
Abstract
Health literacy (HL) is a stronger predictor of an individual’s health status than income, employment status, education level, and race or ethnicity. Lower levels of HL may contribute to low uptake or less adherence to occupational health and safety (OHS) training. This study was conducted among casting factory workers who received OHS training routinely. Data on sociodemographic characteristics, OHS training, and scores of the Health Literacy Survey–European Union (HLS-EU) were collected. Of the 282 of the 600 (47%) workers surveyed, 13.5% had inadequate, 47.5% problematic, 30.9% sufficient, and 8.2% excellent HL scores. There were no statistically significant differences between workers with limited and proficient HL with respect to age group or educational level. Workers with limited HL were less satisfied with OHS training content and were less likely to identify one-on-one health and safety training sessions as training. Limited HL is a universal problem both in the general and working populations, and it may be restricting the workers understanding of OHS training. Occupational health nurses should be aware of the detrimental effects of limited HL and modify their OHS training where needed for purposes of increasing the successful adoption of safe work practices.
Keywords
Introduction
Casting is a manufacturing process in which liquid metal is poured into a mold, so as to obtain the desired solid shape. The casting industry, which is considered high risk for injury (Ministry of Labor and Social Security, 2012), makes up 2.8% of Turkish manufacturing industries and employs more than 33,000 individuals (0.25% of the worker population; Ankara Chamber of Industry, 2017). According to Ministry of Labor and Social Security (2013) guidelines, an employee working in a high-risk workplace must receive at least 16 hours of occupational health and safety (OHS)-specific training per year. Besides general information on OHS, training must include information on labor legislations; legal rights and responsibilities; safety culture; ergonomics; safety signs and signals; personal protective equipment; occupational diseases; biological, chemical, and physical risk factors; first aid and rescue; and manual handling of loads.
Health Literacy
Health literacy (HL) pertains to the cognitive and social skills that determine the motivation and ability of individuals to gain access to, understand, and use the basic health information and services necessary for making appropriate health care decisions in ways that promote and maintain health (Nutbeam, 1998). Health literacy requires reading, listening, analytical, and decision-making skills, and the ability to apply these skills to health situations (Ratzan & Parker, 2000).
Health literacy is a stronger predictor of an individual’s health status than income, employment status, educational level, and race or ethnicity (Weiss, 2007). Individuals with low HL have demonstrated decreased compliance with medical information and medications, increased but ineffective health system use, higher medication use, and higher risk of death (Berkman et al., 2011; Durusu-Tanrıöver, Yıldırım, Demiray-Ready, Çakır, & Akalın, 2014; Sørensen et al., 2015). Low HL also poses an economic burden to society. The annual cost of low HL to the U.S. economy is estimated to vary from US$73 billion to US$238 billion (Georgetown University Health Policy Institute, 1994; Haun et al., 2015; Vernon, Trujillo, Rosenbaum, & DeBuono, 2007).
According to the National Assessment of Adult Literacy conducted in the United States, although 12% of the population demonstrated proficient HL, 53% and 22% reported having intermediate and basic HL, respectively, and 14% had below basic HL (Kutner, Greenberg, Jin, & Paulsen, 2006). In another study conducted by extracting data pertaining to 22,599 individuals from the Medical Expenditure Panel Survey, 77.6% of the population was found to have intermediate, 20.9% had basic, and 1.5% had below basic HL (Rasu, Bawa, Suminski, Snella, & Warady, 2015).
Although it is documented that even well-educated individuals can have limited HL (Karl & McDaniel, 2018; McCarthy et al., 2012), it is higher in certain disadvantaged population subgroups (older, minority, poorly educated, impoverished, and worse health), and it has been consistently associated with increased hospitalizations, greater emergency care use, poorer ability to take medications appropriately, poorer overall health status, and higher mortality (Berkman et al., 2011; Kutner et al., 2006).
The Health Literacy Survey–European Union (HLS-EU) has been conducted in eight countries with 8,000 participants (Sørensen et al., 2015). Although there were significant differences across countries, 47% of the surveyed population had limited (insufficient or problematic) HL. Furthermore, limited HL was more frequently observed in groups with low financial and social status, less education, or older age, and the highest proportion of those with limited HL comprised individuals with self-assessed worse health status, long-term illness, and higher demand for health services (Sørensen et al., 2015).
