
Abstract
Objectives:
Involving practice nurse and other assistant clinical staff members in providing information and education to patients with low back pain at follow-up appointments may release more time and improve care in general practice. However, this requires a shift in the division of tasks, and general practitioners’ barriers and facilitators for this are currently unknown. The objectives were to explore general practitioners’ experiences and perceptions of including assistant clinical staff members in the management of low back pain.
Methods:
This is a semi-structured interview study in Danish general practice. General practitioners with a variation in demographics and experience with task-delegation to clinical staff were recruited for in-depth interviews. We used a phenomenological approach to guide the data collection and the analysis in order to gain insight into the subjective experiences of the general practitioners and to understand the phenomenon of ‘delegating tasks to practice staff’ from the perspective of the general practitioners’ lifeworld. Analysis was conducted using an inductive descriptive method. The sample size was guided by information power.
Results:
We conducted five interviews with general practitioners. All general practitioners had experience with task delegation, but there was a variation in which tasks the general practitioners delegated and to which types of clinical staff members. The following themes were derived from the analysis: general practice organisation, delegating to clinical staff members, doctor–patient relationship, exercise instruction, clinical pathway for patients and external support.
Conclusion:
General practitioners consider patients with low back pain to be a heterogeneous group with a variety of treatment needs and a patient group without any predetermined content or frequency of consultations; this can be a barrier for delegating these patients to clinical staff members.
Introduction
Low back pain (LBP) is very common and is the world’s leading cause of disability. 1 In Denmark, LBP is the reason for 9.5% of consultations in general practice. The proportion of Danes with LBP is increasing.2,3 Furthermore, LBP is one of the leading causes of disability in all high-income, high–middle-income and middle-income countries. 4
In Western countries, the role of general practitioners (GPs) is to perform an assessment of the patient and triage patients with LBP. This aims to identify and appropriately manage serious causes of LBP such as fractures, cancer, infections or inflammatory diseases such as spondylarthrosis. 5 If a serious underlying disease is suspected, patients are likely to be referred for further investigations, specialist assessment and/or treatment. 5 In most cases, however, the underlying causes of LBP remain unknown with only 1%–5% of patients having a serious underlying disease. 6 Adding to this complexity, biological, psychological and social factors all contribute to LBP in various degrees.7,8 Although the majority of patients are not severely affected, many have ongoing pain or experience recurrence.9,10 Treatment based on clinical guidelines, including patient education and support to self-manage, have the potential to improve the care of patients with LBP without a serious underlying cause.5,11–13 Internationally, studies to support the implementation of LBP guidelines have, however, found modest positive results.14,15 High workloads and little available time for consultations have been argued to challenge the delivery of patient education and supported self-management. 16 In Denmark, an intervention aimed at Danish GPs approximately halved the referral of patients to secondary care and reduced costs (£−93.20 per patient) with no negative effects on patients’ pain or functional levels. 17 This previous study applied a multifaceted intervention, which included as a key component multi-professional outreach visits to general practices in order to educate GPs about guideline-endorsed treatments, including providing patients with high-quality information. We believe this intervention can be further improved by integrating it into the organisation of the GP clinics by enhancing the function of multi-professional teams in general practices 18 and making use of the increasing number of available clinical staff members. 19
Involving clinical staff members in the management of some chronic diseases such as diabetes and patients with hypertension has shown to be feasible.19–21 Consequently, involving clinical staff members in providing education and information to patients with LBP might also be feasible and additionally improve the partnership with patients by focusing more on patient information and education. 20 However, barriers and facilitators for this change are currently unknown. 21 Knowledge of GPs’ barriers and facilitators can inform the design of a future intervention to address GPs’ capabilities, opportunities and motivation to include clinical staff members in treating LBP. 22 Consequently, this may lead to feasibility testing and an evaluation of the effectiveness of a theoretically informed intervention. 23
The aim of the present study was to explore GPs’ perceptions of including clinical staff members in the management of LBP in general practice among GPs already delegating tasks for patients with other conditions.
