
Abstract
Obesity is recognized as a national and global health epidemic. Commercial truck drivers (CTDs) have a higher obesity rate and lower life expectancy compared with the general population. CTDs work sedentary jobs with long hours that pose barriers to healthy eating and regular exercise. An evidenced-based practice (EBP) change project that used motivational interviewing (MI) and education regarding diet and exercise over a 4-week period was found to have a positive impact on CTDs behavior. Results revealed an increase in aggregated self-efficacy for weight loss (14.8%, exceeding the benchmark of 11%). For aggregated body mass index (BMI), CTDs lost a mean of 0.65 kg/m2, over a 4-week period which was statistically significant at p = .0001. The results suggest a short-term MI intervention can be effective when implemented as a clinical standard for CTDs.
Keywords
Obesity is a growing public health concern affecting all ages and socioeconomic groups both nationally and globally; the United States has the highest prevalence of obesity in the world (Wills, Fehin, & Callen, 2011). In the United States, commercial truck drivers (CTDs) have a 15% higher rate of obesity compared with the general population (Apostolopoulos, Sonmez, Shattell, Gonzales, & Fehrenbacher, 2013). The clinical problem of obesity among CTDs is a leading health indicator with both national and global implications (Parks, Chikotas, & Olszewski, 2012). To address the problem of obesity in CTDs, an evidenced-based practice (EBP) change project was implemented over a 4-week period. The project used motivational interviewing (MI) and education about diet and exercise to improve CTDs’ self-efficacy and decrease participants’ body mass index (BMI).
Background
Obesity is a precursor of mortality and chronic illnesses in the United States and worldwide. At least 2.8 million individuals die each year as a result of overweight and obesity (World Health Organization, 2015). According to the Centers for Disease Control and Prevention (CDC; 2015a), obesity is measured using BMI, calculated by dividing weight in kilograms by the square of height in meters (kg/m2). The CDC considers a BMI of 30 or greater as obese. Interestingly, Faghri and Buden (2015) have identified a positive association between workers’ BMI and stressful job schedules and work conditions.
Sedentary lifestyles, availability of food, and larger portions of food are the main causes of weight gain in Americans (Fisher & Al-Oballi Kridli, 2014). Commercial truck driving is considered a sedentary job with long hours sitting and driving. The sedentary nature of driving long hours predisposes CTDs to limited physical activity and unhealthy food choices leading to weight gain and obesity. Lemke and Apostolopoulos (2015) reported that life expectancy for CTDs is 16 years less than the general population; Thompson (2007) reported CTDs have a 30% to 50% greater chance of developing chronic health conditions (e.g., myocardial infarction, cerebrovascular accident [stroke], diabetes, obstructive sleep apnea, hypertension, and hyperlipidemia; CDC, 2015b). These conditions are costly and significantly higher for obese CTDs at US$1,944 annually compared to US$1,131 for truck drivers of normal weight (Martin, Church, Bonnell, Ben-Joseph, & Borgstadt, 2009).
Motivational interviewing (MI) is one approach found to positively impact obesity. MI is a form of behavior therapy that can result in individual behavior change in some situations. Individuals are guided by a professional in setting goals to achieve behavior change. During MI sessions, individuals discuss how to achieve behavior change, the importance of reaching goals, and the consequences of choosing not to change behaviors. Low, Giasson, Connors, Freeman, and Weiss (2013) noted that MI is a method of behavioral counseling that impacts obesity by supporting positive behavior change and may benefit those workers who perceive obstacles to losing weight, and are resistant to changing behaviors.
Literature Review
Through a comprehensive review of the literature, MI was validated as a clinical intervention to promote weight loss. Several studies found that when motivation and self-efficacy were both addressed, both concepts were key indicators in weight loss and healthy lifestyle (Fisher & Al-Oballi Kridli, 2014; Greaves et al., 2008; Hardcastle, Taylor, Bailey, & Castle 2008; Low et al., 2013; Meybodi, Pourshrifi, Dastbaravarde, Rostami, & Saeedi, 2011; Vanbuskirk & Wetherell, 2014; Warziski, Sereika, Styn, Music, & Burke, 2008; Wong & Chen 2013).
A systematic review by VanBuskirk and Wetherell (2014) evaluated 12 randomized controlled trials (RCTs) with nine positive results for MI and weight loss. The meta-analysis of body weight reduction from the RCTs found a mean effect size of 0.47 that approached significance (p = .07). Overall, the findings indicated that MI was effective at promoting behavior change to achieve weight loss, and the researchers suggested as few as one MI session could be effective.