Health literacy levels in the Turkish population have been measured using various surveys (Durusu-Tanrıöver et al., 2014; Okyay & Abacıgil, 2016; Ozdemir, Alper, Uncu, & Bilgel, 2010). In one study conducted among 456 patients admitted to a family medicine clinic serving as a free primary health care unit in a suburban area of a metropolitan city, more than 40% were classified as having inadequate or marginal HL (Ozdemir et al., 2010). In a field study conducted among 470 volunteers, selected in public places such as shopping centers, the busiest streets of the province (Aydın), higher education schools (that are not offering vocational health science education such as nursing school), and workplaces, encompassing wide sociodemographic variation, it was found that 69.4% had limited HL (Okyay & Abacıgil, 2016). A more comprehensive field study conducted in seven regions of Turkey through home visits, which enrolled 4,924 volunteers was representative of the adult population of Turkey (Durusu-Tanrıöver et al., 2014). By using the HLS-EU, the general HL index of this population was found to be 30.4, and the HL level for 64.6% of the population was inadequate (24.5%) or problematic (40.1%) (Durusu-Tanrıöver et al., 2014).
The Organisation for Economic Co-operation and Development (OECD) conducted a survey in 28 member and five non-member countries to assess proficiency in three domains including literacy, numeracy, and problem solving in technology-rich environments that included 5,277 adults in Turkey (OECD, 2016). Compared with the other countries, the proficiency of Turkish adults was significantly below average in all three domains. Specifically, they scored 227 points on literacy (OECD average = 268 points) and 219 points on numeracy (OECD average = 263 points), and a majority of the adults showed no or only basic proficiency in problem solving in technology-rich environments. Only Chile and Indonesia scored below Turkey. This survey indicated that workers in Turkey used information-processing skills at work and in their daily lives much less often than workers in other countries (OECD, 2016).
Improving general HL skills in the workplace is a tool to empower individuals to make safe choices. Employees with higher literacy skills can better understand instructions for using equipment and materials, and they are more likely to comprehend and practice workplace health and safety procedures (Campbell, 2008, 2010; Kutner et al., 2006; OECD & Statistics Canada, 2000). Conversely, workers with low literacy skills tend to be overconfident and content with what they know, and they are unlikely to be aware of the personal, economic, and social disadvantages of their low literacy skills (Campbell, 2008; OECD & Statistics Canada, 2000; Wong, 2012). Moreover, they have a higher rate of occupational injuries and sickness and can understand neither health and safety regulations nor their rights to a safe and healthy workplace (Campbell, 2008; Wong, 2012). This connection between literacy levels, injury rates, and industry sectors underlines the need for development of these skills in high-risk work environments to achieve safer and healthier workplaces. When workers with low literacy or language skills are assisted in improving their skills, they are better able to act and react to workplace health and safety issues (Bloom, Burrows, Lafleur, & Squires, 1997). Businesses and their employees realize health and safety benefits when literacy and/or language skills development is introduced in the workplace.
We hypothesized that inadequate HL may contribute to low uptake or less adherence to OHS training and that it may be one of the factors leading to the ineffectiveness of the OHS training provided to workers. Accordingly, we measured HL and its relationship with the efficiency and perceptions of OHS training.
Method
This study was conducted among workers at a casting factory that included a heavy-duty foundry and machines that cast up to 150 tons and is classified as a workplace at high risk for injury (Akdas Casting, 2013).
The OHS team of the casting factory consisted of one medical doctor specializing in occupational health, three certified occupational health nurses, and five engineers who served as occupational safety specialists (OSS). This team provided 16 hours of training per worker each year since 2013. In addition, the physician spent 1 hour with workers individually at the commencement of his or her employment and during the annual physical examination. These sessions included discussion of medical history and job-specific health issues and protective actions. The OSS provided job-specific orientation and initiation training, as well as routine practical/on-the-job training. Although not specifically underlined as “training,” the information provided was defined as “the ideal way of doing a task, using appropriate personal protection equipment, and how the worker is expected to do the defined task.” For example, the physician described how to lift and carry a heavy object, provided a demonstration, and told the worker that he or she was expected to do as described and demonstrated. Moreover, health-related consequences of doing otherwise, and the possible harms it would cause, were also shared with the worker. The correct way of doing a task was described and demonstrated again if the OSS observed that the worker was not following the guidelines or he or she asked for a reminder. This team also provided classroom training on various occupational health topics. Further, if needed, training was provided by different experts outsourced from professional organizations specialized and certified in OHS training.
Data Collection
Approximately, 600 blue-collar workers at this factory, who received the OHS training routinely, were invited to participate in this survey. Data were collected between May and July 2017. Data on the sociodemographic characteristics were collected along with information pertaining to the HLS-EU (Sørensen et al., 2013) that was previously translated to Turkish by Durusu-Tanrıöver et al. (2014). The development, validity, and reliability; specific items of the HLS-EU; and a copy of the survey can be obtained elsewhere (Sørensen et al., 2013). The development of a valid and reliable Turkish version of the survey has been described by Durusu-Tanrıöver et al. (2014).
The workers participating in this study were asked seven questions about the OHS training they received, including about the number of sessions, job title of the trainer (OSS, OHS physician, certified occupational health nurse, or outsourced), location and manner (on the job, classroom presentation, or one-on-one practical), if they found the information useful, the method they preferred for the presentation, and how the training could be more beneficial in their view.
