
Abstract
Background:
Agricultural producers are frequently exposed to noise that is hazardous to their hearing and cardiovascular health, and have among the highest rates of noise-induced hearing loss of all occupations. However, despite information-sharing approaches, few producers wear sufficient hearing protection. There is a need to develop effective methods of protecting producers from their noise exposure.
Methods:
We provided a series of 2 to 3 short (30-minute) telephone-based motivational interviewing (MI) sessions to noise-exposed agricultural producers. We assessed intervention effectiveness through changes in measuring hearing protector use pre- and post-intervention using a one-group pre/posttest design.
Results:
The sample (N = 29) predominantly consisted of crop producers from Michigan. The mean percentage of time hearing protection was used increased from 44.9% to 51.8% after the intervention, approximately a 7% increase (p =.105). Regression analysis suggested the relationship between intervention dose and use of hearing protection was not correlative.
Discussion/Conclusion:
There was a marginal increase in the use of hearing protection after the intervention, although setting-specific increases in use were uneven. Intervention dose did not correlate with a change in hearing protection use. Further research is warranted to determine the effectiveness of MI, how it compares to information sharing, and to identify intervention dose parameters that promote efficiency.
Background
Agricultural producers (“producers”), commonly known as farmers, are disproportionately affected by exposure to hazardous noise. Agricultural work often involves exposure to machines and livestock that produce hazardously loud noise. Most producers in the US are exempt from protection by the Occupational Safety and Health Administration (OSHA) Hearing Conservation Standard, and thus lack many of the safeguards to hearing afforded to workers in other industries (e.g., workplace health and safety programs, supervision, labor unions, and services of trained safety professionals) (Occupational Safety & Health Administration [OSHA], 2007). Consequently, millions of producers in the US are at increased risk of health complications associated with hazardous noise. While approximately 15% of adults in the US report hearing difficulty, some research has suggested that 80% of producers can expect hearing impairment if current trends continue (NIDCD, 2021). In addition, beyond the well-known detrimental effects of noise on hearing, the Centers for Disease Control and Prevention [CDC] (2020) recognizes that hazardous noise exposure can lead to multiple adverse health conditions, including heart disease, high blood pressure, and psychological disorders (including increased stress, anxiety, and depression).
Although engineering and administrative controls of noise are preferred, these are often not feasible in the farm setting. Previous studies have suggested that approximately half of producers do not wear hearing protection devices (HPDs) when exposed to loud noise, and those who wear them at all usually do not wear them frequently enough to prevent them from the harmful effects of noise (McCullagh et al., 2010). The National Institute of Occupational Safety and Health (NIOSH) (2021) reported that approximately 74% of noise-exposed agricultural and forestry workers did not wear HPDs. Perceived barriers and poor accessibility to HPDs are factors that have been shown to negatively impact use (McCullagh et al., 2010).
Implications for Occupational Health Nursing Practice
The results of our study suggest that occupational health nurses may use motivational interviewing as a useful adjunct or alternative to traditional information sharing for increasing the use of hearing protection among producers. Control of noise exposure among agricultural producers is expected to result in conservation of hearing, as well as reduced risk of cardiovascular and other noise-induced health conditions.
These low rates of HPD use persist despite decades of information sharing efforts by the CDC and other agencies concerned with reducing noise exposure in this population (Themann et al., 2022). Examples include CDC distribution of digital and mailed pamphlets targeted at producers that contain information regarding noise exposure risks and prevention and information centered outreach by organizations concerned with producers’ health (CDC, 2014). These information-sharing efforts have been less than successful, as evidenced by the increasing prevalence of occupational hearing loss in the agricultural sector (NIOSH, 2021). This suggests that the benefits of information sharing have been limited and that a new and more effective strategy is needed to reduce the effects of occupational noise exposure. Loughran et al. (2020) suggested that behavior change methods previously unused in this capacity could have utility beyond information sharing alone. Currently, there is no known effective alternative to traditional information sharing for further increasing hearing protection device use among producers.
