
Abstract
Patients undergoing hematopoietic stem cell transplantation are isolated and commonly bedridden. Our aim was to investigate whether a nursing intervention is feasible to increase physical activity after a stem cell transplantation, compared to standard care. A secondary aim was to compare quality of life between the groups. A non-equivalent group pretest-posttest design was applied. Twenty-two patients were included in the standard care group and 21 in the intervention group. The intervention comprised physical activity support pre transplantation, daily during hospital stay, and 14 days post discharge. An activity diary, metabolic equivalent of tasks, the six-minute walking test and the FACT-Anaemia Scale were used for evaluation. This study is reported in accordance with the CONSORT statement. The intervention group was more physically active, walked further in six minutes and seemed to have a slightly better quality of life compared to patients receiving standard care. The nursing intervention increased physical activity and may be associated with a better quality of life in patients undergoing hematopoietic stem cell transplantation.
Background
Annually, more than 50,000 hematopoietic stem cell transplantations (HSCT) are performed worldwide. 1 An HSCT provides patients with new hematopoietic stem cells, either from the patients themselves (autologous HSCT) or from a donor (allogeneic HSCT). For an autologous HSCT, the patient’s own stem cells are collected when the disease is in a quiet phase, and then given back to the patient as support after the conditioning therapy. 2 Allogeneic HSCT is used to treat various malignant and non-malignant conditions, including immune system diseases, and allows for high-dose conditioning regimens, but also utilizes the immune system of the donor to battle the underlying disease. 3
Patients undergoing HSCT are commonly isolated for approximately 2–4 weeks after the procedure because of severe pancytopenia and susceptibility to infections. During isolation, patients require advanced nursing care as they are prone to suffer from nausea, mucositis, pain, fever, fatigue, and psychological distress; the risk of physical inactivity is substantial. 4 , 5 Patients undergoing allogeneic HSCT usually require longer hospital stays than those undergoing autologous HSCT, due to more severe treatment-related complications.6–8 Some patients undergoing autologous HSCT may spend their isolation period in an outpatient setting but are admitted to inpatient care if they suffer severe side effects such as infections, nutrition issues or if they are in need of more help for other reasons.
Physical activity, defined as ‘any bodily movement produced by skeletal muscles resulting in energy expenditure’, 9 is one of the most powerful health-promoting practices that registered nurses (RNs) can recommend. 10 Physical exercise, a subcategory of physical activity, is planned, structured, repetitive, and purposive, aimed to maintain or improve fitness. 11 Recent randomized controlled trials (RCTs) including HSCT patients suggest that physical exercise improves strength, endurance, lung function, functional ability and health related quality of life (HRQoL) and diminishes treatment toxicity. 5 ,12–15 For RNs caring for patients undergoing stem cell transplants it is important to help the patients gain health improvements and prevent adverse events during the commonly inactive isolation period, such as pressure ulcers, back pain, pneumonia and sarcopenia, encouraging them to be physically active – even if it means just sitting in a chair.
Although knowledge regarding the role of physical exercise in cancer care is increasing, the wider concept of physical activity is less examined. To our knowledge, ‘sitting in a chair’ (as compared to lying in bed) as a sort of physical activity has not been investigated in earlier studies of HSCT patients, although bed rest several hours a day is very common in this group. 16 , 17 Extensive bed rest has adverse effects on cardiovascular and muscular systems and causes respiratory complications, including decreased ventilation, atelectasis, and pneumonia, 18 contributing to morbidity and mortality after HSCT. 19 Thus, to increase time spent ‘sitting in a chair’ may be an important way to escalate physical activity in this population.
Increasing patients’ physical activity in a clinical setting may be more challenging than in a research project where patients with severe illness and severe treatment toxicity commonly are excluded. Thus, clinically relevant and feasible strategies to support physical activity need to be developed, tested for feasibility, and thereafter evaluated with regard to efficacy. 20
Objectives of this non-randomized feasibility study were:
To evaluate the feasibility of a nursing intervention aiming to increase physical activity during hospital stay in patients undergoing a hematopoietic stem cell transplantation. To compare HRQoL, medical and clinical outcomes in patients who receive the intervention with patients in standard care.
Methods
Study design
We used a quasi-experimental non-equivalent group pretest-posttest design where the standard care group was included immediately before the intervention group, with an intended allocation ratio of 1:1. A quasi-experimental design is suitable in situations where true experiments (randomization) cannot be used due to ethical or practical reasons as in this study which was conducted in a clinical setting and thus entailed a risk that the intervention would spread to standard care. 21
This study is reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) 2010 statement with extension to randomized pilot and feasibility trials (see online supplementary material file 1) with suitable adaptation of items where necessary. 22
Recruitment and participants
This study was conducted in a clinical setting. Consecutive patients admitted for autologous or allogenic HSCT at the haematology department in Uppsala, Sweden, regardless of diagnosis and according to the clinical waiting list, were approached.
We first included the standard care group between August 2015 and February 2016, followed by the intervention group between June 2016 and May 2017. Patients were only included when the study nurse was on duty, limiting the patients who could be approached for the study and affecting the distribution of patients to the study group as well as prolonging the inclusion time for the intervention group as comparable group sizes were desired. Written and verbal information regarding the study was presented to the patients at their pre-transplant visit and written informed consent was obtained for all patients included in the study before or upon admission to the ward for the transplant procedure.
According to clinical routine, all patients in this study were kept in protective isolation from the day of their transplant until recovery of neutrophil counts (>0.5×109/L). For patients undergoing autologous stem cell transplantation, protective isolation was possible also in an outpatient setting (at home), with twice-daily telephone contacts and physical visits every second day to the haematology ward. Consistent with normal clinical practice, all patients had the possibility to go outside for a walk and had access to resistance bands, dumbbells, exercise bicycles and walking poles on request.
