
Abstract
Background:
Cardiovascular disease (CVD) remains the leading cause of morbidity and mortality in the United States, with 20% of deaths in adults under age 65. Commercial drivers have an increased CVD incidence rate of 50% compared to 30% for the general population, yet one third of drivers will not be screened for risk factors due to a lack of insurance or primary care. With approximately 3.5 million commercial drivers nationally and correlation of CVD to increased motor vehicle accidents, fatalities, and excessive healthcare costs, addressing the care gap for this high-risk population is imperative.
Methods:
An evidence-based practice (EBP) project synthesized the literature and implemented CVD risk screening for commercial drivers examined in an occupational practice setting. Using the non-laboratory Framingham CVD risk score calculator, over 90% of drivers were screened during mandated medical examinations and provided education regarding modifiable risk factors during a 2-month period.
Findings:
Over 40% of commercial drivers were at high risk for CVD with 25% uninsured and 32% without primary care. The average CVD risk score was twice the general population’s risk score, with obesity, hypertension, and smoking being the most common risk factors discussed.
Conclusions/Application to Practice:
Incorporating CVD risk screening and education during opportune encounters is logical, efficient, and financially prudent. The EBP change supports occupational professionals’ standards, and ongoing review of CVD screening guidelines with integration into practice provides health promotion and promotes public safety for these essential workers.
Background
Cardiovascular disease (CVD) encompasses conditions affecting the heart and blood vessels and remains the major cause of morbidity and mortality in the United States, with 20% of deaths occurring in adults under age 65 (Centers for Disease Control and Prevention, National Center for Health Statistics [NCHS], 2021a, 2021b). The use of CVD risk screening, risk reduction strategies, and advanced treatment has decreased mortality by 30.6% during the past 40 years; however, the burden of CVD remains high with costs exceeding $200 billion annually and high disability rates related to post-cardiac event complications (Frieden et al., 2020; Peterson Center on Health Care, Kaiser Family Foundation, 2017; Virani et al., 2020). Therefore, novel approaches to CVD risk screening and risk reduction are needed for the U.S. population.
Cardiovascular disease risk factors (RFs) include smoking, hypertension, obesity, high total cholesterol, low levels of high-density lipoproteins (HDLs), elevated levels of low-density lipoproteins (LDLs), diabetes, and sedentary lifestyle (Centers for Disease Control and Prevention [CDC], 2022b). Commercial drivers continue to have up to a 50% incidence rate of CVD compared with 30% for the general population due to higher smoking rates, poor eating habits, disrupted sleep routines, and metabolic issues (CDC, 2023; Hege et al., 2018; Sieber et al., 2014). Evidence has also related undiagnosed medical conditions and lack of treatment to an increased risk for motor vehicle accidents and fatalities for commercial drivers (FMCSA, 2020; Ronna et al., 2016).
Clinical practice guidelines (CPGs) recommend baseline CVD risk screening at age 20 and biannual with absolute 10-year CVD risk assessment beginning at age 40 (American College of Cardiology/American Heart Association, 2020). The United States Health and Human Services department identified a goal to reduce preventable heart attacks and strokes by 1 million events by 2027 through reduction of RF, care optimization, and improved health equity (United States Department of Health and Human Services, 2021). Unfortunately, 30% of workers in the United States remain uninsured or without primary care and will not receive CVD risk assessment, preventive strategies, or prompt treatment (Tolbert et al., 2022).
The Patient Protection and Affordable Care Act of 2009 improved access to preventive care, but individual health insurance remained expensive for many workers with high deductibles that decrease utilization of primary care services (Tolbert et al., 2022). With 29% of commercial drivers being self-employed and an additional 30% working for small companies (i.e., less than 50 workers), obtaining health insurance remains a significant challenge for this workforce (Day & Hait, 2019). With a projected shortage of 60,000 primary care providers (PCPs), especially in rural areas, efforts to improve health and reduce premature mortality among commercial drivers through occupational programs continue to be a priority (Association of American Medical Colleges [AAMC], 2021; Health Resources and Services Administration, 2013; National Occupational Research Agenda, 2009; National Occupational Research Agenda Transportation, Warehousing, and Utilities Sector, 2018). Ongoing review of insurance coverage and primary care access for working adults are also important topics for occupational practices to assess, especially in rural and medically underserved areas (MUA).
With an estimated 3.5 million commercial drivers in the United States, early identification of CVD risk has become imperative to promote a healthier workforce and a safer community (Day & Hait, 2019). Federal and state regulations mandate annual to biannual medical examinations conducted by certified medical examiners (CMEs) who review commercial drivers’ medical history, height, weight, blood pressure, smoking status, and urinalysis CLIA-waived test results (FMSCA, n.d.). Current examination guidelines do not require a calculated body mass index (BMI), lipid levels, or physical activity documentation; however, CMEs routinely discuss these RFs during medical examinations and can address the gap in CVD screening for commercial drivers. In addition, providing standardized yet individualized CVD RF education would serve as a preventive strategy to encourage health behavior changes that could reduce morbidity and mortality for these essential workers.
Finding a solution to address the clinical problem of increased CVD risk and decreased access to primary care for commercial drivers utilized an evidence-based practice (EBP) process. Integration of CVD risk screening and standardized RF education for this population supported occupational professionals’ standards related to assessment, diagnosis, implementation, collaboration, and disease prevention (American Association of Occupational Health Nurses [AAOHN], n.d.; American College of Occupational and Environmental Medicine [ACOEM], 2021). Factors that influenced EBP implementation in a rural occupational practice, process and outcomes evaluation, and practice considerations that enhanced sustainability are presented.