Non-educational methods for invoking behavior change, such as motivational interviewing (MI), have been shown to be more effective than traditional information sharing in selected settings and populations (Lundahl et al., 2013). However, MI has yet to be tested with producers and use of hearing protection (Lundahl et al., 2013).
MI is a counseling technique used for eliciting change in health behavior. It primarily involves an interviewer using open ended questions to explore beliefs and perceptions of the interviewee and help the interviewee connect with their own values and desired behavior change (Miller & Rollnick, 2004). MI has broad utility and is more effective than traditional information sharing techniques (Lundahl et al., 2013). It is a brief, inexpensive, and highly individualized method for behavior change that can be implemented in a robust collection of settings, including over the phone or internet (Lundahl et al., 2013).
The principles of MI were used to guide the intervention used in this study. MI is a goal-directed, facilitative counseling approach used to promote behavior change. It is used to elicit change talk in the interest of making a change in behavior. A major focus of MI is the resolution of client ambivalence toward behavior change. Secondarily, the Transtheoretical Model of Change is useful for quantifying an interviewee’s position on the spectrum of behavior change, it may be used to enhance MI or for comparison before, in between, and after intervention (Boston University School of Public Health, 2019). Collectively, these models act as a foundation for which MI can be applied by providing guidance related to interviewee assessment and MI conduction.
The purpose of this pilot study was to determine the preliminary effectiveness of a telephone-based MI intervention in increasing hearing protection device use among producers. In an earlier study, the intervention was found to have high rates of acceptability and mixed results concerning feasibility (Ridge et al., 2022).
Methods
Using a one-group pre-posttest design, the study tested for changes in hearing protector use after the intervention. Following informed consent, participants pre-tested hearing-related beliefs and behaviors, then engaged in a series of telephone-based health coaching sessions with a trained health coach. After the participant’s goals were met, the coaching sessions concluded, and participants were post-tested for changes in hearing-related beliefs and behaviors.
The study recruited participants who were English-speaking adults active in production agriculture at least half-time who also had access to a phone, computer, and internet. Recruitment was accomplished through contact with selected farmer trade groups, snowballing, personal contacts, and flier distribution at a farm trade show.
Information regarding the outcome variable, hearing protection device use in high-noise environments, was collected in a series of five items querying the percent time of use (0 to 100) in the shop, barn, field, grain management system, and during recreational activities (e.g., use of all-terrain vehicles, firearms). HPD use scores were calculated by averaging the percent time of use of hearing protection when in high noise across the five settings. Additional items were queried about hearing protection-related attitudes and beliefs, noise exposure, and participant demographics. All instruments were previously validated (McCullagh et al., 2002) and administered online through a survey management system (Qualtrics).
Interested persons were supplied with a link giving them access to the study survey site, where they were invited to complete an eligibility screening survey and informed consent. After subsequent completion of hearing, noise, and demographic instruments, the project manager contacted participants via email to schedule their first phone-based interview.
In the first session, interviewers built rapport, identified beliefs regarding barriers and motivators related to hearing protection device use, and aided participants in creating their own goals for behavior change. Subsequent sessions were planned based on client need and used to assess progress toward goal achievement and continue to address challenges relating to those goals.
The analysis included both descriptive statistics and bivariate analyses assessing pre- and post-intervention survey data assessing hearing protection use. In particular, linear regression models using generalized estimating equations (GEE) methodology with an exchangeable correlation structure which was used to assess if exposure to the MI intervention was associated with an increase in the percentage of the overall time hearing protection was worn when exposed to high noise (Zeger et al., 1988). Both the unstandardized beta estimate and standard error were reported in the GEE models. Due to the relatively small sample (and specific directionality based on the hypothesized efficacy of the intervention), statistical significance was set at a .10 alpha level. All analyses used STATA 17.0 (Stata Corp., College Station, Texas).
The study protocol was reviewed and approved by the University of Michigan School of Nursing institutional review board.
Results
The total number of participants who initiated the pre-intervention survey was 36; of those, 29 completed the intervention and post-intervention survey. The seven who did not complete the study were lost to follow-up. The dropout rate was approximately 20%, there was no statistically significant difference in demographic characteristics between participants who completed the study and those who did not. Table 1 lists sample demographic characteristics.
