reducing anxiety, depression, and stress (Soares et al., 2022). Social distancing during the pandemic meant many individuals would now conduct work and school from home and find alternative forms of socializing. Most participants in this study were frontline and essential workers; however, they experienced the impact of the pandemic on their social activities. The sense of threat presenting uncertainty, risk, and thinking about COVID-19 was on the minds of HCPs in this study. Recognizing that interrupted plans and threats had a persistent impact on distress among HCPs is an important finding and can be used to plan for ongoing resources, including opportunities for social interaction.
Although HCPs are trained to respond to crisis situations, there was a constant elevated level of crisis during the pandemic. Being able to remain calm under constant pressure not only has a calming effect on others but also inspires confidence (Overby, 2019). The ability to stay calm under pressure in health care could be the difference between life and death for a patient. Calming techniques can be learned; therefore, offering these techniques could assist with managing stress (Alpert, 2022). Ongoing training for crises will help staff remain calm (Flowerdew et al., 2012).
The definition of worry is described as mental distress or agitation resulting from concern -usually for something impending or anticipated (Merriam-Webster, 2023). HCPs in this study were asked whether they consider themselves to be a worrier. For all three waves, worry was a significant contributor to distress. Chronic and constant worry can cause issues with your body both physically and mentally (Mayo Clinic, 2023a). Even people who do not usually struggle with anxiety experienced more worry and anxiety during the pandemic (Anxiety Canada, 2023). Chronic worrying can affect one’s daily life to the extent of interfering with appetite, sleep, and job performance (WebMD, 2023). Fatigue was significant in wave 2 and was not impacted by the ability to remain calm or by increased exposure. Prolonged pandemics will lead to fatigue. Recognition that staff will need rest, designated uninterrupted breaks, limits in overtime, and encouragement of use of time off might be strategies to decrease fatigue (Cooks-Cambell, 2022; Kester et al., 2021). Occupational health nurses can help HCPs overcome physical, mental, and emotional challenges related to extreme worry and fatigue experienced in the health care setting.
At the study site, a wide range of resources are accessible on demand that require the staff to visit the intranet site. The dedicated site contains COVID-19 information and links to various resources. The resource accessed most across all waves was “Your Well-Being” which provides self-help topics on “taking care of me,” “taking care of my team,” and “taking care of my family.” Reasons for utilizing the different resources were not assessed in this study. Many HCPs chose not to access resources despite knowledge of their existence. A consequence of not attending to mental, emotional, and physical well-being, is compassion fatigue (CF). This can occur when HCPs take on patient’s suffering such as extreme stress, trauma, or COVID-19 (American Psychological Association, 2022). Components of CF include burnout and secondary traumatic stress associated with excessive work and minimal resources (American Psychological Association, 2022). Website analytics and insights can be used by occupational health to determine which topics are accessed most frequently and offer additional self-service resources. Provision of self-service resources is helpful; however, integrating self-care opportunities into the workday is essential to HCP well-being. Occupational health practitioners add value to workplace well-being initiatives in the health care setting by building multimodal programs with a variety of activities which include on-unit, off-site, and online options (Daniels et al., 2019; Mayo Clinic, 2023b).
There were several limitations of this study. Enrollment of nonclinical HCPs was less than expected in the first survey due to the inability to directly email HCPs and having to rely on posters and flier distribution in common areas. Throughout the pandemic, many nonclinical staff members worked offsite limiting their exposure to recruitment fliers and posters. In waves 2 and 3, recruitment expanded to include HCPs who opted in to receive the internal newsletter via email. With the addition of posting the study in the institutional newsletter, nonclinical HCP respondents increased. Given the study site had 8,802 employees in 2021 and recruiting methods were revised after Wave 1, we do not expect there to be a significant overlap of survey participants across time points. The normality of scores was assumed due to sample size. Generalizability may be limited due to the demographic makeup of participants, nonetheless, insight into the experiences of HCPs during the COVID-19 pandemic is valuable. We did not find any difference in response based on job type. This study did not follow participants over time, so we cannot make any inference about changes over time. By design, the survey was meant to be a pulse check at each given time.
