
Abstract
Objective. Pediatric traumatic brain injury (TBI) is associated with physical and psychobehavioral impairment in children. Effective rehabilitation programs postinjury are critical for children with TBI. Virtual reality (VR) has been increasingly adopted for brain injury rehabilitation. However, scientific synthesis is lacking in evaluating its effectiveness in pediatric TBI rehabilitation. This article aimed to conduct a systematic review on the effectiveness of VR-based pediatric TBI rehabilitation. Methods. A systematic literature search was conducted in PubMed, PsycInfo, SCOPUS, CENTRAL, BioMed Central, CiNAHL, and Web of Science through November 2015. Personal libraries and relevant references supplemented the search. Two authors independently reviewed the abstracts and/or full text of 5824 articles. Data extraction and qualitative synthesis was conducted along with quantitative assessment of research quality by 2 authors. Results. A positive impact was found for VR-based interventions on children’s physical rehabilitation post-TBI. The quality of research evidence was moderate, which largely suffered from small samples, lack of immersive VR experience, and lack of focus on socioemotional outcomes post-TBI. Conclusions. The present review identified positive effects of VR interventions for pediatric TBI rehabilitation especially in physical outcomes. Future research should include larger samples and broader post-TBI outcomes in children using VR-based interventions.
‘Head injuries are present in 75% of injured children and account for 70% of deaths among children with trauma.’
Labeled as “the silent epidemic,” traumatic brain injury (TBI) has become an increasing threat to children’s health and well-being in the past few decades. TBI is caused by a bump, blow, or jolt to the head or a penetrating head injury, which disrupts the normal function of the brain. 1 As a leading cause of acquired disability in children and youths in the United States, the Centers for Disease Control and Prevention estimated that 700 000 children suffer from TBI every year, mostly from motor vehicle crashes or falls.2,3 Head injuries are present in 75% of injured children and account for 70% of deaths among children with trauma. 4 Since 2001, young children (less than 4 years of age) have the highest TBI rate increase. Rates of TBI-related emergency department visits increased by 60% from 1374.0 to 2193.8 per 100 000 from 2008 to 2010, respectively. 2
Pediatric TBI results in both short-term and long-term impairment in physical and psychosocial functioning. Physical deficits after pediatric TBI include changes in motor skills (eg, muscle tone, paralysis, balance, walking) and/or sensory abilities (eg, vision, hearing). 5 The impact on children’s psychosocial abilities after pediatric TBI can be more enduring with potentially detrimental outcomes on cognitive, emotional, and interpersonal skills.6,7 One strategy to improve health outcomes among children with TBI is through postinjury rehabilitation interventions. These interventions include (a) physical rehabilitation focused on restoring a child’s strength, endurance, and motor flexibility and (b) cognitive rehabilitation comprising a broad collection of interventions that aim to improve psychosocial skills.8,9
Traditional physical and cognitive rehabilitation therapies are administered in-person by trained staff at hospitals, schools, communities, and/or homes. These therapies require significant amounts of costly medical personnel resources. Inaccessibility for some patients, especially those living in nonurban areas, or those without adequate medical insurance, leads to greater health disparities. To overcome such access barriers, modern technologies such as web-based/computer-assisted counseling programs and video games are increasingly being used to deliver rehabilitation interventions for children with TBI.10-12 Such preprogrammable interventions are more cost-effective because they can be remotely accessed and require significantly less medical staff resources, while still delivering training content that can be tailored to the specific needs of the child.