Sample Characteristics
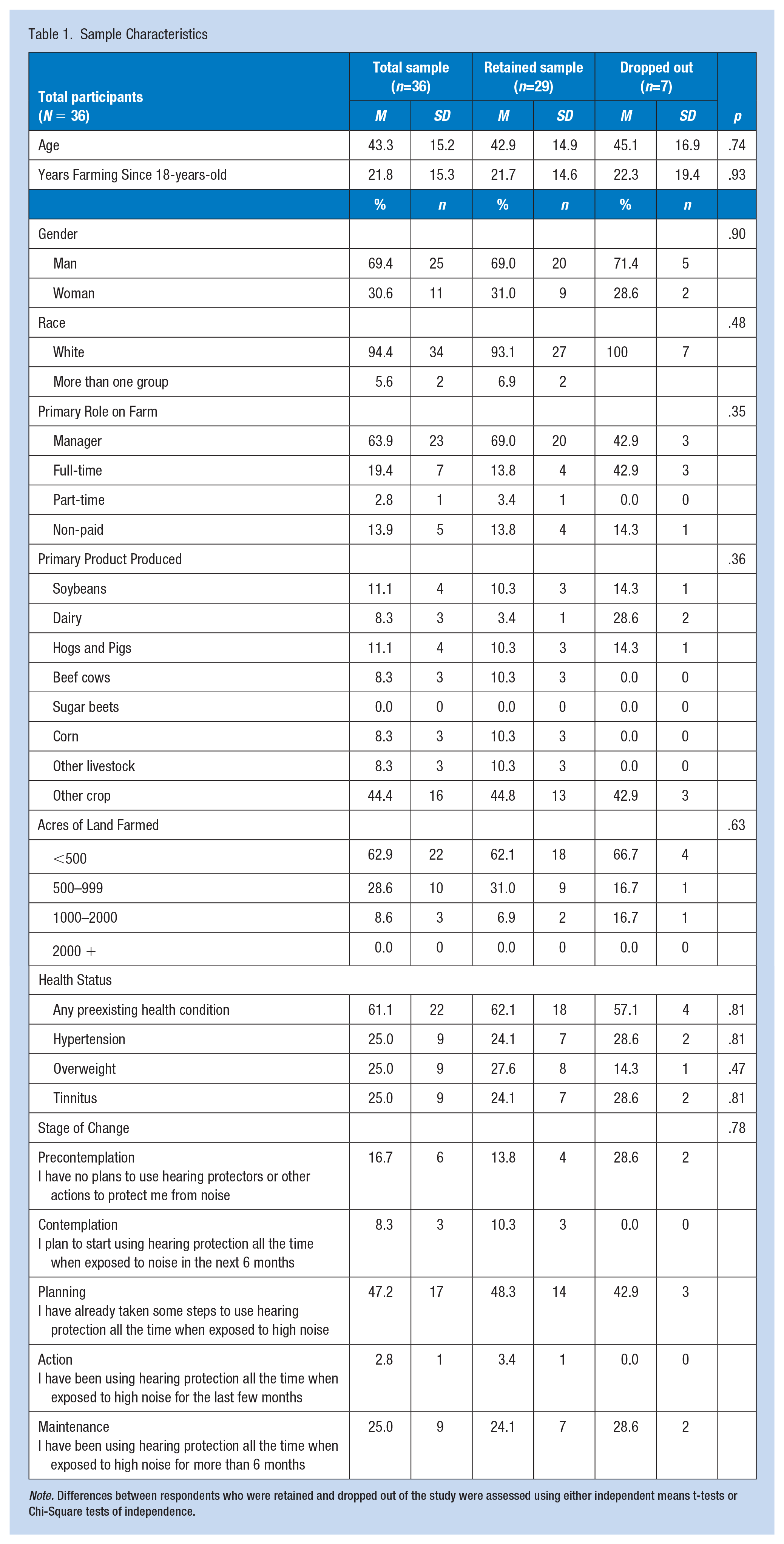
Note. Differences between respondents who were retained and dropped out of the study were assessed using either independent means t-tests or Chi-Square tests of independence.
