
Abstract
Background:
Ophthalmology practice entails many hours of physical inactivity, a potential long-term health hazard. This study aims to perform a pedometer-based evaluation of the physical activity (PA) levels of ophthalmologists at work.
Methods:
This is a prospective observational study. Ophthalmologists from a single tertiary medical center were monitored with electronic pedometers during six morning sessions in the ophthalmology clinics. Working hours and the number of patients seen per clinic session were retrieved. The age and body mass index (BMI) of participants were documented. Step number per working hour (SPH) was calculated for all participants. Comparisons between males and females, practicing ophthalmologists (attendings) and ophthalmology residents (residents), and sub-specialties were performed. Correlations between SPH and age, BMI, and patients seen per clinic session were computed.
Findings:
Pedometer readings for a total of 673 working hours were analyzed for 24 ophthalmologists, 17% female, 17 attendings, mean age 44.2 years (standard deviation (SD = 9.8). The average number of SPH for all participants was 359.7 (SD = 166.7). The mean PA level of residents was significantly higher than that of attendings (410.17 SPH vs. 338.95 SPH, respectively, p = .019). Oculoplastic surgeons demonstrated significantly higher step counts per hour than cornea specialists (439.90 SPH vs. 245.55 SPH, respectively, p = .002). A negative correlation was observed between SPH and the number of patients seen per clinic session (ρ = −0.274, p = .001).
Conclusions/Applications to Practice:
Low number of SPH for ophthalmologists in this study indicates ophthalmology to be a highly sedentary medical occupation. PA levels of ophthalmologists in the workplace may indicate a personal health care challenge.
Background
Low levels of physical activity (PA) are an important risk factor for diabetes (Bowden Davies et al., 2018), obesity (Rosenthal et al., 2017), and cardiovascular disease (Noda et al., 2005). To confront the ongoing sitting epidemic (Bailey et al., 2019), a recommended goal of 10,000 daily steps has been promulgated as a preventive health strategy (Choi et al., 2007). This effort has proven to be markedly effective in several studies and clinical scenarios (Castres et al., 2017; Schneider et al., 2006).
Electronic pedometers have been developed and validated as an inexpensive tool for assessing energy expenditure (Tudor-Locke et al., 2004). Pedometers have been successfully utilized to monitor daily PA both in clinical practice and clinical trials, including a number from workplace environments (Freak-Poli et al., 2011; Harris, Kerry, Limb, et al., 2018; Harris, Kerry, Victor, et al., 2018).
Physicians report many barriers to achieving desired levels of PA, including some which are workplace-related (Williams et al., 2015). Ophthalmology practice in hospital outpatient clinics, operating rooms, and community clinics entails many daily hours of physical inactivity. Ophthalmology practice is unique in that the physicians perform most examinations and surgical procedures while seated. Musculoskeletal disorders in ophthalmologists have been reported as a result of prolonged and improper sitting (Dhimitri et al., 2005).
Only a small number of studies have evaluated the PA levels of physicians during work hours, and even fewer pedometer-based studies have been conducted on practicing physicians (Abd et al., 2012; Atkinson et al., 2005; Beringer et al., 2020; Conzett-Baumann et al., 2009; Cuthill et al., 2008; Peters et al., 2020). To the best of our knowledge, no study has investigated the physical activity of ophthalmologists in the workplace. In this study, we sought to perform the first quantitative evaluation of the PA levels of ophthalmologists at work by using an electronic pedometer.
Methods
Data Collection
Resident and attending ophthalmologists from a single academic tertiary medical center were recruited to the study. Physicians who were pregnant or reported different injuries or movement limitations were excluded. Participants’ age, height, weight, and body mass index (BMI) were documented. Each participant was asked to wear a consumer-grade fitness wristband during six non-consecutive morning sessions in the ophthalmology outpatient clinic. Ophthalmologists received pedometers upon entrance to the clinic and were instructed not to alter PA habits. Pedometers were collected at the end of each clinic day. Working hours and the number of patients seen per session were retrieved from the electronic record management software.