Methods
A synthesis of literature identified that CVD risk screening was feasible to implement in occupational practice, thereby supporting translation of evidence into practice (Melnyk and Fineout-Overholt, 2019). Regardless of insurance or primary care status, CVD risk screening was offered to commercial drivers obtaining their mandatory medical examinations during a 2-month period. Consenting drivers were provided with a CVD risk score based on a valid, reliable screening tool along with discussion of the results and modifiable risk factors by the CME. Demographic and screening data were collected through chart reviews. Demographic data was compared to commercial drivers examined during the same 2-month period in the prior year to enhance generalizability of findings. The CVD risk scores were categorized and compared to the general population’s provided as part of the screening tool. Cardiovascular disease RFs were categorized and compared to the literature in addition to capturing information related to insurance and PCP status.
Evidence-Based Practice Interventions
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA, n.d.) 2020 process provided structure for the initial literature review in 2014 and updated review in 2022 as overviewed in the PRISMA flow diagram (Figure 1). The synthesis of evidence supports ongoing implementation of CVD risk screening for commercial drivers using a non-laboratory method, application in occupational practice, and standardized CVD RF education.
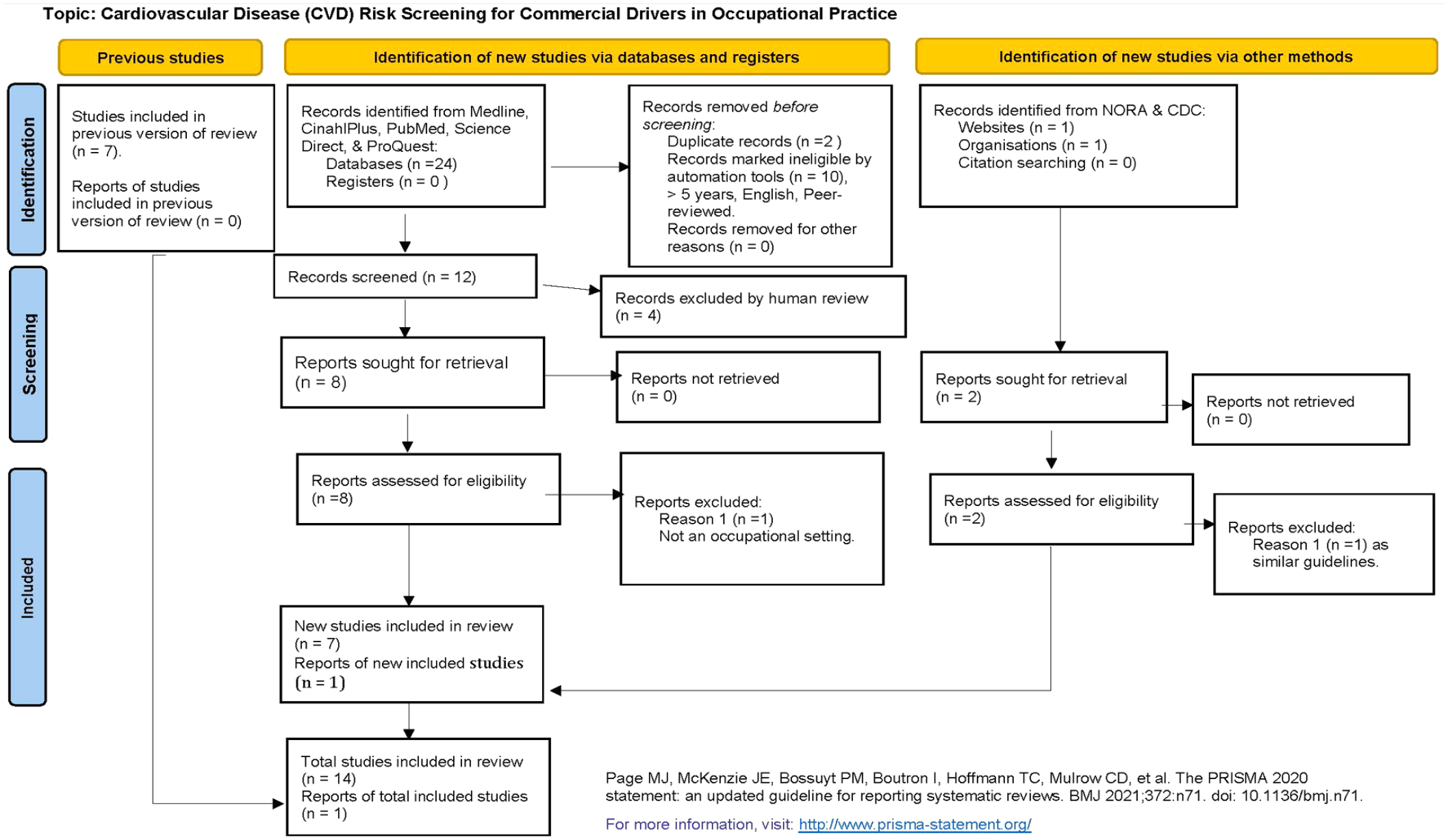
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) Flow Diagram.
Non-Laboratory CVD Risk Screening
Research demonstrated that the non-laboratory, Framingham 10-year CVD risk score accurately discerns CVD and should be considered when laboratory data is unavailable or resources limited (Jones et al., 2015; Rezaei et al., 2021, 2022). Non-laboratory risk models have been validated and provided reliable results with superior sensitivity and specificity when compared to other CVD risk algorithms (Gaziano et al., 2008; Kariuki et al., 2017; Rezaei et al., 2022).
