
Abstract
Background:
Workers in production agriculture are frequently exposed to high noise levels and face unique barriers to implementing hearing protection, leading to occupational hearing loss. Motivational interviewing is a promising approach to assist workers in preserving their hearing.
Methods:
This pilot study used a mixed-method approach to evaluate the feasibility of an innovative motivational interviewing intervention for agricultural producers from February to May 2021. Qualitative data included coaches’ and participants’ comments and were coded using a structural coding approach. Quantitative data included Likert-type-style responses given by participants in a post-intervention survey. Data types were then integrated.
Results:
Sixteen participants were recruited during the 4-month pilot. Participants’ satisfaction scores averaged above six on a 7-point scale for all satisfaction questions. Implementation factors included the intervention’s flexibility, services provided by the coaches beyond motivational interviewing, and difficulties with recruitment.
Conclusions/Applications to Practice:
This motivational interviewing intervention was highly acceptable to participants, but factors affecting implementation may challenge scalability.
Background
In the United States, occupational hearing loss caused by noise exposure is the most common work-related illness (National Institute for Occupational Safety and Health, 1996). Noise exposure is an especially severe issue for those working in production agriculture, as they are frequently exposed to high noise levels. Researchers have documented hearing impairments rates as high as 80% among agricultural producers (Carruth et al., 2007).
However, these producers are not mandated by systems designed to protect workers in other occupational sectors (i.e., Occupational Safety and Health Administration, 2008). By a large margin, most farms in the United States are small, family-run operations (United States Department of Agriculture, 2022). As such, many farm operators experience unique barriers using hearing protection devices (HPDs) due to their role as small business owner-operators who are primarily concerned with the fiscal stability of their businesses. Production agriculture workers cite challenges to using HPDs as the fear of missing important mechanical sounds or communication during work that may result in negative consequences to the financial well-being of their business (Carruth et al., 2007; McCullagh & Robertson, 2009). Farm operators rarely are served by hearing health services such as noise level monitoring, annual audiometric testing, and training in use of HPDs (Masterson et al., 2018).
Although many workers recognize the hazards to hearing associated with noise exposure, fewer are cognizant of the hazards that noise presents to their health beyond the auditory system. For instance, noise exposure is associated with worsened cardiovascular health (e.g., high blood pressure, heart disease, heart attack, and stroke), obesity, fatigue, headache, and high blood sugar (Basner et al., 2015; Kerns et al., 2018; Münzel et al., 2014; Pyko et al., 2015; Ristovska et al., 2014; Tzivian et al., 2015; Yoon et al., 2015).
Educational approaches associated with noise exposure have had limited results in promoting behavior change (McCullagh et al., 2016). Researchers have found that simply providing information to farmers produces increases in health literacy without producing behavior change and that greater involvement among agricultural producers in these initiatives was both more desirable and effective (Kline et al., 2008). Thus, there is a need to better understand other strategies for behavior change. Motivational interviewing (MI), which provides health coach–facilitated counseling sessions, is one such strategy. MI works to identify barriers affecting change in partnership with participants and to assist participants toward achieving a specific behavior change. This technique has been successful in many health behaviors including prevention of noise exposure (Rubak et al., 2005; Solheim et al., 2018; Zomahoun et al., 2016). MI can be effective when administered remotely, with telephone-based interventions, showing particular promise (Patel et al., 2019). The purpose of this study was to describe the feasibility of an innovative MI intervention designed to improve use of noise control strategies among agricultural workers by assessing its acceptability and implementation.
Methods
Motivational Interviewing for Hearing Protection
This innovative intervention pilot was designed to improve use of noise control strategies, particularly adherence to HPD use, among agricultural producers using an MI approach. Agricultural producers were recruited remotely via study team attendance at Michigan Farm Bureau meetings and circulated flyers. To participate, producers had to work in agricultural production at least half-time, be of 18 years of age, capable of receiving the intervention in English, and have a reliable phone connection. Once producers confirmed eligibility and completed a pretest, they were connected to one of four study team members, all of whom were nurses who had completed additional training in MI. Figure 1 summarizes this process for the February–May 2021 portion of this pilot.
