
Abstract
Background:
Peer-support specialists—individuals with diagnosed mental illnesses who provide support services to other adults with diagnosed mental health issues—often feel stigmatized and undervalued at work, leading to negative personal- and job-related outcomes. Given their important link to positive service user outcomes, this study assessed how peer-support specialists perceive fairness and feel valued in the workplace.
Methods:
Peer-support specialists (N = 274) were recruited online from peer-support specialist listservs, social media groups, and patient-run organizations to take a cross-sectional survey that included a 14-item scale on how workplace fairness relates to job satisfaction and four questions on how valued they felt by administrators, clinicians, the people they serve, and fellow peer-support specialists. Descriptive and bivariate statistics were used to assess total scores and differences by gender and race.
Findings:
Ranging in age from 20 to 77 years and identifying predominantly as White (81.0%) and female (62.9%), respondents noted that fair practices in the workplace would increase their job satisfaction, with no significant differences observed by gender or race. Most peer-support specialists felt valued by the people they serve (97.1%) and fellow peer-support specialists (92.7%). However, fewer reported feeling valued by administrators (64.6%) and clinicians (60.6%).
Conclusions/Application to Practice:
Peer-support specialists value fairness at the workplace and feel undervalued by some staff. This study highlights peer-support specialists’ important role in behavioral health services and suggests that healthcare professionals, including occupational health specialists, are important stakeholders in creating fairer workplaces and increasing peer-support specialists’ sense of being valued, leading to improved personal and organizational outcomes.
Keywords
Background
The Substance Abuse and Mental Health Services Administration (SAMHSA, 2017) has classified the peer support of individuals with psychiatric disorders as a critical component of mental health services. This is important, as rates of serious mental illness among U.S.-based adults have been increasing over the past decade with more than 1 in 20 adults experiencing a serious mental illness in 2020 alone (SAMHSA, 2021). Certified peer-support specialists are individuals who have a diagnosed mental illness and provide support services to other adults with diagnosed mental health issues, often in tandem with formal behavioral health services (Chinman et al., 2014; Fortuna et al., 2019). They focus on long-term recovery and build on the strengths and goals of service users to support individualized treatment plans (SAMHSA, 2017). In at least 40 states, these services are Medicaid reimbursable (Kaiser Family Foundation [KFF], 2023), although states also may use state or grant funding to offer peer-support services outside of Medicaid (Government Accountability Office, 2020).
Peer-support specialists represent one of the most rapidly growing mental health workforces in the country (Mental Health America, 2017), and while their services are generally offered throughout the United States, they are more common in densely populated areas (Videka et al., 2019). Currently, there are an estimated 30,000 peer-support specialists in the United States working in both clinical (e.g., community mental health centers, inpatient facilities) and non-clinical (e.g., homes, peer-run organizations) settings (Government Accountability Office, 2020). While this article focuses on the United States, comparable peer-support programs exist throughout the world within high-, middle-, and low-income countries at various levels of integration within the provision of mental health services (Krumm et al., 2022; Puschner, 2018).
A central tenet of peer support is collaboration with service users. Peer-support specialists work together with service users to identify their unmet needs, offer lived experience expertise from their own recovery process, and foster empowerment through self-determination, with service users taking an active role in determining their own trajectory (Chinman et al., 2014; Fortuna et al., 2019; Solomon, 2004). Previous studies have uncovered a number of benefits, including decreased social isolation, improved communication with non-peer providers, and reduced inpatient service use (Chinman et al., 2014; Fortuna et al., 2019; Salzar et al., 2010). Furthermore, service users report increased engagement in self-care, sense of control over their own lives, and feeling that their needs are being adequately taken into consideration and responded to over the course of their treatment when working with peer-support specialists (Davidson et al., 2012).
Despite these benefits to service users, organizational dynamics can lead peer-support specialists to feel stigmatized, undervalued, or excluded, ultimately leading to dissatisfaction and impacting retention (Almeida et al., 2020; Jones et al., 2019). A recent study of peer-support specialists found that they experienced both overt stigmatization (e.g., negative treatment toward people with a mental illness) and microaggressions (e.g., negative messages about peer support) in the workplace related to their role and diagnostic status and did not feel valued by clinical teams (Firmin et al., 2019). Participants reported that these macroaggressions and microaggressions had a negative impact on their personal well-being, job satisfaction, and willingness to remain in the workplace, with these experiences also indicating to peer-support specialists that they are not valued at the workplace (Firmin et al., 2019). Less-perceived workplace fairness was also associated with more exhaustion among peer-support specialists (Ostrow et al., 2022).