The HLS-EU survey contained 47 items evaluating the process of accessing, understanding, appraising, and applying health-related information within three domains including (a) health care, which ascertained information about their ability to access information on medical or clinical issues, to understand and evaluate medical information and to make informed decisions on medical issues and comply with medical advice; (b) disease prevention, which ascertained details about their ability to access and understand information on risk factors for health, to understand and evaluate information about risk factors and to make informed decisions to protect against risk factors for health; and, (c) health promotion, which gathered information about the ability to regularly update oneself on determinants of health in the social and physical environment, to interpret and evaluate information on determinants of health in the social and physical environment, and the ability to make informed decisions on health determinants in the social and physical environment and also engage in joint action.
For each item, respondents were asked to rate their perceived difficulty of a given task from very difficult to very easy on a 5-point Likert-type scale (1 = very difficult, 2 = difficult, 3 = easy, 4 = very easy, and 5 = does not know). The category “does not know” was used by the interviewer only in case the subject was unfamiliar with the item. The HLS-EU survey was read, and the workers’ answers were marked by the certified occupational health nurses employed at the factory after the workers provided informed consent. The questions evaluating the sociodemographic characteristics and OHS training were handed to the workers after finishing the HLS-EU survey, and they wrote down their answers to these questions by themselves.
Selecting one of the five choices was considered a legitimate response. To simplify comparisons, all scores were converted into a unified metric with a minimum score of 0 (least possible) and maximum of 50 (best possible), which were then classified as inadequate (0-25), problematic (26-33), sufficient (34-42), and excellent (43-50). The inadequate and problematic levels were combined into a single level, limited HL (0-33), and the sufficient and excellent levels into proficient HL (34-50) (Durusu-Tanrıöver et al., 2014; Sørensen et al., 2015).
Data Analysis
