
Abstract
Background:
Assisted falls occur when staff try to minimize the impact of falls by slowing a patient’s descent. Assisting a patient fall may decrease patient injury risk, but biomechanical risk of injury to staff has not been evaluated. Assisted falls virtual reality (VR) simulations were conducted to examine staff low back injury risk during common assisted falls scenarios.
Methods:
VR simulations of a toilet to wheelchair transfer were developed with a male patient avatar for three assisted falls scenarios: standing up from toilet, sitting down on wheelchair, and ambulation. Patient avatar weight was modified to reflect normal, underweight, and overweight adult patients. The average spinal compression force at L5/S1 was calculated for each participant with five trials per three scenarios while utilizing physical ergonomic techniques and compared to the safe spinal compression limit of 3,400 Newtons (N).
Findings:
Six staff participants completed 90 VR simulations in total. The average calculated spinal compression force ranged from 7,132 N to 27,901 N. All participant trials exceeded the safe spinal compression limit of 3,400 N for every assisted falls scenario and avatar weight despite application of ergonomic techniques including wide stance, knees bent, and backs straight.
Conclusions/Application to Practice:
Staff are at risk for low back injury if they assist falls regardless of the adult patient weight and application of ergonomic techniques. Safer alternatives like the implementation of mobility screening tools and safe patient handling and mobility technology are needed to help prevent assisted falls to decrease injury risk to both patients and staff.
Background
The National Database of Nursing Quality Indicators (NDNQI) defines an assisted fall as a “fall in which any staff member was with the patient and attempted to minimize the impact of the fall by slowing the patient’s descent (National Database of Nursing Quality Indicators [NDNQI], 2020).” Studies have reported that 80% to 90% of inpatient falls are unassisted and are associated with higher patient injury rates than assisted falls (Staggs et al., 2014; Venema et al., 2019). These findings may encourage staff to assist falling patients to help decrease patient fall injury risk (Staggs et al., 2014; Venema et al., 2019). However, to our knowledge, there are no studies that performed biomechanical evaluations of staff safety during assisted falls. The Bureau of Labor Statistics (BLS) reported that back injuries accounted for 38.5% of all work-related musculoskeletal disorders (WMSD) in 2016 and contributed to more than half of all injuries among nursing assistants (Bureau of Labor Statistics, U.S. Department of Labor, 2016). In 2020, the BLS reported days away from work for occupational health illness and injury, including for nursing occupations, have risen to a median of 12 days (Bureau of Labor Statistics, U.S. Department of Labor, 2020). The literature indicates that low back injury is the most common WMSD among healthcare professionals, and this could include injuries related to assisted falls (Garg & Owen, 1991; Schulte et al., 2010; Zhang et al., 2020). Excessive spinal compression force is a common mechanism of low back injury, especially at the fifth lumbar (L5) and first sacral (S1) intervertebral disk space and can result in low back pain (Zhang et al., 2020). Occupational health costs of work-related low back pain exceed 100 billion dollars annually in the United States and WMSD prevention is imperative (Zhang et al., 2020).
The National Institute for Occupational Safety and Health (NIOSH) has developed and tested equations to predict staff safety risk for low back injury in the workplace (Waters, 2007). NIOSH endorsed the safe spinal compression limit also known as the action limit of L5/S1 defined as 3,400 Newtons (N) or about 770 pound force (National Institute for Occupational Safety and Health [NIOSH], 1981). At that time, the NIOSH Work Practices Guide applied this action limit to two-handed and symmetrical lifting tasks (NIOSH, 1981). The Occupational Safety and Health Administration (OSHA) and NIOSH support ergonomic techniques to prevent WMSD, such as for staff to stand close to patients with knees bent and feet apart while avoiding back twisting and reaching (Chao & Henshaw, 2009; Cornell University Ergonomics Web, n.d.; Waters, 2007). However, there are no OSHA or NIOSH guidelines specific to ergonomic techniques that would prevent staff low back injury during assisted falls. These organizations recommend comprehensive safe patient handling programs which include ergonomic hazard assessments, appropriate technology, and staff training as opposed to manual lifting (Elnitsky et al., 2015; Waters, 2007). In a sentinel study by Garg and Owen (1991), six nursing students were found to have spinal compression forces at L5/S1 during manual toilet to wheelchair transfers that exceeded 3,400 N for all patient weights (Garg & Owen, 1991). This study evaluated staff low back injury risk during patient transfers and provided a conceptual framework for our spinal compression calculations (Garg & Owen, 1991). The Assisted Falls in Veterans Health Administration (VHA) project addressed the clinical question of whether it is safe for staff to assist a falling patient. Virtual reality (VR) lab simulations were conducted to ensure participant safety during the biomechanical evaluation of assisted falls (Gasteiger et al., 2022).