Virtual reality (VR), a rapidly developing field in computer technology, has drawn increasing attention in the pediatric health literature including TBI rehabilitation.13-15 According to the Merriam-Webster Dictionary, “virtual reality” is defined as “an artificial environment which is experienced through sensory stimuli (such as sights and sounds) provided by a computer and in which one’s actions partially determine what happens in the environment.” This definition of VR, which has been widely adopted in the health literature,16-20 permitted the inclusion of both traditional video gaming consoles (eg, Wii, PlayStation, Xbox Kinetic) and the more cutting-edge VR technologies (eg, Oculus, HTC VIVE), as long as patients are able to experience live interactions with the gaming environment through sensory stimuli and/or motor feedback. In addition to offering the same flexibility, customizability, and accessibility as other computer-assisted interventions, VR-based rehabilitation can provide children with TBI at least the following 3 unique advantages over traditional paper-and-pencil and computerized interventions. First, VR interventions have the capability to offer a multitude of activities for training children with TBI following their injuries within a versatile virtual environment. Such environments offer interaction at all levels, from sensory and motor to cognitive and socioemotional, which greatly facilitate patients’ structural and functional recovery of their brains and are especially effective for children with TBI whose developing brains are highly plastic. 16 Second, VR-based rehabilitation can be readily provided remotely by medical providers directly to patients’ home or nearby facilities either via the Internet or mobile apps, allowing postdischarge training sessions to be completed without requiring children to leave home. This could potentially reduce the long-term health outcome disparities especially for patient families who live in rural or remote areas. Last but not least, unlike traditional computerized rehabilitation training (especially in the domain of cognitive training), VR-based interventions may improve children’s adherence to training plans because of youth population’s increasing exposure to electronic games and the novelty of VR-based games.
Therefore, it is critical for both researchers and clinicians to gain a big-picture understanding of the current practices and empirical evidence accumulated thus far regarding this emerging VR-based approach to pediatric TBI rehabilitation, for which purpose a systematic review on this topic would be appropriate. However, although existing syntheses on the effectiveness of VR-based interventions on TBI rehabilitation outcomes provided encouraging findings, they often failed to adopt a systematic review approach.16-18 Our literature search identified only one 2015 systematic review on the effectiveness of VR on TBI rehabilitation constrained to only adult patients with TBI, 19 and one 2009 systematic review on VR application in acquired brain injury for upper limb rehabilitation. 20 Hence, the objective of the present article is to conduct a systematic review on the effectiveness of VR-based interventions post-TBI children’s rehabilitation outcomes so as to further our understanding of the best practice for evidence-based rehabilitation for pediatric patients with TBI.
Methods
Information Sources
The databases searched included PubMed, PsycInfo, SCOPUS, CENTRAL, BioMed Central, CiNAHL, and Web of Science. We searched all years (earliest data available in each database through November 18, 2015) and all languages available in each database without restriction. We also reviewed our personal literature libraries and followed relevant references in articles to supplement these searches.
Search Strategy
We used the following search term for all queries: “(virtual real* OR virtual technolog* OR virtual gam* OR virtual environment* OR simulat* OR video gam* OR computer gam* OR electronic gam*) AND (child* OR pediatric OR paediatric OR adolescen*) AND (brain injur* OR head injur* OR concussion* OR TBI).” The search and review protocol is available from the authors on request.
Eligibility Criteria
Studies were included in this systematic review if they described any empirical research evaluating an intervention that utilized VR technology for rehabilitation among children less than 18 years of age with TBI. We considered all types of study designs including randomized controlled trials, observational studies using case-control designs, uncontrolled before-after designs, and case reports. Nonempirical articles including commentary, reviews, editorials, and letters and empirical articles without intervention evaluation were excluded.
Studies were excluded if no group/condition in the study involved VR technology (ie, video/video games/computer games that simulate fictional and/or real-life environments), or no branch of the study sample included children under 18 years of age. Studies were also excluded if no portion of the study sample were explicitly identified as patients with TBI (defined by ICD-9 diagnosis codes 850, 851-854, and 803). Although studies were included from all regions of the world, unpublished documents (eg, dissertations, unpublished manuscripts, etc) were excluded due to lack of peer review. Following a preschemed written protocol, two researchers independently reviewed all search results based on the aforementioned criteria. Disagreements were resolved through discussion and adjudicated by a third experienced researcher.
