
Abstract
Background:
Recent research suggests a need for worksite programs that promote structured physical activity (PA) among hospital staff. The objectives of this study were to assess the hospital employees’ acceptance of PA opportunities that could be implemented at the worksite, and the association between worksite PA and commuting and other sociocognitive factors.
Method:
Acceptance of seven PA opportunities from the WHO guidelines was correlated with commuting and socio-cognitive factors through an online survey conducted among the workforce of the University Hospital of Angers, France (N = 6874) between April 25 and May 22, 2022.
Results:
Only three PA opportunities in the seven proposed reached high approval rates among at least 50% of the 1,427 participants, namely, provide cycle facilities onsite, create a fitness room onsite, and establish partnerships with private associations or sports clubs, albeit rates decreased significantly with commuting distance for the first and the last proposals. The number of approved PA opportunities was positively related to the perceived negative influence of commuting on well-being and self-rated concerns with current PA level. It was negatively related to older age, long commuting, and flexible rest days.
Conclusion:
Based on these results, we recommend raising PA awareness and self-efficacy before implementing an easily accessible fitness center for employees. Providing cycle facilities and a more walkable environment in the hospital setting while encouraging active traveling between home and work for short commuters could additionally increase the level of physical activity on an equitable and sustainable basis.
Keywords
Background
Physical inactivity has been widely reported in healthcare workers (Alyafei et al., 2023; Younis et al., 2023). High levels of occupational stress resulting from heavy workloads, extended working hours, and high levels of time pressure tend to jeopardize healthy lifestyle behaviors and increase the risk of musculoskeletal conditions (Zhang et al., 2020). Barriers to health-promoting self-care in registered nurses include lack of time/overwork, lack of resources/facilities, fatigue, outside commitments, supportive versus unsupportive individuals, and positive versus negative role models (Ross et al., 2019). These problems may be aggravated in employees living far away from work, as lengthy commuting time increases the risk of physical inactivity and sleep problems if individuals have longer than normal weekly working hours (Halonen et al., 2020).
In response to these problems, the World Health Organization (WHO) initiated the Health Promoting Hospitals Project, which aims to reorient hospitals into health-promoting environments, with active community participation (Pelikan et al., 2001). More recently, the Dr. Lorna Breen Health Care Provider Protection Act (H.R.1667) has been introduced and passed by the House and Senate to reduce behavioral health conditions among healthcare professionals in the United States (“Dr. Lorna Breen Health Care Provider Protection Act,” 2022). Several research findings have emphasized the need for worksite health promotion programs (WHPP) to foster physical activity (PA) among employees (Pronk, 2021; Shimo et al., 2021). According to the WHO Regional Office for Europe, PA opportunities that have the potential to transform the work environment to foster active lifestyles include creating onsite fitness facilities, giving easy access to walking/running routes, offering reduced-fee fitness or recreation center memberships to employees; and promoting participation to sporting events (WHO, 2000). Apart from increased PA and improved physical fitness (Henriques-Neto et al., 2020), walking or cycling to work is perceived as more relaxing and exciting than commuting by car or public transport, which is reported as being more stressful and boring (Chatterjee et al., 2020). Fostering active commuting is therefore increasingly recommended as well (Herman & Larouche, 2021).
One of the key motivations for WHPP is the potential to reach a high percentage of people and to modify the health of employees who would be unlikely to participate in preventive health behaviors (Hogsbro et al., 2018), but participation levels are often limited (Lier et al., 2019; Tsai et al., 2019). Employees may differ in their personal profile, beliefs about health, and awareness of health behaviors, all of which shape their acceptance of the intervention, which in turn may affect participation (CDC, 2018; Kaveh et al., 2020; Rossi et al., 2022). The degree to which an intervention is appraised as easy to apply and adhere to in daily life is also pivotal (Safi et al., 2022; Sekhon et al., 2017). For instance, distance between home and workplace constitutes a barrier not only to active commuting (Aranda-Balboa et al., 2021) but also to other health behaviors, as many nurses spoke of commutes in excess of 1 hr that, coupled with shifts, left little time for exercising (Ross et al., 2019; Safi et al., 2022). To design and implement effective WHPP, it is imperative beforehand to use a multifaceted approach taking into account the complex factors influencing employees’ acceptance of PA opportunities.