Methods
Project Overview
The Assisted Falls in VHA project was determined to be quality improvement (QI) by the James A. Haley Veterans’ Hospital Research and Development Committee. VR simulations of common assisted falls scenarios were used to calculate spinal compression forces to correlate to staff low back injury risk (Bulat et al., 2020; Gasteiger et al., 2022).
Simulation Development
The VR simulations of a computer-generated bathroom environment were designed for the Steam platform with Unity, Autodesk Maya, and Adobe software at the University of South Florida Advanced Visualization Center lab. Simulations were developed based on the three most common assisted falls scenarios identified by our qualitative review of VHA patient safety narratives: fall upon standing from toilet, fall upon sitting down on wheelchair, and fall upon ambulation (Bulat et al., 2020). A male patient avatar was programmed to simulate the three most common independent transfer scenarios from toilet to wheelchair in the VR bathroom but did not have communication capabilities. The patient avatar was selected as male to best represent the current older Veteran population in the VHA.
Simulation Variables
Our selected variables during assisted falls were the patient avatar weight and application of physical ergonomic techniques to explore staff low back injury risk during toilet to wheelchair transfers. Ergonomic techniques are defined as body postures, positions, and movements that promote comfort and protection in the work environment and potentially reduce excess motion and forces (Chao & Henshaw, 2009). Patient avatar anthropometric data were obtained from the National Health Statistics 2015 to 2016 mean height and weight for men 20 years and over (age-adjusted rates) for the 50th weight percentile (overweight Body Mass Index [BMI]) (Fryar et al., 2018). The patient avatar was programmed at 1.76 meters (~69 inches) for height and 89 kg (~196 pounds) for weight (50% percentile American adult male) in the VR simulation for all 3 scenarios (Fryar et al., 2018). The spinal compression forces were then calculated for 10th and 25th weight percentiles for an American adult male (Fryar et al., 2016). Centers for Disease Control and Prevention (CDC) anthropometric data from 2011 to 2014 were obtained for 10th (underweight BMI) and 25th (normal weight BMI) weight percentiles that reflected males ages 80 years and older for whom toilet to wheelchair transfers may be most applicable (Centers for Disease Control and Prevention [CDC], 2021; Fryar et al., 2016). Patient avatar weights for BMI 30 and over were excluded given staff manual lifting of bariatric patients is discouraged in the literature and clinical practice due to higher risk of WMSD (CDC, 2021; Waters, 2007).
Simulation Participants
VR simulation participation (N = 6) was completed voluntarily by interested interdisciplinary staff with expertise in nursing or patient safety from our QI project team at James A. Haley Veterans’ Hospital. Information collected from staff participants included: age, sex, height, weight, and calculated BMIs.
Simulation Ergonomics
Ergonomic techniques regarding optimal staff body postures, positions, and movements were applied to VR simulations for best approaches to assist falling patients based on resources from NIOSH, OSHA, and an ergonomic specialist (Chao & Henshaw, 2009; NIOSH, 1981). The ergonomist trained staff participants immediately prior to VR simulations to stand with a wide symmetrical stance close to the patient avatar, maintain knees bent, tighten abdominal muscles, and straighten backs (Chao & Henshaw, 2009; NIOSH, 1981). Ergonomic techniques entailed for staff to step forward in a staggered stance, simulate embracing the falling patient avatar with a hugging position, and during ambulation to simulate lowering the patient avatar with their front leg in between the patient’s legs (Burke, n.d.; Chao & Henshaw, 2009; NIOSH, 1981). The ergonomist recorded these instructions on paper and short video demonstration that were displayed to participants prior to VR simulations and read the instructions out loud and answered questions.