Similar to MI, evidence supported self-efficacy for weight loss. An 18-month behavioral weight loss study by Warziski et al. (2008) examined a total of 170 individuals’ level of self-efficacy, meaning their ability to maintain a diet and lose weight. The outcome of the study revealed that self-efficacy was associated with weight loss (p = 0.02), and an average weight loss of 4.64% of baseline weight was achieved as well as an 11.7% increase in self-efficacy. According to Miller and Rollnick (2002), self-efficacy is an essential component of MI.
Meybodi et al. (2011) investigated the effectiveness of MI to increase self-efficacy for weight loss. Thirty overweight and obese Iranian women were randomized to either an MI intervention group or control group. The MI intervention group received four MI sessions, and the control group did not receive any intervention. After 2 months, the participants in the intervention group showed significant reduction in BMI (p = .001) and improvement in self-efficacy (p < .05).
Method
A 12-week institutional review board (IRB)–approved EBP change project was conducted in a health clinic located in eastern Pennsylvania. Workers employed at a global battery manufacturing plant were invited to participate in the project if they were age 18 years or older, male or female, and inclusive of all races and ethnicities. Participants were recruited through flyers and posters displayed at the clinic and the plant. Approximately 400 CTDs were employed at the plant and receive care at the clinic. Total time requested of each participant was approximately 2 hours over a 4-week period. The project implementer (PI) met with each participant individually during the first week of the project when the initial MI and educational sessions were scheduled. During the following 2 weeks, the PI called each participant to evaluate their progress, offering support and guidance. During the fourth week, the PI met in person with each participant for a final individual MI session to review individuals’ progress, reinforce goals, distribute educational materials, and address any questions participants had. The overall goal of the project was to increase self-efficacy and decrease BMI.
A modified version of the Weight Efficacy Lifestyle Questionnaire (modWEL-tool) was used to measure self-efficacy pre- and post-MI intervention. The modWEL-tool is comprised of 24 questions using a 10-point Likert-type scale. Participants were asked to quantify self-efficacy on a scale of zero (0) to nine (9), with 0 being no confidence and 9 being complete confidence. For scoring purposes, the questions were grouped in seven subscales: Negative Emotions, Availability, Social Pressure, Physical Discomfort, Positive Activities, Exercise, and Genetics. Mean modWEL-tool total scores were computed by summing all items and dividing by the total number of items. Subscale scores were computed by summing the items for each of the seven subscales and dividing by the number of items in the subscale. Overall group mean scores were calculated by summing all participants’ scores and dividing by 24, the number of questions. Individual subscales were calculated by summing item scores for each subscale and dividing by the number of items for each subscale. The tool was administered during the first and last individual MI sessions.
Schulz and McDonald (2011) modified the original Weight Efficacy Lifestyle Questionnaire (modWEL-tool), adding four questions related to exercise and genetics to create a 24-item questionnaire. By adding four questions, information was gathered specific to exercise and genetics. The authors noted that using the modWEL-tool did not change the internal consistency of the tool (Cronbach’s α = .93). In 2015, Ames, Heckman, Diehl, Grothe, and Clark also demonstrated statistical and clinical validity for the original Weight Efficacy Lifestyle Questionnaire (WEL-tool) for measuring self-efficacy related to weight loss in multiple studies.
The original WEL-tool was created in 1991 by Clark, Abrams, Niaura, Eaton, and Rossi to assess individual self-efficacy for weight loss; the tool has been used in multiple studies for over two decades. The WEL-tool measures individuals’ confidence or self-efficacy to control eating behaviors with higher scores reflecting greater self-efficacy. The WEL-tool has been found to have acceptable validity (p < .05) and reliability (p < .05-.0001) in several studies (Ames et al., 2015; Clark et al., 1991; Hays, Finch, Saha, Marrero, & Ackerman, 2014; Rejeski, Mikhalko, Ambrosius, Bearon, & McClelland, 2011). Content validity was confirmed by Ames et al. (2015) and Cronbach’s alpha of .92 established internal consistency reliability.
Participant’s height, weight, and BMI were calculated at the first and last individual MI sessions. Paired t tests were used to determine whether changes in BMI and self-efficacy were achieved. A p value of .05 indicated statistical significance.