Intervention
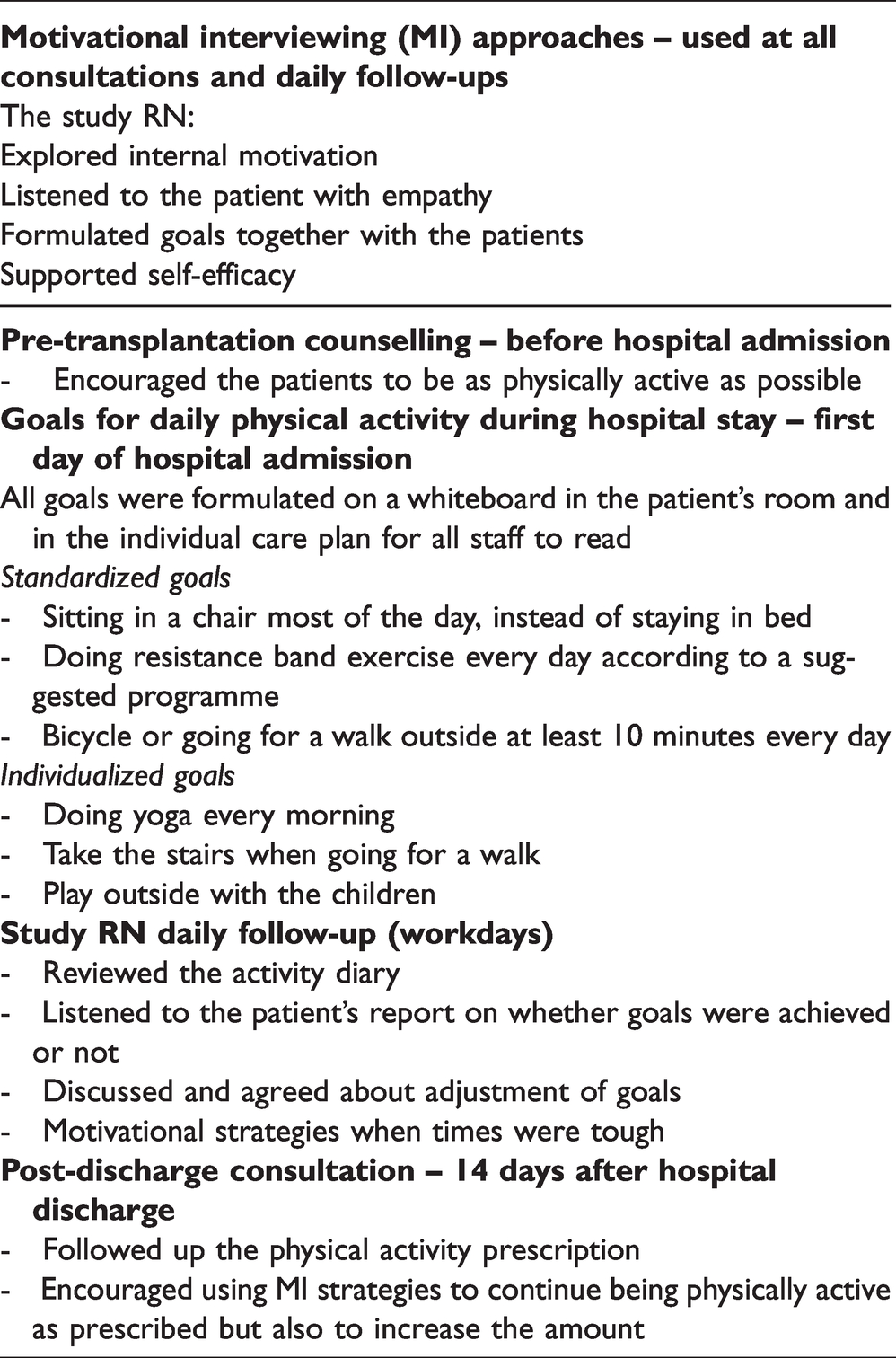
The study RN delivered the intervention. The intervention comprised a pre-transplantation consultation, daily support during the entire hospital stay (weekdays) and a post-discharge consultation (Table 2). The intervention was based on motivational interviewing (MI), a well-established technique which is used to help people find their internal motivation for behavioural changes. 23 Motivational interviewing is a practical, empathetic, and short-term process to inspire and challenge patients using simple advice and goalsetting. The pre-transplantation consultation (baseline) took place 2–4 weeks before the HSCT, either in the hospital ward (autologous HSCT) or by phone (allogenic HSCT) and patients were encouraged to be as physically active as possible before the HSCT hospital admission. The daily support during the hospital stay comprised four standardized goals such as ‘sitting in a chair instead of staying in bed most of the day’, and light to moderate physical activities such as ‘doing resistance band exercise when you are able to’, ‘bicycle’ or ‘going for a walk outside when you are able to’, but they were also allowed to make additional alternative individual goals. In the goalsetting, the patients defined type, duration and frequency of physical activity for each day. These goals, both standardized and individual, were formulated on a whiteboard in the patient’s room, noted in each patient’s individual nursing care plan, 24 and followed up on all weekdays by the study RN, who gave advice and encouragement using MI. Patients were encouraged to take part in everyday cleaning of the room, including making the bed. The goalsetting was essential, whereas the type of physical activity did not matter as much as staying out of bed. At discharge, patients in the intervention group received a prescription for physical activity, 25 including type of activity, how often and for how long on each occasion. Fourteen days post discharge, study subjects received a phone call from the study RN for a follow-up on the physical activity prescription and to encourage them to keep up an active lifestyle.