Amid the deleterious impact of the COVID-19 crisis on employees’ health and well-being, the Angers University Hospital (AUH) authorities proposed the introduction of a WHPP designed to foster employees’ healthy lifestyles including (but not limited to) PA. The proposed plan sets out a considerable agenda for action that will have to meet with the approval and majority support of the hospital staff. To date, however, few studies have examined employees’ acceptance of PA opportunities in hospitals. The objectives of this study were to assess the hospital employees’ acceptance of PA opportunities that could be implemented at the worksite, and its associations with commuting and socio-cognitive factors.
Method
Participants and Procedures
To meet the study’s objectives, we conducted a cross-sectional study among the Angers Hospital staff to assess their opinions on several PA opportunities that could be implemented at the worksite. An online survey was conducted between April 25 and May 22, 2022, at the University Hospital of Angers (AUH), in France. This 1,729-bed University Hospital with a clinical and non-clinical workforce of 6874 provides health care to nearly 200,000 patients a year. The 89-acre main campus is located within cycling distance of the center of town and comprises facilities devoted to health care, administration, research, and logistics. The survey was advertised through meetings in all AUH departments, followed by email dissemination, posters, and word of mouth. Written study information was provided to the participants and their electronic consent was obtained prior to commencement. The survey was anonymous. The participants were both clinical staff, including medical, nursing, and allied health, and non-clinical staff including administrative, management, logistics, and research personnel. All AUH staff working during this time and willing to complete the survey met the inclusion criteria.
Measurements
Participants were presented with seven PA opportunities from the WHO guidelines (WHO, 2000), which might reasonably be implemented at AUH in the coming years: (a) provide cycle facilities (additional garages, pumps, etc.); (b) establish partnerships with associations or sports clubs; (c) create a fitness room at the worksite; (d) establish partnerships with fitness rooms; (e) create a pedestrian health trail at the worksite; (f) organize and/or foster participation in sporting events; and (g) communicate on staff achieving significant sports performance in sports events. The participants were asked to rate how much they agree or disagree with each proposed opportunity on a Likert-type response scale. The response options were ranked from 1 to 6, with the following description: strongly disagree = 1, disagree =2; rather disagree=3; rather agree=4; agree=5; strongly agree= 6. To obtain conservative estimates, we considered that respondents approved a given measure if they responded, “agree” or “strongly agree” to the question. To facilitate the treatment of the data, approvals obtained from each measure were added to generate a cumulative score ranging from 0 to 7 that enabled the research team to assess the number of approved PA opportunities.
Commuting characteristics: Commuting distance (in kilometers) and perceived influence of commuting on well-being (none, positive, negative) were assessed, together with active commuting. The term “active commuting” referred to those modes of travel to and from work, which involved PA (walking and cycling). According to this definition, active commuting can involve commuting solely by walking or cycling. Walking or cycling in combination with passive commuting (e.g., a combination of car with walking, or of train with cycling) is considered “mixed” commuting. The term “short commuters” referred to participants with a commuting distance ≤ 5 km, while others are labeled “long commuters” in this study.
Socio-cognitive factors: Participants self-rated their health by answering the question: “In general, how would you rate your health?” and their physical condition by answering: “In general, how would you rate your physical condition?.” The response options were ranked from 1 to 6, with the following description: very poor =1, poor = 2; rather poor = 3; rather good = 4; good = 5; very good = 6. They also self-rated their PA frequency (1 = never; 2 = sometimes; 3 = often; 4 = every day), and how much they were concerned with their current PA level by answering the following question: “In general, how much are you concerned with your level of PA ?” The response options were ranked from 1 to 6, with the following description: not concerned at all = 1, unconcerned = 2; unconcerned = 3; rather concerned = 4; concerned = 5; very concerned = 6. Sociodemographic variables such as age in years (18-34; 35-44; 45-54; 55 and older), gender (male/female), occupational status (medical; paramedical; non-clinical staff), and professional constraints such as having duty periods (e.g., on duty doctors attending emergency cases outside regular work schedule) and flexible rest days (i.e., having to work on Sunday and holidays at least 10 days per year) were also collected.