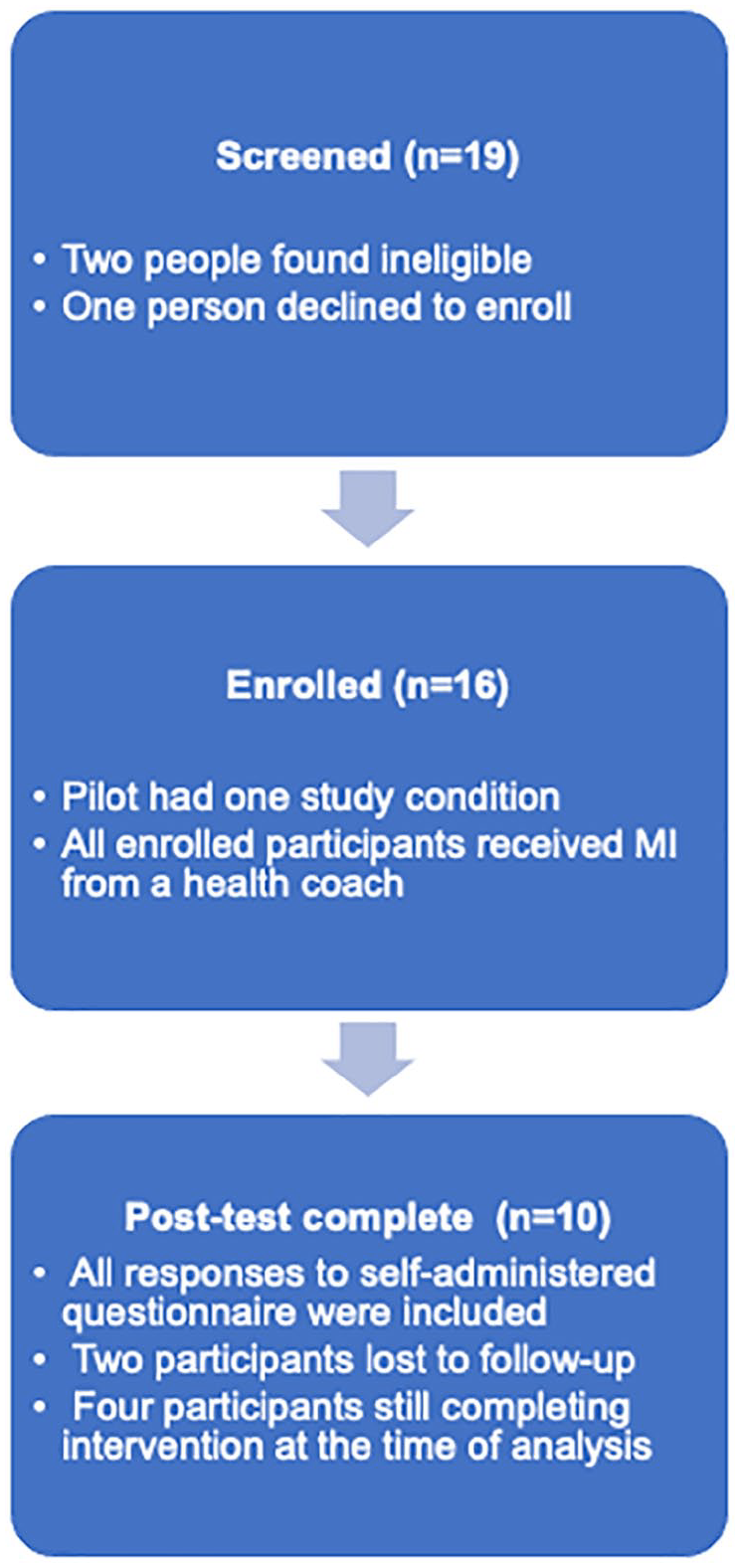
Flow of participants through pilot study.