Scores of respondents who provided valid answers of ≥43 of the HL questions and ≥80% of the remaining survey items (sociodemographic characteristics and OHS training) were included in the analysis. The sociodemographic characteristics, general HL index, and subdomain indices (health care, disease prevention, and health promotion) measured by the HLS-EU and answers about OHS training were calculated as means, standard deviations, and percentage distributions. The chi-square test was used to compare differences between limited and proficient HL groups, and 95% confidence intervals (CIs) were calculated. Statistical significance was indicated by p < .05. The SPSS statistics software was used for data analysis. Gender and income-based comparisons of HL were not made owing to the fact that the majority were males or the number of workers who answered the income question was not adequate to stratify and compare various income levels by HL scores.
The study protocol and survey questions were approved by the Institutional Review Board of TOBB Economics and Technology University.
Results
The population of this study consisted of approximately 600 workers in a casting factory located in Ankara, Turkey. Of these, 394 (65.7%) consented to participate in this study, and 378 (63.0%) completed the survey questions. Scores of respondents who provided valid answers to ≥43 of the HL questions and ≥80% of the remaining survey items were included in the analysis. Thus, the final sample comprised 282 (47% of 600) workers.
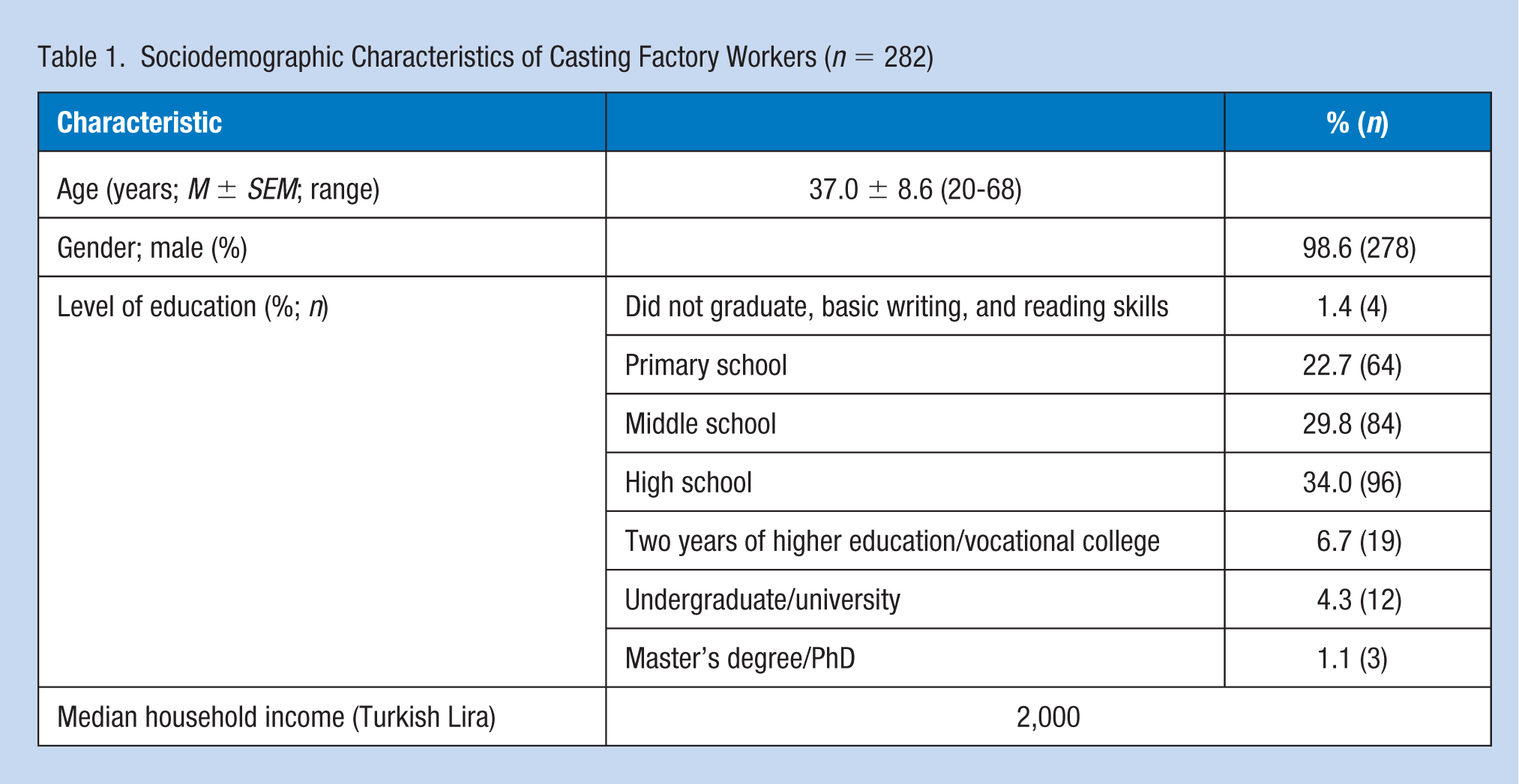
Sociodemographic characteristics are presented in Table 1. Owing to the physical requirements of the casting sector, most (98.7%) of the study population was male and specialized in metal manufacturing (forging, casting, cutting, stamping, and foundry works). Female workers were generally employed in administrative or housekeeping positions. Only 53.5% of the participants provided a response to the income question, the median of which is 2,000 Turkish Liras (approximately US$570 according to July 2017 exchange rates). This can be considered low income as the minimum net wage was 1,600 Turkish Liras. Of the participants, 39.3% indicated their unwillingness to answer the income question, and 7.2% stated that they did not know their household income.
Sociodemographic Characteristics of Casting Factory Workers (n = 282)
Among the respondents, 13.5% had inadequate, 47.5% problematic, 30.9% sufficient, and 8.2% excellent HL scores (Table 2).
HL Index Score a Among Casting Workers (n = 282)
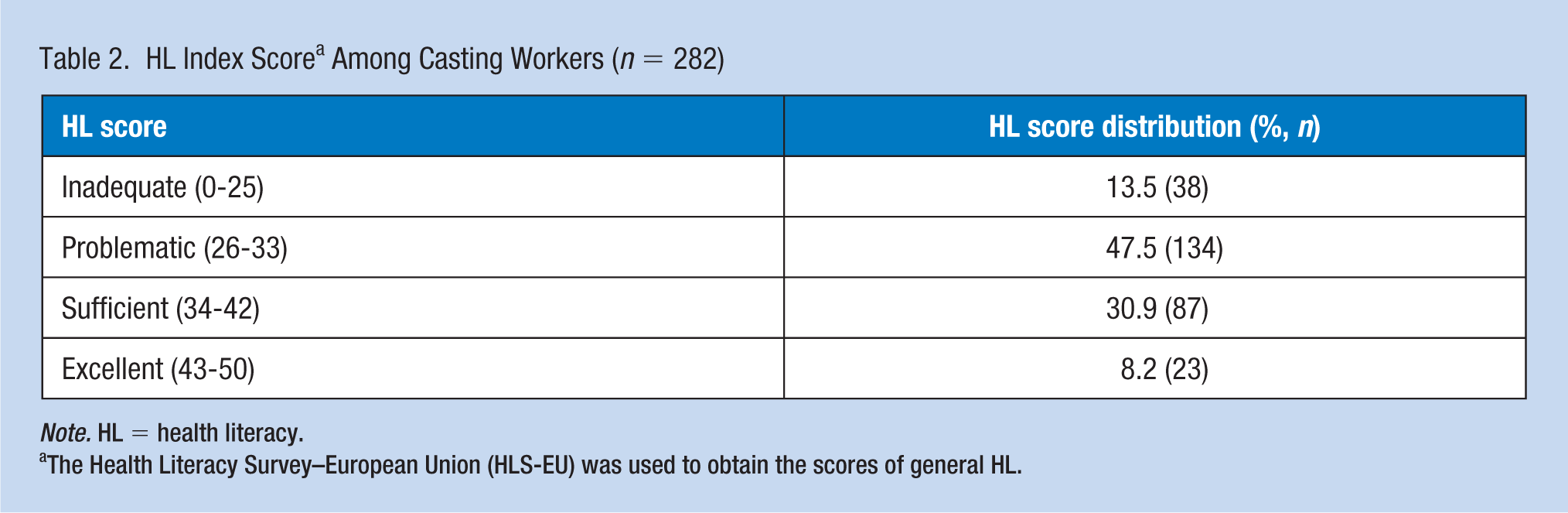
Note. HL = health literacy.