Methods
Theoretical framework
This is a qualitative, semi-structured interview study. We used a phenomenological approach in the data collection and analysis to gain an insight into the subjective experiences and perceptions of the GPs and to understand the phenomenon of ‘delegating any treatment tasks to any practice staff’ from the perspective of the GPs’ lifeworld.24–26 Prior to the study, the interviewer declared her pre-understanding of the field and the expected findings to create awareness about the interviewers’ possible influence on the results and to allow for the later validation of the findings. This study is reported according to the reporting guideline for consolidated criteria for reporting qualitative research (COREQ). 27
Interviewer and research team
All interviews were conducted by R.H.K., as part of her medical master thesis. R.H.K. had no prior experience with research interviewing, but she had received extensive training in interview techniques such as open-ended questions, active listening and probing as part of her medical training. R.H.K. was supervised by J.L.T. (GP and professor), C.A.A. (GP in training and PhD), T.A. (health economist) and A.R. (physiotherapist and PhD). C.A.A. is experienced in conducting interviews. J.L.T., C.A.A., and A.R. are experienced in analysing qualitative data. Prior to interviewing, R.H.K. stated her pre-understanding (Supplementary information). R.H.K. had no prior knowledge of the participants.
Participant selection
In Denmark, general practices are small office-based practices providing primary health care for patients and acting as gatekeepers to secondary care specialist care through a referral system. This maintains the GPs’ role as the first point of contact in health care and supports the idea of the continuity of care by a family doctor. 28 GPs are trained generalists and there are no sub-specialties in Danish general practice. 28 The total number of GPs in Denmark has dropped from 3639 to 3402 (6.5%) between 2008 and 2018. 29 The average age of a Danish GP is 52 years and just above 50% are women. 29 The majority of GPs are self-employed and thereby practice owners. Consequently, GPs are able to organise their practices and manage patients in the manner best suited to them. 28 However, having a tax-financed public health care system means that GPs largely have the same resources available and the vast majority are organised as solo-practices (~31%), partnership-practices (~21%) or collaboration-practices (~48%). 29
Participants
GPs working in the North Denmark Region were eligible to participate. GPs who had finished general practice/family medicine training were practice owners (collaborative, partnership or solo practice), were active practitioners in general practice and had clinical staff members performing clinical tasks (e.g. diabetes controls) were eligible for inclusion. We excluded participants working in a general practice with another participant and participants working in a general practice with a researcher from The Center for General Practice at Aalborg University. Eligible GPs were identified by J.L.T. and A.R. and through public homepages. Seventeen eligible GPs were selected based on the variation in their background characteristics with the aim of recruiting at least one GP for each category of the baseline variables (Table 1). Possible participants were contacted by e-mail and/or telephone by R.H.K. R.H.K. scheduled an interview and briefly explained that she conducted this study in collaboration with the Center for General Practice at Aalborg University. Participants did not have further personal information about the interviewer (Table 1).
Baseline characteristics.
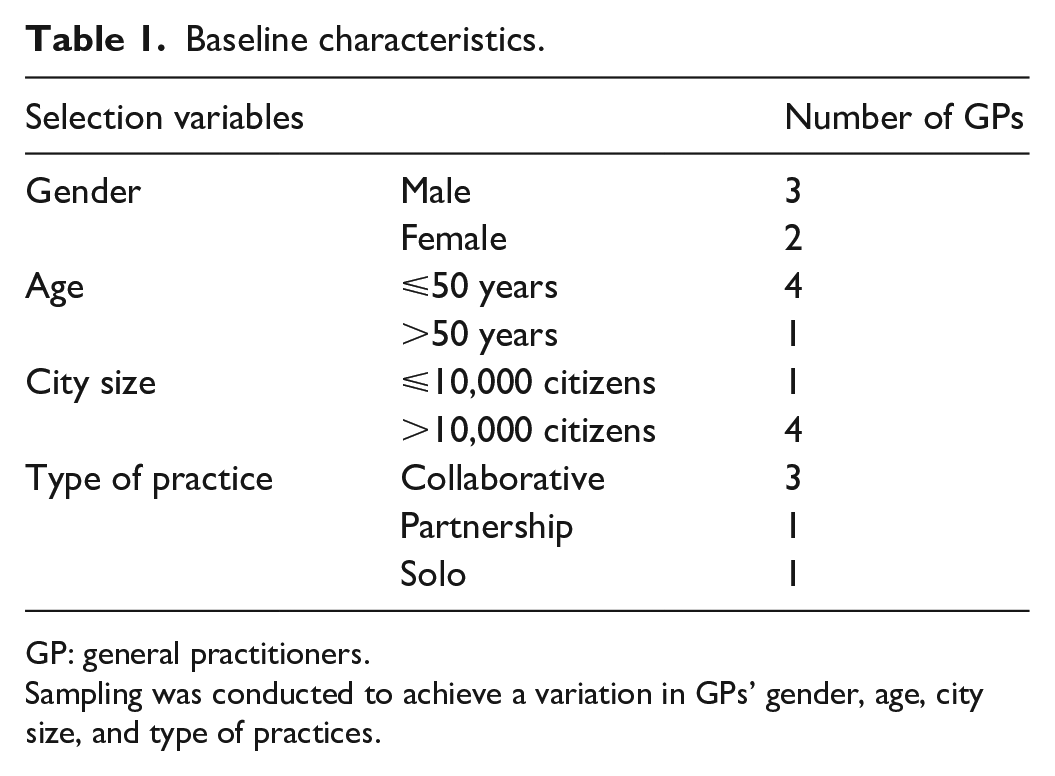
GP: general practitioners.