Baseline characteristics of patients undergoing a hematopoietic stem cell transplantation (HSCT), included in a Standard Care Group (SCG) or a physical activity nurse Intervention Group (IG).
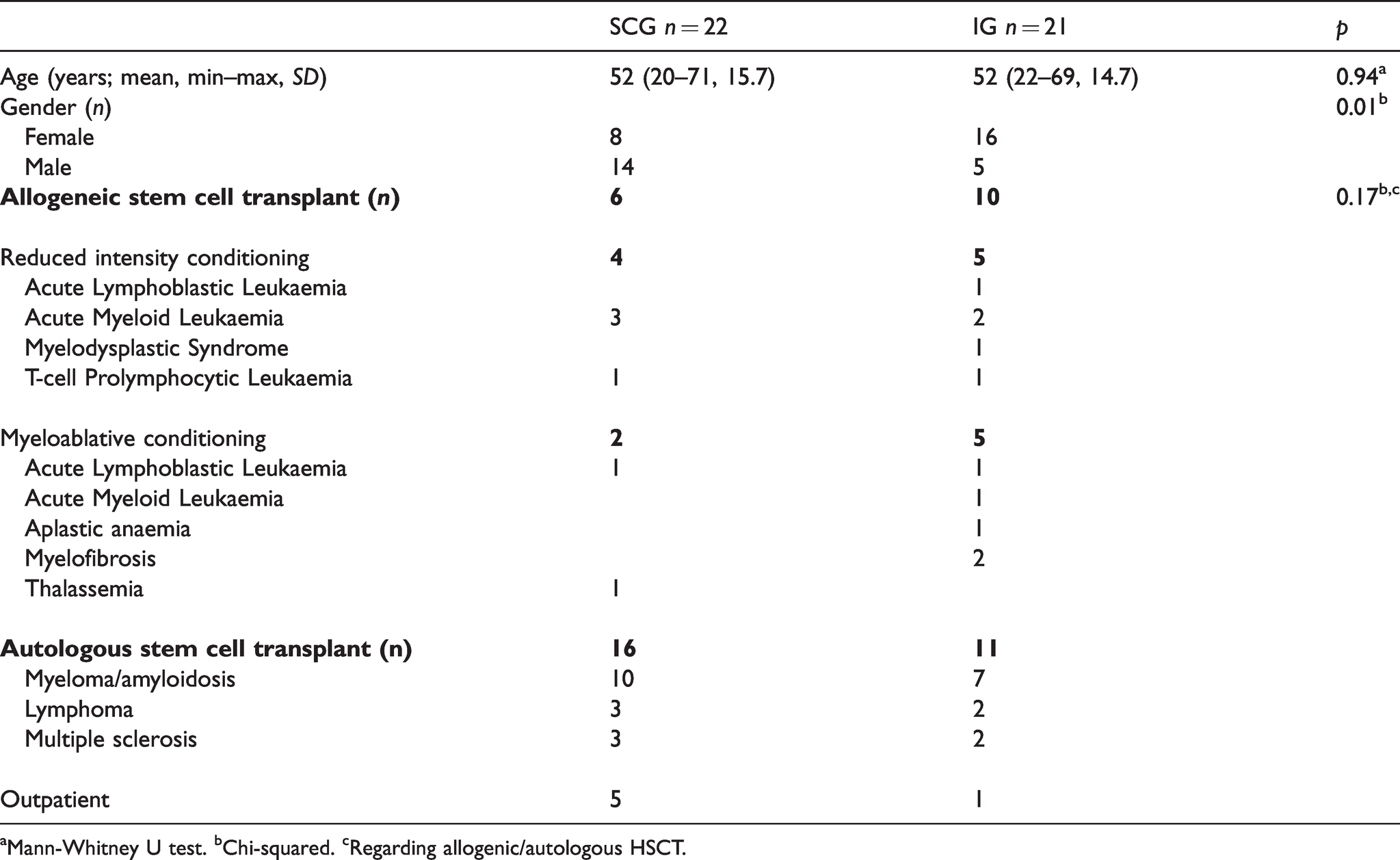
aMann-Whitney U test. bChi-squared. cRegarding allogenic/autologous HSCT.
Standard care
Patients receiving standard care were informed that research indicates that physical activity is important for people undergoing HSCT. They were instructed to keep an activity diary during the entire hospital stay but did not receive any extra physical activity support.
Data collection
The data collection concerned data on feasibility, HRQoL and fatigue, and medical and clinical characteristics.
Data regarding feasibility
Patient-reported activity
All patients reported their physical activities daily during the entire hospital stay, using a project-specific activity diary (see online supplementary material file 2). Patients registered all out of bed activities, such as sitting in a chair, cycling, walking outdoors, doing strength training, taking a shower, cleaning or making the bed, with frequency, duration and type of activity noted. The study RN checked the compliance with the diary every day as part of the daily follow-up session. The Borg Rating of Perceived Exertion (RPE) scale 26 was used to assess exertion during activities on a scale from 6 to 20, (6 = no exertion at all, and 20 = maximal exertion).
Metabolic equivalent of tasks
Metabolic equivalent of tasks (MET) estimates the amount of energy used by the body during physical activity, compared to resting metabolism. One MET is defined as energy expenditure while resting and is equal to 1 kcal per kilogram of body weight per hour. 27 The 2011 Compendium of Physical Activities, 28 quantifies sitting as 1.5 METs and light to moderate intensity activities, e.g. going for a walk, or taking a shower, as 2.0–5.9. METs were calculated for all patients by summing up time spent for each activity (in hours) and multiplying by the Compendium’s defined METs quantified for every activity mentioned.