Quality Assessment of Included Studies
The present review used the Checklist for Measuring Quality (CMQ) 21 to assess the methodological quality of included studies. The CMQ was created to provide quantitative assessment of both randomized and nonrandomized studies involved with health care interventions. Therefore, the CMQ is especially suitable to provide quantitative synthesis of the quality of included studies in the present review, which focused on VR-based health care interventions for pediatric TBI rehabilitation and may include nonrandomized studies (eg, pre-post designs or case reports). The CMQ, consisting of 27 items with a possible maximum score of 31 points for each assessed study, assesses the following 5 methodological domains of a study 21 :
Reporting: The extent to which the information reported in the study was sufficient to make an unbiased assessment of the study findings. Example item: “Is the hypothesis/aim/objective of the study clearly described?”
External validity: The generalizability of the study findings from sample to population. Example item: “Were the subjects asked to participate in the study representative of the entire population from which they were recruited?”
Internal validity (measurement bias): The measurement biases of the intervention and outcome(s). Example item: “Was an attempt made to blind study subjects to the intervention they have received?”
Internal validity (selection bias): Biases in the selection of study sample. Example item: “Were the patients in different intervention groups (trials and cohort studies) or were the cases and controls (case-control studies) recruited from the same population?”
Study power: The extent to which negative findings from the study could be due to chance. The only item in this domain is “Did the study have sufficient power to detect a clinically important effect where the probability value for a difference being due to chance is less than 5%?”