Simulation Data Collection
The VR simulations utilized the Valve Index Kit that included two hand controllers, base, and headset tethered to a PC Windows 10 operating system. The VR floor space occupied three meters squared with two base stations aimed toward the center of the VR area with headset cords hung on an overhead rolling board. The assisted falls VR lab data collection began with the operator ensuring that each participant was positioned in the VR space for the initial calibration. Participant height and weight measurements were collected to determine their center of gravity. The distance from the shoulder at the acromion process to the wrist and spinal length from the seventh cervical to first sacral spine were measured for each participant. HTC VIVE trackers were strapped to the participants’ bilateral ankles, bilateral knees, bilateral shoulders at the level of the acromion processes and at L5/S1 spine level. The trackers were numbered to correlate to data points in the Windows 10 operating system for data analysis.
The operator manually initiated the patient avatar falls on the computer-generated bathroom scene once the participants indicated they were ready to begin the scenarios. The patient avatar fell during standing up from toilet, sitting down on wheelchair, and ambulation between toilet to wheelchair VR simulations. Each participant performed five trials for the three scenarios to permit data calculations of spinal compression forces. The VR simulation captured positional, rotational, and impact/collision data at every 10th of a second and stored as CSV files on the PC for data analysis. The collision data provided the reference time of when the firsthand controller of each participant contacted the patient avatar during the assisted falls. The positional data set provided three coordinates labeled x (horizontal axis), y (vertical axis), and z (rotational axis) for the various body sensors for data analysis.
Data Analysis