Each coach used the tenets of MI to assist the participant in understanding and therefore improving adherence to HPDs, primarily by identifying and addressing barriers to their use, and discussing whether new approaches had, in fact, increased HPD use. Two or three MI phone sessions were scheduled at the participants’ convenience, with coaches and participants maintaining contact via email in between sessions. Throughout the intervention, coaches also maintained field notes on participant meetings, and met weekly to discuss progress. After completing their sessions, participants completed a posttest assessing for satisfaction and behavior change. Participants were offered $30 as an incentive.
Evaluating the Program for Feasibility
This feasibility study took a convergent parallel mixed-method approach (Creswell, 2014), with quantitative and qualitative data collected simultaneously throughout the first phase of the intervention pilot, February to May, 2021. End of May was selected as the time for analysis as recruitment was anticipated to slow during subsequent months due to the seasonal work patterns for this agricultural worker group. A posttest from June 3 was included in the analysis; subsequent tests were not. Of the components of feasibility identified by Bowen et al. (2009), we selected acceptability and implementation as our two areas of focus. These components captured both the participants’ and the study teams’ experiences and explored facets of those experiences that were of greatest concern to the study team.
Bowen et al. (2009) defined acceptability as the participants’ reaction to the program. Reaction was assessed quantitatively via the participant retention rate and response to satisfaction questions administered in a participant posttest. Posttest questions, given as a self-administered computer-based questionnaire, were designed to assess reactions to specific components of the program as well as the program overall. Participant reaction was assessed qualitatively by coding field notes made by study team members and the free-text comments participants entered in the posttest using a structural coding approach. Structural coding is well suited to studies exploring specific research questions, in this case, “How did participants react to the intervention?” (Saldaña, 2021). Furthermore, this approach allowed the researcher to compare the relative frequencies of certain findings (Saldaña, 2021). Two researchers coded the data independently and then discussed their findings to resolve any coding discrepancies.
Bowen et al. (2009) proposes the question “What factors affect implementation ease or difficulty?” to assess implementation. Quantitative implementation measures included: responses to posttest questions designed to assess the participants’ attitudes toward intervention delivery, the number of participants who had been successfully recruited, and the duration of participant engagement. Qualitative data again came from field notes and posttest comments, which were coded a second time, using structured coding to answer the research question, “What factors affected implementation ease or difficulty?” While the previous round of coding focused specifically on participants’ reactions, this round included analysis of both the coaches’ and the participants’ perspectives.
Statistical Analysis
Calculation of the means was completed in Microsoft Excel (v 16.49; Microsoft Corporation, Seattle, WA). Content analysis was completed in Microsoft Word.
This study was deemed exempt and not regulated by the Institutional Review Board of the authors’ university (HUM: 00186053).
Results
Acceptability scores generated from the posttest (n = 10) appear in Table 1. Scores reflecting satisfaction with the MI intervention and its flexibility of scheduling were particularly high. Retention was also high: at end of May, 86% of participants (n = 16) who had begun the initiative had completed two interviews or more, and 63% (n = 16) had completed the posttest.