The CMQ has established adequate face and content (translation) validity, criterion-related validity, and internal and external reliability. 21 Conventionally, “good-quality” studies have total scores greater than 20; “moderate-quality” studies have total scores between (and including) 11 and 20; and “poor-quality” studies score below 11. 20 Two researchers independently scored each of the 3 included studies on the aforementioned domains. Discrepancies in ratings were rare and were solved through discussion until a consensus was reached.
Results
Included Studies
The process and results for study inclusion in this review are summarized in a Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (Figure 1). The initial search identified 5824 articles, with 4936 articles remaining after deleting duplicates. As described in the Methods section, 2 independent reviewers following a preschemed written protocol reviewed the abstracts of all 4936 articles. The inclusion and exclusion criteria disqualified 4724 articles. Full-text articles of the remaining 212 studies were then reviewed by the two independent reviewers using the same protocol. Interrater reliability was strong (κ > 0.90). Only 3 studies were determined eligible for the present review, with the other 209 studies excluded for various reasons (Figure 1).
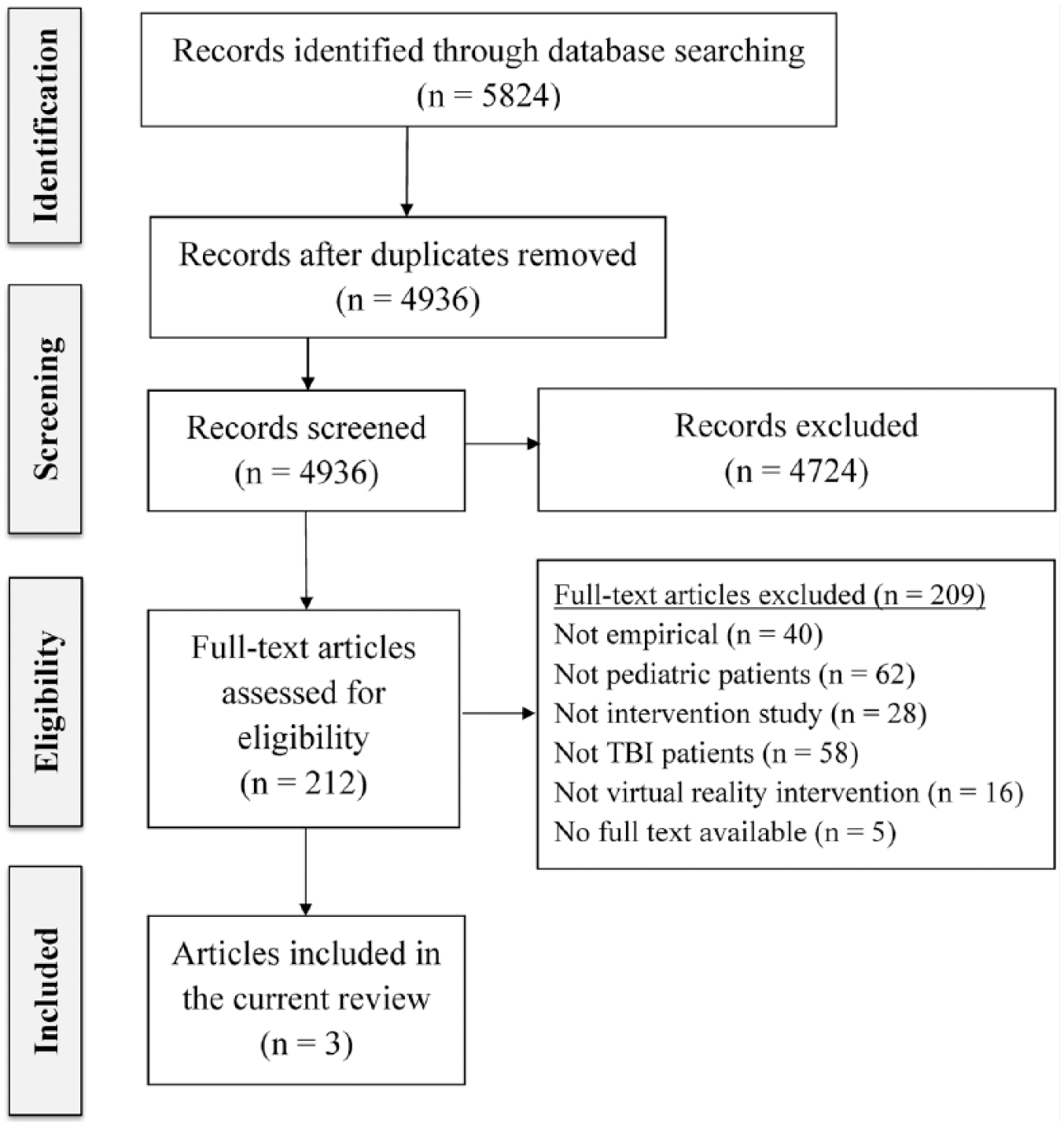
PRISMA Flow Diagram of Included Studies.
Descriptive Characteristics of Included Studies
Detailed information was extracted from the 3 included studies for the present review (Table 1). All 3 studies were published in or after 2011. All 3 studies were conducted in developed countries (2 in the United States and 1 in Canada). Below we summarize the descriptive characteristics of the included studies in four aspects: Types of research design, Types of VR intervention, intervention effectiveness, and quality of research evidence.
Descriptive Information on Included Studies (N = 3).