Six-minute walking test
The six-minute walking test (6MWT) was used to assess physical capacity at admission and at the end of the hospital stay and carried out according to the American Thoracic Society guidelines. 29 Every patient in the study completed the test. The 6MWT is as valid and reliable in patients with cancer as in healthy elderly and patients with cardiac or pulmonary diseases. 30
Health-related quality of life and fatigue
FACT-An
HRQoL and fatigue were measured at admission, discharge and six months post transplant, using the Functional Assessment of Cancer Therapy – Anaemia scale, version 4 (FACT-An). FACT-An comprises aspects which are important to consider when assessing quality of life, fatigue, and anaemia in cancer patients and is proven to offer good reliability and validity. 31 FACT-An consists of FACT-General (FACT-G), assessing physical well-being (PWB), social well-being (SWB), emotional well-being (EWB), and functional well-being (FWB), and the anaemia subscale (AnS) including a fatigue scale. A higher score indicates better well-being on all scales. Cronbach’s alpha varied between 0.68–0.81 at baseline, 0.62–0.84 at discharge and 0.60–0.84 at the six-month follow-up. At all measurement occasions the EWB had the lowest value, all other scales had values above 0.70. Clinically important differences according to estimates derived by Cella et al. 32 have been determined as 4 points for FACT-G total score, 3 points for the fatigue scale, 6 points for the Trial Outcome Index Anaemia (PWB+FWB+AnS) and 5 points for the Trial Outcome Index Fatigue (PWB+ FWB+FS). 32
Medical and clinical characteristics
Medical background data were collected from the medical records as well as duration of isolation period and hospital stay.
Data analyses
As this is a feasibility study, a formal sample size calculation was not performed. Due to the small sample, differences between the intervention group and standard care with regard to physical activity, MET hours, 6MWT, HRQoL and fatigue were analysed using the Mann-Whitney U test or the chi-squared test. All statistical analyses were performed using SPSS (Statistical Packages for the Social Sciences), version 23.
Ethical considerations