Frequencies and descriptive statistics were used to analyze participant demographics. A modified static equilibrium equation of the spine was developed to calculate the total spinal compression force at L5/S1 during assisted falls VR simulations as shown in Table 1. The static equilibrium equation of the spine balances moments of force that equals force times length or weight times the distance from the center of weight of load to a fulcrum such as the L5/S1 spine (Tözeren, 2006; Venkatasubramanian, 2021; Zhang et al., 2020). The modified calculation for the total spine compression force at L5/S1 equals the clockwise moment of the staff upper body plus the clockwise moment of the patient avatar upper body load plus the counterclockwise moment of the erector spinae low back muscles which are 5 cm behind the spine (Tözeren, 2006; Venkatasubramanian, 2021; Zhang et al., 2020). The upper body segment was computed to be 55% and the staff upper body center of gravity was empirically calculated to be 0.86 in the clockwise moments of force based on the literature and analysis of participant upper body segments (Ramachandran et al., 2016; Tözeren, 2006). Average spinal compression forces calculated from the five trials for the three scenarios were compared to the safe spinal compression limit of 3,400 N to determine if they exceeded the safety threshold for staff low back injury (Zhang et al., 2020).
Modified Calculation of Spinal Compression Force at L5-S1 for Assisted Falls VR Simulations
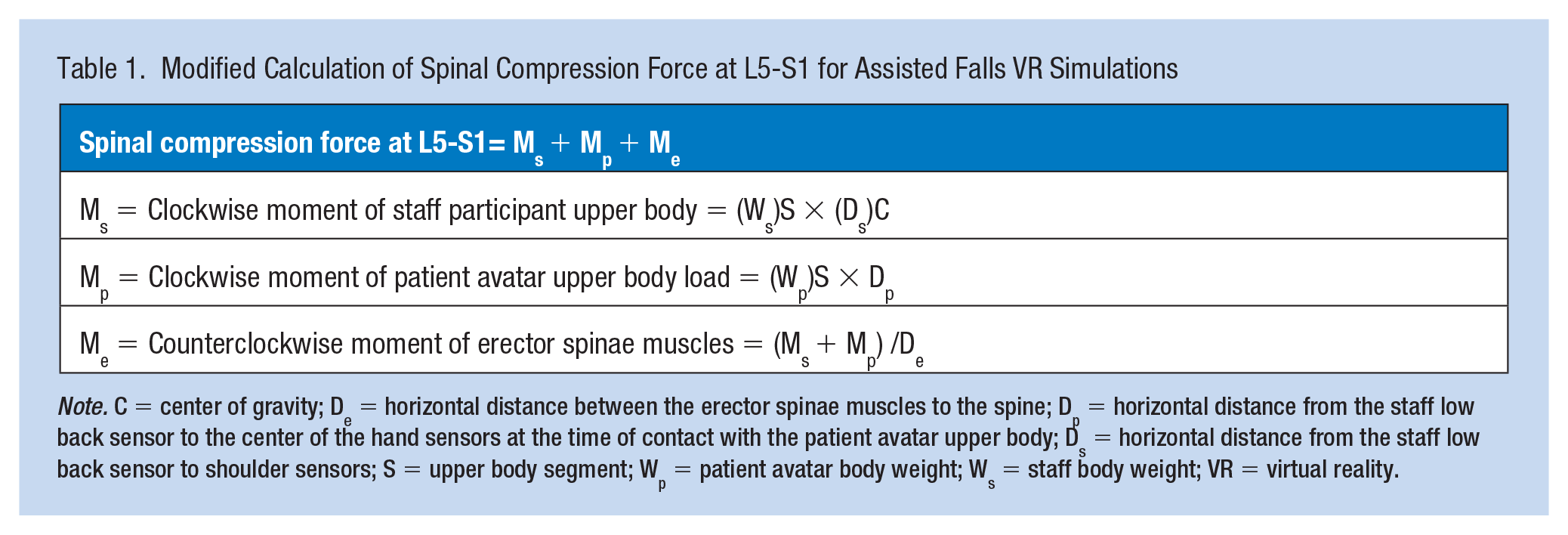
Note. C = center of gravity; De = horizontal distance between the erector spinae muscles to the spine; Dp = horizontal distance from the staff low back sensor to the center of the hand sensors at the time of contact with the patient avatar upper body; Ds = horizontal distance from the staff low back sensor to shoulder sensors; S = upper body segment; Wp = patient avatar body weight; Ws = staff body weight; VR = virtual reality.
Results
Participants
Six volunteer participants completed a total of 90 assisted falls VR simulations (6 participants x 3 scenarios x 5 trials). The average age of the participants was 44.8 years old (SD = 10.3) with an average height of 1.68 meters (~66 inches; SD = 0.1 m) and an average weight of 78.9 kg (~174 pounds; SD = 12.4 kg) as presented in Table 2. Participants were mostly female and represented various disciplines including nursing, health science, medicine, and physical therapy.