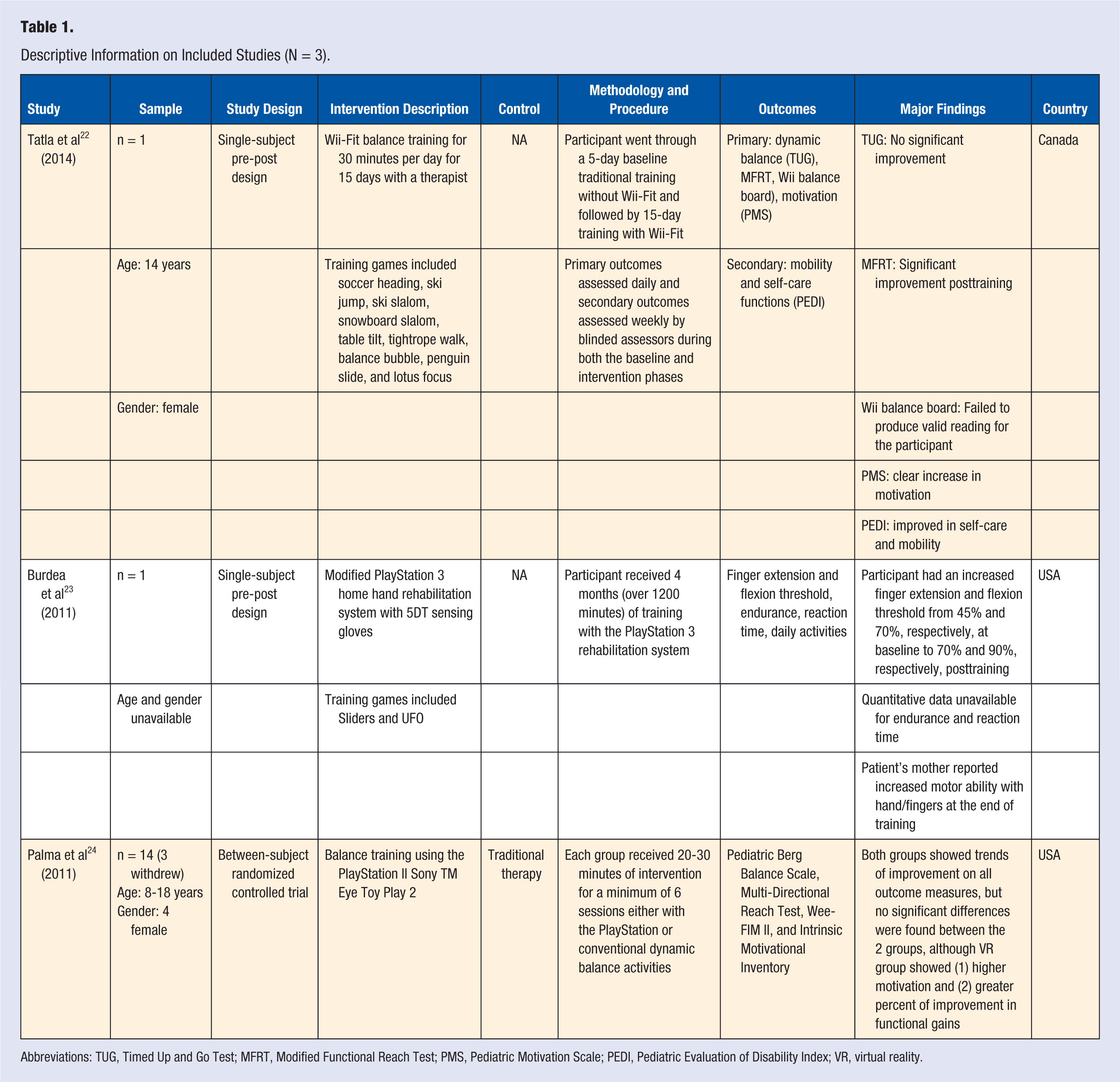
Abbreviations: TUG, Timed Up and Go Test; MFRT, Modified Functional Reach Test; PMS, Pediatric Motivation Scale; PEDI, Pediatric Evaluation of Disability Index; VR, virtual reality.
Types of Research Design
Two of the included studies, Tatla et al 22 and Burdea et al, 23 used a single-subject pre-post design without a control/comparison group. Although both studies included additional children without a TBI, these children were not designed to match the children with TBI as controls. The third study, Palma et al, 24 used a larger sample (n = 14; albeit small sample size) and the between-subject randomized controlled trial design with 2 experimental groups: an intervention group that received VR-based therapy and a control group that received traditional therapy.
Types of Virtual Reality Intervention
All 3 studies used commercially available games and gaming consoles, such as Wii, 22 PlayStation 2, 24 and PlayStation 3. 23 VR experience was primarily provided by flat-screen TVs, as well as video cameras and/or sensory trackers such as sensing gloves to interact with avatars in the games. Such setup is often adequate to provide study participants with at least semi-immersive virtual environment for them to engage in live interactions with the game characters.