Participant Satisfaction With Program Overall (n = 10)
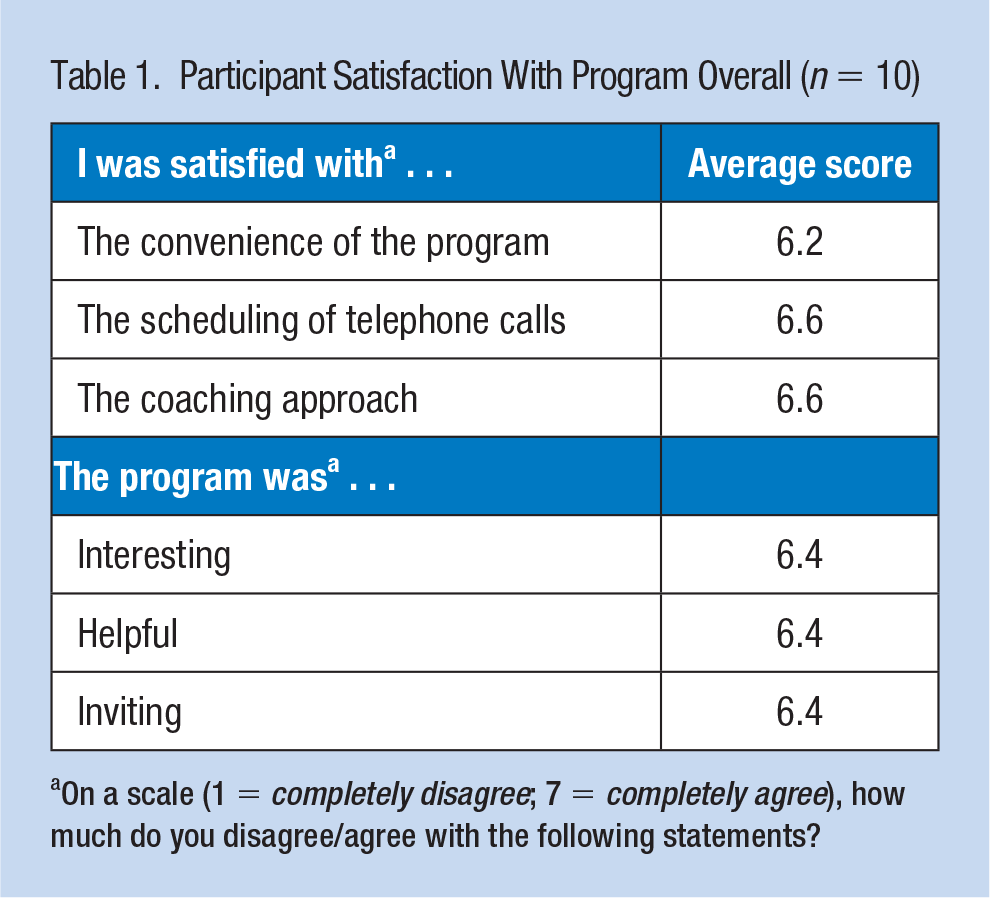
On a scale (1 = completely disagree; 7 = completely agree), how much do you disagree/agree with the following statements?
Field notes from 35 interviews (the number of interviews per participant varied from one to three), and five free-text comments made in the posttest, were coded using structural coding. Overall, notes and comments reflected positive participant experiences. A participant wrote that the intervention, “Was pleasant and helped me strategize . . .” A coach noted that one participant: “Found the past conversation very helpful to kick things into gear.” Most participants were rated by their coaches as “engaged,” although one was noted to be “pleasant, somewhat disinterested.” Three participants offered to recruit for the initiative due to their own positive experiences. One coach noted a participant say, “would recommend our study at the Farm Bureau meeting in April.”
Implementation scores appear in Table 2. These scores, though they ask about satisfaction, were included in the implementation analysis because they reflected the logistics of program delivery, including whether participants would have preferred to speak with a coach in person. In 4 months, 16 participants had been recruited. Thirty-five MI sessions averaged 18.5 minutes, ranging between 52 and 6 minutes.