The pedometer utilized in this study (Garmin Vivosmart 4, Garmin, Olathe, KS) is a wrist-worn device and part of a series of products that accurately record steps at different walking speeds (Wahl et al., 2017). In a previous paper that evaluated wearable activity monitors and their selection for research, Garmin Vivosmart exhibited high performance based on user experience, functionality, and infrastructure criteria and was consequently chosen for this study (Connelly et al., 2021). Two authors first tested the pedometer for one working day to ensure it did not interfere with routine procedures and examinations. Five pedometers were utilized. Automatic notifications and widgets were disabled. Pedometer data were extracted using the manufacturer’s designated software and online interface (Garmin Express 7.7.1.0, Garmin, Olathe, KS). Data reflecting relevant working hours were extracted, and participants were not informed of study results until study completion.
Statistical Analysis
Statistical analyses were performed using the MATLAB R2020b software package (MathWorks, Natick, MA). Descriptive statistics, including means and standard deviations (SD), were utilized to summarize the collected data. The number of SPH of work was calculated for each clinic session for every physician. Based on this variable, comparisons were performed between attendings and residents, male and female subjects, and sub-specialties that included at least two participants. Correlations between SPH, age, BMI, and the number of patients seen per clinic session were computed.
All data sets were tested for normal distribution utilizing the Kolmogorov-Smirnov test. For comparisons between means of two groups, an unpaired two-tailed student’s t-test was performed. One-way analysis of variance (ANOVA) was utilized to compare means of three groups or more, along with Tukey’s range test, which enabled paired comparisons within the ANOVA. Correlations were assessed with a Pearson correlation coefficient (ρ). A p-value < .05 was considered significant.
Ethics and Informed Consent
This study followed the tenets of the Declaration of Helsinki. The Institutional Review Board (IRB) approved the study and written informed consent was obtained from all participants. Physicians were offered to receive their personal statistics following data collection. No funding was received for this study.
Results
Demographic and Overall Pedometer Data
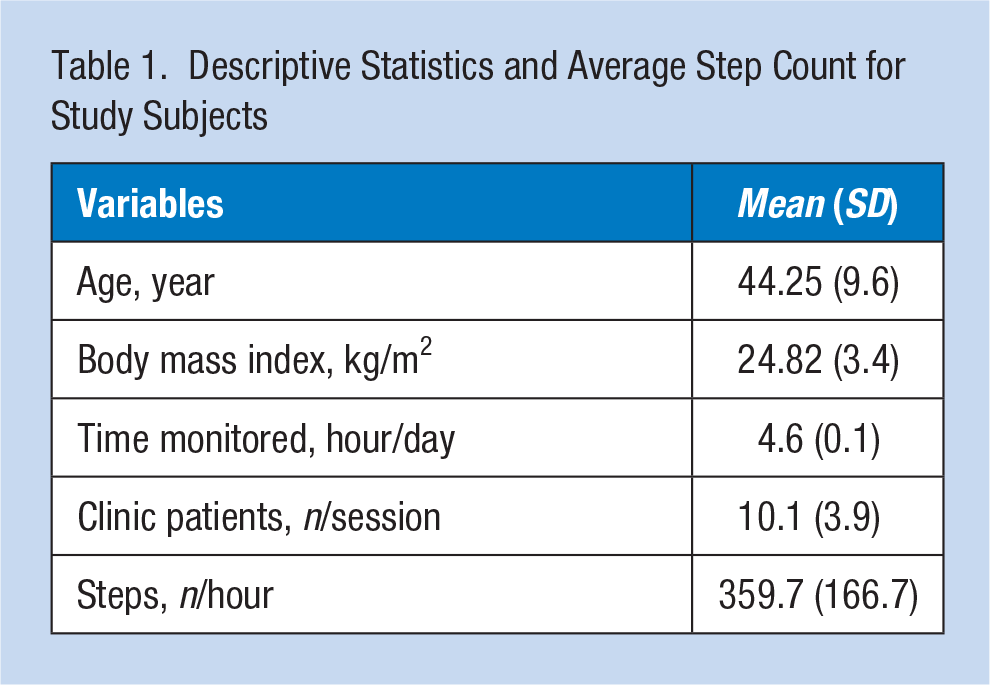
Subject demographic data, BMI, number of patients seen per clinic session, and SPH, are summarized in Table 1. A total of 673 hours of pedometer data was collected from 24 practicing ophthalmologists (17 attendings, seven residents). The sub-specialties of attendings were as follows: retina (six), cornea (three), oculoplastic surgery (three), cataract (two), glaucoma (one), pediatrics (one), and general practice (one). During six non-consecutive morning clinic sessions over 8 weeks, participants averaged 359.7 (SD = 166.7) steps per working hour. Differences in PA levels between male and female ophthalmologists were not observed, n = 20, 360.79 SPH (SD = 170.3) versus n = 4, 354.43 SPH (SD = 150.7), respectively, p = .865.