Statistical Analyses
Categorical data were expressed as numbers and percentages, whereas ordinal data were expressed as medians and interquartile ranges (IQRs). The chi-square test was used to compare categorical data at the baseline. The Kuder-Richardson Formula and the Cronbach alpha test were used to assess the reliability of the cumulative score by assessing the number of approved PA opportunities (Foster, 2021). As this study’s outcome was a count variable, we used a generalized Poisson regression model to estimate the strength of the association between the number of approved PA opportunities and each covariate (univariate analysis). To determine variables independently associated with the outcome, all variables that demonstrated an association with p < .05 in the univariate analysis were considered candidate variables in the multivariate model. The goodness of fit of the multivariate model was assessed using the Value/df for the Deviance statistics. Statistical analyses were performed using the SPSS statistical package, version 19 (SPSS, Chicago, Illinois, United States).
The research protocol met the General Data Protection Regulation criteria and was approved by the hospital ethical board (Comité d’éthique du CHU d’Angers; decision # 2022-082).
Results
Participants
Among the 6,874 persons working at the Angers University Hospital, 1,425 completed the survey, corresponding to a participation rate of 20.7%. The study sample comprised 43.2% of non-clinical staff (administration, management, technical services. . .) and 22.7% of medical personnel while they account for 18.1 % and 34.9 % of the workforce, respectively. Conversely, paramedical staff accounted for 34.0% of the study sample while representing 47.0% of the workforce. Based on these estimates, weights were applied for the weighted study sample to matches the population distribution (Weighted N = 1,427).
The majority of the participants (Table 1) were women (80.3%), aged between 18 and 44 years (63.7%), and were long (69.3%) and passive commuters (61.9%). A majority of participants reported a positive influence of commuting on well-being (52.8%) as well as exercising often (37.1%) or almost every day (17.3%). On average, participants rated their health and their physical condition as “rather good” (medians = 4, IQR [4-5]), and reported being “rather concerned” with their current level of PA (median = 4, IQR [4-5]). Only 31.2% of participants had duty periods (weighted N = 445) and 34.6% of them had flexible rest days (weighted N = 494).
Participants’ Characteristics, Weighted Estimates (N = 1,427)
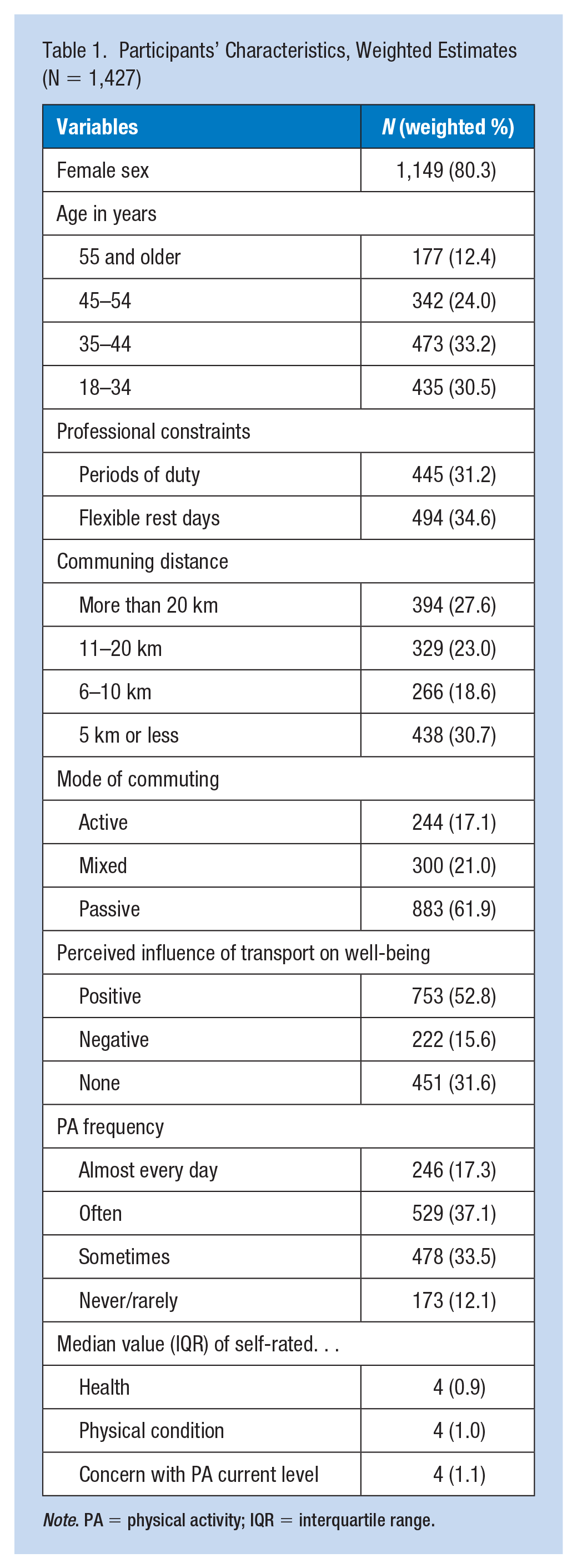
Note. PA = physical activity; IQR = interquartile range.