Participant Satisfaction With Specific Program Factors (n = 10)
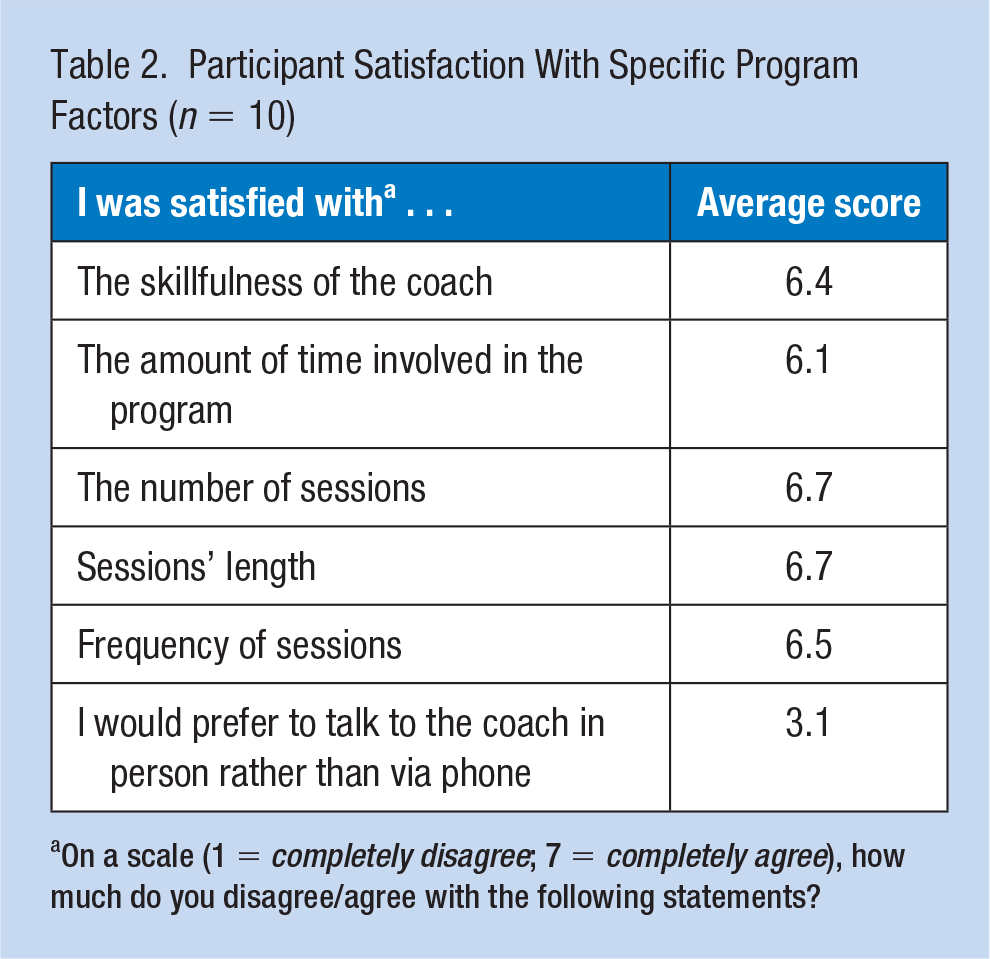
On a scale (1 = completely disagree; 7 = completely agree), how much do you disagree/agree with the following statements?
Implementation findings highlighted the importance of the intervention’s flexibility, which allowed for ad hoc scheduling tailored to each individual. Three notes indicated this feature was important to busy participants. One coach wrote: “He would like a chance to try some hearing protection, so he wants to have a third interview, I will email him in a couple weeks to set a time.” Another coach similarly noted a different participant asking for an additional week between sessions, “as he has been very busy.”
Another implementation issue that recurred in the notes was the provision of services beyond MI by the study team. One coach consulted with an audiologist about a participant’s unique needs. On five occasions, coaches noted they had sent a participant information on topics related to hearing health, such as tinnitus, or a smartphone-based application that measured noise levels. On seven occasions, coaches wrote participants about HPDs that the coach had identified as meeting the participants’ individual needs, usually via email between sessions. One representative coach comment: “Discussed some options from the company Decibullz and emailed a link as a resource. The products are specifically made for hunting and concerts and are less than $100.” Once, a coach noted he had sent information both on hearing health and products. These informational services, while not central to the technique of MI, were mentioned in four of the five participant free-text comments as well, with one participant’s typical comment: “Shout out to [Coach] for the advice and sending me links to the hearing protection I hadn’t heard of!”
Last, the pilot’s timing was also mentioned. Two participants noted that the upcoming growing season was increasing their workload; one specified she was busy “getting corn planted” as of late May. One participant reported “fatigue from Zoom calls.” Although this intervention was designed to be telephone-based prior to the onset of pandemic-related restrictions, this comment was worth highlighting as an example of the adaptability of the intervention to conditions related to the global pandemic that was ongoing during this pilot.