Patient Avatar and Participant Demographics
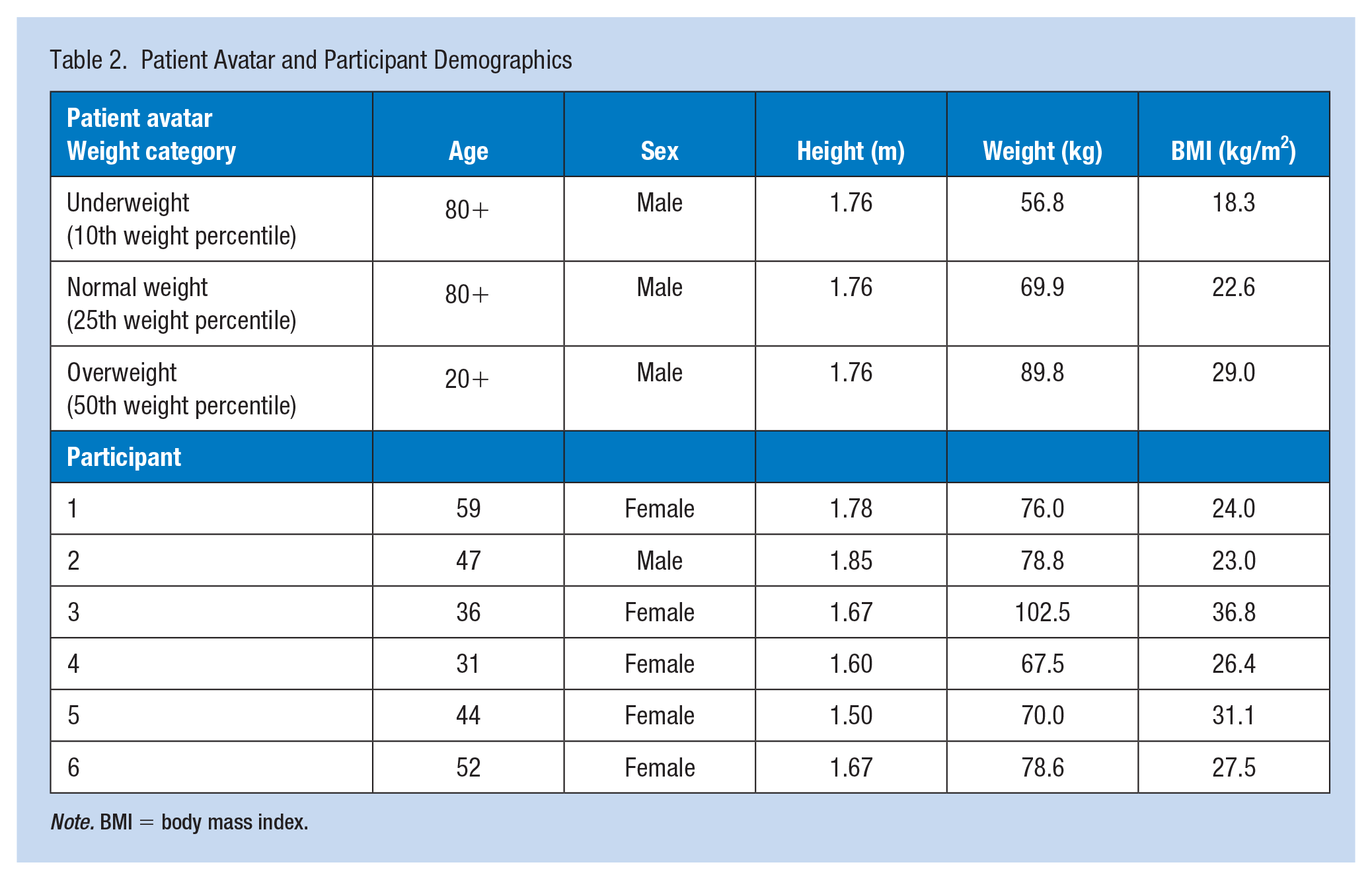
Note. BMI = body mass index.
Calculated Spinal Compression Forces
Table 3 presents the calculated average spinal compression forces for each participant for each scenario. The average time to patient avatar contact in the VR simulations ranged from 0.11 seconds (s) to 1.34 s with a mean of 0.77 s. The spinal compression forces exceeded the compression limit of 3,400 N for all calculated patient weight percentiles despite staff application of ergonomic techniques. The spinal compression forces were high for all assisted falls scenarios regardless of staff assisting a fall toward the floor or a seat. The average spinal compression forces for all assisted falls scenarios across participants ranged from 7,132 N to 27,901 N, with forces between two and eight times over the safety threshold. Our results did not demonstrate any scenario where staff can safely assist a falling adult patient without risk of low back injury despite application of ergonomic techniques and regardless of patient weight.
Assisted Falls VR Simulations Calculated Spinal Compression Forces Across Patient Avatar Weight Categories (Underweight, Normal, and Overweight)
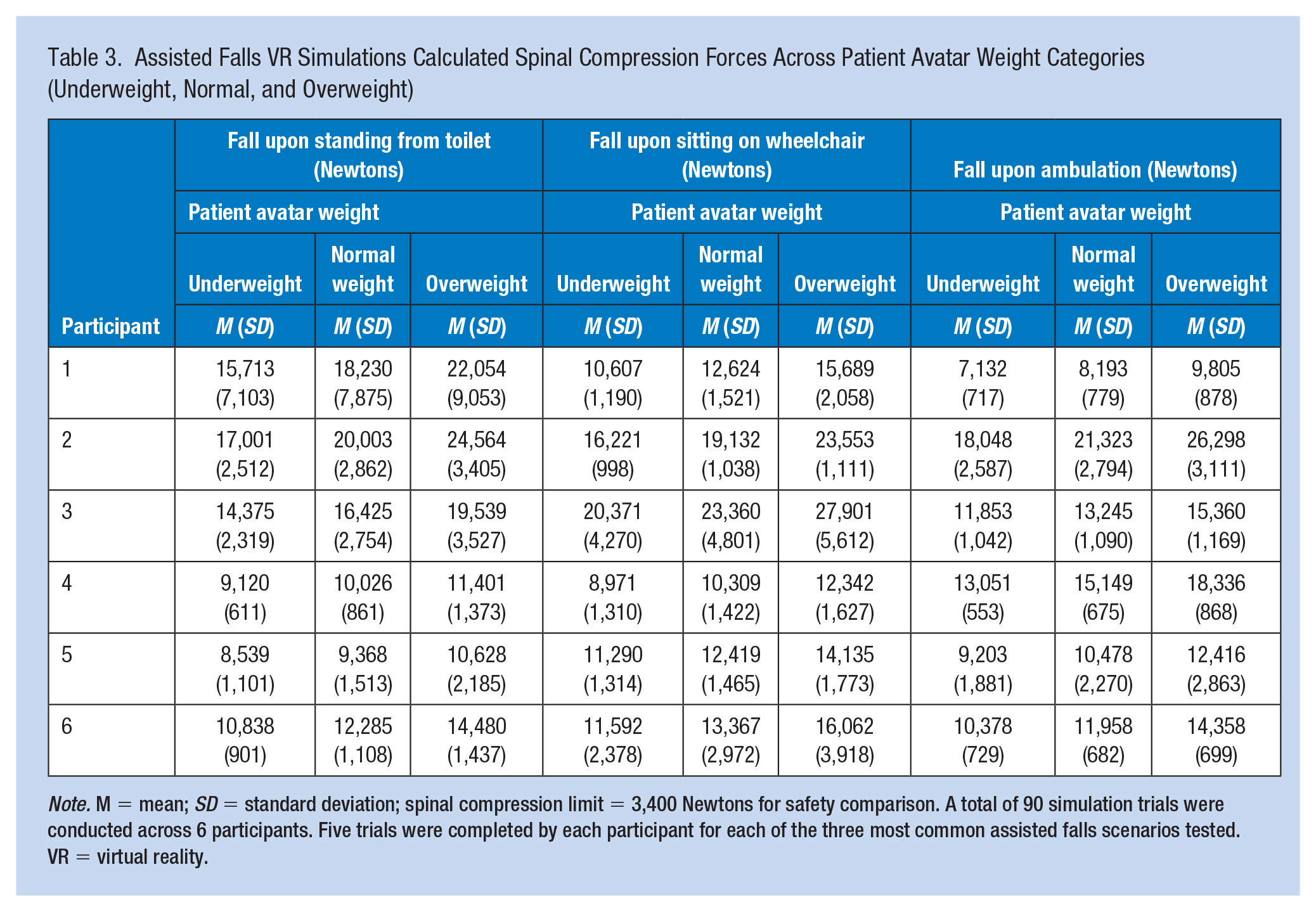
Note. M = mean; SD = standard deviation; spinal compression limit = 3,400 Newtons for safety comparison. A total of 90 simulation trials were conducted across 6 participants. Five trials were completed by each participant for each of the three most common assisted falls scenarios tested. VR = virtual reality.
Discussion
Conclusions
Assisted falls occur when staff try to minimize the impact of a patient’s fall by slowing the descent. Research studies suggest assisted falls may decrease patient’s fall injury risk, but staff injury risk was not reported in these studies (Staggs et al., 2014). Our VR laboratory findings demonstrate that assisted falls may increase low back injury risk to staff. There was no safe scenario where staff could safely assist a patient fall without surpassing the