The Health Literacy Survey–European Union (HLS-EU) was used to obtain the scores of general HL.
Table 3 includes HL scores by workers’ age and educational levels. The comparisons were made between limited HL (0-33; inadequate and problematic levels) and proficient HL (34-50; sufficient and excellent levels). There were no statistically significant differences between workers with limited and proficient HL with respect to age group. Similarly, when the workers were stratified according to educational level, no statistically significant difference between HL levels was observed.
Comparison of Limited and Proficient HL Levels by Age and Education (n = 282)
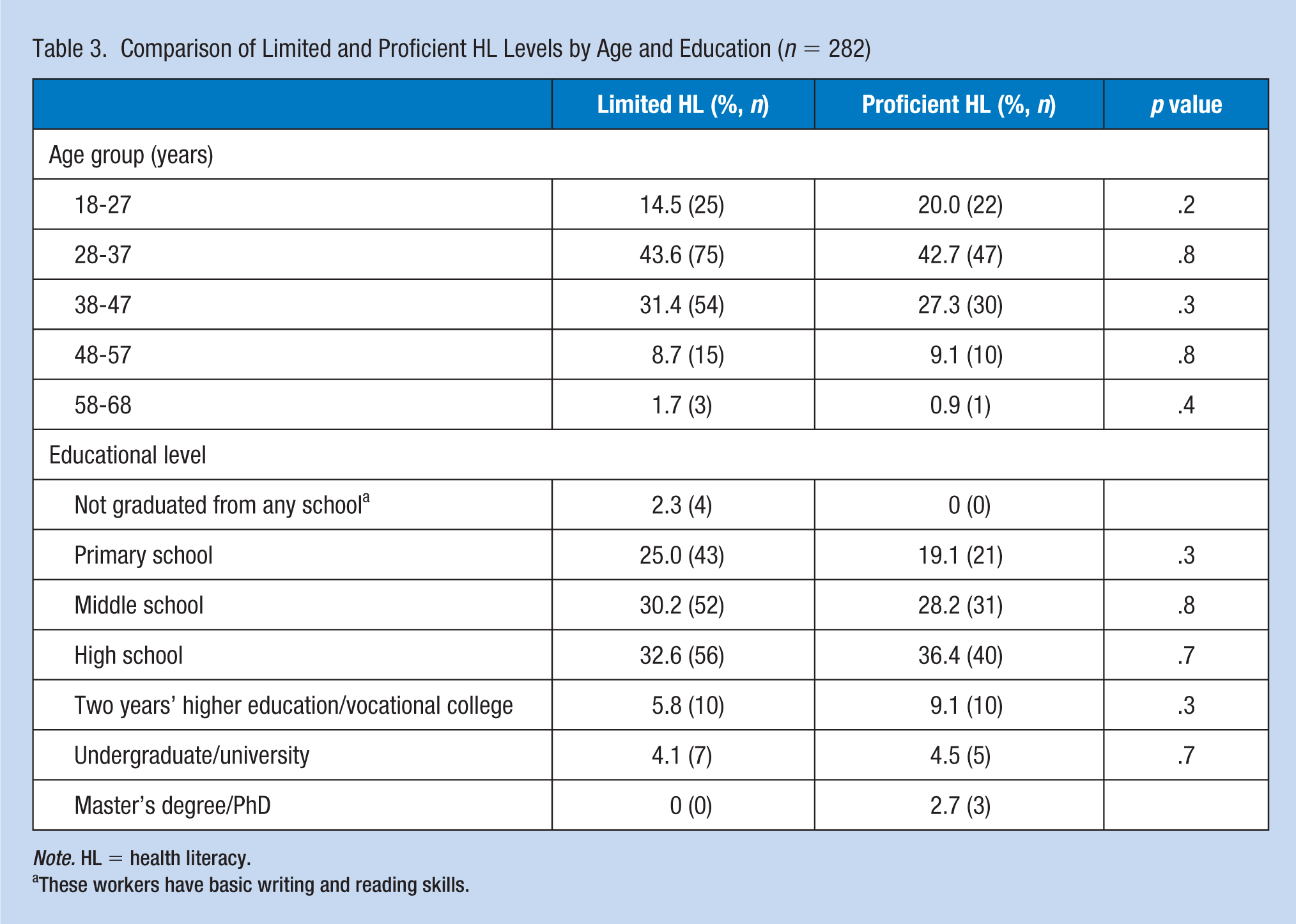
Note. HL = health literacy.