The project was approved by the regional ethical review board in Uppsala (Dnr 2015/090) and adapted to the General Data Protection Regulation (GDPR) standards. All procedures were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The intervention implicates a presumed improvement in the care of patients undergoing HSCT. Potential risks may arise if any participant performs physical activity in an incorrect or not recommended way. These potential risks were limited by daily follow-ups and access to a physiotherapist and medical staff. Physical activity goals were also adjusted daily depending on the medical status of the patients to avoid harm, but also to reduce the risk of feeling ‘inadequate’ by not fulfilling daily goals due to medical reasons. Answering questionnaires might be perceived as violating privacy, but the patients were informed by the study RN repeatedly that answering the questions was voluntary, and that they could withdraw their consent at any time.
Results
Twenty-two of 59 eligible patients (37%) were included in the standard care group between August 2015 and February 2016 and 21 of 137 eligible patients (15%) were included in the intervention group between June 2016 and May 2017 (Figure 1). One eligible patient declined study participation and three approached patients were excluded due to cognitive or physical disability or inability to read and write in Swedish. A larger proportion (48%) of the participants in the intervention group underwent an allogeneic HSCT compared to 27% in standard care (Table 1). Only 1 of the 11 patients in the intervention group who underwent an autologous HSCT was managed as an outpatient compared to 5 out of 16 in standard care. None of these differences were statistically significant but suggest that participants in the intervention group were more fragile (lower proportion of patients in outpatient care) and received a tougher conditioning treatment (higher rate of allogenic transplants), compared to participants in standard care. A gender difference was observed between the groups with fewer men in the intervention group (24%) compared to standard care (64%) (p = 0.01; Table 1).
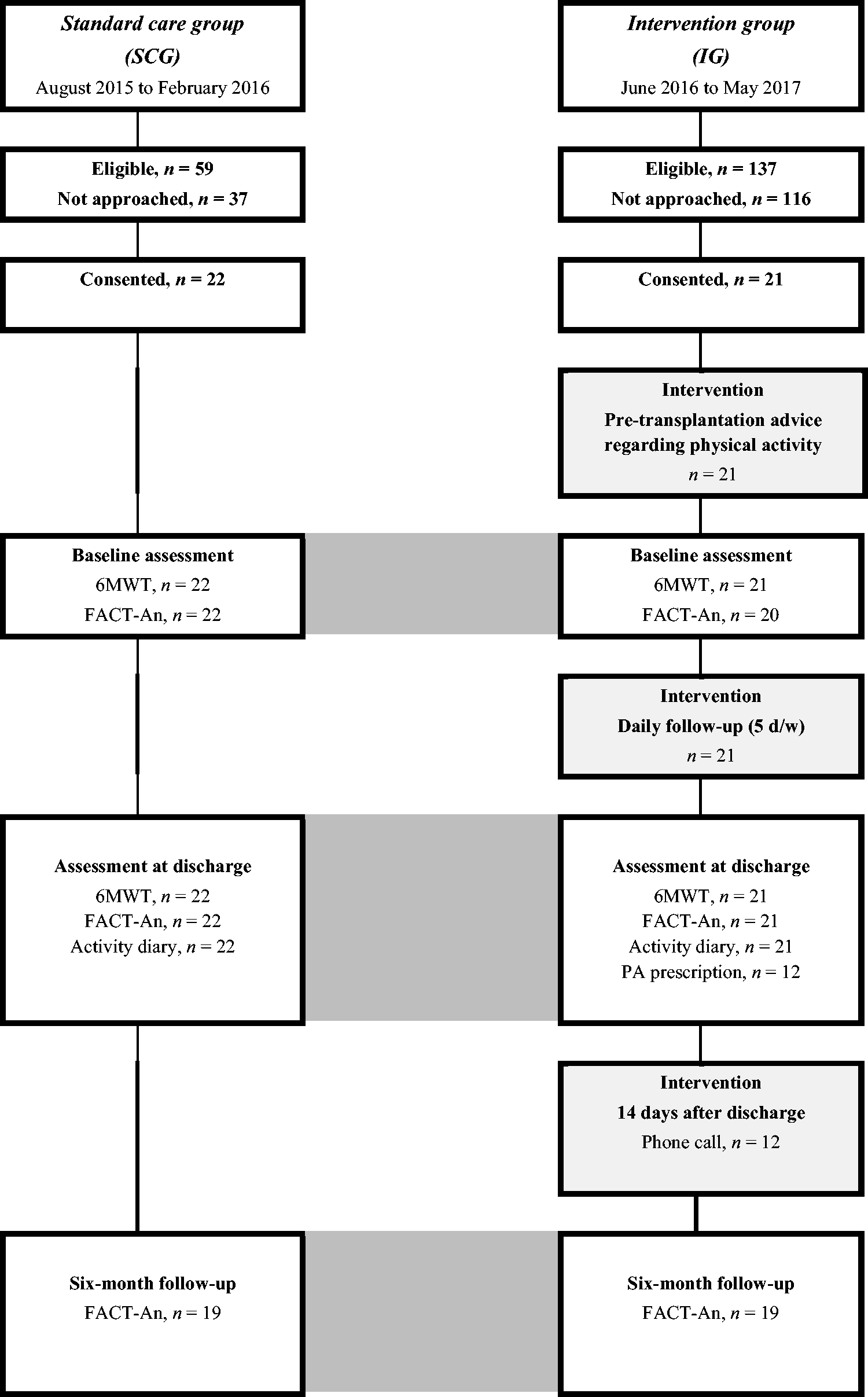
Flow chart for the study.
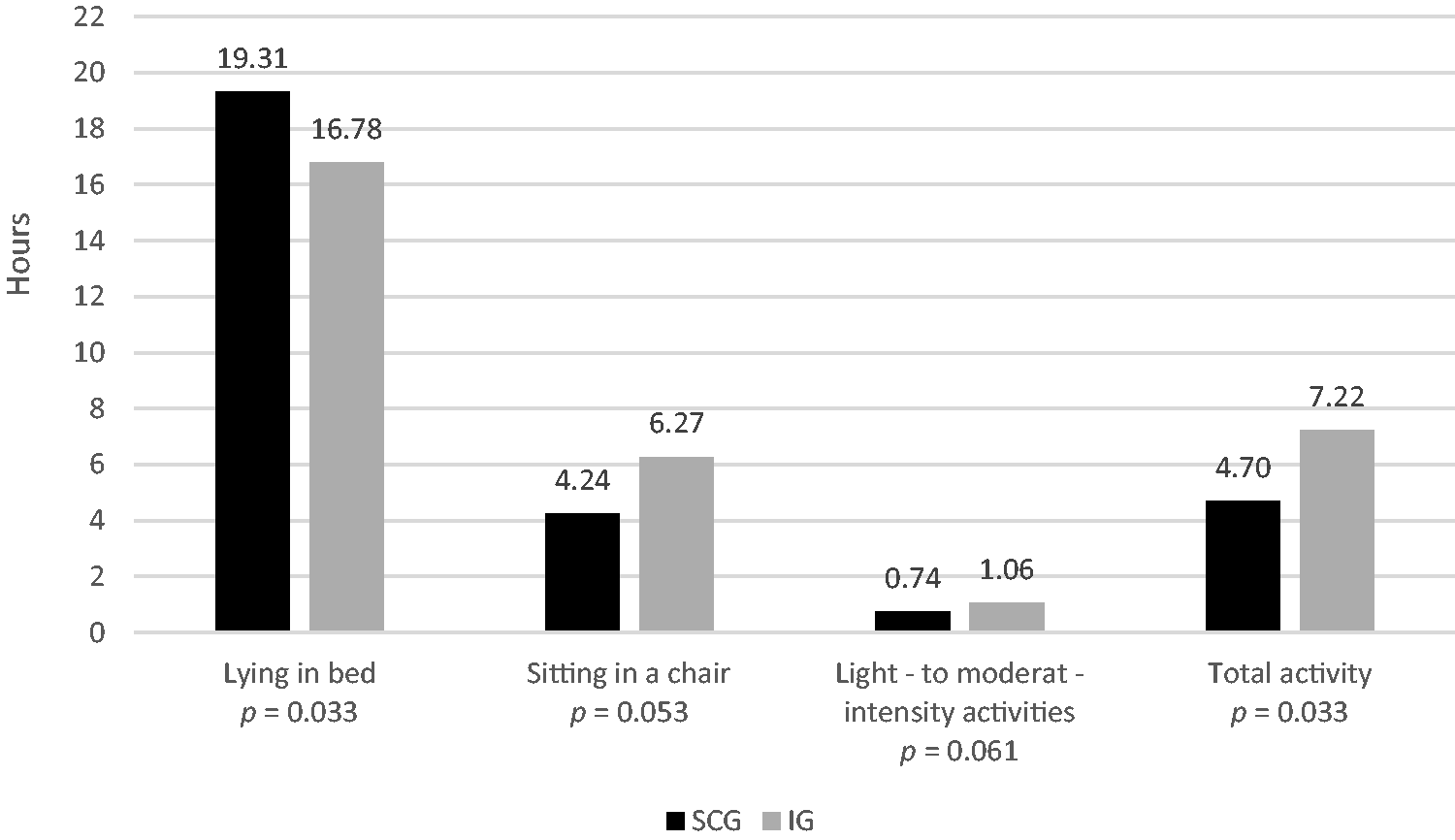
Feasibility outcomes. All activities mentioned in the diaries, showing median hours per day for patients undergoing a hematopoietic stem cell transplantation (HSCT), included in a Standard Care Group (SCG) or a physical activity nurse Intervention Group (IG).