Implementing the Framingham non-laboratory method using BMI instead of cholesterol levels increases application of CVD risk screening and reduces initial cost. In addition, the Framingham non-laboratory method for CVD risk screening is logical to implement because laboratory tests are not part of the drivers’ medical examinations.
Occupational Practice Setting
National recommendations have demanded increased health prevention and promotion efforts in occupational programs (NORA TWU, 2018). Studies conducted in occupational settings have demonstrated the ability for early detection of CVD risk, reduction in CVD RF with behavioral interventions, and overall benefits for the worker, employer, and healthcare system (Andres et al., 2013; Arena et al., 2013; Iakoubova et al., 2019; Marcinkiewicz et al., 2021). Although national and international guidelines remain obscure regarding screening, the need to assess CVD risk for workers in high-risk occupations such as commercial driving remains a current and relevant topic (Apostolopoulos et al., 2013; Parsons et al., 2022). In addition, engaging young adults aged 21 to 39 years in opportune settings such as occupational practice and using technology such as the risk score calculator could increase engagement in health promotion efforts (Gooding et al., 2020). Furthermore, CVD risk screening supports ethical practice by decreasing maleficence through advanced assessment of drivers’ fitness for duty, increasing beneficence through screening of a high-risk population, and promoting social justice through improved access to care (Hirsch et al., 2014; Kaspin et al., 2013).
The rural occupational practice that integrated EBP of CVD risk screening during commercial drivers’ medical examinations routinely discusses health risks and refers drivers with new or uncontrolled conditions to primary care. Established PCPs and agencies that accepted insured and uninsured patients are identified prior to implementing CVD risk screening to promote referral for preventive care or follow-up for identified health conditions including hypertension and diabetes mellitus.
Health Behaviors for CVD
Identification and reduction of CVD RF have significantly lowered the morbidity, mortality, healthcare costs, and disability for workers globally (Frieden et al., 2020; Goyer et al., 2013; Hirsh et al., 2014). Therefore, standardized education on CVD RF is included from reliable sources such as the American Heart Association, American Lung Association, Centers for Disease Control and Prevention, U.S. Department of Nutrition, and the U.S. Preventive Services Task Force. Since implementation in 2014, educational materials for CVD RF have been updated as evidence-based guidelines are published or revised.
EBP Implementation and Participation
Initial EBP implementation was completed in the fall of 2014 following training from the National Institute of Health on protection of human research participants and university Institutional Review Board (IRB) approval for a Doctor of Nursing Practice (DNP) project. The process to include the CVD risk screening as part of the commercial driver’s medical examination process was developed (Figure 2). All drivers over age 21 were eligible to participate with informed consent obtained prior to CVD risk screening to ensure privacy, justice, respect, and decision-making. Since implementation in 2014, CVD risk screening using the non-laboratory method continues for commercial drivers who provide verbal consent to the CME during their medical examinations.
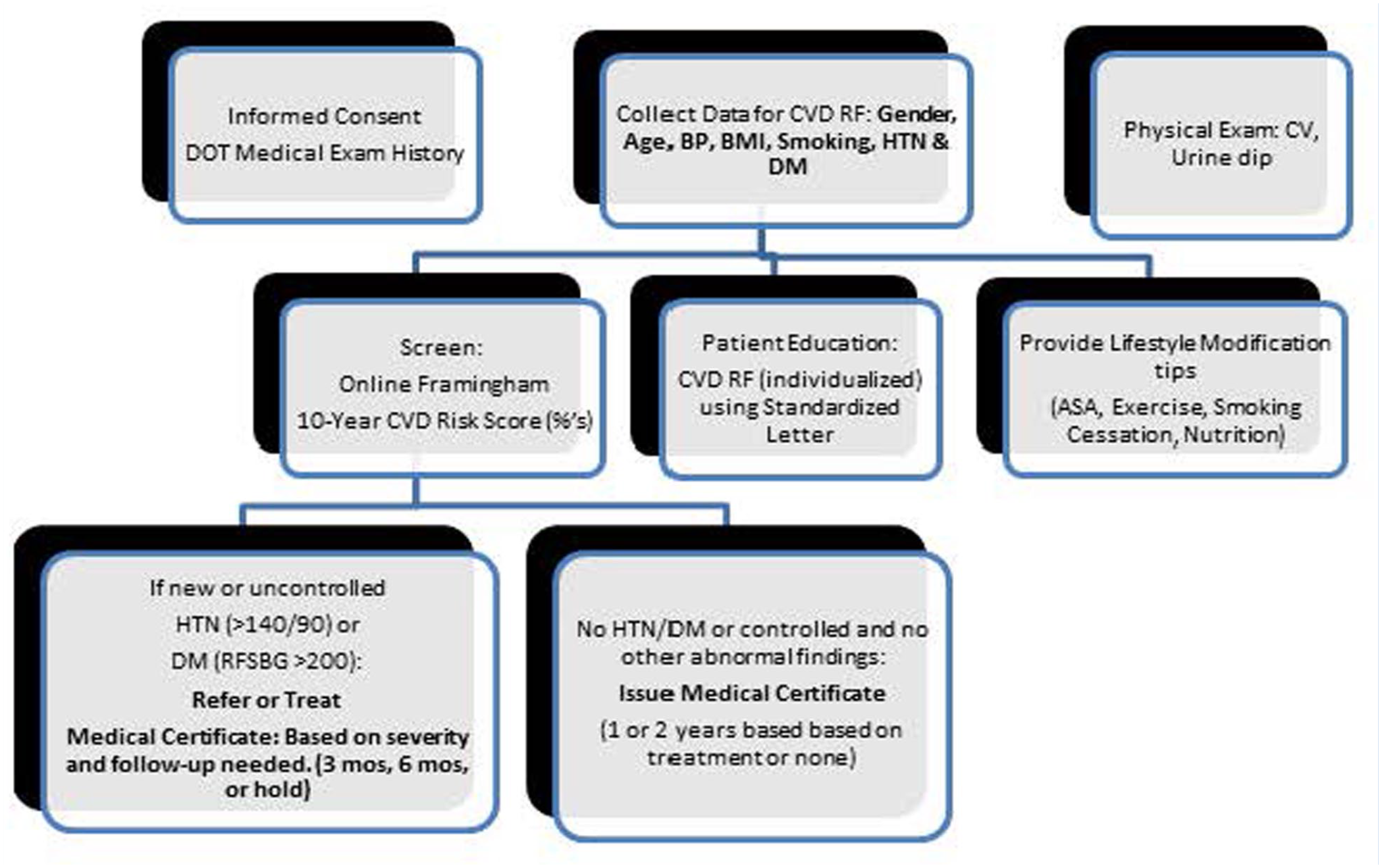
Process for CVD Risk Screening in Occupational Practice.