spinal compression threshold of 3,400 N (NIOSH, 1981; Waters, 2007; Zhang et al., 2020). VR simulations of a patient fall during a toilet to wheelchair transfer demonstrated that calculated spinal compression forces at L5/S1 to the low backs of staff participants exceeded the safety spinal compression limit for all common assisted falls scenarios even with application of ergonomic techniques. Furthermore, every patient avatar weight calculated resulted in spinal compression forces above the threshold of 3,400 N, placing staff at risk for low back injury. Thus, assisted falls were deemed unsafe for staff to perform regardless of the adult patient weight due to risk of low back injury.
While we support staff to be trained on ergonomic techniques if they are involved in direct mobilization of patients, ergonomics alone is unlikely to prevent staff injury during assisted falls. The safest approach is to prevent assisted falls from occurring. We recommend the use of mobility screening tools that assess the patient’s mobility level and therefore guide SPHM technology selection and use to help prevent patient falls and reduce the injury risk to both patients and staff. There are many mobility clinical tools such as the Bedside Mobility Assessment Tool (BMAT) and Veterans Administration Mobility Screening and Solutions Tool (MSST) (Health Services Research & Development Forum, 2020; Hoyer et al., 2018; Lininger et al., 2021; Melillo et al., 2022). Most mobility screening tools evaluate patient functional status such as ability to sit on the edge of bed, upper and lower body strength, ability to stand, and ability to step or walk (Health Services Research & Development Forum, 2020; Hoyer et al., 2018; Lininger et al., 2021; Melillo et al., 2022). SPHM technology such as lateral transfer devices or powered sit to stand lifts may be used for toilet to wheelchair transfers depending on the mobility screening results (Andersen et al., 2014; Bergman & De Jesus, 2021; Kucera et al., 2019). Mobility screening tools and SPHM technology were not used in our VR simulations and permit opportunity for future research on their impact to patient and staff safety.