Feasibility of the nursing intervention
Patient-reported physical activity
Patients in the intervention group were more physically active compared to patients receiving standard care, and reported more light to moderate intensity activity – 1 hour vs. 45 minutes (median) per day (p = 0.06) – and time sitting in a chair – 6 hours and 16 minutes vs. 4 hours and 14 minutes (median) per day (p = 0.05). Patients in the intervention group were consequently less bedridden – 16 hours and 46 minutes vs. 19 hours and 18 minutes (p = 0.03) per day – compared to patients receiving standard care. There were no differences concerning the number of activities out of bed or the perceived exertion on the Borg RPE scale (Table 2), although a tendency for higher values was seen in the intervention group. The most frequent prescription for physical activity chosen at discharge was ‘going for a walk’ for 30 minutes daily.
Feasibility outcomes. Comparison of MET hours, number of activities out of bed, exertion on Borg RPE scale and distance walked in 6MWT for patients undergoing a hematopoietic stem cell transplantation (HSCT), included in a Standard Care Group (SCG) or a physical activity nurse Intervention Group (IG) (Mann-Whitney U test.).
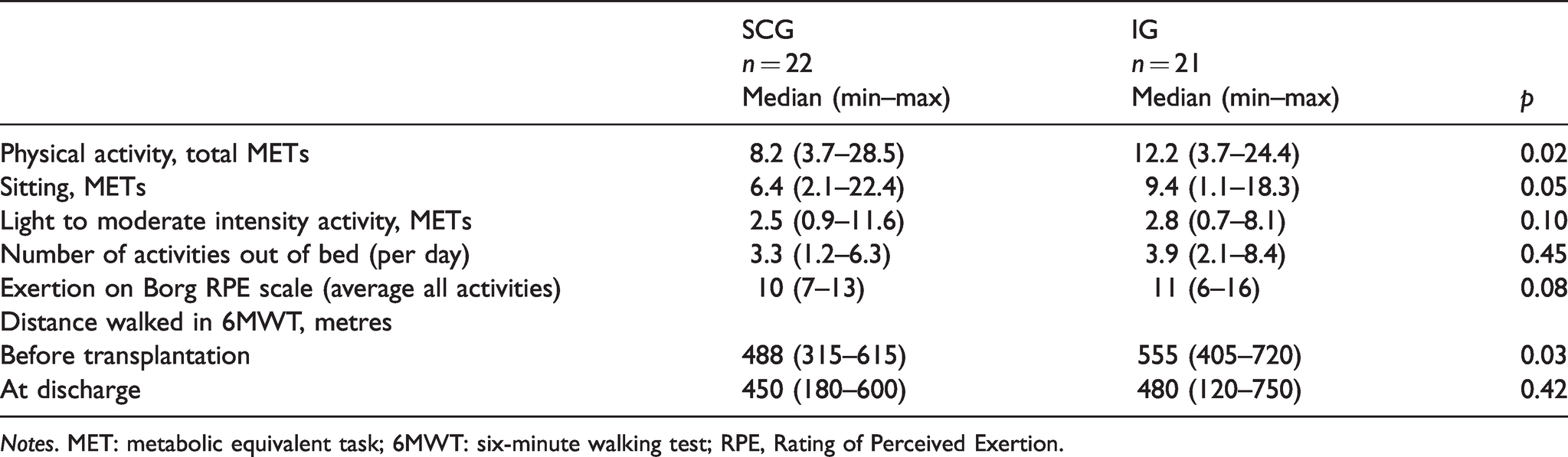
Notes. MET: metabolic equivalent task; 6MWT: six-minute walking test; RPE, Rating of Perceived Exertion.
METs
The mean daily METs was 12.4 in the intervention group and 8.2 in standard care (p = 0.02; Figure 2). The mean daily METs from sitting in a chair totalled 9.4 in the intervention group and 6.4 in those receiving standard care (p = 0.05). There was no statistically significant difference regarding METs from light to moderate intensity activity.
Six-minute walking test (6MWT)
Patients in the intervention group walked a longer distance (555 m) than patients receiving standard care (488 m) at baseline 6MWT (p = 0.03). The 6MWT distances shortened by 14% in the intervention group and 8% in patients receiving standard care at discharge. However, patients in the intervention group walked almost as many metres at discharge (480 m) as patients receiving standard care did at baseline (488 m; Table 2).
Health-related quality of life
FACT-An
There were no statistically significant differences between the intervention group and standard care regarding HRQoL or fatigue. However, according to the estimates derived by Cella et al. 32 there were minimal clinically important differences between the intervention group and standard care with regard to fatigue (median 37 vs. 34), the Trial Outcome Index Anaemia (116 vs. 110), the FACT-G total score (156 vs. 152), and the Trial Outcome Index Fatigue (91 vs. 86) six months post discharge. Fatigue remained stable from before the start of transplant treatment to discharge (median 37 at both time points) in the intervention group but worsened in patients receiving standard care (from median 41 to median 34) (Table 3).