Most commercial drivers have been English speaking with an online language translator available for use as needed. To minimize conflict of interest, no revenue is generated from CVD risk screening with results provided for patient education and health promotion only. Documentation of the CVD risk score is not disclosed to employers or external agencies to maintain privacy and confidentiality of a driver’s health information.
Data Collection
The non-laboratory Framingham 10-year CVD risk score using BMI for the online calculator or Excel spreadsheet is utilized for screening in consideration of no cost, no routine laboratory results required for the medical examination, and literature findings (Framingham Heart Study, 2022). The electronic health record (EHR) has not been utilized for CVD risk screening, although clinical alerts for blood pressure, smoking, BMI, and diagnosis of hypertension or diabetes are pertinent to review for returning drivers. The CVD risk score does not directly affect medical certification; therefore, it is not included on federal examination forms, or the medical certificate provided to employers, the Department of Motor Vehicles, and the Federal Motor Carriers Safety Administration (FMCSA).
After an initial 2-month EBP implementation period from November to December 2014, chart reviews were completed to collect demographic data regarding participants’ age and gender for comparative analysis to drivers examined during the same 2 months of the prior calendar year. Additional data for analysis included the participants’ CVD risk scores, CVD RF, insurance status, and PCP status. Following the initial implementation period, identified trends and updates are discussed.