Intervention Effectiveness
All 3 identified studies focused on rehabilitation of children’s physical functions using VR-based interventions, which yielded promising results. Specifically, Tatla et al 22 and Palma et al 24 focused primarily on balance training. After VR-based intervention, children with TBI had marginal to significant improvement on some balance-specific measurements (eg, dynamic balance). Both studies showed significant improvement in functional abilities after the intervention and increased motivation in participating in VR-based rehabilitation programs. Burdea et al 23 used a VR-based intervention to target another aspect of physical rehabilitation, namely, finger flexion. After training 4 months with the VR system, the participant showed significant improvement in both finger extension/flexion and motor ability with hand/fingers in daily life. Functional outcomes in daily life were only reported in 1 of the 3 included studies. Tatla et al 22 indicated that the participant demonstrated a significant improvement of self-care abilities postintervention as reported by the child’s mother.
Quality of Research Evidence Assessment
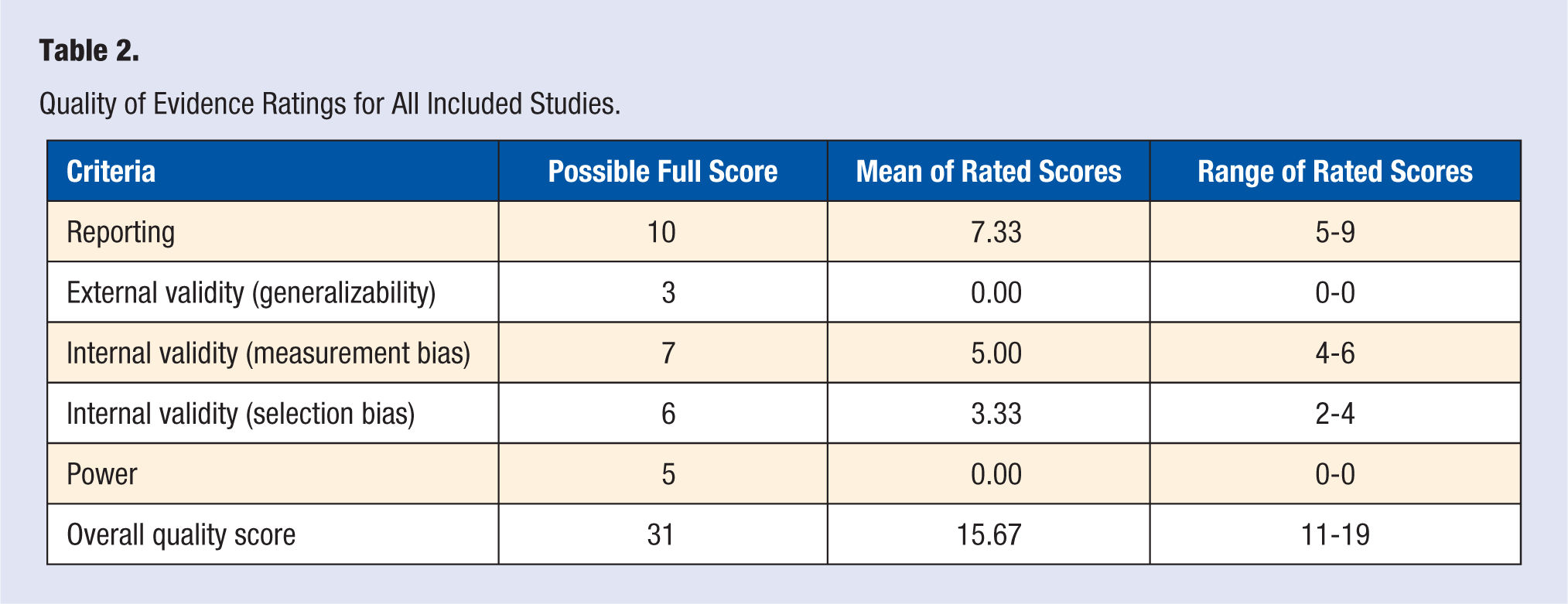
Possible full scores, mean, and range of rated scores for the 3 included studies using the CMQ are reported in Table 2. The mean total score for the included studies was 15.67 points, with a range from 11 to 19 points, falling into the “moderate-quality” category. The included studies scored well in 2 domains: reporting (7.33 of 10 points) and internal validity (measurement bias; 5 of 7 points). These studies scored worst on external validity (generalizability; 0 of 3 points) and power (0 of 5 points).