The typical participant was a 43-year-old non-Hispanic white male farm manager with 22 years of experience and at least one pre-existing health condition. Pre-intervention, the most common self-reported stage of change relative to the Transtheoretical Model was preparation, meaning the average participant was planning to increase their hearing protection use, but had not done so at that time.
Of those who completed the study, 100% reported exposure to high noise. Prior to the intervention, the mean composite percentage of time participants wore hearing protection when in high noise was 44.9%.
The mean number of MI sessions received was 2.4, with a mean total intervention dose of 48 minutes per participant. After the intervention, the percentage of time hearing protection was worn overall increased to 51.8% (p = .105), an increase of about 7%. Table 2 demonstrates the comparison of HPD use prior and after the intervention.
Noise Exposure and Hearing Protection Device Use Before and After the Motivational Interviewing Intervention, Composite Score
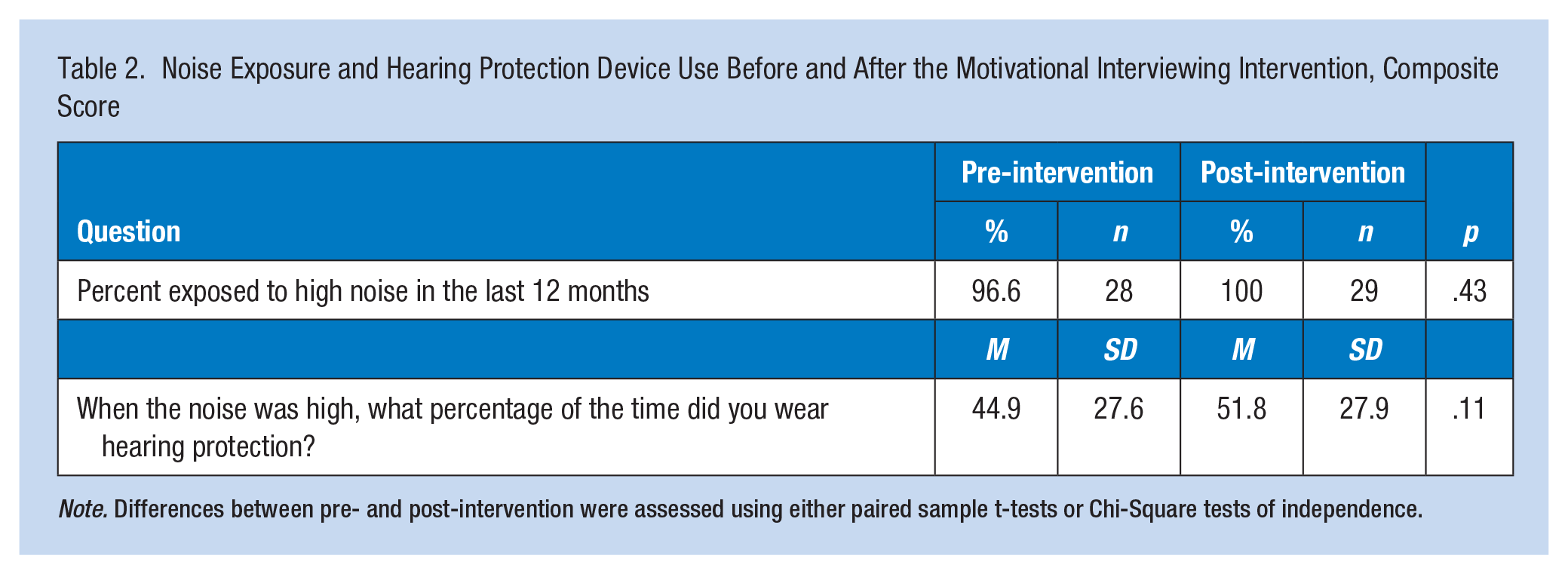
Note. Differences between pre- and post-intervention were assessed using either paired sample t-tests or Chi-Square tests of independence.