Sampling was conducted to achieve a variation in GPs’ gender, age, city size, and type of practices.
Sampling
Based on a narrow research question, the expected similarity in the organisation of task delegation across clinic types and the interviewers’ experience with interview techniques, we aimed for a smaller sample supported by the concept of information power. 30 Sampling was established with specific aspects of demographic variation in mind. 30 During the last interview, only few new aspects were covered. However, with a sample size of five, we acknowledge the risk of missing new important information.
Interviewing
To support and maintain the GPs’ role as health care professionals in their natural work environment, interviews were conducted in the GPs’ own consultation rooms. 24 The GPs were seated in their usual chair and the interviewer in the patients’ chair. No other persons were present in the consultation room during the interviews. An interview guide (Table 2) was developed for this study through discussions in the research group and pilot-tested on C.A. with A.R. present. Following the pilot test, we amended the arrangement of questions and made small adjustments in terms of language and sentence structure. The interview guide included open questions that allowed the participants to elaborate using examples from their clinical routines. Questions involving possible conflicts were saved for the last part of the interview. The interview guide was adjusted after the pilot test and we allowed for small adjustments after each interview if new knowledge emerged. During the interviews, R.H.K. continuously summarised the participant’s accounts to secure the correct understanding and interpretation. By the end of each of the 60 min scheduled interviews, R.H.K. asked whether participants had other important issues to add. R.H.K. did not take field notes. R.H.K. conducted, audio-recorded and transcribed all interviews. Transcription was conducted verbatim using SoundScriber software (SOFTPEDIA). Transcriptions were not returned to participants for feedback. Participants provided written informed consent prior to interviewing.
Interview guide.
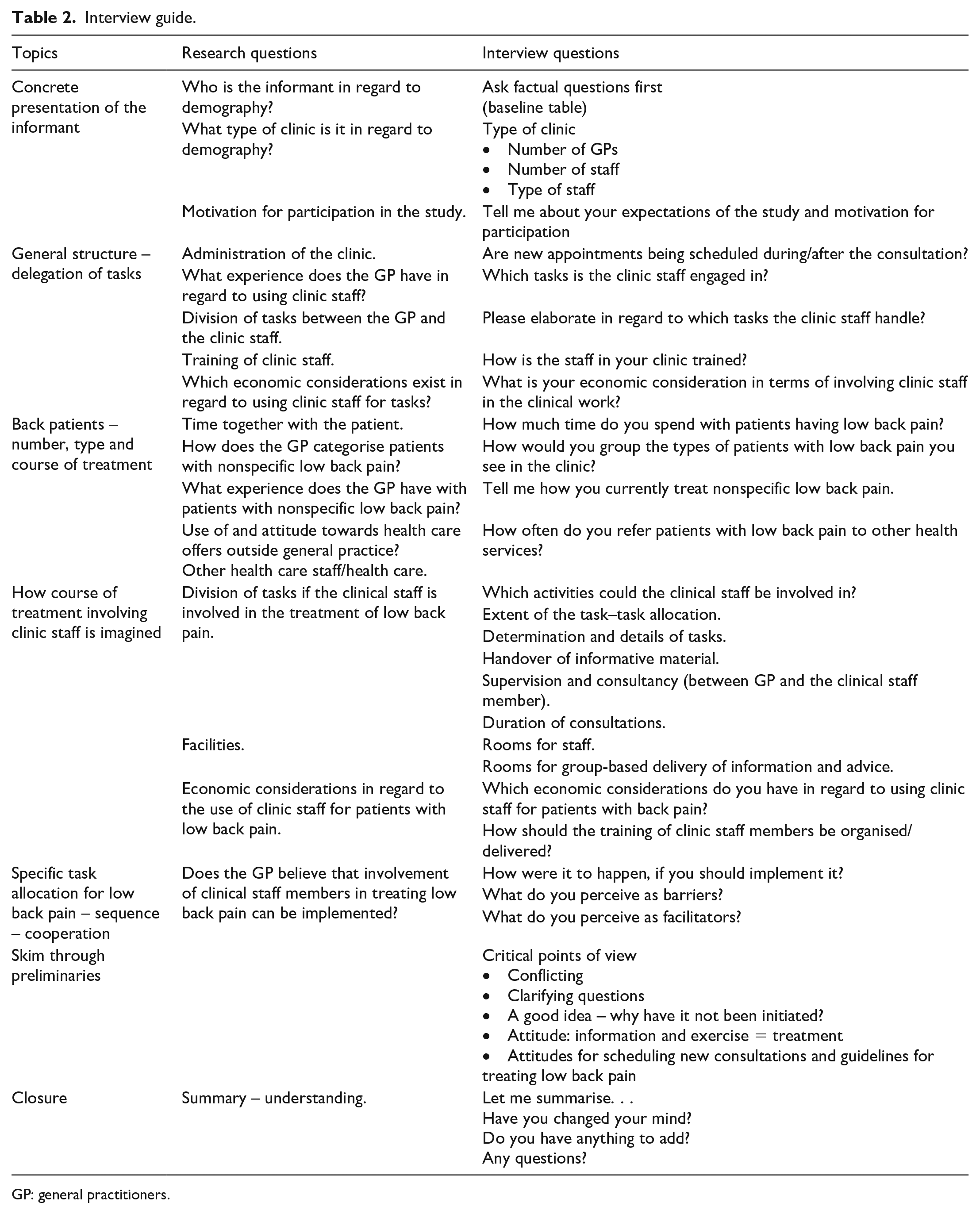
GP: general practitioners.
Data analysis