Descriptive Statistics and Average Step Count for Study Subjects
Correlations Between Step Counts and Personal Variables
A negative and statistically significant correlation was found between SPH and the number of patients seen per session (ρ = −0.274, p = .001; Figure 1a). A similar negative correlation was observed when attendings only were analyzed (Figure 1b, ρ = −0.242, p = .015) but was insignificant for residents alone (Figure 1c, ρ = −0.168, p = .287). No correlation was found between SPH and age (ρ = −0.251, p = .236) or BMI (ρ = 0.164, p = .443).
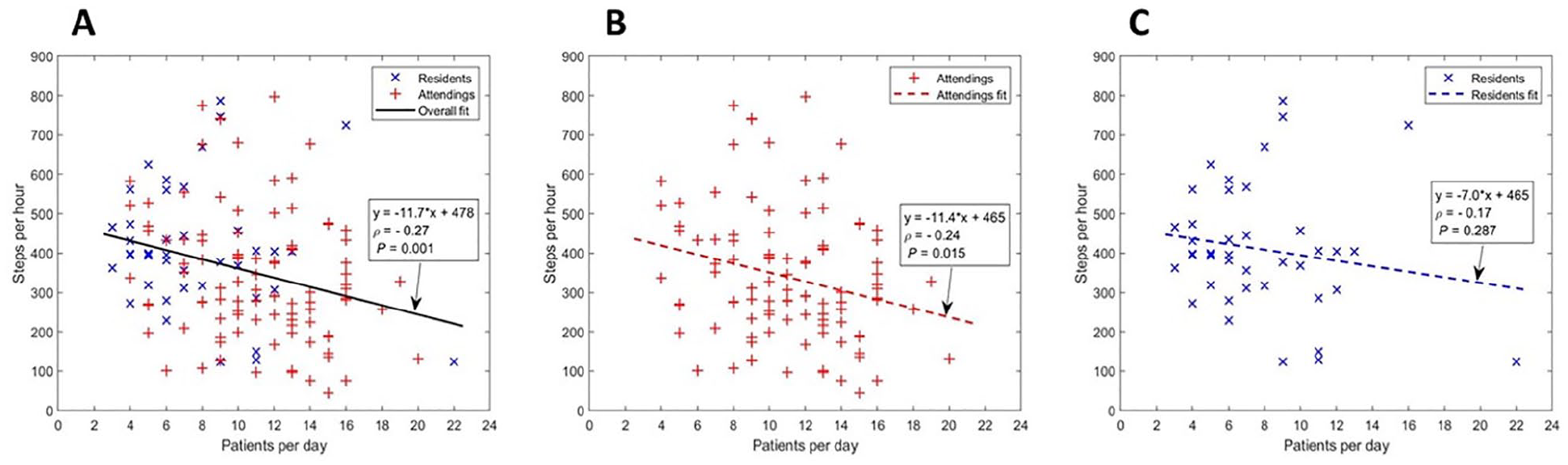
Correlations between step counts of study subjects and patient volume. Scatterplots of steps taken per working hour in relation to patients seen per clinic session for all study subjects (a), attending physicians (b), and residents (c).
Differences Between Attendings, Residents, and Different Sub-Specialties
Residents averaged a higher number of SPH than attendings (Figure 2a, 410.17 SPH vs. 338.95 SPH, respectively, p = .019). Attendings examined more patients per clinic session than residents (10.13 vs. 7.79, respectively, p < .001).