Three in seven proposed PA opportunities reached high approval rates among at least 50% (n = 714) of participants (Table 2), with the highest ratings for proposed #1 (Provide cycle facilities onsite), proposed #2 (Create a fitness center onsite), and proposed #3 (Establish partnerships with associations or sports club). The proposed #4 (Establish partnerships with private fitness rooms) reached a high approval rate in nearly half of the participants, while proposed #5 (Creating a pedestrian health trail onsite), proposed #6 (Organizing and/or foster participation to sporting events), and proposed #7 (Communicate on staff achieving significant sports performance) reached approval rates in a minority of participants. However, rates decreased significantly (p < .001) according to the commuting distance for proposed #1, proposed # 2, proposed #4, and proposed #6. Approvals for each PA opportunity were added to generate a cumulative acceptance score ranging from 0 to 7, with a satisfactory reliability coefficient according to the Kuder-Richardson Formula and the Cronbach alpha test (α = .73). On average, participants approved three in seven proposed PA opportunities (median = 3, IQR [1-5]).
Number and Percentage (%) of Participants With Highest Approval Rates for Each Proposed PA Opportunity According to Commuting Distance, Weighted Estimates (N = 1,427)
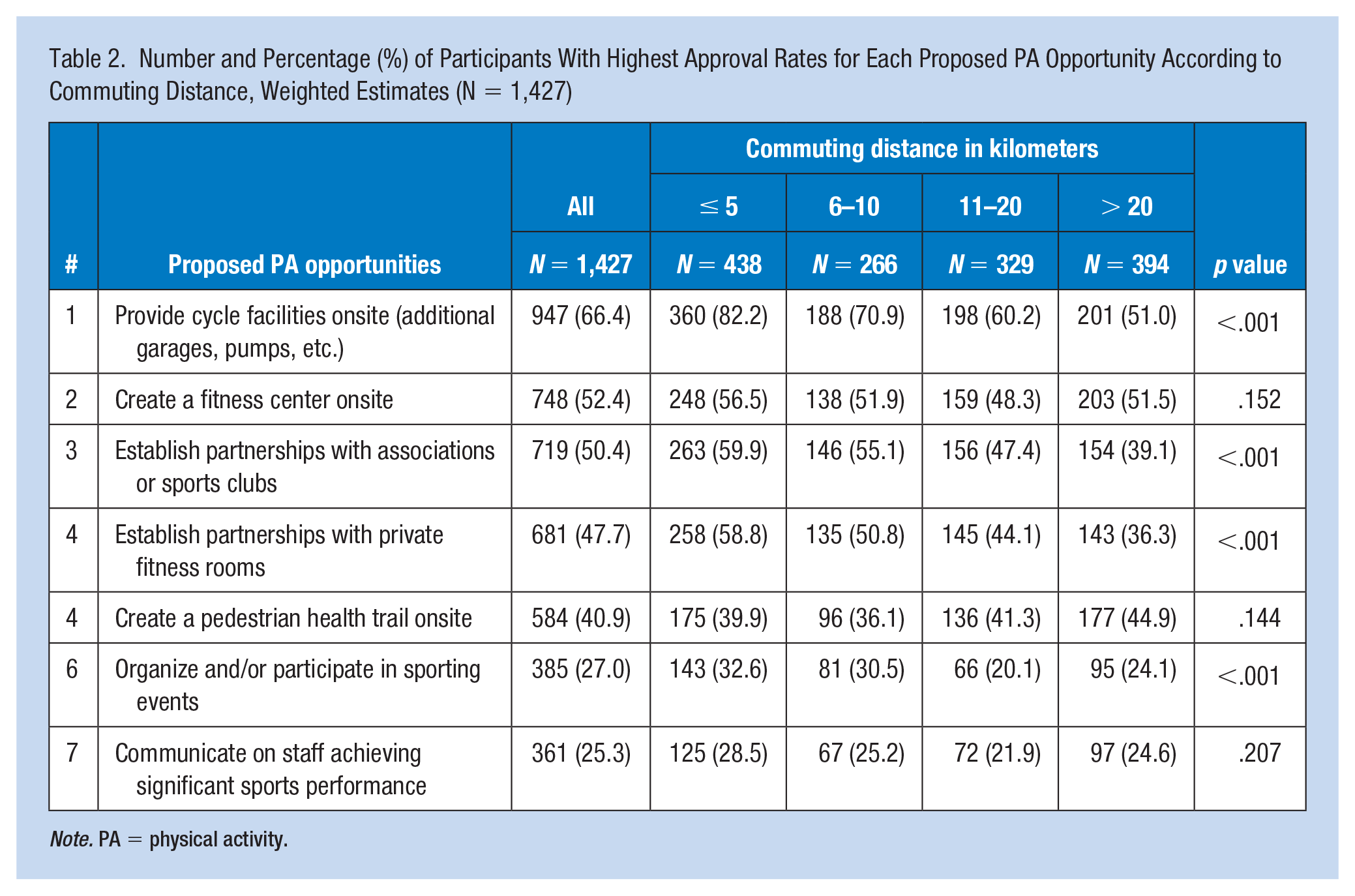