Interview data was analysed by R.H.K. using an inductive thematic analysis based on descriptive phenomenology. 18 R.H.K. familiarised herself with the data through several rounds of reading and identification of preliminary codes in the transcribed interviews to achieve a deeper understanding of the experiences the GPs described. R.H.K. identified codes using Nvivo 12 software (Alfasoft AB, Gothenburg, Sweden) and organised these codes into preliminary themes in search of meaning and understanding. These codes and themes were discussed with A.R. and T.A. and subsequently redefined, reorganised and labelled. After rereading the transcriptions and adjusting the themes accordingly, R.H.K. wrote a descriptive text including the participants’ experiences within each identified theme. To validate the final analytical results, the transcriptions were reread and recoded by C.A.A. to search for any contradicting evidence. The findings were discussed with R.H.K. and A.R. and incorporated into the final analytical text. An example of the analysis steps is included in Table 3. Results are preprinted at Research Square (DOI: 10.21203/rs.2.11548/v1).
Example of the analysis.

LBP: low back pain.
In step 1, the text was read, preliminary categories were identified, the text was coded and quotes were identified. In step 2, coding of text was placed in the initial categories. In step 3, sub-themes were identified. In step 4, new main themes were identified. In step 5, the text was reread and the main themes were corrected. Finally, the narrative was written.
Results
Eight participants were invited to participate. Three GPs refused to participate because of a high workload in their practices. Consequently, five interviews were conducted in October 2018. Small adjustments were made to the interview guide after the two first interviews. After the initial analysis, the level of information power in the conducted interviews was discussed in the research group and no further interviews were conducted. The participants varied in baseline characteristics (Table 1).
Generally, some GPs were eager to delegate, while others were more reluctant to delegate tasks. Some GPs also described having many patients with LBP, but none of the GPs were currently delegating the care of this patient group to their staff. Through the analytical process, the following main themes emerged: General practice organisation; Delegation to clinical staff members; Doctor–patient relationship; Exercise instruction; Clinical pathway for patients; and External support. The sub-themes within each theme are illustrated in Figure 1.

Themes and sub-themes.