Theoretical Framework
Key to the design of the project was the Rosswurm and Larrabee model (1999), a framework to guide project design. The model offered organized steps that have been used successfully in primary care settings which are similar to some occupational health settings. The six steps of the Rosswurm and Larrabee model include assessment, linking the problem to the intervention, synthesizing evidence, designing change, and evaluating change. Basically, the model guided the practice change by linking the clinical problem to an intervention, providing structure for implementation of the intervention and the evaluation, and disseminating outcomes.
A second framework used to guide project design was Bandura’s social cognitive theory (SCT) which evolved from his original social learning theory (Bandura, 1977). Bandura’s SCT focuses on the learner’s cognitive perspective and the components of self-regulation and self-efficacy (Bandura, 1977). Principles of behavior modification originated from SCT in which person, environment, and behavior interact reciprocally (Butts & Rich, 2011). Bandura believed self-efficacy to be the most important and influential aspect of behavior change (Bandura, 1977). Self-efficacy refers to individuals’ confidence in their ability to successfully reach a goal by being motivated to overcome obstacles (Zulkowsky, 2009). Self-efficacy can increase or decrease motivation to achieve a goal. The goals for this EBP change project were to increase self-efficacy, promoting weight loss and reduction in BMI.
Butts and Rich (2011) explained that individuals learn health behaviors within the context of family and community; health behaviors are influenced by the environment. The most important component of behavior change is individuals’ perceptions of their state of health, and the role of occupational health nurses includes raising awareness of healthy behaviors and supporting behavior change (Butts & Rich, 2011). The application of SCT to practice was applied to this project when occupational health nurses offered MI to CTDs to increase self-efficacy, ultimately affecting CTDs’ ability to decrease BMI.
Results
Nineteen of 400 CTDs volunteered and completed the project, a response rate of 4%. All participants were male, between the ages of 26 and 69 years (mean age: 44.8 years). Reported ethnicity was 95% (n = 18) Caucasian and 5% (n = 1) Hispanic.
Differences between initial and final aggregate BMI were calculated and then compared with an accepted benchmark (i.e., a decrease in BMI of 0.5 kg/m2). For this population, average height is 70 inches, so a decrease in BMI of 0.5 kg/m2 is equivalent to 3.5 pounds of weight loss. Across the expected range of height for this project (60-80 inches), a decrease in BMI of 0.5 kg/m2 is equivalent to 2.6 to 4.5 pounds of weight loss. The CDC (2015c) recommended healthy weight loss as 0.5 to 2 pounds per week (2-8 pounds over a 4-week period), which included the range of weight loss targeted as the benchmark for this study.
The second outcome was an increase in CTD self-efficacy. A benchmark was established based on two studies that explored self-efficacy and weight loss using the WEL-tool questionnaire. The studies found similar results with an approximately 11% increase in total questionnaire scores reflecting an increase in self-efficacy (Hays et al., 2014; Warziski et al., 2008). Based on these outcomes, an aggregate mean of 11% increase in the postintervention group total scale score was used as the benchmark for overall self-efficacy.
Table 1 presents total and subscale aggregate mean scores for weight, BMI, and self-efficacy. Statistically significant results were found for weight and BMI (p < .0001) and total self-efficacy (p < .0002). Interestingly, six of the seven subscales were also statistically significant with p values ranging from .0002 to .038. The one subscale that was not statistically significant was Genetics. Figure 1 displays percentages of participants who (a) gained weight (>0.5 kg/m2 increase in BMI), (b) maintained weight (stayed within 0.5 kg/m2 of baseline BMI), or (c) lost weight (<0.5 kg/m2 decrease in BMI). Overall, 84% of participants showed improvement.