Note. PA = physical activity.
In the univariate analysis (Table 3), the number of approved PA opportunities was positively related to active communing, to PA frequency, to perceived commuting influence on well-being (either positively or negatively), and to self-rated health, physical condition, and concern with current PA level. It was negatively related to older age, long commuting, and flexible rest days. In the multivariate analysis (Table 3), the number of approved PA opportunities was positively related to the perceived negative influence of commuting on well-being and self-rated concerns with current PA level. It was negatively related to older age, long commuting, and flexible rest days.
Rates Ratios (RR) and Confidence Intervals (95% CI) of the Number of Approved PA Opportunities, Weighted Estimates
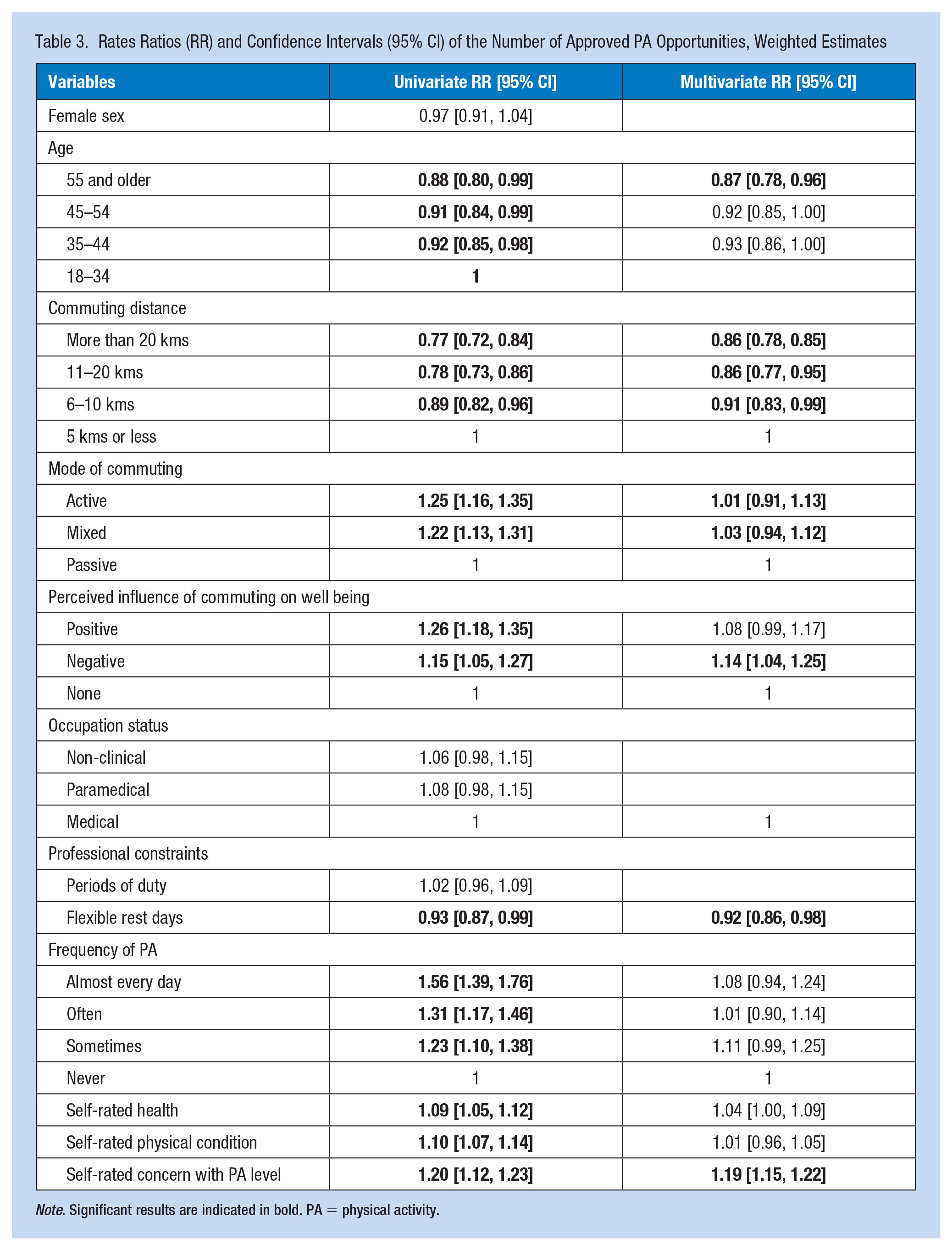
Note. Significant results are indicated in bold. PA = physical activity.
Discussion
Only three PA opportunities in the seven proposed reached high approval rates among at least 50% of participants, namely, provide cycle facilities onsite, create a fitness room onsite, and establish partnerships with private associations or sports club, albeit rates decreased significantly with commuting distance for the first and the last proposed PA opportunities. The number of approved PA opportunities varied according to age, commuting, and socio-cognitive factors.
Data were collected after the third lockdown in France, in a period when COVID-19 cases and deaths were minimal. However, the pandemic jeopardized healthy lifestyles in whole segments of the population (Constant et al., 2020), and had a detrimental impact on hospital workers’ mental health (Fournier et al., 2022). In such a context, the implementation of a WHPP should have been of interest to the entire AUH workforce. But only 20% of employees responded to the survey, with paramedical staff being particularly underrepresented. Previous studies highlighted that the low level of nurses’ involvement in health policy is common because most participants, besides their roles in workplace, had family obligations making them allocate little time for health policies activities. Lack of mentoring by nursing leaders could also negatively affect their involvement in policies development (Hajizadeh et al., 2021), highlighting the need for WHPP to gain support from nurse leaders and intermediate-level management. Conversely, the administration/management staff participated massively in the study, as these employees generally work in a sitting position for much of the day, putting them at risk of musculoskeletal conditions (Putsa et al., 2022). Of note, these participation rates by occupation are consistent with other findings (Chiou et al., 2014).