General practice organisation
The GPs all described having experiences in delegating assignments and patient care to nurses, medical students or health care assistants under their supervision. Examples of delegated tasks were controls for diabetes, chronic obstructive pulmonary disease and birth-control pills. The GPs described how they typically delegated tasks to relieve the pressure on themselves, and how a generally increasing work load in general practice due to, for example, outsourcing/relocation/transference of health care from secondary care to general practice had increased the need for delegating tasks to the clinic staff. However, because of the tasks that had already been delegated to the clinical staff members and the balance between these, their readiness for taking on new tasks was affected: Right now I think that there is a longer waiting time for our nurses, than for ourselves [. . .] right now we are holding back on giving them tasks. (#5)
Although some GPs expressed a desire to delegate more tasks to practice staff, economic concerns and the physical space in the clinic limited their opportunities for expansion. Several patients consulted general practice again for continuous treatment after having completed treatments with the physiotherapist. Some of the GPs described how patients with LBP have a strong presence in the everyday clinical life: It’s an incredible number of people, and they have an immensely strong presence in our work day [. . .] in comparison to so many other conditions [. . .] but low back pain really has volume. (#2)
Meanwhile, others did not experience that patients with LBP constituted a group of patients that was sufficiently large to necessitate a change in the current management strategy: It [. . .] is [not] at the top of the list of things I would think, I could delegate to the nurse [. . .] because it does not take up enough time, even though we see some, you know, we see the problem regularly, but they do not go through long courses of treatment most of them [. . .] I cannot see that it would change much. (#4)
GPs described that it was difficult to manage a sufficient back examination within the time frame they have in general practices, and how conversations about LBP often demand extensive explanations to the patient. One of the GPs described how delegating treatment of LBP to the clinic staff would be a new way of involving the staff, but that this is not straightforward, as it involves complex problems. On the contrary, the GP also described how the patient often needed a more pedagogical than medical effort.
Delegating to clinical staff members
Delegation to the clinic staff depended on the staff’s professional and individual competencies. Most commonly, GPs delegated these tasks to nurses and some also delegated to care assistants. One of the doctors also had a medical student employed.
It was explained how the tasks and patient population had to be clearly defined, stable and uncomplicated in order for it to be possible to delegate. There also had to be a certain volume of patients with LBP in order for the staff to gain experience with the task: There needs to be a homogeneity within the patient group, and there has to be some volume of patients for delegation to be suitable. (#2)
Delegating a task to the clinic staff required proper staff training and supporting tools, for example, flow charts clearly defining the patients’ course of treatment as well as ‘red flags’ that would lead to physician involvement. Furthermore, it was explained that delegating task required trust and confidence in the clinical staff and their abilities to acknowledge the limits of their own competencies. Some GPs had scheduled appointments for supervision with their clinic staff, meanwhile all performed ad hoc supervisions.
GPs described how delegating a task required training the clinical staff in the form of theoretical teaching and supervised consultations. The GPs had developed and defined this training themselves and described it as an investment. Consequently, one of the GPs mentioned how it should not be for temporary staff that is, medical students: Training takes time and resources [. . .] it should be for the permanent staff. (#3)
It was expressed how the nurses were especially suited to taking on independent tasks because of their extended education in comparison to other staff groups: We choose two nurses because we believe that they had an education [. . .] that makes them able to handle these things. (#5)
It was described how the nurses were good at following set procedures and at knowing their own limitations, but they also described limits in terms of what the nurses could undertake, for example, nurses are not trained to diagnose: I might fear [. . .] that we still risk. . . losing some, but also risk over-diagnosis [. . .] I think the nurses have more of a tendency to do that than the rest of us. (#1)
Some GPs consequently questioned whether the nurses would be able to manage the first diagnostic consultation with the patient and thereby performing triage, while others could see the nurses performing a pre-consultation in advance of a consultation with a doctor. Regardless, the GPs found follow-up consultations by nurses feasible: ‘[it] could provide the patient with a coordinator, who could offer [. . .] the individual patient some more opportunities for contact than I am able to. [The patient] gets worried [. . .] so I could see the nurses having skills that would be good for accommodating this [. . .] as some of the patients have a need for more frequent consultation, which I am not able to offer them. (#2)
Generally, the GPs did, however, describe that it would require extensive training of the clinical staff members before delegating the treatment of LBP.
GP/patient relationship
The GPs described how delegating tasks to the clinic staff had consequences for their knowledge of the patients and consequently, the continuity of care and the doctor–patient relationship: it [also] harm the continuity, you do get a little out of touch [. . .] because you hand over [the patients], and then it is suddenly [the nurse] who knows them the best. (#4)
GPs described how the knowledge of the patients’ history and the complete medical overview are prerequisites for diagnostics in many in many patient cases.