Quality of Evidence Ratings for All Included Studies.
Discussion
The present article conducted a systematic review of the published literature on the effectiveness of VR-based interventions on pediatric TBI rehabilitation. Of 5824 articles identified, only 3 studies from 2011 to 2014 qualified. Overall, current VR-based interventions on children’s physical rehabilitation post-TBI have a positive impact with a moderate quality of evidence.
Due to small samples sizes (n = 1 or n = 14) in all 3 included studies, findings from these studies have inadequate power (0 out of 5 points on the CMQ scale) to detect statistically meaningful effects of the intervention and lack the capability to generalize the findings to the larger pediatric TBI population. The small sample sizes may be attributed to at least 2 causes. First, since VR is still an emerging technology in medical settings, particularly in pediatric TBI rehabilitation, small sample trials are usually required for proof-of-concept or demonstrating feasibility and validity before applying the intervention to larger clinical populations. Second, limited funding resources are available to researchers to support larger implementation of VR-based rehabilitation programs. Although these justifications are understandable, the small sample sizes do not make the studies representative and, hence, hinder generalizing the findings to a greater pediatric TBI population. The small sample sizes also explain the low overall score on the External Validity (generalizability) domain on the CMQ checklist (Table 2).
Despite the small sample sizes, all 3 studies incorporated relatively high-quality research designs appropriate to their sample size. In 2 case studies (each n = 1),22,23 Tatla et al and Burdea et al both used pre-post designs that controlled for baseline covariates among other confounding variables (Table 2). Palma and colleagues (n = 14) 24 adopted a randomized controlled trial design (ie, an intervention group for VR therapy and a control group receiving traditional TBI therapy), the typical “gold standard” in empirical research. Furthermore, 2 of the 3 studies did not blind measurement assessors from knowing the intervention that participants received (Tatla et al 22 was the exception). Moreover, none of the studies blinded participants from the intervention they received. Both practices resulted in a moderate CMQ rating on Internal Validity (selection bias; Table 2). While one could argue that case studies blinding participants from knowing if they are receiving an intervention is implausible, potential options do exist to improve the design of randomized controlled trials in future research. Instead of having the control group receiving standard therapies, controls could be assigned to an equivalent VR-based game during the study period, but without the training (intervention) component within the game.
Our review also revealed that traditional TV-based gaming consoles were adopted in all 3 studies to provide nonimmersive 2-dimensional VR interventions for children with TBI. The predominant use of traditional TV-based gaming consoles is also consistent with findings from literature on adult TBI rehabilitation using VR interventions. 20 One advantage of using commercial TV-based VR systems with children is familiarity with the interfaces and interaction mechanisms, especially among those children experienced with video games. Commercial TV-based VR systems are also more cost-effective than developing custom VR training systems. However, adopting more advanced VR systems is an increasing trend in both medical research (eg, stroke rehabilitation 25 procedural pain management 26 ) and other fields of scientific research (eg, distracted driving 27 and pedestrian safety28,29). Immersive VR systems, combined with custom-designed software specifically for children with TBI, could provide children with a highly engaging, individualized, and realistic intervention system, which may ultimately enhance the transfer of skills children learned in a virtual system to real life activities post-intervention.