CVD Risk
Information used to calculate the 10-year CVD risk score include the driver’s age, gender, height/weight to calculate BMI, smoking, history of hypertension, and history of diabetes. An individual CVD risk score is obtained after entering the information into the non-laboratory Framingham calculator or Excel spreadsheet as well as the risk category stratified as low (<10%), intermediate (10%–20%), or high (>20%). The calculated risk score is also compared to normal and optimal scores for the population and discussed with each driver using a patient education form (Figure 3).
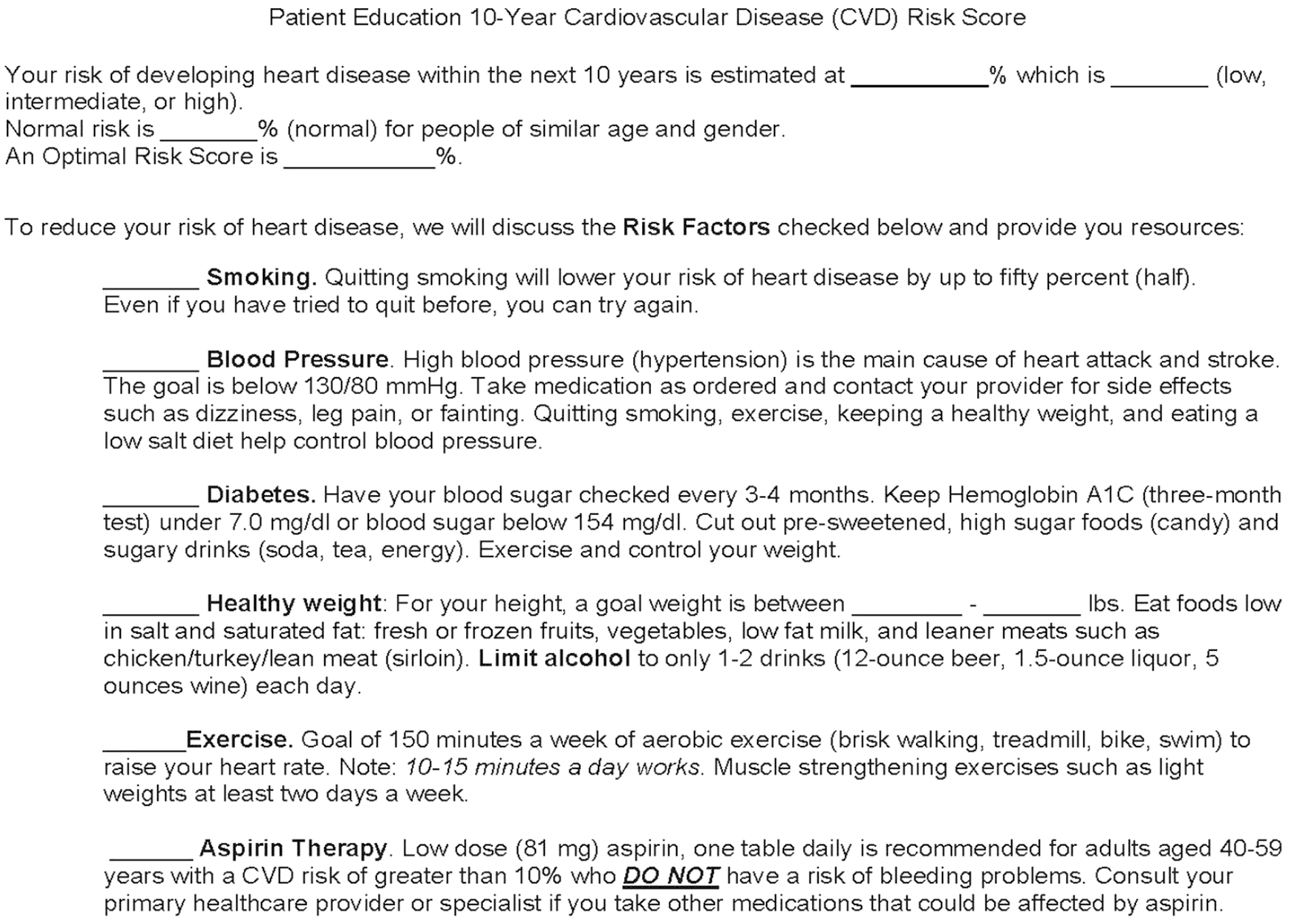
Patient Education Form
CVD Risk Factors and Health Behaviors
Identified, modifiable CVD RFs are also reviewed by the CME with each driver using the patient education form. The Framingham guidelines emphasized addressing multifactorial RF; therefore, standardized education and local or national resources are provided for smoking cessation, dietary intake, weight goals, and physical activity (Hajar, 2016). Low-dose aspirin therapy recommendations follow national guidelines that include risk review with updated guidelines for adults aged 40 to 59 years for more recent screenings (United States Preventive Services Task Force [USPSTF], 2009, 2022; Wolff et al., 2009). An example of the CVD risk score calculation with RF education and medical certification considerations for a commercial driver is provided (Figure 4).
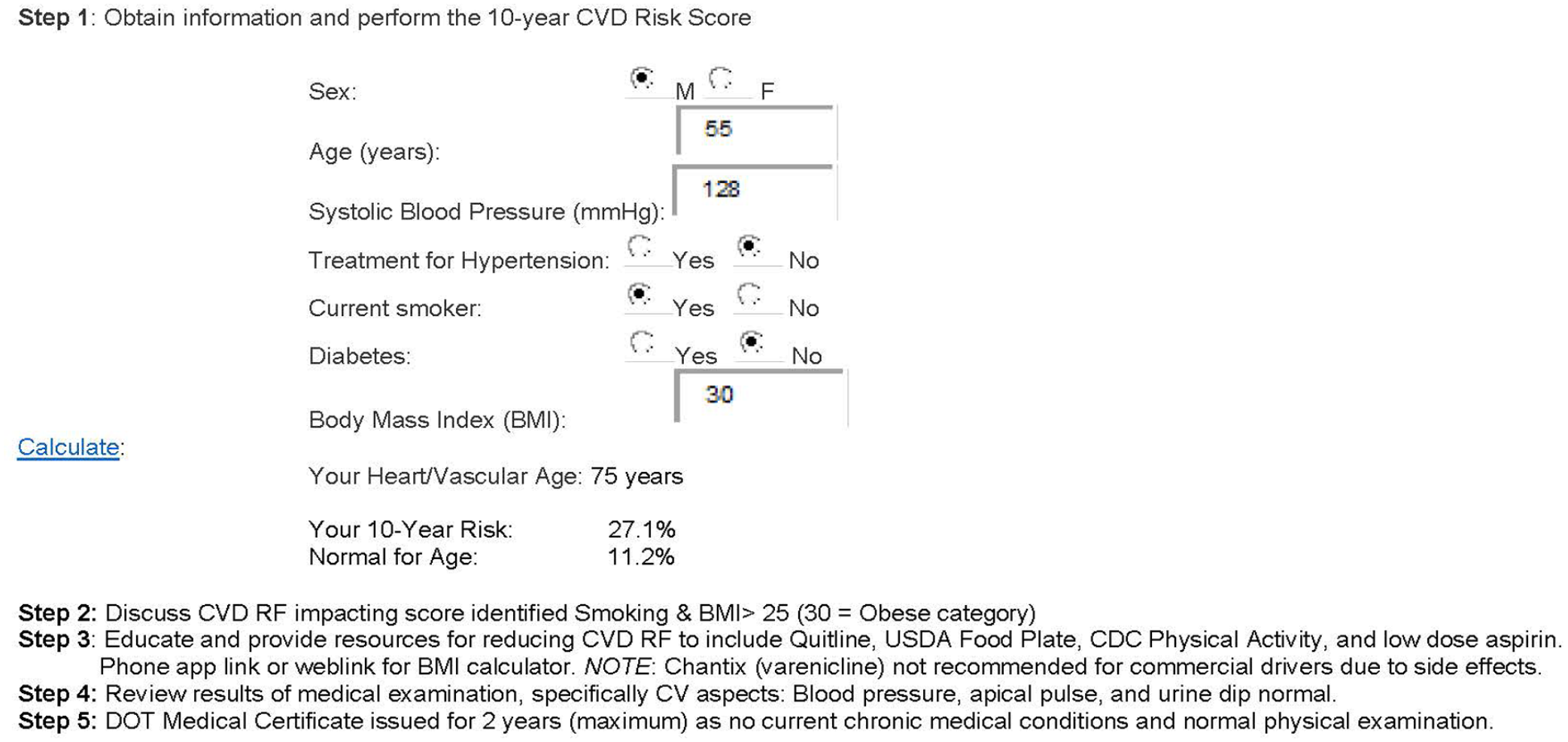
CVD Risk Score Participant Example.