Mean Change in Self-Efficacy Items From Before and After Motivational Interviewing Among CTDs (n = 19)
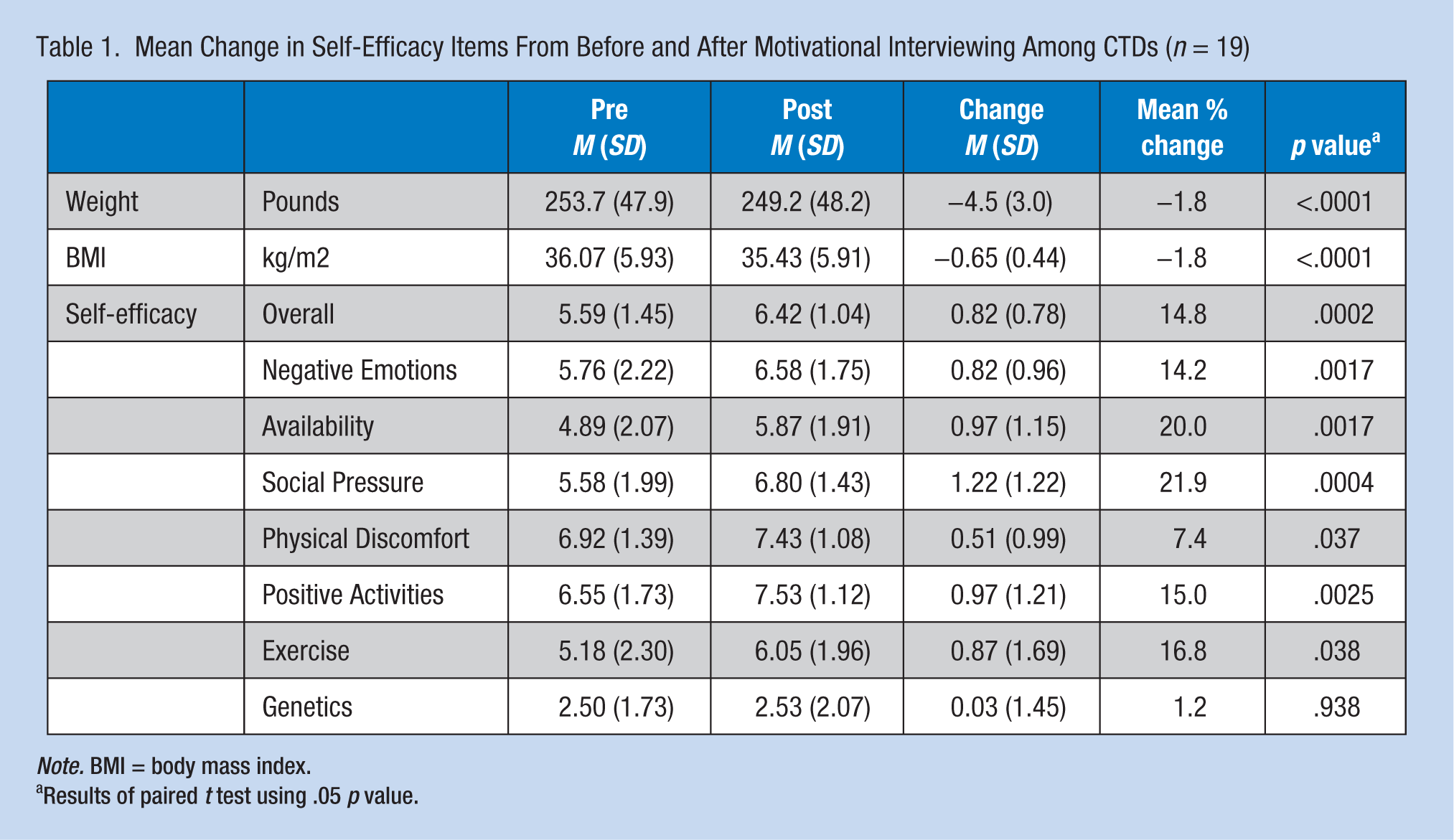
Note. BMI = body mass index.
Results of paired t test using .05 p value.
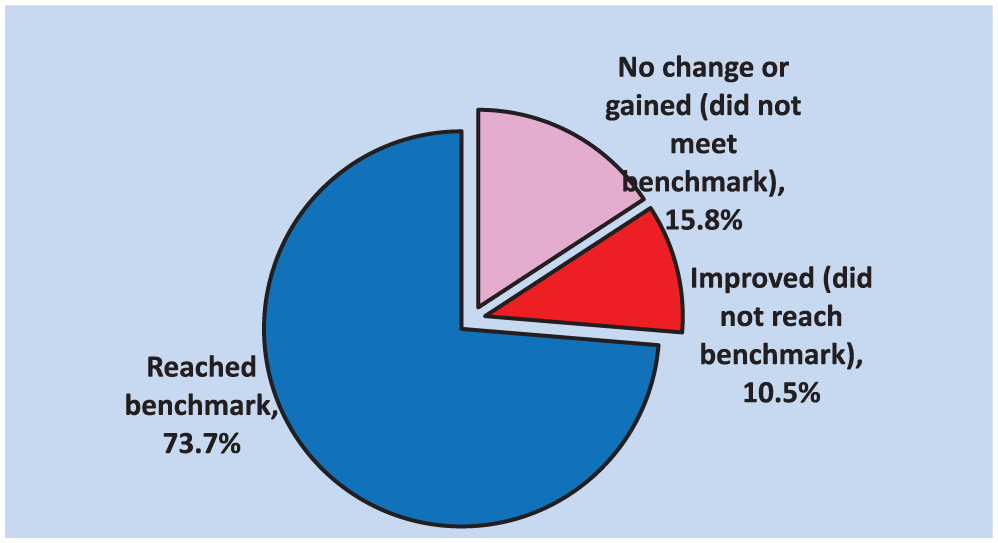
Percentage of participants with change in BMI.