Discussion
Overall, these data reflect an intervention that was highly acceptable to participants. All quantitative acceptability metrics averaged within one point of the highest possible score. Qualitative data affirmed this acceptability as a strength, as participants were warmly positive in their comments, and were consistently seen as engaged by their coaches. Furthermore, we believe three participants’ voluntary offer to recruit for the study was a sign of unusual enthusiasm for this approach.
Data on program implementation were more mixed. The intervention’s flexibility and timing, from February to the end of May, made implementation easier from the participants’ perspective. Participants generally viewed the time associated with participating in the intervention positively, and they found their coaches to be sufficiently skilled. Furthermore, they rejected the idea that they would have preferred an in-person coaching session. The average length of time participants stayed on the phone with coaches was satisfactory to participants and, according to coaches’ field notes, allowed ample time to discuss achievement of the goals of the MI session.
Some of the participants’ enthusiasm may have been due to the information and personalized product recommendations that were shared with them outside of the MI sessions. Other services provided by the coaches, such as consulting the audiologist, and seeking out information on hearing-loss-related topics, might also be difficult to offer at scale.
While this additional information was provided by the study team out of their passion for hearing protection, it did increase the resources needed for continued implementation, and might affect the feasibility of this intervention in less-flexible settings.
Another major limitation was that only 16 people were recruited over the 4-month pilot. The initiative was designed pre-COVID-19, with the phone-based approach selected because it was seen as well suited to reaching a rural population. Indeed, the study team believed the phone-based approach facilitated implementing the pilot during the pandemic in every way but one: recruitment. It was a major disadvantage for recruitment to be restricted to telephone and internet-based conferencing rather than face-to-face, particularly when some participants were already reporting “Zoom fatigue.” The study’s principal investigator, who has years of experience recruiting agricultural producers for studies, reported much more difficulty recruiting for this project compared to previous studies. There is a need to repeat testing of recruitment when in-person methods are permitted.
Overall, we found these results to be encouraging, and we believe this feasibility study established that this intervention was highly acceptable to its intended users. We further believe this telephone-based MI approach has the potential to increase use of noise control strategies and reduce adverse effects of noise exposure such as hearing loss and cardiovascular disease among agricultural producers. The importance of involving agricultural producers, rather than simply providing them with information, in producing behavior change, had been identified by both researchers and agricultural producers alike (Kline et al., 2008). We felt that the high acceptability of the pilot-indicated producers had been successfully involved, while the implementation data indicated that we were able to successfully execute a program as planned. We also believed that implementation was likely to improve as the threat of COVID-19 recedes, although we expect participants will continue to take advantage of the intervention’s flexibility. Furthermore, we are excited at the possibility of reaching rural agricultural workers who typically do not receive occupational health services in their work setting. Last, this feasibility study adds to the growing body of evidence supporting the utility of phone-based MI interventions (Patel et al., 2019) and suggested that this utility may extend into occupational health.
Implications for Occupational Health Nursing Practice
MI is a highly acceptable intervention to agricultural producers seeking to limit their noise exposure by improving use of HPDs. It may also be acceptable to workers who would benefit from other forms of behavior change and should be considered in conjunction with educational interventions by occupational health nurses, particularly if rural workers are being targeted. However, frontline occupational health practitioners should anticipate the need to be flexible when administering the intervention, and the likelihood of recruiting challenges when workers cannot be approached face-to-face.
Applications to Professional Practice
This study suggested that occupational health practitioners consider motivational interviewing as a strategy to encourage behavior change. Although this study addressed noise reduction among agriculture workers, the model described herein may apply to any occupational sector or setting where noise poses an occupational health risk.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this study was provided by NIOSH T42 OH 008455 Occupational Health Workforce Training (PI: Batterman) and by a Postdoctoral Fellowship Training Grant (grant no. T32 NR016914. PI: Titler) Complexity: Innovations in Promoting Health and Safety. Funding was also provided by Sigma Theta Tau, Rho Chapter. Funders had no input into study design.
Ethical Approval
This study was approved and deemed exempt from review by the University of Michigan’s IRB on September 1, 2020, HUM00186053.