These workers have basic writing and reading skills.
Table 4 includes findings pertaining to OHS training and HL level. There were no significant differences between groups regarding the number of training sessions and training providers. However, the limited HL group reported receiving training from other sources (outsourced) more than the proficient HL group did.
Perception of OHS Training Characteristics in the Limited and Proficient HL Groups
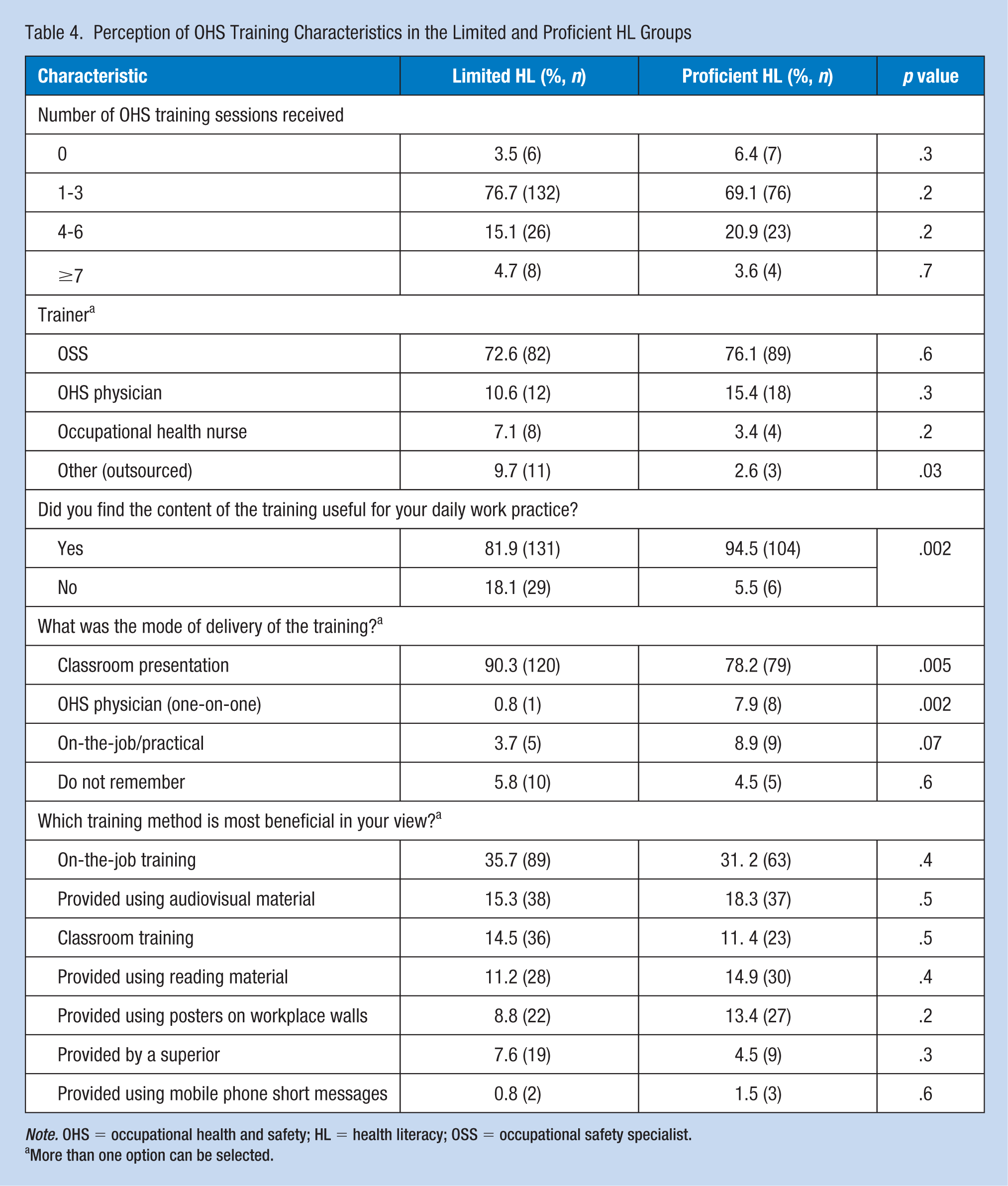
Note. OHS = occupational health and safety; HL = health literacy; OSS = occupational safety specialist.
More than one option can be selected.