Commercial drivers identified with uncontrolled or new hypertension or diabetes mellitus are referred to PCPs, local health centers, or initially treated if access to care would be delayed. Detection and evaluation of hypertension and diabetes follow CPGs with initial treatment including first-line, generic medications, and minimally necessary laboratory tests (e.g., comprehensive metabolic panel, hemoglobin A1C) at reduced fees to control cost and promote adherence (ADA, 2014, 2022; Whelton et al., 2018).
Results
Chart reviews were completed for consenting commercial drivers following the initial 2-month implementation period to collect data related to demographics, CVD risk score, RF, insurance, and primary care status. Additional chart reviews were completed for commercial drivers seen in a similar 2-month period the prior year related to demographics only. Data analysis for participants during the initial EBP implementation period consisted of descriptive statistics and univariate analysis related to CVD risk, CVD RF, education, and referral or treatment (Barnes, 2015). Formative evaluation included review of participant and staff feedback obtained through visit comments and informal interviews.
Of 89 commercial drivers examined from November through December 2014, 83 or 93% consented and received CVD risk screening. Only one driver indicated prior CVD risk screening through a voluntary, community health screening. Ninety-seven percent (n = 81) of participants were male, aged 21 to 76 with an average age of 49.9 years. The sample population was comparative to 90 drivers examined in November through December 2013 of which 97% were male, aged 21 to 78 with an average age of 50.6 years, thereby supporting the generalization of findings to the occupational practice’s population. With ongoing implementation since 2014, most of the drivers receiving the CVD risk screening continue to be males over 40 years of age, which is comparable to commercial drivers in the United States being 91% male with an average age of 41 years (Zippia, 2022).
CVD Risk and Age-Related Findings
During initial implementation, the 10-year CVD risk scores calculated for the eighty-three participants ranged from 1.1% to 85.5%. Younger drivers, aged 21 to 39 years, had 10-year CVD risk scores below or equal to normal risk. A significant increase in participants’ CVD risk scores began at age 40 with commercial drivers’ CVD risk scores significantly higher than normal risk for age groups 50 to 59, 60 to 69, and 70 to 79 years (Figure 5), which is consistent with research reporting age as an independent risk factor for CVD (Rodgers et al., 2019). The average CVD risk score was significantly higher than anticipated at 18.8% for the 83 participants, almost double the 9.7% of the general population per the risk score calculator.
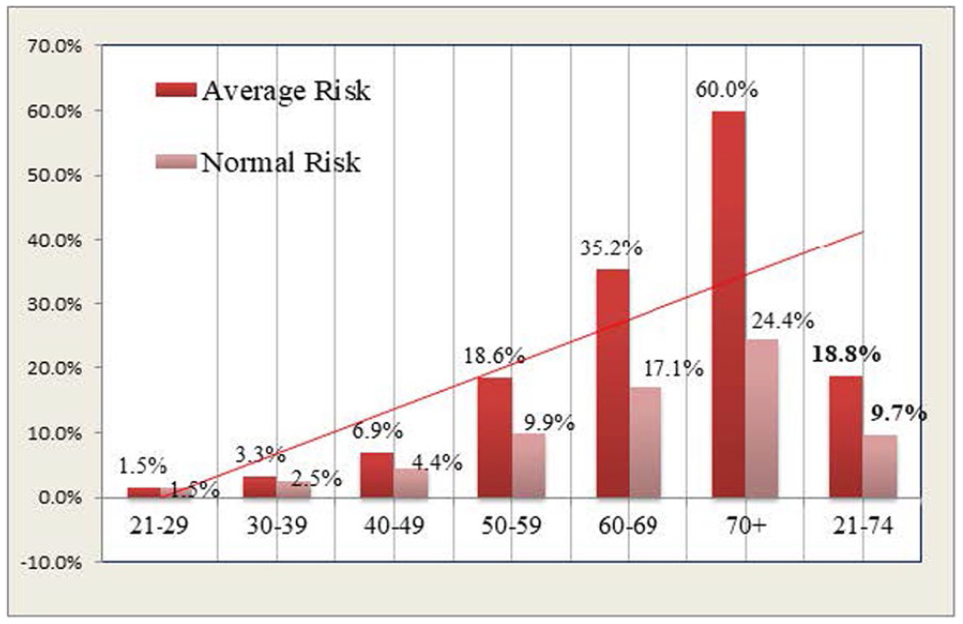
Average Cardiovascular Disease (CVD) Risk Score by Age Group.
Stratification of participants’ 10-year CVD risk scores yielded 39% (n = 32) at low risk, 22% (n = 18) at intermediate risk, and 40% percent (n = 32) at high risk. Risk stratification and comparison to normal and optimal risk scores were shared with each participant with the emphasis on reducing individual CVD RF. With continuing implementation, a shift in the 10-year CVD risk scores of participants has been noted with more scores falling in the intermediate risk category during the past few years. This shift could be due to decreased smoking rates and longer periods of physical activity noted for men; although e-cigarettes and vaping need to be considered regarding long-term, adverse CVD effects for this population (Cho et al., 2022; Münzel et al., 2020).