Most participants were passive and long commuters yet reported positive or no influence of commuting on well-being. Providing cycling facilities onsite was nevertheless the most popular proposed PA opportunity. While commuting distance constitutes an important barrier to cycling, most long commuters still approve this measure. One possible explanation is that increasing the number of cyclists coming to work could reduce traffic jam around and within the hospital setting (Hamilton & Wichman, 2018) and therefore benefit long commuters coming by car. Participants were for the most part physically active but self-rated their health and physical condition as “average.” They could therefore benefit from easy access to PA facilities, which can lower perceptions of inadequate time as a constraint to participation (Safi et al., 2022). In this study, however, partnerships with associations, sports clubs, or private fitness room were less popular among long commuters, as these structures could be located far from living residences. Conversely, most employees approved a fitness center onsite, with similar rates among short and long commuters. A qualitative study indicated that fitness centers are described as easily accessible and comfortable place for PA, and some female participants emphasized the feeling of safety compared with outdoor activity (Riseth et al., 2019). More walkable environments at the hospital could however be relevant to help employees be active through recreational walking (Marquet et al., 2020) and could benefit patients and visitors from all social backgrounds (Christie et al., 2022). Only a sizable minority of participants approved this PA opportunity but with similar rates among short and long commuters. Finally, involving employees in team sports events and communicating on sports performances were the least popular proposed PA opportunities, probably because of the high proportion of women among participants. For instance, a study conducted in adults showed that PA opportunities for women may be more appealing if they are for women only, supervised, and done at a fixed time, while men are attracted to PA opportunities that have a degree of competition, are vigorous, skill-based, and outdoors (van Uffelen et al., 2017). In the present study, ancillary analyses showed that the approval rate of team sport events decreased with age (odds ration [OR] = 0.82 [0.73, 0.93]) and was lower in women as compared with men (OR = 0.60 [0.46, 0.79]). Considering the high proportion of women in the healthcare sector (Eurostat, 2021), taking into account their expectations in the design of WHPP seems pivotal to optimize participation.
In multivariate analysis, the number of approved PA opportunities was higher in participants concerned with their current level of PA, indicating that acceptance is higher among employees who were already aware of physical activity (Martins et al., 2021). The first step of the WHPP should therefore be to make people aware of the PA benefits, for instance in terms of quality of life, physical function, and independence (Lechner et al., 2006). Expectedly, the number of approved PA opportunities was lower in long commuters, but also in those aged 54 years of age or older, and with flexible rest days. Increased middle management support for engaging in PA and having flexibility during working days could therefore possibly increase motivation for PA (Kaveh et al., 2020; Safi et al., 2022). Other indicators of occupational constraints (occupation status; duty periods) were unrelated to acceptance rates.
The results of this study must be viewed in light of its main limitations. First, the cross-sectional design does not allow causal inferences about relationships between variables to be determined. Second, time limits and psychological variables such as lack of confidence in being active, intrinsic motivation, and reasons for practice such as enjoyment, challenge, and affiliation were not assessed. Finally, a low proportion of the paramedical staff answered the survey, which may limit the generalizability of our results. The large size of our cohort and the inclusion of diverse professions nevertheless have offered an interesting opportunity to assess the acceptance of WHPP and select beforehand the most appropriate PA opportunities to be implemented.
Implications for Occupational Health
Changes in social and physical worksite environment designed to foster active lifestyles among hospital staff should gain support from the entire workforce, especially long commuters, aged employees, and women. Based on these results, we recommend raising PA awareness and self-efficacy before implementing an easily accessible fitness center for employees. Providing cycle facilities and a more walkable environment in the hospital setting while encouraging active traveling between home and work for short commuters could additionally increase the level of physical activity on an equitable and sustainable basis.
Applying Research to Occupational Health Practice
While initiatives such as The Health Promoting Hospitals Project and the Dr. Lorna Breen Health Care Provider Protection Act encourage nurses and other healthcare providers to take care of their body, programs promoting physical activity (PA) at hospitals must meet with approval and receive the support of the majority of employees to foster participation. Considering the employee perceptions, sociodemographic and commuting characteristics allowed the selection of a limited number of PA opportunities to be implemented, namely, provide cycle facilities onsite, create a fitness room onsite, and establish partnerships with private associations or sports club, albeit approval rates decreased significantly with commuting distance for the first and the last proposed PA opportunities. The number of approved PA opportunities was higher in participants concerned with their current level of PA, indicating that acceptance is higher among employees who were already aware of physical activity. The first steps of the worksite programs should therefore be to make people aware of the PA benefits, increase self-efficacy, and middle management support for engaging in PA.
Footnotes
Acknowledgements
Authors with to express their gratitude to Mrs Jaglin-Grimonprez, and Dr Aurore Armand, for their support.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics
The research protocol met the General Data Protection Regulation criteria and was approved by the hospital ethic committee (# 2022-082).