The impact of COVID-19 on HCPs is not a singular set of responses to a particular event. Coronavirus is everchanging with new variants, symptomology, and treatments. Findings from this study provide insight into various facets of HCPs experience of a novel virus. Staff with greater exposure to COVID-19 had greater distress overall, and self-service resources were not well utilized. The ability to remain calm was protective against distress. Staff who described themselves as a worrier showed higher distress scores including all subscales of anxiety, depression, anger, and fatigue in all three surveys even 2 years from the start of the pandemic. The sense of threat and interrupted plans significantly impacted distress, anxiety, depression, anger, and fatigue. Globally, pandemics will be an ongoing part of health care. While the pandemic agent may change, findings of increased distress in HCPs should be an impetus for appropriate development and implementation of self-help resources by healthcare leadership. Future studies should be conducted exploring how to improve clinical and nonclinical staff utilization of employee resources and what helps mitigate distress. In addition, following participants over time would add insight.
Implications for Occupational Health
Occupational health is dedicated to the safety and well-being of HCPs in an organization. Occupational hazards include exposure to COVID-19 and prolonged use of personal protective equipment (World Health Organization [WHO], 2020). Occupational health staff are in a key position to evaluate the impact of a pandemic on HCPs and can become important advocates for maintaining their mental and physical health. Pandemic-related examples include evaluating unit mental health resources and education on calming strategies. Screening for mental health wellness in all staff is imperative to maintaining a healthy workforce. The mental health impact on HCPs will most likely persist beyond the end of the pandemic. Addressing these impacts can help build a stronger and more resilient health care system for the future (Assistant Secretary for Planning and Evaluation [ASPE], 2022).
Future pandemics will occur, thus understanding the impact of this pandemic on HCPs can guide future responses to maintain a healthy workforce. COVID-19 must be managed the same way as any workplace health and safety threat. Organizational change is necessary to improve the health of HCPs in future pandemics. Occupational health is a key stakeholder in designing and evaluating necessary changes to improve the physical and mental health of HCPs enduring and recovering from a crisis such as a worldwide pandemic. Occupational Safety and Health Administration (OSHA, 2023) launched a website to address workplace stress and mental health which states “. . . workplaces can be a key place for resources, solutions and activities designed to improve our mental health and well-being.”
Applying Research to Occupational Health Practice
This study surveyed clinical and nonclinical healthcare professionals (HCPs) beginning a year after the onset of the COVID-19 pandemic to determine the impact of COVID-19 on HCPs. There were no significant differences in distress between job type at each survey time point. Study findings indicated HCPs with greater contact to COVID-19 experienced more distress, anger, and fatigue. Interrupted plans, threat, and worry impacted overall distress. The ability to remain calm decreased HCP distress. Understanding how a pandemic impacts all HCPs will help occupational health practitioners (OHPs) identify ways to improve mental and emotional health of HCPs. OHPs can develop personal and organizational interventions to address study findings, including stress reduction techniques, fatigue management, and strategies to control anger. They can help mitigate HCP feelings of threat and worry by providing continuous pandemic-related health and safety resources. Proactive engagement with HCPs will strengthen the workforce and improve the well-being of HCPs
Supplemental Material
sj-docx-1-whs-10.1177_21650799241260604 – Supplemental material for Impact of COVID-19 on Healthcare Professionals at a Midwestern Quaternary Academic Urban Health Center
Supplemental material, sj-docx-1-whs-10.1177_21650799241260604 for Impact of COVID-19 on Healthcare Professionals at a Midwestern Quaternary Academic Urban Health Center by Jennifer A. Sledge, Donna Prentice and Cassandra Arroyo in Workplace Health & Safety
Footnotes
Acknowledgements
The authors would like to thank Becky Meyer, PhD, RN, NDP-BC for useful comments on and for editing a draft of this manuscript. The authors would like to thank the participants as well as all health care professionals for their service.
Author Contributions
J.A.S., D.P. and C.A. contributed to the design and implementation of the research, to the analysis of the results and to the writing of the manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics
This study was given Institutional Review Board approval from the Washington University Human Research Protection Office #202101139
Data Availability Statement
The data that support the findings of this study are available from
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.