In more general terms, the GPs described how delegating tasks and patients to clinic staff members affected the tasks they were left with. One of the doctors mentioned how the delegation of simple tasks to the clinic staff members led to doctors treating all the complex problems: Now we have moved the easy stuff [. . .] and then it is replaced with something which is more complex. That is always the risk. (#1)
Another GP experienced great satisfaction in seeing patients with LBP and performing manipulation. This GP was reluctant to hand over these patients to a clinical staff member.
Exercise instruction
GPs described how exercise instruction was part of the treatment for patients with LBP. However, the short time frame at the GP consultation compromised the delivery of exercise instructions. The GPs who instructed patients in exercises did this very quickly and often by recommending websites with exercise programmes: I partly use different web resources [. . .] with good instruction videos [. . .] generally I stick to [. . .] I do not have half an hour like the physios do, so I give one to three exercises max [. . .] because I do not have the time. (#2)
GPs explained how instructing the patients to carry out exercises were within the physiotherapists’ remit and that they often referred patients to them. They also said that they both refer patients to physiotherapists for complete low back examinations and assessments and exercises/training. Several of the GPs described how they often instructed patients in a few exercises that the patient could use while they were waiting for an appointment with a physiotherapist. One of the GPs explained that patients would refrain from doing their exercises if they were not properly instructed.
Other GPs preferred not to step into the physiotherapists’ area of expertise; partly because physiotherapists traditionally perform exercise instruction and partly because physiotherapists are more skilled for these tasks and had the necessary setting: I do not [think] that it is our job [. . .] I [think] the physiotherapists can do it better [. . .] that what we would do, would be a light setup [. . .] when you go to a physiotherapist, [. . .] they have some proper training equipment. (#1)
GPs thought that physiotherapists employed in general practices could help with the diagnostics: If there were to be a physiotherapist here, [. . .] their role should be diagnostics and not treatment. (#1)
However, the GPs did not think that they had enough patients to justify hiring a physiotherapist in their clinic, but that a physiotherapist would be suitable in a large practice with a large patient base.
The clinical pathway for patients
Although the GPs described that they frequently consulted patients with LBP, they rarely scheduled new appointments and thereby creating a predetermined LBP treatment course in general practice: I don’t see particularly many patients with LBP in what I would call predetermined treatment courses. (#1)
The GPs described how they referred to a physiotherapist, but still gave the patients the opportunity of returning to the clinic on their own initiative: [we] agree to talk at a later time. I do not schedule a new appointment [. . .] we have such easy access here [. . .] so I would say ‘well, let’s talk in a couple of weeks’, or ‘we should see each other again if it is not better by then’ [. . .] if they are in the process of a good successful treatment with the physiotherapist, I don’t necessarily need to see them again after 14 days. (#1)
If the GPs scheduled a new appointment for a follow-up, it was mostly given as a precaution for the patient and not necessarily as a planned clinical pathway: I would offer him or her a new control session 14 days after, because then they sort of get a feeling of [. . .] them having some safety net, that they can come back. (#3)
The GPs believed that involving clinical staff members could enable a systematic treatment course for LBP. This could improve the treatment of patients: It would be motivating for patients, and that they are able to come back and talk about ‘well, I did not quite understand the thing he showed me’ or ‘it hurts when I do it’ [. . .] it is definitely possible to imagine that it would be helpful that they see a nurse who would be able to do a follow up. (#3)
It was, however, expressed as important to consider how this should be organised in terms of the division of work between the GP and the clinical staff member: Our collective agreement with the public health care providers, is not suited to patients first [having] ten minutes with the [nurse] and then ten minutes with me. (#2)
GPs said that delegation could potential cause confusion when patients saw different health care professionals in the same clinic. Furthermore, delegation of work could lead to too much repetition of tasks: You would definitely have to be aware that if you divide it too much, what the risks are for both the patients’ sake and in terms of duplication of work. (#1)
External support
The GPs described how they usually introduced a training programme and support tools for the staff prior to delegating tasks. These were developed by the GPs or adapted from clinical guidelines. The GPs also described how they previously had used formalised courses for practice staff. As the GPs considered delegating the treatment of LBP to staff members a larger task, they called for help and support from outside the clinic for example, in the form of clinical guidelines: It would be highly relevant to have a proper guideline from the national society for general practitioners. (#2)