Perceptions of feeling valued at the workplace and fairness within the workplace can significantly impact individual (e.g., mental health, satisfaction with life) and organizational (e.g., sense of inclusion, turnover intention) outcomes; more so, these perceptions can differ by demographic groups, such as gender, race, and ethnicity, reflecting organizational and societal issues related to diversity, equity, and inclusion (Halvorsen et al., 2020). Given that the lack of feeling valued and a sense of unfairness at work is linked to negative personal and workplace outcomes for peer-support specialists (Firmin et al., 2019; Ostrow et al., 2022), it is important to understand the experiences of this understudied class of worker. In response, the aim of this study was to explore how attributes of fairness at the workplace are related to job satisfaction among peer-support specialists as well as their perception of being valued by fellow healthcare staff and service users.
Methods
Overall Approach and Participant Selection
This study utilized a cross-sectional online survey that was hosted on Qualtrics from September to November 2020. Participants were recruited through three online newsletter announcements sent out over a 4-week period through the last author’s peer-support specialist listserv, which included email addresses from 1,500 peer-support specialists. The newsletter included a link to the informed consent text and the online survey. This information was also sent out via popular peer-support media outlets on Facebook as well as on Twitter.
Status as a peer-support specialist was self-reported by participants, who needed to have a diagnosed mental health issue, be currently in recovery, and be providing Medicaid-reimbursable services to other adults with a diagnosed mental health issue. No incentive was provided for participation to limit false reporting of job status. Dartmouth College’s Institutional Review Board granted approval for this study, and informed consent was obtained before participants were shown the survey.
Data Collection
Participants (N = 274) answered a 14-item workplace fairness scale (WFS, α = 0.93; Halvorsen et al., 2020) and four questions on how valued they felt by fellow healthcare staff in their jobs. The WFS, designed to be answered by employees to measure the perceived organizational justice of jobs and workplaces, was adapted for this study by including the “peer-support specialist” term in the instrument language. Each item provided a situation related to fair practices at work and asked peer-support specialists to rate on a scale of one to seven how much these practices would increase their overall job satisfaction. For example, “Peer-support specialists’ opinions about how decisions are made in the organization would be considered” with 1 = “would not increase job satisfaction at all” and 7 = “would increase job satisfaction to a great extent” (see Supplemental Material 1 for the full adapted WFS). Answering “yes” or “no,” participants also reported if their life and work experiences were valued at the workplace by fellow peer-support specialists, clinicians (non-peers), the people served, and administrators (see Supplemental Material 2 for the value questions). Correlations between the WFS and values questions were low (see Supplemental Material Table 3 for the results).
Data Analysis
Descriptive statistics were employed for the demographic characteristics, as well as mean WFS scores and percentages for feelings of value in the workplace. We then compared mean scores and percentages based on gender identity, age, and race/ethnicity through a series of t, χ2, and analysis of variance tests to assess potential significant subgroup differences. Due to an initial error in the online survey instrument, early respondents did not receive several demographic items, resulting in missing data for gender (40% missing) and age (35% missing). Because missingness was caused by a technical error, we consider the missingness to be “missing completely at random” and will report the results.
We conducted stratified analyses by demographic groups regardless of cell size to ensure that findings from smaller groups (e.g., non-binary individuals, select racial groups) were also highlighted. Furthermore, we stratified our results by organization type to illustrate the experiences of peer-support specialists within a diverse set of agencies. However, these groups were excluded from our bivariate statistical analyses due to small sample sizes.