CVD Risk Factors and Preventive Behaviors
Body mass index of 25 or greater identified 88% of initial participants (n = 73) as overweight or obese, and 30 participants had elevated BMI as the only CVD RF. Other identified CVD RF were hypertension (n = 28), smoking (n = 18), diabetes (n = 11), and systolic blood pressure above 139 mmHg (n = 8). Over 50% (n = 46) of the drivers had two or more CVD RF, and no driver had all the risk factors.
Reduction of BMI did not significantly reduce the overall CVD risk score when demonstrated using the calculator; however, BMI >30 or obesity has been related to a higher incidence of CVD (Khan et al., 2018). Therefore, reduction of BMI is routinely encouraged with healthy weight ranges discussed, based on current guidelines (CDC, 2022a).
Control of hypertension and diabetes without medication reduced the 10-year CVD risk score by 3% to 5%, respectively. Smoking cessation had the most impact on the CVD risk score, reducing it by up to 50%; this impact is demonstrated to participants who smoke using the risk calculator.
Recommendations for starting or continuing low-dose aspirin therapy followed the U.S. Preventive Task Force guidelines and were initially provided to women aged 45 to 69 (n = 2) and men aged 45 to 79 (n = 52). Drivers are advised to discuss risk versus benefits of low-dose aspirin therapy with their PCP or cardiologist, if under care. Drivers without insurance or primary care are advised of risk versus benefit and contraindications to low-dose aspirin therapy that includes history of bleeding or gastrointestinal problems (USPSTF, 2009). Updated guidelines for preventive low-dose aspirin therapy are currently utilized when providing RF recommendations for drivers aged 40 to 69 years (USPSTF, 2022).
Treatment and Referrals
For the initial 83 participants, no drivers were identified or treated for new-onset hypertension or diabetes. Of eight participants with elevated systolic blood pressure, ranging from 140 to 160 mmHg, four were under care, three were referred to primary care, and one participant without insurance or PCP was followed without need for medication. Of 11 participants with known diabetes, no findings on the examination necessitated immediate referral or treatment.
All commercial drivers identified with intermediate or high CVD risk (n = 50 in initial group), or age 30 years or older, are encouraged to obtain health insurance and a PCP for routine preventive care. Drivers without insurance or PCP are advised of services in the local area including two federally qualified health centers (FQHCs). Short-term follow-up is provided in the occupational practice for drivers with newly diagnosed hypertension or diabetes mellitus until primary care is established.
Insurance and Primary Care Provider Status
Of the 83 commercial drivers screened in 2014, 25% (n = 21) were uninsured, and 32% (n = 27) did not have a PCP. From the literature review, it was estimated that 30% to 40% would be uninsured; therefore, the lower percentage could have reflected utilization of federal and state health insurance programs enacted in 2014 and early 2015.
Enrollment in a plan through the Health Insurance Marketplace increased from 3.8 million people in 2013 to 14.5 million in 2022; however, many plans remain costly for independent or contracted drivers (Kaiser Family Foundation, 2022). Since early 2020, decreased access to primary care secondary to the coronavirus pandemic significantly increased participation of drivers in CVD screening in the occupational practice and collaboration with PCP (Tuczyńska et al., 2021). As utilization of preventive services can increase early detection of CVD and RF modification education, access to primary care for drivers remains extremely important. Although screening is only the first step in comprehensive care to address CVD morbidity for this high-risk population, applying the 10-year risk assessment through “improvements in health systems approaches” is identified as the most critical step (Agency for Healthcare Research and Quality, 2022; Lloyd-Jones et al., 2019, p. e1173).
Discussion
Implementation of evidence-based CVD screening for commercial drivers in the occupational practice requires knowledge of CPGs, screening tools, advanced physical assessment, pharmacologic therapies, non-pharmacologic therapies, and patient education resources. Practice issues that could decrease effective CVD screening are addressed through identification of referral resources, staff education regarding EBP goals, and inclusion of drivers over age 21 as potential participants for screening. Transfer of evidence-based knowledge into practice supports standards of occupational professional practice including assessment, diagnosis, implementation, professional development, and collaboration (AAOHN, n.d.; ACOEM, 2021). Regular review of evidence-based guidelines regarding CVD risk screening and RF education serves to sustain the practice change.
Of note, the federal Medical Examination Report Form MCSA-5875 (FMCSA, n.d.) for commercial drivers no longer requires identification of gender, although sex disparities have increased among younger adults due to “worsening BP (i.e., blood pressure) and smoking status for men, and worsening physical activity for women” that could significantly affect CVD risk (Cho et al., 2022, p. 6). However, review of social determinants of health (SDOH) such as socioeconomic status and access to care along with promoting early adoption of health behaviors (i.e., physical activity, stress reduction, social support, not smoking) promote gender equality in CVD risk reduction efforts as providers also consider the impact of biological research (O’Neill et al., 2018).
Cost of EBP Implementation
Financial considerations for EBP implementation were reviewed. Staff education for registered nurses (RNs) and medical assistants in the occupational practice takes approximately 1 hour at an estimated cost of $15.00 per person. Review of a driver’s health history, smoking, height, weight, blood pressure, and urinalysis results (i.e., glucose, protein, blood) are routinely completed; therefore, calculating BMI requires minimal time using an online calculator or manual tool. Experienced CMEs have sufficient knowledge and experience to provide the CVD screening and patient education without an impact on time or cost. Discussion of the 10-year CVD risk score is easily integrated into the CME’s overview of examination findings with each participant. Patient education on CVD RF provided by the CME uses standardized resources at low or no cost, at an average of three handouts per participant. A participant letter is easily completed to summarize CVD RF, again requiring minimal time using a checklist format.