Table 3 provides the results from the regression analysis. Model 1 tests for the relationship between exposure to the intervention and hearing protector use. The overall (composite) average percentage of time participants wore hearing protection pre-intervention was 44.9% (α = 44.96, p < .001), which increased to 51.8% post-intervention (b = 6.90, p = .088). Model 2 demonstrates that there was not a statistically significant association between number of sessions and percentage of time hearing protection was used. Similarly, Model 3 shows that intervention dose in total minutes of MI across sessions was not statistically significant regarding its association with the percentage of time participants wore hearing protection.
Intervention Dose Table of Regression
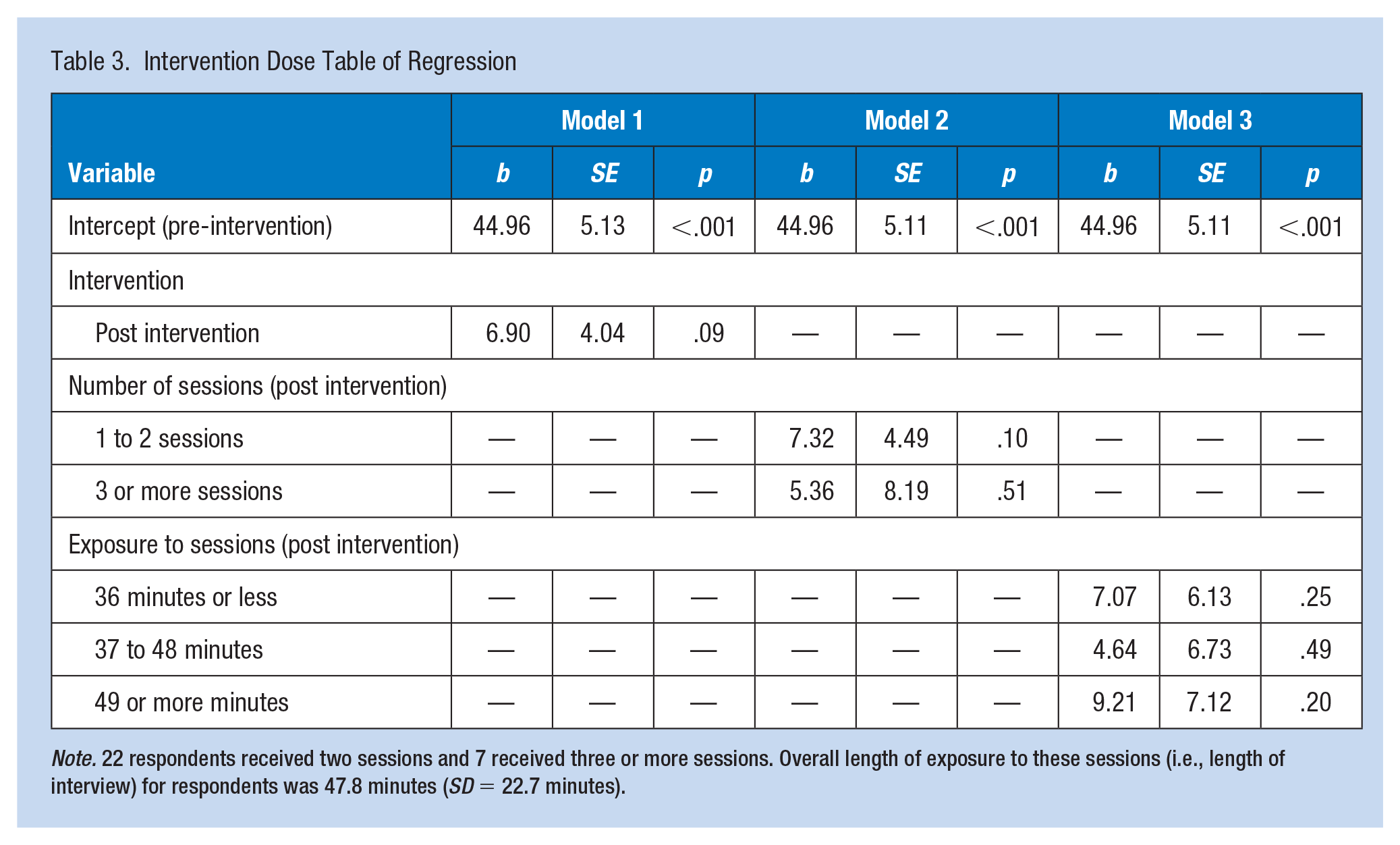
Note. 22 respondents received two sessions and 7 received three or more sessions. Overall length of exposure to these sessions (i.e., length of interview) for respondents was 47.8 minutes (SD = 22.7 minutes).