The second outcome was to achieve an increase in overall self-efficacy. Figure 2 displays percentages of participants who did or did not have changes in overall levels of self-efficacy. The figure reflects calculated percentages of participants who (a) had a decrease in overall self-efficacy, (b) had small increases in self-efficacy (<11% increase), and (c) had large increases in self-efficacy (>11% increase). Of the 19 participants who completed the project, 52.6% reached benchmark. In addition, 31.6% of participants experienced an improvement in overall self-efficacy but did not reach benchmark. In overall group comparison, the mean change in overall self-efficacy was 14.8%, which was greater than the benchmark of 11%. Paired t tests suggested the changes in overall self-efficacy were statistically significant (p = .0002).
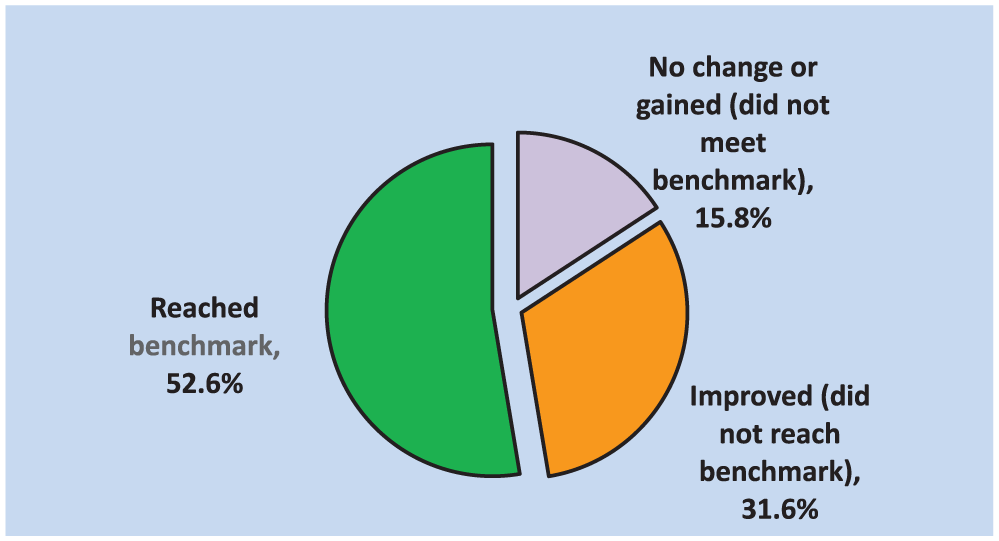
Percentage of participants with change in overall self-efficacy.
In summary, the majority of participants (52.6%) met the benchmark of 11% increase or greater in self-efficacy as well as 73.7% of CTDs met the benchmark for BMI reduction. Pretest and posttest self-efficacy showed a statistically significant increase of 14.8%, greater than the benchmark (p = .0002). Paired t tests of grouped means (self-efficacy) revealed statistically significant differences (p < .05) in total outcomes for six of the seven subscales of the modWEL-tool questionnaire including Negative Emotions, Availability, Social Pressure, Physical Discomfort, Positive Activities, and Exercise.
Discussion
The project was successfully implemented but did require modification to the original plan. The PI determined that the original recruiting timeline needed to be extended from 7 weeks to 9 weeks, due in part to the summer timeframe for project implementation and many CTDs and health center staff on vacation. Fortunately, no limitation to the recruitment timeline was included in IRB approval. Another challenge was scheduling CTDs. Due to the nature of the CTDs’ erratic travel schedules, PI flexibility was required; the PI saw participants when it was convenient to their schedules. Often, visits and phone calls with CTDs were scheduled early in the morning, late in the evening, or on weekends to accommodate schedules. Having only one health care provider for this project was another challenge and not necessarily practical due to the need for flexibility with CTDs’ schedules. Another limitation was the homogeneity and small sample size of the study sample, for 19 of the participants were Caucasian males. Finally, the participant population may not represent all CTDs and all companies that employ CTDs; the feasibility of applying an MI intervention to every CTD worksite has not been determined. These limitations create uncertainty as to whether the same outcomes would be achieved for CTDs employed in other organizations.