Results
As shown in Table 1, a majority of our sample was female (62.9%), included a mix of ages (20–39 years: 25.3%; 40–59: 53.4%; 60+: 21.3%; range: 20–77), and was predominantly White (81.0%), which is consistent with the demographic makeup of the peer-support specialist workforce in the United States. Specialists worked in a variety of governmental, non-profit, and for-profit organizations, with more than half working in community mental health centers (34.3%) and peer-run organizations (23.4%). The average 14-item WFS score was toward the upper end of the seven-point scale at 5.61 (SD = 1.15), indicating that fair practices in the workplace would lead to higher levels of job satisfaction among peer-support specialists. The vast majority of participants reported feeling that their life and work experiences were valued by fellow peer-support specialists (92.7%) and the people served (97.1%). However, less than two third reported that their life and work experiences were valued by clinicians (60.6%) and administrators (64.6%), a pattern which held across gender and age groups.
Workplace Fairness and Perceptions of Value Among Peer-Support Specialists (N = 274).
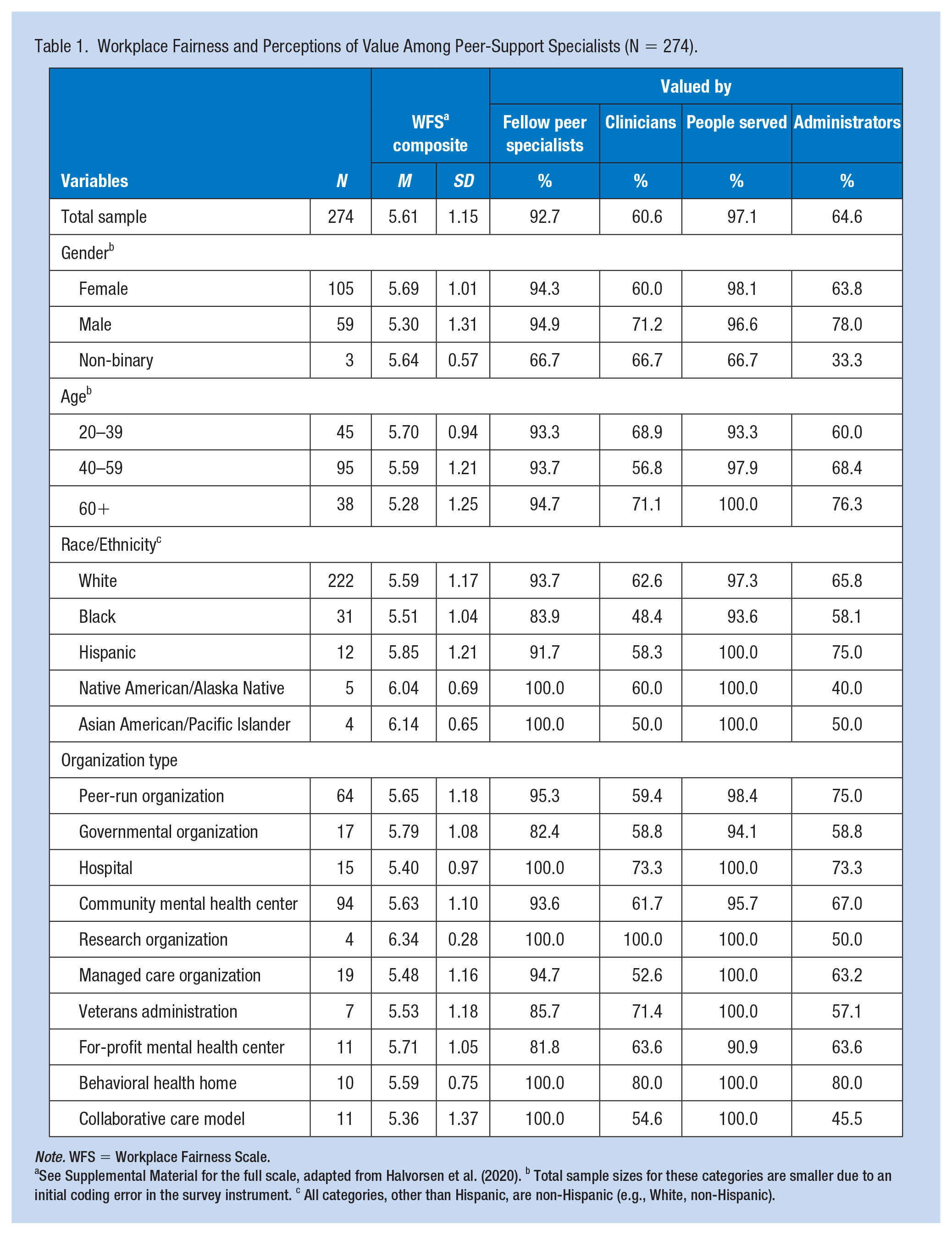
Note. WFS = Workplace Fairness Scale.