Discussion
The aim of this study was to determine the preliminary effectiveness of MI as a strategy for increasing hearing protection use among agricultural producers. The high rate of noise-induced hearing loss in this population, along with the low rate of use of hearing protection, point to the need for the development of effective interventions in this worker group. The universal report of exposure to high noise, together with the low rate of use of hearing protection in this sample, affirmed the need for programs to protect these workers.
The percentage of time hearing protection was used while noise was high increased marginally after the intervention. While these study results suggest there may be a positive relationship between phone-based MI and hearing protection device use, the magnitude of the effect may have been dampened by the convenience sample. The study may have attracted producers who had a higher-than-usual interest in hearing health. In addition, regression analysis suggested that intervention dose was independent of hearing protection use outcomes, alluding to the possibility of using shorter or fewer sessions without sacrificing effectiveness in future trials. Further investigation is needed to determine the effectiveness of MI and how the intervention dose relates to outcomes. These future studies would benefit from a larger sample size, random sampling, a control group, and groups who received varying intervention doses.
Historically, MI has been successful in eliciting behavior change in various settings and for a variety of behaviors (Lundahl et al., 2013). This study suggested that telephone-based MI has the potential to increase the use of HPDs. These results are consistent with previous findings and continue to provide evidence that MI may be of benefit in modifying numerous worker health behaviors.
This study also offered some unique contributions to the knowledge of MI. First, few previous studies of MI interventions have measured intervention dose and its relationship to behavior change. In this study, findings indicated a weak relationship between frequency and duration of interventions and behavior change. The relationship between intervention dose and behavior change outcomes was an important one and should be included in future study measurements. Second, this study represents the first known test of MI as an intervention to promote hearing protector use among agricultural producers.
Limitations of this study include constrained recruitment, a small sample size, convenience sampling, and lack of a control group. Recruitment was slower than expected. This is thought to be the result of two historical events. First, the study was conducted during the SARS-COV-2 pandemic, when in-person opportunities for recruitment, generally successful for similar studies, were not possible. Second, slow recruitment led to recruitment activities into the growing season when producers were less receptive to committing to study activities due to perceived schedule conflicts with work responsibilities. Due to these experiences, we recommend future investigations structure their recruitment to take place during the off-season and to take advantage of in-person opportunities for recruitment which often occur during this time.
This novel pilot study provided preliminary evidence that MI may be a useful adjunct or alternative to traditional information-sharing for increasing the use of hearing protection among producers. In addition, it contributes to the understanding of the relationship between MI and behavior modification in this population and can be used to inform future intervention design in this field.
In Summary
Agricultural producers are universally exposed to hazardous noise.
Despite knowledge of and access to hearing protection, many agricultural producers do not use hearing protection devices enough to prevent noise-induced hearing loss and other health problems, such as cardiovascular disease.
Hearing protection use among agricultural producers increased after a brief phone-based MI intervention.
Beyond educational approaches, occupational health nurses may include MI as a strategy to increase workers’ use of noise control and hearing protection.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this study was provided by NIOSH T42 OH 008455 Occupational Health Workforce Training (PI: Batterman). Funding was also provided by Sigma Theta Tau, Rho Chapter.
Ethical approval
This study was approved and deemed exempt from review by the University of Michigan’s IRB on September 1, 2020 (HUM00186053).