The overall cost of implementation is estimated at $16.00 per participant; however, staff concurred that CVD risk assessment is easily incorporated within the normal time of 15 to 20 minutes for each medical examination. Only minor cost for printing educational materials had been incurred by the occupational practice with no increased cost to commercial drivers or employers. Adjustment to cost should be considered based on the salary of participating staff, experience of the CME, and if future screening guidelines recommend a laboratory component (i.e., cholesterol tests) requiring an alternate screening method. Additional cost considerations could include delegation of the CVD screening and RF feedback to a RN or Certified Occupational Health Nurse (COHN) which would decrease the CME’s initial time.
Staff and Participant Feedback
The occupational practice concluded that implementation of the CVD risk screening is logical, efficient, and cost-effective to complete during the commercial drivers’ mandated medical examinations. Recommendations from staff to enhance CVD risk screening have included delegating risk score calculation to trained staff, encouraging screening for drivers without insurance or PCP, and developing an EHR template with an embedded score calculator.
The 10-year CVD risk score has been well received by commercial drivers, and participants routinely express gratitude for the time taken to provide screening and education which further serves to sustain the practice change. This positive feedback is consistent with participant feedback during large-scale screening efforts in occupational settings with an emphasis on collaboration with primary care for consistent recommendations (DiBattista et al., 2019).
Strengths, Limitations, and Barriers
Factors that hinder EBP implementation have been identified as competing priorities, lack of time, and decreased awareness of the impact on health outcomes (Melnyk and Fineout-Overholt, 2019). Therefore, the occupational practice identified a validated, simple tool and included standardized patient education that provides relevant information that could affect a driver’s future ability to work. Using guidelines and EHR reminders have been significant facilitators of EBP; therefore, reminders are included in the electronic scheduler and linked to visits for “Commercial Driver (DOT) Physical” and “School Bus Driver Physical” to ensure drivers are consistently offered the CVD risk screening.
Potential barriers to implementation included staff’s limited knowledge of EBP, new patient–provider relationships, limited time for medical examinations, privacy issues, and limited EHR utilization. These issues are addressed through staff training, non-invasive CVD risk screening, rapid development of trusting relationships, participant consent (i.e., signed, verbal), and use of EHR clinical data for some RF (i.e., past medical history). Additional implementation barriers include the limitation of the online CVD calculator for younger adults (i.e., 21–29 years), multiple CVD risk factors, specialty care (i.e., cardiology), internet downtime, and walk-in clients. Barriers are addressed through discussion of identified CVD RF and routine care with established providers, use of an Excel CVD risk calculator during internet downtime, and scheduling appointments for walk-in clients when not urgent. Consideration of CVD risk screening for commercial drivers using telehealth or conducted by a RN or COHN as part of a corporate wellness program could also address these barriers and provide more time for follow-up. However, the focus of this EBP project was providing CVD screening during opportune visits in the occupational practice.
Staff education is crucial to EBP implementation, and formal training included an emphasis on staff roles and goals of the practice change to enhance care for the population. Training has been routinely updated and provided to nurses and medical assistants since 2014. Positive perceptions toward the practice change, willingness to facilitate screening, high self-efficacy of staff, and use of a low-cost screening tool have promoted sustainability of the CVD risk screening for commercial drivers. Other factors that have facilitated EBP implementation include an experienced CME, minimal time for screening with the non-invasive process, established collaborative relationships, standardized educational resources, and receptive participants.
Identifying CVD risk for commercial drivers supports professional standards to implement EBP and develop surveillance programs in occupational practices that prevent or reduce the incidence of disease (AAOHN, n.d.; ACOEM, 2021). With ongoing review of CVD screening guidelines, occupational professionals can identify and address gaps in primary care, improve overall health of a high-risk population, and promote access to primary screening. The American Rescue Plan Act of 2021 asserted it would eliminate healthcare insurance premiums; therefore, assessment regarding insurance and PCP access among the population should continue (The White House, 2022). Overall, providing CVD risk screening and education to reduce RF education for commercial drivers examined in occupational practice serves to champion the health of essential workers, enhance preventive care delivery, and ensure public safety.
Applications to Professional Practice
The incidence of cardiovascular disease (CVD) in the United States has decreased significantly in the past 40 years; however, it remains the major cause of death, disability, and healthcare costs for working adults. Commercial drivers have a significantly increased risk of CVD that negatively affects their overall health, the workforce, and public safety. Implementing evidence-based practice (EBP) of CVD risk screening for drivers using a non-laboratory method during mandated medical examinations in occupational practice was found to be logical and sustainable with minimal impact on workload, time, or cost even in consideration of managing multiple priorities. Including CVD screening enhances national health promotion strategies to fill a gap in preventive care for these essential workers that may not be identified otherwise. Routine CVD risk screening and education regarding modifiable risk factors supported occupational professional standards for EBP implementation during opportune encounters with this high-risk population.
Footnotes
Acknowledgements
Special acknowledgment and thanks to Dr. Dorothea Winter, Professor of Nursing, who served as the author’s Doctor of Nursing Practice (DNP) Project faculty advisor during the initial implementation, evaluation, and internal dissemination period from September 2014 through May 2015 and provided invaluable guidance for successful completion.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Human Subjects Review
Approval for the initial implementation as a Doctor of Nursing Practice (DNP) Project was provided by the Institutional Review Board (IRB) at Salisbury University on November 5, 2014, Protocol #32.