In addition, those in the limited HL group were significantly less satisfied with the utility of the training relative to those in the proficient HL group. This group’s perception of the delivery method was significantly different from that of the proficient HL group; whereas classroom presentation was selected more often, training by an OHS physician (one-on-one) and on-the-job/practical training were selected significantly less often by workers with limited HL. Furthermore, both groups most frequently selected on-the-job training as a beneficial training method.
Discussion
The primary finding of this study was that those with limited HL were less satisfied with the training content and were less able to identify training when it was conducted by an OHS physician or OSS in a one-on-one session. The workers did not view information received during a physical examination as “training,” although the trainer explicitly stated the reason and expected outcome during such interactions. However, classroom training was self-explanatory in this sense. As the general aim of one-on-one training is to obtain an immediate behavioral change, we suggest that trainers be more clear and descriptive about the content and expected outcomes and that the session be initiated with an explicit statement identifying it as “training.”
According to Berkman et al. (2011) lower HL was associated with increased hospitalization, greater emergency care use, lower use of mammography, lower receipt of influenza vaccine, higher risk of mortality, poorer ability to demonstrate taking medications appropriately, poorer ability to interpret labels and health messages, and poorer overall health status. Despite the fact that individuals with limited HL benefit less from what health care systems have to offer as compared with those with proficient HL, the content and delivery method of health information generally is not changed by the health care provider based on the individuals’ HL levels (Berkman et al., 2011). Moreover, routinely screening individuals for HL is not recommended as it has not been shown to improve outcomes (Hersh, Salzman, & Snyderman, 2015). Accordingly, improving communication quality in health care organizations and implementing universal HL precautions as described in the National Action Plan to Improve Health Literacy (U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion, 2010) to provide understandable and accessible information to all users of the health care system, regardless of their HL levels, seems to be a better approach (U.S. Department of Health and Human Services, Office of Disease Prevention and Health Promotion, 2010; Weiss, 2007; World Health Organization [WHO], 2009; Wynia & Osborn, 2010).
Occupational HL was first defined by Rauscher and Myers in 2014 as “the degree to which workers have the capacity to obtain, communicate, process, and understand OHS information and services to make appropriate health decisions in the workplace.” Regardless of the value of that study, it did not measure occupational HL with a tool that had been proven valid and reliable for that sole purpose. Besides, the literature referred to as the source of this tool does not claim to measure occupational HL; instead, it describes their methodology as a telephone survey questioning adolescents on whether they were exposed to hazards at a workplace or their injury experience (Dunn, Runyan, Cohen, & Schulman, 1998). However, both studies provided valuable information on the OHS training, knowledge, and awareness of adolescent workers and their work-related injury experiences (Dunn et al., 1998; Rauscher & Myers, 2014). A more recent study claiming to measure “occupational HL” did not describe the basics of the survey employed (Yusida, Suwandi, Yusuf, & Sholihah, 2016). Based on the limited literature on the subject, as there are no tools with proven validity and reliability, it was not possible to measure occupational HL specifically in this study. Thus, we measured general HL and related it with workers’ perceptions of OHS training.
OHS training is a fundamental element in improving the safety culture at the workplace and in promoting a healthy workplace environment by encouraging employees to make safer choices. Companies provide and spend a considerable amount of monetary and human resources for such training, but they are unable to achieve desired outcomes such as proper use of personal protective equipment, adoption of all safety rules, and minimization of risky behaviors. Although employers expect a sufficient return on their investment, the achievement of successful training outcomes, such as preventing injuries, is not as high as anticipated (Robson et al., 2010). The employees’ inability/incapacity/unwillingness to adopt a safety culture and to make safe choices is one of the main reasons for this failure. Regardless of a country’s geography, culture, and development status, this is a universal problem that reveals the need to improve the effectiveness of OHS training efforts (Robson et al., 2010).
Health is a key asset for the economy, and companies play an essential role, both as the determinant and the main beneficiaries of health outcomes. The economic burden of poor health not only includes medical and pharmaceutical expenses but also health-related productivity loss due to absenteeism or presenteeism, the effect of which is generally much greater than that of medical/pharmaceutical expenses (Loeppke et al., 2009; Nagata et al., 2018). The three main issues influenced by HL are defined as access and utilization of health care, patient–provider relationship, and self-care (Paasche-Orlow & Wolf, 2007). Although we did not examine the association of HL with absenteeism/presenteeism in the present study, it would not be wrong to assume that low HL has a negative impact on these concepts, which can be evaluated under all three of the abovementioned issues.