Comparison of HRQoL and FACT-An for patients undergoing a hematopoietic stem cell transplantation (HSCT), included in a Standard Care Group (SCG) or a physical activity nurse Intervention Group (IG) (Mann-Whitney U test).
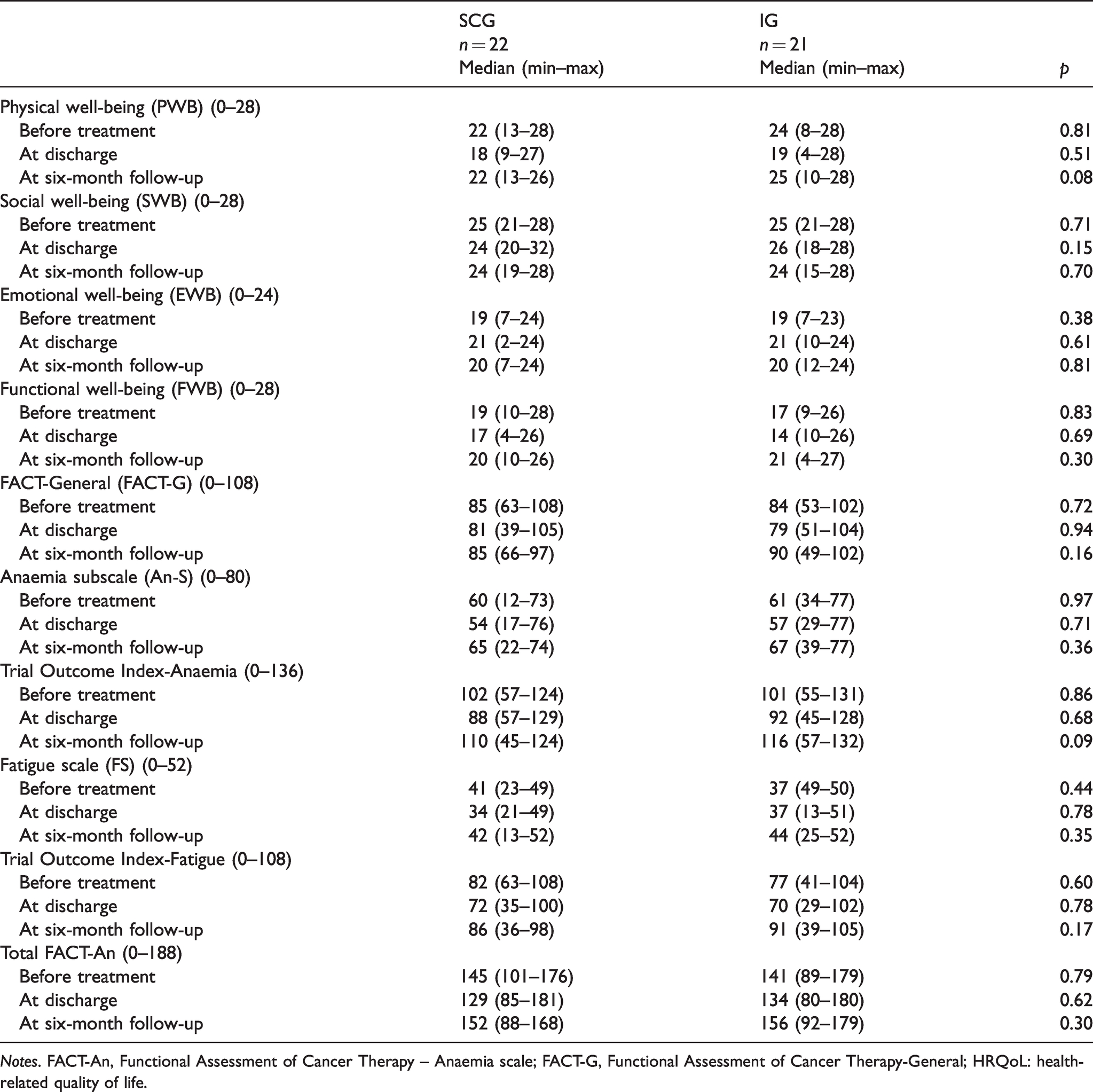
Notes. FACT-An, Functional Assessment of Cancer Therapy – Anaemia scale; FACT-G, Functional Assessment of Cancer Therapy-General; HRQoL: health-related quality of life.
The content, structure, and timing of the registered nurse (RN) intervention aiming to increase physical activity in patients undergoing a stem cell transplantation.
Medical and clinical characteristics
No differences regarding duration of hospital care, time in isolation, need of intravenous antibiotics, or number of transfusions were observed between the two groups. No adverse events related to physical activities during the study were reported.
Discussion
Patients who received a physical activity intervention during the hospital stay were more physically active than patients who received standard care. Patients in the intervention group were less bedridden, spent more time sitting in a chair, performed more light to moderate intensity physical activities and reported more MET hours than patients receiving standard care, suggesting that the intervention was feasible and that RNs are well situated to support patients undergoing an HSCT to be more physically active. In addition, patients who received physical activity support did not experience worsening fatigue during hospital stay and a slightly better HRQoL was indicated after six months compared with patients receiving standard care. Thus, physical activity support provided by RNs in clinical haematological care may be associated with improved patient-reported outcomes, although properly designed effect studies are required to study the effects of increased physical activity.