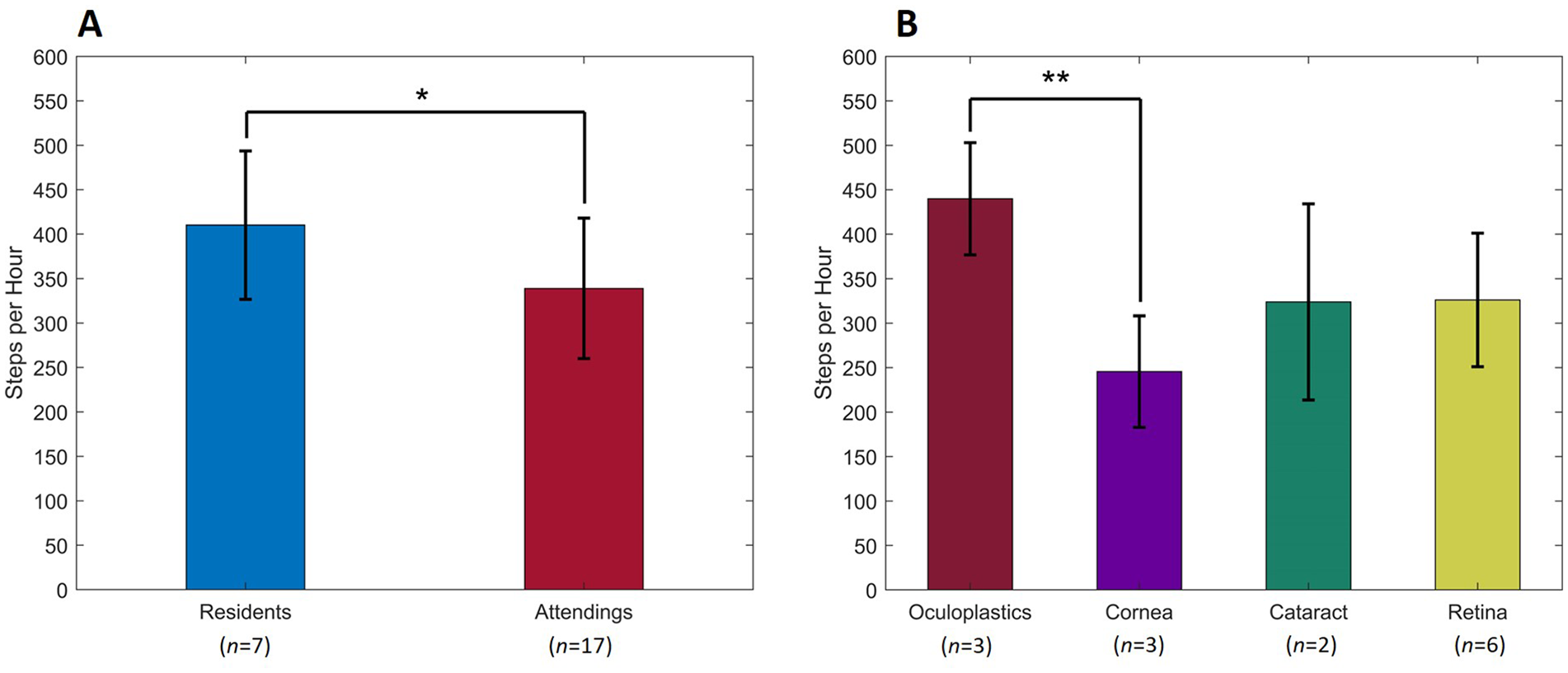
Step count per hour by group: attending physicians, resident physicians, and stratified by sub-specialty. A comparison between resident physicians and attending physicians (a), and stratified by sub-specialty (b), of steps per working hour. Comparisons were performed utilizing an unpaired two-tailed student’s t-test and one-way analysis of variance (ANOVA) with Tukey’s range test.
In a comparison between sub-specialties, a significant difference was observed only between oculoplastic surgeons and cornea specialists (Figure 2b, 439.90 SPH vs. 245.55 SPH, respectively, p = .002). These two groups did not differ in the average number of patients seen per session (cornea, 10.33 vs. oculoplastics, 9.16, p = .231).
Discussion
Health authorities recommend at least 150 to 300 minutes of moderate to vigorous aerobic activity each week for adults (Health.gov, 2018). It has been postulated that this recommendation is fairly equivalent to the contemporary goal of 10,000 daily steps (Tudor-Locke & Bassett, 2004). Although physicians are more likely to achieve the above fitness goals than the general population (Stanford et al., 2012), workplace-associated limitations present a significant challenge toward reaching recommended levels of daily PA, even in relatively “active” specialties (Beringer et al., 2020; Williams et al., 2015). Based on reviews done by the authors, this study is the first to document pedometer-measured PA levels among ophthalmologists in the workplace.