See Supplemental Material for the full scale, adapted from Halvorsen et al. (2020). b Total sample sizes for these categories are smaller due to an initial coding error in the survey instrument. c All categories, other than Hispanic, are non-Hispanic (e.g., White, non-Hispanic).
As shown in Table 2, scores did not differ significantly across racial/ethnic or age groups, but women reported significantly higher WFS scores than male participants (p = .03). When comparing non-Hispanic Black and White peer-support specialists, Black participants were significantly less likely to report feeling valued by their fellow peer specialists in the workplace (p = .047).
Subgroup Differences in Workplace Fairness and Perceptions of Value Among Peer-Support Specialists.
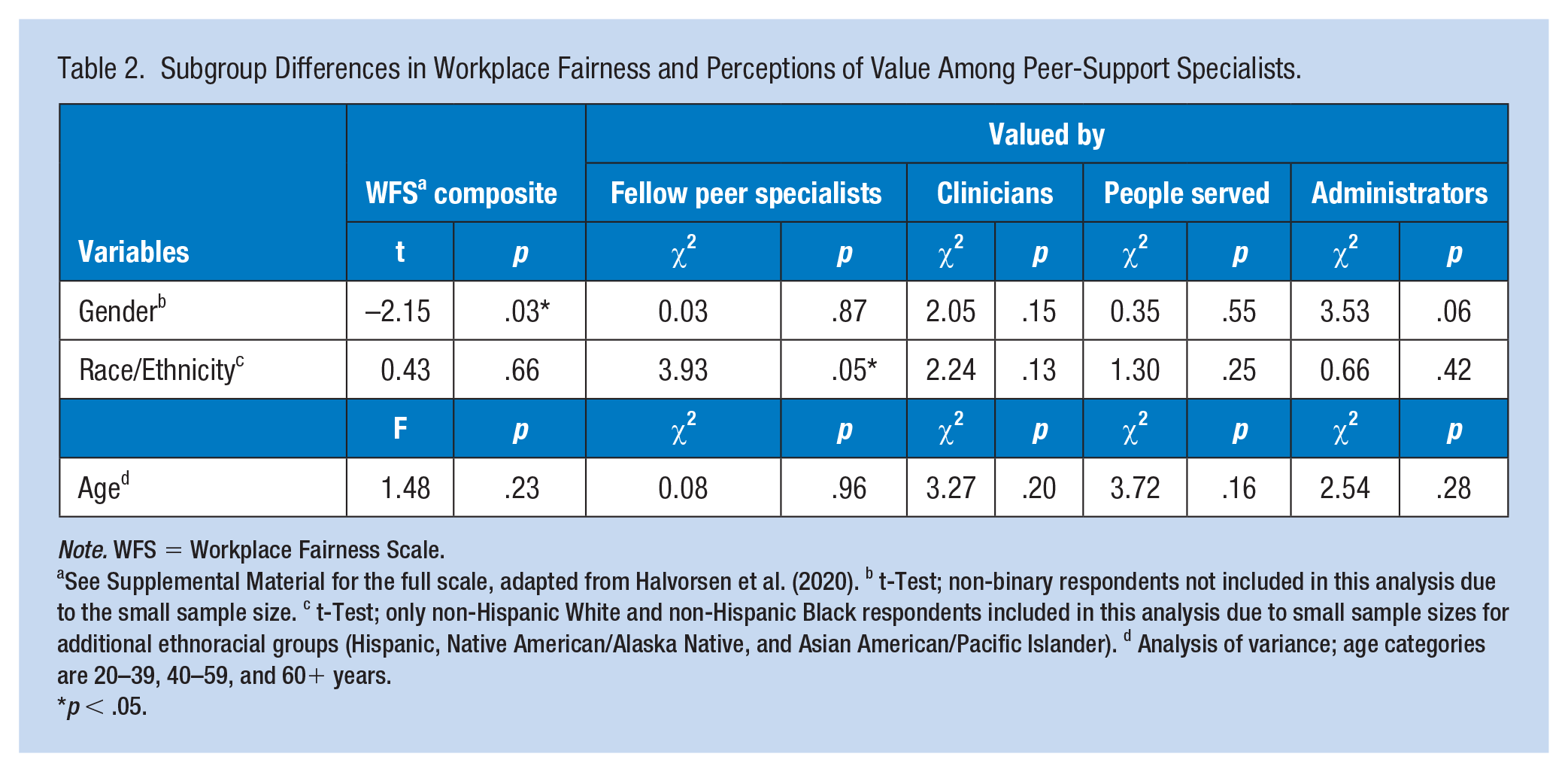
Note. WFS = Workplace Fairness Scale.