Finally, previous research has consistently suggested that TBI exerts significant effect not only on outcomes like children’s physical functioning but also on their cognitive,30,31 emotional,32,33 and social functioning.34-36 Although the present review aimed to evaluate the effectiveness of VR-based rehabilitation programs on children with TBIs for a variety of outcomes, only physical outcomes post-TBI were targeted in all 3 eligible studies identified in our systematic literature search. Reported evidence was also limited on outcomes like functional skills and VR experience (eg, motivation). However, research on other brain injuries including adult TBI and stroke have suggested a positive impact of VR-based interventions on patients’ nonphysical outcomes, primarily focusing on cognitive rehabilitation (eg, memory and attention).16,19 Future VR-based rehabilitation programs should incorporate a broad range of components that offer a training system comprising a spectrum of interventions for physical to psychological functioning and for cognitive to socioemotional skills.
Limitations
Several limitations of the present review should warrant readers’ caution when interpreting our findings. First, the present review focused only on TBI rehabilitation among school-aged children. Therefore, findings from this study may not be generalizable to other age groups or other clinical conditions. Due to the different brain plasticity and vulnerability during infancy and early childhood, brain injuries among infants and preschoolers might lead to very different outcome trajectories than brain injuries among older children and adolescents. 37 For instance, previous research has suggested that although most mild head injuries in younger children were able to recover without any adverse effects, such neurological plasticity may not hold in more severe injuries among preschoolers. 38 Future VR-based rehabilitation programs should therefore design age-appropriate interventions that target different injury severities and developmental stages (eg, facilitating movement and exploratory behaviors for infants and preschoolers versus social skills and cognitive/emotional functions for older children). Second, the limited number of eligible studies synthesized in the present review hindered our ability to conduct quantitative analysis of the effect size. The limited amount of available evidence in VR-based pediatric TBI rehabilitation is not surprising since VR is a relatively new technology and has only recently been applied in medical research. Yet the promising findings synthesized from these studies establish that the field of technology-assisted pediatric TBI rehabilitation interventions affords great opportunities for future research. Finally, our literature search excluded thesis/dissertation documents and government reports. Although, generally, a higher level of confidence is usually vested in evidence vetted through the peer-reviewed process, these reports might offer additional data and perspectives to understand the efficacy of VR-based intervention on pediatric TBI rehabilitation for future research.
Implications
The implications of the present review extend to both research and clinical practice in pediatric TBI rehabilitation. As an emerging technology in research, VR has been increasingly used for physical rehabilitation after pediatric TBI. The promising impact of such interventions on children’s health outcomes encourage researchers and sponsors to further support the exploration of the potential of VR-based interventions for the psychological and social rehabilitations in children with TBI, with potentially tailored applications for children with different injury severities and at different developmental stages. Clinically, VR technology provides an engaging and safely controlled system to supplement both inpatient and outpatient rehabilitation care, both in terms of ameliorating injury-related functional impairment and facilitating the development of remaining functions within pediatric patients. In addition to improved health outcomes, such technology-assisted programs are also likely to increase patient compliance and satisfaction and enable hospitals and medical centers to provide high-quality health care services with existing personnel resources.
Conclusions
This systematic review analyzed current literature on the use of VR-based interventions in pediatric TBI rehabilitation. Information synthesized herein on VR-based programs found these programs to exert a positive impact on physical outcomes such as balance and flexibility among children with TBI. More research is needed to examine VR-based programs’ impact on children’s psychological and social outcomes, both in the short term and long term at different developmental stages of an individual. Future VR-based pediatric neurorehabilitation programs should also broaden to develop tailored interventions for not only the amelioration of impairment but also the facilitation of remaining development for pediatric patients at all stages. Findings of this review hold significant implications for future research and clinical practice in pediatric TBI rehabilitation.
Footnotes
Acknowledgements
Thanks to Dr Melody Davis for providing professional edits and comments throughout the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All phases of this study were supported by the Clinical and Translational Research Intramural Funding Program at Nationwide Children’s Hospital.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.
Informed Consent
Not applicable, because this article does not contain any studies with human or animal subjects.
Trial Registration
Not applicable, because this article does not contain any clinical trials.