Due to the time constraints of the 14-week project plan, the PI was unable to extend the intervention with the CTDs. More studies are needed to validate the effectiveness and sustainability of MI to promote weight loss with CTDs. The PI recommends that additional MI sessions be offered as well as data collection at 3 months, 6 months, 9 months, and 1 year post intervention. Engagement, support, and relationship-building that may occur with more MI sessions and monitoring could promote sustained weight loss for CTDs.
The PI used various forms of technology to enhance EBP outcomes. For example, the PI introduced several diet and exercise apps and exercise videos on YouTube. The PI used an iPad to review and discuss recommended websites and apps for diet and exercise education. After completion of the EBP change project, the PI recommended several services offered by the employer to sustain weight loss. The CTDs could take advantage of discounted services provided by the employer such as national and local gym memberships and Fitbit purchase discounts. In addition, the employer offered CTD participants who completed the project paid registration fees for Weight Watchers (WW) online to assist in sustaining success with their weight loss goals. The WW program offers mobile tools such as an app that tracks individual food intake, weight, and exercise. This type of technology provides convenience for individuals who travel. The sustainability of weight loss and obesity management for CTDs is vital to the health and safety of this population.
The positive findings from this EBP change project add to the potential knowledge occupational health practitioners can extend to current employees whose jobs require travel for extended periods of time or who have limiting physical activity opportunities. Occupational health practitioners must consider the needs of all employees in the workplace to prevent and treat obesity.
Future Implications for Clinical Practice
Future practice implications from this project revealed that MI can promote health behavior change in clinical and worksite settings and should be considered to address obesity for mobile populations. The use of various forms of technology (e.g., cell phones and apps) should also be considered when addressing worker obesity. Occupational health practitioners can engage mobile employee populations (e.g., CTDs and marketing and sales personnel) by using technology to provide education and monitoring. For example, the occupational health practitioner could reach CTDs with text messages to schedule MI sessions. MI sessions along with diet and exercise education could be offered using a tablet or laptop that had voice over Internet protocol (VoIP) broadband capability. Internet videos can support diet and exercise education, and apps could be used to track progress with weight loss. These strategies could improve worker engagement challenged by travel schedules.
Using MI in combination with diet and exercise education, and technology to engage participants in healthy decision making is a cost-effective and easy-to-implement solution to the obesity epidemic. These interventions should be considered useful not only to CTDs but also for the population at large.
Conclusion
An EBP change project was conducted at a workplace with CTDs. MI is a compelling intervention that can reduce obesity. MI explores individuals’ motivations to change health-related behaviors by asking questions to determine desire, ability, reasons, and need for change (DARN; Miller & Rollnick, 2002). MI supports self-efficacy, a prerequisite for changes in diet and exercise. Overall, the project was an effective approach to increase self-efficacy and reduce BMI.
Footnotes
Acknowledgements
The authors gratefully acknowledge the consultation, participation, and contributions of Laurie Heagy, MPH, RN, COHN-S, Medical Services Manager, East Penn Manufacturing.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Juanita L. Wilson is an Associate Vice President of Operations for Premise Health managing onsite occupational health clinics across the nation. Dr. Wilson is an AANP board certified nurse practitioner and a Certified Occupational Health Nurse Specialist from the American Board of Occupational Health Nurses. In addition she has a Master of Science degree in Health Care Administration.
Debra M. Wolf is an Associate Professor of Healthcare Informatics and Nursing at Chatham University located in Pittsburgh, Pennsylvania. Dr. Wolf is the Program Coordinator for the Master of Science in Healthcare Informatics (MHI) program. In addition, she is an independent healthcare informatics consultant supporting healthcare institutions and IT vendors integrate new technology into a health setting. Dr. Wolf has published numerous articles, book chapters and coauthored a book titled Social Media for Nurses: Educating Practitioners and Patients in a Networked World.
Kimberly A. Olszewski is the Nurse Practitioner Program Director & Associate Professor at Bloomsburg University in Bloomsburg, PA, and is Vice President and Nurse Practitioner at Mid State Occupational Health Services Inc. in Lewisburg, PA. Dr. Olszewski is an ANCC board certified adult nurse practitioner and is a Certified Occupational Health Nurse Specialist and Case Manager from the American Board of Occupational Health Nurses.