Motivating patients undergoing HSCT to be physically active during the hospital stay is a challenging task. Incentive primarily comes from a readiness to change something in life, but according to our experience, many people undergoing HSCT need all their energy to cope with the disease and treatment. Nevertheless, it may be possible for RNs to support patients to increase their level of physical activity leading to associated benefits for the patients. A recent meta-analysis confirmed that early physical exercise might help prevent decline in muscle strength caused by immobility and prolonged bed rest in HSCT patients. 33 Daily exercise programmes encompassing a wide variety of tools, such as bicycles and strength training equipment, have been used to increase physical activity during isolation after an HSCT. 12 , 34 However, a need for more low-intensity exercise interventions suitable for clinical practice has been identified. 5 Our study aimed to meet this challenge and the intervention was applied in a real-world clinical setting. We found that it was possible for patients to be physically active in an isolation setting and that physical activity could be increased using simple tools and exercise programmes supported by an RN. To succeed, we believe that individual care plans including goalsetting, advice and regular follow-ups are crucial. The activity diary and individual goalsetting are simple and appreciated tools to encourage HSCT patients to engage in physical activity, and have been used in previous studies, although most often in the outpatient setting. 35 All patients in our study used the diary as instructed and tried to continue their physical activity throughout the hospital stay. Daily follow-up visits by the study RN, who used an MI approach to inspire and evaluate goals, give simple advice, and challenge the patients, was used in the intervention. Tarasenko et al. 36 found that healthcare providers’ recommendations are associated with higher levels of leisure-time aerobic physical activity among cancer survivors; using an MI approach makes this even more effective. 23
To our knowledge, sitting in a chair instead of lying in bed as an ingredient in physical activity in patients isolated due to an HSCT has not been investigated previously. According to our results, sitting in a chair was the physical activity most easily increased by the intervention. Some patients estimated sitting as very exhausting, possibly making sitting instead of lying in bed an important physical activity strategy for this severely ill group of patients. This is supported by Morishita et al., who described it as a sedentary intensity physical activity. 37
Jarden et al. 13 found that fatigue was the most prevalent symptom for patients undergoing HSCT. Interestingly, the patients in the intervention group maintained their fatigue levels from baseline to discharge, whereas fatigue worsened for those receiving standard care. However, the effects of physical activity support, provided by RNs in a clinical setting, on patient-reported outcomes need to be evaluated in randomized controlled trials.
Patients in the intervention group walked longer distances in the 6MWT before treatment start than the patients receiving standard care did. We believe that this partly can be attributed to the physical activity advice given to the patients in the intervention group pre transplantation setting, indicating that verbal advice only may be of importance to increase physical activity before an HSCT. Liang et al. reported, in their meta-analysis, that the optimal timing of physical activity for patients undergoing HSCT is in the pre-transplantation phase. 33 Previous studies have concluded that supervised exercise prior to HSCT is safe and feasible 38 and that patients in partly self-administered pre-transplantation physical exercise programmes can become stronger and achieve better physical condition compared with a control group. 39
The reduced physical capacity at discharge in the intervention group was expected, since about half of them underwent the tougher myeloablative regimens. However, the 6MWT distances of patients in the intervention group at discharge were close to those of patients receiving standard care at baseline. An important finding was that the RN managed to support patients undergoing HSCT to achieve the same level of physical capacity as patients in previous studies, comparing 6MWT before and after HSCT. 37 , 40
Strengths and limitations
The main strength of the present study is that it was conducted in a clinical setting and that the physical activity support administrated by a study RN was possible to implement without large additional costs. Satisfactory Cronbach’s alpha values support the use of FACT-An in our study population. A quite large proportion of patients in the intervention group underwent an allogenic HSCT which is a tougher treatment than autologous HSCT. This complicates the comparison between the groups but suggests that the intervention is feasible also for more severely diseased haematological patients. Future studies regarding implementation of physical activity support in routine care should apply strategies to ensure equal groups when it comes to treatment regimens. Another limitation was that the baseline assessment was conducted after the intervention group received the pre-transplantation consultation about physical activity, which made it impossible to determine whether the noted difference regarding the 6MWT was due to the pre-transplantation consultation or other initial differences between the groups. Thus, a more precise design should have been applied. Due to the unanticipated increased need for the study RN to work in routine care, data have not been reported earlier. Although a limitation of this study, strategies for physical activity support in a clinical setting are, although highly warranted, still lacking, making the findings current and relevant.
Conclusions
A structured intervention to increase physical activity in patients undergoing HSCT seems to be feasible in routine care. An increase in physical activity may be associated whether a better HRQoL indicated by clinically important differences from the FACT Anaemia Scale. However, larger studies with a more rigorous design are needed to evaluate the effects of physical activity support on patient-reported outcomes.
Supplemental Material
sj-pdf-1-njn-10.1177_20571585211005439 - Supplemental material for Is it possible to increase the amount of physical activity in patients isolated due to hematopoietic stem cell transplantation using a nursing intervention? A feasibility study
Supplemental material, sj-pdf-1-njn-10.1177_20571585211005439 for Is it possible to increase the amount of physical activity in patients isolated due to hematopoietic stem cell transplantation using a nursing intervention? A feasibility study by Sölvi Vejby, Anna Eriksson, Karin Nordin and Birgitta Johansson in Nordic Journal of Nursing Research
Footnotes
Author contributions
All authors contributed to the acquisition, analysis, and interpretation of data for the work, although the majority of the practical data acquisition was made by the study RN (S. Vejby). All authors drafted the work and revised it critically for important intellectual content, approved the final version to be published, and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the Swedish ‘Blodcancerfonden’. The support was granted without any kind of involvement in the conduct of the research or the preparation of this article.
Declaration of conflicting interests
The authors declares that there is no conflict of interest.
Supplementary material
The supplementary material is available online with the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.