See Supplemental Material for the full scale, adapted from Halvorsen et al. (2020). b t-Test; non-binary respondents not included in this analysis due to the small sample size. c t-Test; only non-Hispanic White and non-Hispanic Black respondents included in this analysis due to small sample sizes for additional ethnoracial groups (Hispanic, Native American/Alaska Native, and Asian American/Pacific Islander). d Analysis of variance; age categories are 20–39, 40–59, and 60+ years.
p < .05.
Discussion
This study provides a descriptive overview of a relatively understudied group of mental healthcare workers. The first set of results considered hypothetical situations related to workplace fairness and job satisfaction, with our findings suggesting that peer-support specialists across subgroups link working for organizations that value fairness and equity with job satisfaction. Our second set of results considered participants’ perceptions of how peer-support specialists’ life and work experiences are valued at the workplace, in contrast to the first set of hypothetical questions.
It is notable that peer-support specialists reported feeling undervalued by administrators and non-peer clinicians. Our findings align with previous studies of peer-support specialists’ experiences. For example, they have reported facing discrimination based on both their own mental health diagnoses and their position as non-clinical staff, leading to a perceived lack of workplace value (Almeida et al., 2020; Firmin et al., 2019; Jones et al., 2019). Evidence suggests that this lack of perceived value negatively impacts peer-support specialists’ psychosocial well-being and is detrimental to the functional capacity of healthcare workplaces.
Our subgroup findings indicate that, overall, there were few differences in the role of workplace fairness in job satisfaction as well as feeling valued by fellow peer specialists, non-peer clinicians, administrators, and people served. However, future research with larger sample sizes for underrepresented subgroups (e.g., non-binary, Hispanic, Native America/Alaska Native, and Asian American/Pacific Islander respondents) is needed to better assess possible associations. Given the role of perceptions of fairness in the workplace for subsequent employee outcomes (Halvorsen et al., 2020), further research with larger and more diverse groups of peer-support specialists is needed to better understand their unique experiences at the intersection of workplace role and identity.
Although peer-support specialists were less likely to feel valued by administrators and clinicians, almost all reported feeling valued by their fellow support specialists and patients. While further research is needed to assess the effects of these results, they indicate the development of “collaborative capital” in the workplace—positive and supportive interpersonal communication and trust, often among workers within similar roles—just as previous research has documented among nurses and midwives, who experienced reduced burnout and stress and increased enjoyment at work due to its formation (McDonald et al., 2010). Feeling valued by others experiencing a serious mental illness may similarly buffer the effects of feeling less valued by administrators and clinicians.
While informative to the field and providing evidence that peer-support specialists feel valued more by those with similar experiences (fellow peer-support specialists as well as service users) and less by those in different positions (administrators and clinicians), this study has important limitations. First, it is unfortunate that due to an initial error in our survey coding, respondents did not see our questions related to gender and age. However, this was fixed partway through the field period, and we were glad to have enough data to conduct our planned analyses. Second, our questionnaire did not define the term “clinician,” although we did add “non-peers” after this term in the instrument to provide more context. Furthermore, while our survey did ask peer-support specialists what type of organization they worked for, it did not ask about the environmental context of their work (e.g., clinical settings, home or office settings, etc.). While these limitations make it impossible to differentiate between types of clinicians (e.g., physicians, nurses, nurse practitioners, pharmacists, etc.) or environmental contexts, our data still provide an overview of how peer-support specialists perceive their sense of being valued by non-peer staff who work in clinical roles. Finally, data were collected during the first year of the COVID-19 pandemic, a time when many mental health providers, including peer-support specialists, shifted to virtual or telephonic roles (Adams et al., 2022). Because our study was not designed to capture information on shifting roles, we are unfortunately unable to describe how their experiences differed between in-person, virtual, and telephonic environments. A major strength of our study is the documentation of peer-support specialists’ sense of feeling valued in the workplace and opinions on the link between workplace fairness and job satisfaction.