Limitations
We used VR simulations to calculate spinal compression forces, because the weight of falling volunteer patients or mannequins would pose too much safety risk to participants. Our VR data collection and analysis had several limitations. The effect of height differences among staff participants and the patient avatar was not tested as: (a) height in the static equilibrium equation of the spine had minimal impact compared to weight and (b) modifying the height variable would have altered the VR positional data (Tözeren, 2006; Zhang et al., 2020). Furthermore, the static equilibrium equation of the spine does not typically calculate for unexpected tasks such as assisted falls that require quick reaction times to make contact with the load (Tözeren, 2006; Zhang et al., 2020). Dynamic factors like shear, tension, and torsion were not studied given that all trials exceeded the safety threshold of 3,400 N and adding these factors would have likely further increased the spinal compression forces (Tözeren, 2006; Zhang et al., 2020). This project focused only on staff low back injury in a small sample size and did not address other less common injury sites which may occur during assisted falls like the knees, shoulders, and neck (Bulat et al., 2020).
Biological sex considerations were limited in this ergonomic evaluation, potentially impacting the generalizability of the findings. We did not examine sex as a variable for calculated forces given our hypothesis was that weight, as opposed to center of gravity of the load, would most impact the spinal compression forces in the static equilibrium equation of the spine. Males typically have a higher center of gravity than females and thus more upper body weight distribution (Ramachandran et al., 2016; Tözeren, 2006). Possible sex-related variances among participants may impact the spinal compression forces calculations especially at extreme height and weight differences. However, all spinal compression forces exceeded the 3,400 N safety threshold regardless of participant sex. Future evaluations may design a female patient avatar for representation of female weight composition and include a larger sample size of both sexes for comparison.
Our findings suggest that it is unsafe for staff to assist falling patients. The average calculated spinal compression forces exceeded the spinal compression limit of 3,400 N for all assisted falls clinical scenarios and patient avatar weights tested. For all VR simulation trials, these forces were about four times the spinal compression limit indicating staff low back injury risk. Ergonomic techniques applied by staff participants during the VR simulations did not eliminate this safety concern. Based on our results, we recommend utilizing mobility screening tools that would guide the use of appropriate SPHM technology to prevent both patient injury from falls and staff low back injury risk. Given there is no safe way for staff to manually assist a falling patient, appropriate SPHM technology use is necessary to prevent assisted falls before they occur. SPHM programs in the VHA have been integrated through national directives to promote tools and technology to optimize patient and staff safety during mobility. We support implementation of comprehensive SPHM programs as the best practice approach to prevent patient falls without placing staff at risk of injury in healthcare workplaces.
Applications to Professional Practice
There is no safe adult patient weight for staff to assist a falling patient without risk of staff low back injury. While physical ergonomic techniques are important to optimize staff body postures, positions, and movements during patient transfers, they do not eliminate excessive spinal compression forces during direct patient maneuvers. The best practice to ensure safety of both patients and staff is to integrate effective safe patient handling and mobility (SPHM) programs into healthcare workplaces where assisted falls may occur. Evaluation of patient fall risk and mobility should be incorporated to guide SPHM technology use. We recommend utilizing mobility screening tools that guide the choice of SPHM technology to prevent assisted falls. Comprehensive SPHM programs help prevent assisted falls which in turn prevents injuries to both patients and staff.
Footnotes
Acknowledgements
None.
Author Contributions
Project concept and design: T. B., L. C., B. B., Y. F., V. B., M. C., J. L., S. P., and A. M. Acquisition of data: S. P., A. M., H. K., V. B., L. C., M. C., J. L. Analysis and interpretation of data: S. P., A. M., V. B., B. B. Drafting of the manuscript: V. B., B. B., T. B., L. C., Y. F., M. C., and S. B. Critical revision of the manuscript for important intellectual content: All authors.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Veterans Health Administration (VHA) National Center for Patient Safety (NCPS) and the James A. Haley Veterans’ Hospital and Clinics. The content of this publication does not represent the views of the Department of Veterans Affairs or the United States Government.
Human Subjects Review
This project was determined to be quality improvement (QI) by the Research and Development Committee at James A. Haley Veterans’ Hospital and Clinics, Tampa, FL, USA.