Walking speed, stride length, and exact energy expenditure are highly individual (Hagoort et al., 2022; Kavanagh, 2009). As such, this study focused on the average number of SPH as a comparable variable that represented PA levels at work. In this study, participants averaged only 360 SPH during morning clinic sessions. A review of the literature suggested that this step number was the lowest among all medical disciplines that have been evaluated similarly; cardiologists, cardiothoracic surgeons, anesthesiologists, emergency physicians, internists, and others, averaged between 430 and 744 SPH in previous pedometer-based studies (Abd et al., 2012; Atkinson et al., 2005; Beringer et al., 2020; Conzett-Baumann et al., 2009; Cuthill et al., 2008; Peters et al., 2020).
Assessments of other sedentary occupations may assist in putting our findings into a broader context. In a study on 72 full-time office workers, participants averaged 435 SPH at work (Clemes et al., 2014). In another paper that analyzed PA at the workplace by occupational categories, 30 professionals (managers, administrators), and 30 white-collar workers (clerks, service workers) averaged 364 and 469 SPH, respectively (Steele & Mummery, 2003). These data imply that ophthalmology practice in outpatient clinics is a sedentary occupation, even compared with strictly desk-based professions.
Several aspects of ophthalmology practice may account for this noticeable low level of PA. First, ophthalmology practice is mainly limited to clinic offices and operating rooms, unlike other disciplines that require walking through large areas of hospital wards. The ophthalmology clinic setting is arranged to optimize the practitioner’s time so that, in most cases, the mobile patient approaches the physician, and not the opposite. Second, as the slit-lamp is a primary tool for the ophthalmologist, most physician-patient interactions are performed while the doctor is seated. Other examinations, such as indirect ophthalmoscopy, the neuro-ophthalmological exam, and strabismus assessment, require only minimal amounts of movement. This study did not monitor the subjects in operating rooms due to the surgical scrubbing and gowning protocols. However, we assume that our results still indicate the low PA levels of ophthalmologists at work as most surgeries in ophthalmology are performed in the seated position.
A negative correlation between SPH and the number of examined patients per clinic session was observed. This correlation was statistically significant when the entire cohort or attendings alone were analyzed, conceivably due to differences in sample size between attendings (17) and residents (seven). A heavy workload prevents the physician from taking even short breaks, which could increase PA levels, even unintendedly. This finding is a potential contributor to the established damage to physician wellness caused by excessive workload (Wallace et al., 2009) and to the burnout of ophthalmologists in particular (Cheung et al., 2020). In an era of health care systems that maximize profitability, the long-term well-being of health care providers needs to be prioritized.
Although a statistically significant correlation between step counts and BMI was not detected, the mean BMI of participants (24.82 kg/m2) approached the upper limit of the normal range (18.5-24.9 kg/m2). In this cohort, low PA levels at work may partially account for borderline BMI values. This possibility seems reasonable considering the findings of a previous trial, which reported an inverse correlation between the daily walking distance of internal medicine residents at work and their BMI (mean 22 ± 2 kg/m2; Conzett-Baumann et al., 2009). However, a pedometer-based study on internists and general surgeons (548 SPH on average) proposed that high BMI is a predictor of lower step counts rather than the opposite (Goosen et al., 2008). Therefore, we assume that the possible relationship between high BMI and low PA levels of ophthalmologists at work is probably bi-directional.
In this study, pedometer data suggested that ophthalmology residents were more active at work than attendings by nearly 25%. Previous pedometer-based studies demonstrated similar differences between residents and attendings (Atkinson et al., 2005; Peters et al., 2020). One reason for the lower PA levels of attendings appears to be the larger number of patients seen per clinic session. Second, residents are required to consult with attendings frequently. These consults may lead to increased physical activity as they necessitate walking across the clinic several times a day. Third, in the hospital setting, residents are required to perform various tasks throughout the day that cause them to be more mobile, such as consultations in the medical wards.
Nevertheless, even during regular working days, residents averaged only slightly above 400 SPH, indicating low levels of PA at work. In a study regarding burnout among ophthalmology residents, the authors proposed that higher levels of physical activity throughout the entire day may reduce resident burnout (Feng et al., 2020). This proposal highlights yet another reason to find ways to increase physical activity in the workplace for ophthalmologists.