GPs described how the challenge could be addressed by courses for clinical staff members and a proper plan for how tasks are delegated: you could solve that challenge by letting an employee in the regional quality unit for general practice arrange a course for clinic staff members and make a model for implementation. (#3)
Furthermore, GPs said that courses for clinical staff members could strengthen the overall knowledge in the practice: we [also] learn from our nurses [. . .] it could also be them who took a course and came back and taught us how you [. . .] divided management of LBP into different things and then moved forward, and in that manner I actually also think that you would reach most possible general practices if it was the staff you reach out to. (#5)
GPs expected their future work to entail managing more patients with LBP as part of a negotiation of collective agreements with the national health care providers. However, GPs were uncertain of the extent of this and they described it as lacking structure and alignment in this area: What you [. . .] could have use of, and that might be in the program for course of treatment [. . .], that is [. . .] a structured stratification of what non-specific LBP is. Who should be sent to secondary sector, on which indication should they be sent, when should we talk to the back surgeons [. . .] so that it would be easy for the staff to know when they should knock on the door [. . .] that I would [. . .] like to see schematically. (#2) It is a help with things like a flowchart and that it is set up in a schematic manner. (#5)
Another GP added that GPs were interested in enhancing their knowledge about LBP: We only know what we know, you know we have to handle a lot of different tasks, it would be really good for all of us to be upgraded in this field. (#2)
Discussion
Principal findings
This study describes that GPs consider patients with LBP to be a heterogeneous group with a variety of treatment needs. The mapping of the findings below according to the theoretical concepts of capability, opportunity and motivation for introducing a delegation of tasks to clinical staff members 22 highlights the complexity of the issue.
Capability
A barrier for delegating the management of LBP to clinical staff members is the need for clinical support within the practices in terms of staff training and suggestions for specific internal delegation guidelines. Some GPs expressed that the use of clinical staff members to instruct in exercise was considered as a light version compared to referring the patients to a physiotherapist. Letting go of all their easy patients was also considered as a barrier for some GPs.
Opportunity
Some GPs had a large volume of patients with LBP. Consequently, involving clinical staff members could release GP time. Another facilitator for involving clinical staff members was the possibility to improve the uptake of clinical guidelines. The involvement of clinical staff members with a practice nurse education could improve the provision of information to patients and lead to greater self-management among patients with LBP.
Motivation
While some GPs were reluctant to delegate tasks, others were motivated to involve clinical staff members in the treatment of LBP.
Strengths and weaknesses of the study
A population of GPs with a variation in baseline characteristics was recruited to this study. We took several precautions to ensure a strong dialogue in the interviews: all interviews were conducted in the GPs’ own environment; the interviewer was a medical student with plans of becoming a GP, which was considered to build an alliance, and increase the confidence as the interviewer was considered ‘one of us’. At the same time, a medical student would be someone that GPs would be eager to help by explaining their considerations to without the use of esoteric expressions. A weakness of the study was that only one researcher (R.H.K.) did the initial analysis; however, after the initial analysis C.A.A. recoded and checked it. Although sampling was aimed at achieving variation and no new information emerged in the last interview, five participants were a small sample. We need to acknowledge that more participants could have resulted in new information and the sample size is a weakness of the study. In Denmark, physiotherapists usually do not work in general practice. Consequently, GPs do not have experience of this kind of collaboration. Therefore, the findings of the study cannot be generalised to general practices having physiotherapists in the clinic. Physiotherapists are generally more trained in providing advice about LBP and in exercise instruction to patients with LBP than practice nurses. Consequently, we expect that GPs would be less reluctant to involve clinical staff members in treating LBP if physiotherapists were part of the clinical staff in general practice.
Prior to this study, R.H.K. wrote her pre-understanding (Supplementary information) and this was later compared to the findings of this study. The findings of this study are substantially different from the pre-understanding. This validates the analysis process and is considered as a strength.