Implications for Occupational Health Practice
This study encourages organizations that hire peer-support specialists to consider and value the unique benefits offered by this class of employees to both patients and workplaces. Perceptions of fairness at the workplace are linked to individual, family, and organizational outcomes (Halvorsen et al., 2020; Ostrow et al., 2022), and qualitative research has indicated that peer-support specialists do not feel valued for the experiences and skills they bring to the role (Firmin et al., 2019). However, strategies by clinicians and administrators to increase peer-support specialists’ sense of value may benefit both the workforce and the workplace. Recent studies have shown that healthcare workers feeling valued by their organizations had lower odds of experiencing stress, anxiety, and burnout, as well as higher reported engagement at work (Haizlip et al., 2020; Prasad et al., 2021; Teo et al., 2021). Findings from multiple studies have highlighted the importance of developing mutual respect and supportive relationships between peer-support specialists and clinicians in increasing workplace satisfaction (Agarwal et al., 2020; Firmin et al., 2019; Gillard et al., 2022). Although literature on potential interventions is limited, some agencies, such as the City of Philadelphia Department of Behavioral Health and Intellectual Disability Services, have developed training toolkits to better integrate peer staff in the workplace (Philadelphia Department of Behavioral Health and Intellectual Disabilities Services & Achara Consulting, 2017).
Given the increasing mental health needs within the U.S. population (Mental Health America, 2022) and concurrent growing demand for behavioral health workers (Mental Health America, 2017), healthcare organizations must address barriers to successful integration of clinical and non-clinical staff. To do so requires a better understanding of the lived experiences of peer-support specialists. Future studies should delve deeper into the unmet needs of this critical class of workers.
Applying Research to Occupational Health Practice
This study highlights the important role that peer-support specialists play in behavioral health services. It assessed how peer-support specialists—individuals who have a diagnosed mental illness and provide support services to other adults with diagnosed mental health issues—perceive fairness and feel valued in the workplace. We analyzed results from a national, online survey of peer-support specialists (N = 274) to understand their perceptions of workplace fairness and how valued they felt by their fellow peer-support specialists, the people they serve, administrators, and clinicians. Peer-support specialists indicated that fairer workplaces would lead to higher levels of job satisfaction. While most felt valued by their fellow peer-support specialists and the people they served, far fewer felt valued by administrators and clinicians. Occupational health practitioners can play an important role in creating fairer workplaces and increasing peer-support specialists’ sense of being valued, which may lead to improved personal and organizational outcomes. For example, efforts to develop mutual respect and supportive relationships between peer-support specialists and clinicians or administrators (including occupational health practitioners) may lead to increased workplace satisfaction and engagement and lower levels of stress, anxiety, and burnout. Working in partnership with peer-support specialists, occupational health practitioners can also utilize existing toolkits or create new ones to better integrate peer staff into the workplace.
Supplemental Material
sj-docx-1-whs-10.1177_21650799231200028 – Supplemental material for Assessing Mental Healthcare Worker Experiences of Workplace Fairness and Organizational Value: A National Survey of Peer-Support Specialists
Supplemental material, sj-docx-1-whs-10.1177_21650799231200028 for Assessing Mental Healthcare Worker Experiences of Workplace Fairness and Organizational Value: A National Survey of Peer-Support Specialists by K. Megan Collier, Cal J. Halvorsen and Karen L. Fortuna in Workplace Health & Safety
Footnotes
Conflict of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Fortuna offers consulting services through Social Wellness and partners with Emissary Health.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The survey was funded by a grant from the National Institute of Mental Health (NIMH K01MH117496).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.