Finally, this study measured higher levels of PA among oculoplastic specialists when compared to cornea specialists. A possible explanation for this difference may be related to the dependence of cornea specialists on the slit-lamp examination. In addition, oculoplastic surgeons may perform minor procedures in separate clinic rooms, thus increasing their PA levels. In many tertiary medical centers, oculoplastic specialists are frequently called to assess patients in trauma and intensive care units.
Despite our concern regarding the physically inactive nature of ophthalmology practice, recent occupational medicine publications have reported associations between high levels of occupational PA and adverse health outcomes. In a meta-analysis of 17 studies, male workers with high levels of occupational PA had an 18% higher risk of early mortality compared with their relatively sedentary counterparts (Coenen et al., 2018). A cross-sectional survey study with 16,974 respondents detected increased odds for cardiovascular disease in those reporting high levels of PA at work (Quinn et al., 2021). Several explanations have been proposed in those papers for the “paradox of occupational PA,” such as low socioeconomic class of workers, which often correlates with both highly active jobs and higher morbidity rates. Another claim is that the presumed damage caused by increased levels of PA at work is relevant mainly to highly physical occupations, in which sufficient recovery time for reducing cardiovascular load is prevented. However, in ophthalmology, routine practice does not involve such intense tasks, and walking is probably the main form of adding to the total daily PA. Therefore, we suggest the results of this study be considered a potential for a long-term occupational health hazard.
This study has several limitations. First, data were obtained from a single tertiary medical center. This prevented comparisons between different practice settings and locations, such as private and community clinics. Second, the study sample size was limited to 24 physicians. While this number is similar to previous pedometer-based studies, more extensive studies would enable better generalizability of the findings. Third, pedometers do not allow a thorough analysis of PA intensity and energy expenditure. Studies utilizing accelerometers, which include features that allow for the differentiation between sitting and standing, may provide a more detailed picture of the PA levels. The utilization of such devices should be considered in future evaluations of the PA levels of ophthalmologists. Fourth, the study location was limited to outpatient clinics within a medical center.
Nevertheless, we postulate that the low levels of PA demonstrated in this study extend to other activities of ophthalmologists during their workday. Finally, this study enrolled more male physicians than female physicians. This imbalance may have occurred due to female physicians’ pregnancy and maternity leave in this center during the study period.
Implications for Occupational Health Practice
This is the first pedometer-based study conducted on practicing ophthalmologists during working hours. Our results indicated ophthalmology to be a highly sedentary medical discipline. It would seem that practicing ophthalmologists working full-time have a very challenging gap to fill to achieve recommended daily PA levels. This is even more of a concern for attendings who appear less mobile during their workday. However, residents should also be aware of this issue as the long-term implications on mental and physical health can be crucial. As workplace productivity becomes a primary focus in clinical practice, emphasis should be placed on increasing levels of PA to ensure the health and wellness of ophthalmologists. Based on our observations, we can offer several practical facilitators of physicians’ PA in ophthalmology clinics. First, proper planning of patient queues can create more opportunities for increasing physicians’ step counts. When patients undergo the necessary preparations (pupils dilation, imaging, refraction, etc.) in a timely manner and are invited to specific hours accordingly, the ophthalmologist may have more opportunities to take short breaks between patients. Second, placing the personnel-only facilities (restroom, coffee area) relatively away from the examination rooms potentiates increased PA at work. Finally, a working routine in which patients of the same session are parallelly seen in different rooms by residents or other trainees encourages the attending to rotate between them and perform more steps.
Applying Research to Occupational Health Practice
A quantitative assessment of the physical activity levels of ophthalmologists at work was never performed before. In this pedometer-based study, 24 attending and resident ophthalmologists averaged only 360 steps per hour (SPH) during outpatient clinic sessions, indicating very low physical activity levels in the workplace. Residents were slightly more active than attendings; however, their step counts were still low. As ophthalmology appears to be a highly sedentary medical occupation, physicians’ long-term wellness and health may be compromised. The findings of this study warrant further evaluations of workplace-related health and wellness risks for ophthalmologists. Furthermore, it may be advisable for healthcare administrators to seek ways to increase the physical activity levels of practitioners and medical staff at work, particularly in sedentary occupations.
Footnotes
Authors’ Note
This work has been presented as a poster in the American Academy of Ophthalmology Annual Meeting, November 2021.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Written approval to conduct the study was obtained from the Ethics Committee (Helsinki committee) of Shaare Zedek Medical Center on December 10, 2020, trial number: 0495-20-SZMC.