Comparing findings to other studies and discussion of differences in results
A previous study on the association between degrees of task delegation and GP satisfaction found that greater clinical staff member involvement was associated with increased job satisfaction for GPs. 31 In line with this current study, GPs applied a great variation in the degree of task delegation in clinics. 31 The more positive responses to task delegation in the previous study can be explained by their use of chronic obstructive pulmonary disease as the condition. 31 Patients with chronic obstructive pulmonary disease can be considered as a more homogeneous group compared to patients with LBP and the management with specific examinations for chronic obstructive pulmonary disease and lifestyle advices may be easier to structure and to delegate. Consequently, providing general practice with structuring tools and delegation guidelines can enable them in successfully involve clinical staff members in the management of LBP. However, accordingly to GPs, clinical staff member involvement is most suited for follow-up consultations. This is in line with findings from a survey among GPs regarding the role of practice nurses, where follow-up consultations were found more suited to clinical staff members than new episodes according to GPs. 32 Practice nurses were considered skilled in communication techniques by GPs in our study and oriented communications skills has previously been mentioned as important for improving the care of LBP in primary care. 33 A previous review of qualitative studies found moderate evidence for a lack of communication skills among GPs to negotiate why the guideline concordant advice to stay activity is needed, while patients preferred rest. 34
Meaning of the study
In our study, one GP expressed concerns about exercise instruction being provided in general practice instead of in a physiotherapy practice. However, improving treatment in general practice does not necessarily reduce the use of primary care physiotherapy or chiropractic management. On the contrary, a combined strengthening of all three major primary health care professionals may lead to achieving the overarching aim of reducing unnecessary referrals of patients with LPB to secondary care 13 and taking a multi-professional approach in the treatment of LBP is supported by international guidelines. 13 Meanwhile, patients seek a variety of health care professionals. In Canada, about 54% of patients with chronic LBP seek care only with a GP and between 16%–20% seek combined care with a GP and a physiotherapist or chiropractor, while less than 3% sought care with a physiotherapist or a chiropractor only. 35 Consequently, supporting GPs in managing LBP is essential and releasing GP-time is furthermore important in addressing the shortage of GPs. 36 In the presence of easier access to clinical staff member other than GPs, letting clinical staff members provide information and advice to patients to stay active is a promising solution for general practice. Furthermore, delegating the provision of information and patient education to others, might allocate more time for triage and assessment by the GPs. On the contrary, letting clinical staff members assess and triage the patient might involve a risk of over-diagnosing. Most importantly, general practice and clinical staff members need training to change the management of LBP. This training can be offered by external organisations, already involved in post-graduate training in general practice. The variation in practice size and organisation, the different combinations of health care professionals working in the clinical setting, the staff members’ interests and skills, and the clinics’ tradition for delegating tasks are all reasons to explain why some GPs are motivated for delegation and others are reluctant.
Unanswered questions and future research
Strengthening the treatment in general practice may generate more attention towards which patients will benefit from supplementary treatment in primary care. Involving physiotherapists in the management of LBP can lead to patient involvement in decision-making and more satisfied patients. 37 Furthermore, involvement of practice nurses has previously led to a reduction of unnecessary ordering of diagnostic imaging, 38 but the involvement of clinical staff members may require addressing patients’ expectations, in particular if clinical staff members are to assess and triage the patients. 39 Given the small sample size, further studies to confirm our findings are needed. Future implementation of a broad clinical staff involvement can be carried out by conducting intervention workshops or by more complex interventions. 21 However, the effects of these interventions need to be further proven in future clinical studies, especially where patients’ perspectives are also important when altering the future roles of primary health care professionals. 32
Conclusion
This study describes that GPs consider patients with LBP to be a heterogeneous group with a variety of treatment needs and a patient group without a predetermined content or frequency of consultations; this can be a barrier for delegating these patients to clinical staff members. In addition, some GPs consider the examination and treatment of patients with LBP as a coherent process, which further challenges the division of work between health care professionals.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211039660 – Supplemental material for Involving practice nurse and other assistant clinical staff members in the management of low back pain: A qualitative interview study from Danish general practice
Supplemental material, sj-docx-1-smo-10.1177_20503121211039660 for Involving practice nurse and other assistant clinical staff members in the management of low back pain: A qualitative interview study from Danish general practice by Randi H Knudsen, Janus L Thomsen, Camilla Aakjaer Andersen, Tamana Afzali and Allan Riis in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank the general practitioners for participating in the study and for the invitation to conduct the interviews at their clinics.
Author contributions
R.H.K., J.L.T. and A.R. initially conceptualised this manuscript. R.H.K., J.L.T. and A.R. recruited GPs to the project. R.H.K., C.A.A., T.A. and A.R. drafted the interview guide. R.H.K. conducted and transcribed the interviews. R.H.K. and C.A.A. analysed the data, supported by T.A. and A.R. All the authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Danish Rheumatism Association (R168-A5653) and by the Novo Nordic Foundation (NNF17OC0024422).
Ethical approval
The manuscript does not include patient data. Consequently, the Ethics Committee in The North Denmark Region has stated that ethics approval was not required for the study (2019-000199). The study follows the principles of the Declaration of Helsinki.
Informed consent
GPs received written and verbal information about the study at least one day before the interviews and GPs provided written consent before being interviewed. Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.