Both limited HL and OHS issues are global public health problems. Based on the report of the Institute of Medicine on HL (2004), 90 million adults have trouble understanding and acting on health information, and it is suggested that institutions and health care providers need to improve their communication skills and provide people with clear information. Similarly, if workplaces arrange and provide OHS training modified in accordance with universal HL precautions, the probability of workers’ adoption of a safety culture will increase, and accordingly, workplace-related accidents, sickness, and even deaths will decrease. Moreover, these workers will transfer their knowledge to those in their social circle. Together, these factors will improve productivity and welfare and decrease costs related to health and safety behavior.
Limitations
The main limitation of this study is the number of workers who provided consent to participate (394 out of 600 workers) and the number of workers who answered the questions adequately (n = 282). The reasons for not consenting can be unsuitability of shift schedules or feeling uncomfortable about participating. The reasons for not completing the survey could be difficulty in understanding the study procedures or tools, or feeling uncomfortable with some of the questions.
Almost half of the participants did not complete the income portion of the survey. Income is a determinant of HL level; however, we were unable to perform the planned comparisons based on this parameter.
Trainers did not provide workers with the formal definition of “training” during the OHS unit visits or on-the-job/on-site training, which we believe had an effect on successfully identifying training as such.
In general, focus group interviews would add more value to our findings by revealing the rationale behind some of the answers provided by the workers. However, this study was not designed accordingly.
Implications for Occupational Health Nursing Practice
In the factory where this study was conducted and, we assume, in most of the OHS units of such workplaces, the OHS personnel workers most often encountered are occupational health nurses. Thus, it is essential that occupational health nurses are aware of the prevalence of limited HL, its possible effects on OHS, and the need of a better approach to workers with low HL.
The main finding of this study was that workers may not be able to recognize training and its importance for their health and safety, especially if they have limited HL. Abandoning the one-size-fits-all approach is the first step to be taken. It is not feasible and may be considered unethical to measure each and every worker’s HL and classify them. However, increasing the occupational health nurses’ awareness of the effects of limited HL on health and safety may be the initial step toward creating a “health literate” environment at the workplace. Strategies to improve HL for employers and the attributes of a health-literate organization are well-defined by Wong (2012); this study provides a guideline to initiate the change. The ability of occupational health nurses to work with multidisciplinary stakeholders makes them the major player with a significant role in building health literate workplaces.
Occupational health nurses are expected to be proactive in developing strategies to promote health and work ability by considering even nonwork-related factors that may affect workers’ ability to maintain attendance or performance at work. Workers with limited HL may not be aware of the environmental, social, and other factors that would affect these abilities. However, because of the occupational health nurses’ direct access to workers and vice versa, occupational health nurses generally become the first point of contact for many health-related questions and problems. Thus, occupational health nurses’ awareness of limited HL and its effects on physical and social well-being is essential for increasing the efficiency of OHS units and the training they provide. Underlining the fact that the meeting is a training session; providing the information and facts in a clear, understandable fashion; asking workers to describe and demonstrate what they have learned; repeating the information after sufficient intervals; and close monitoring following the training session are expected to lead to behavioral change and increase efficiency.
Conclusion
In conclusion, limited HL is a universal problem both in the general and working populations. Workers face varying levels of hazards depending on the risk level of their workplace, and limited HL may be one of the factors restricting their understanding of OHS training, which limits efficiency and in turn limits the improvement in their safety.
Applying Research to Practice
As the Occupational Health and Safety personnel workers most often encountered are occupational health nurses, it is essential that occupational health nurses (OHN) are aware of the prevalence of limited health literacy (HL), its possible effects on health and safety, and the need of a better approach to workers with low HL. Increasing the OHNs’ awareness of the effects of limited HL on health and safety may be the initial step toward creating a “health literate” environment at the workplace. Abandoning the one-size-fits-all approach is the first step to be taken. Underlining the fact that the meeting is a training session; providing the information and facts in a clear, understandable fashion; asking workers to describe and demonstrate what they have learned; repeating the information after sufficient intervals; and close monitoring following the training session are expected to lead to behavioral change and increase efficiency.
Footnotes
Acknowledgements
The authors would like to thank İsmail Taşan, Birol Ağa, and Özkan Sarıkaya for collecting data, and Güneş Ekmekci and Nazlı Yağmur Erhan for data entry. We would also like to thank Occupational Health and Safety Manager Ayşe Gül Mangan and Dr. Önder Güner for their valuable inputs during the planning and conduct of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Muberra Devrim Guner, MD, PhD, is an associate professor in the Department of Medical Pharmacology at TOBB Economics and Technology University Medical School, and has publications on basic pharmacological research and clinical trials. Current research areas include pharmacovigilance, pharmacoepidemiological studies, health literacy, and ethical aspects.
Perihan Elif Ekmekci MD, PhD, is an associate professor in the Department of History of Medicine and Ethics at TOBB Economics and Technology University Medical School, and was elected as the first Turkish fellow for Western Institutional Review Board Research Ethics Program. Her research interests are ethical aspects of clinical trials, health literacy, and pharmacogenomics information and history of medicine.