
Abstract
How do you assess the mental wellness of your work-from-home employees? This case study reports on how an occupational health nurse used work-from-home employee’s own phone and Fitbit™ smartwatch to obtain heart rate data to screen for high periods of stress. Telemedicine and telemetry allowed the occupational health nurses to screen an employee when the nurse could not assess the employee face-to-face. When the occupational health nurses identified an at-risk employee, the occupational health nurses referred the employee to the Employee Assistance Program (EAP) for counseling. Leveraging heart rate data on a smartwatch is a free intervention that is scalable and has a demonstrated outcome measure with a positive return on investment.
Background
Twenty-five percent of workers report undiagnosed stress that affects their work, and 12% of workers are at risk of suicide (Hoying et al., 2020; Melnyk, 2020). Occupational health nurses focusing on health promotion typically include a psychosocial or stress screening in their practice. The transition to work from a traditional work setting to the home environment may increase stress for some employees. The remote nature of the worker makes an assessment of stress levels difficult for the occupational health nurse. This case study presents a framework for screening work-from-home employees for stress.
Prior to the COVID pandemic, Mr. F was a senior vice president with 15 years of top 10% performance evaluations who recently transitioned to a work-from-home position. He regularly traveled internationally pre-COVID and attended large regional and global meetings. Recently, co-workers complained to the CEO that Mr. F’s behavior was becoming louder and more forceful. However, when his boss or HR had conducted video calls, Mr. F was pleasant and collegial. Human resources referred the employee to the occupational health nurse for a wellness check.
Clinical Findings
At the time of a telemedicine assessment, the occupational health nurse determined that Mr. F was a 43-year-old male with a body mass index (BMI) of 35, a history of hypertension, and currently on no medications. No complaints of palpations, shortness of breath, anxiety, or feelings of losing control were reported. The employee indicated that he consumed 2 to 3 alcohol drinks per day. The employee denied any recreational or prescribed drug use. Due to the remote work arrangement, the nurse could not conduct any physical examination nor collect any vital sign data. However, the patient stated he routinely wore a Fitbit™ watch as he was trying to lose weight. The nurse asked the patient whether he could download and send the heart rate data from the Fitbit™ for the past 6 months.
The Fitbit™ captured heart rate data and showed marked variations on specific dates. The nurse compared the days with a high average heart rate with the employee’s outlook calendar appointments. Mr. F worked from home; however, he occasionally had to fly to meet his supervisor face-to-face. The nurse recognized that the average daily heart rate increased 4 beats per min (BPM; 68 vs. 72 BPM) whenever the employee traveled to meet his immediate supervisor (Figure 1). Longer trips demonstrated a larger increase in average daily heart rate. The dates of the highest average daily heart rate also reflected the dates emails were sent to HR describing the employee’s odd behavior. The nurse then contacted the employee for a follow-up call to learn his perspective on these data.
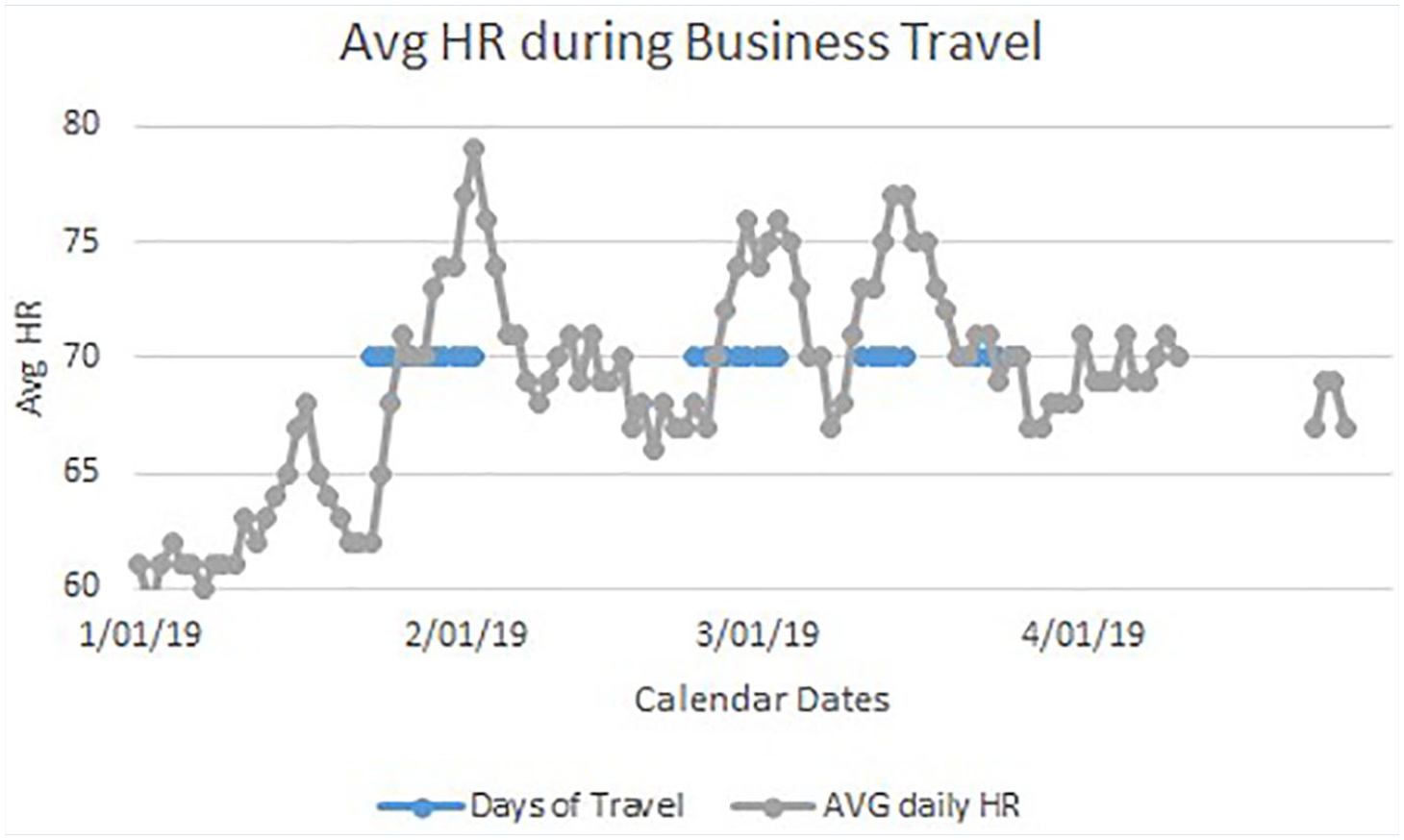
Average heart rate overlay when traveling compared with work from home.
Diagnostic Assessment
During this follow-up visit, and following the Canadian clinical practice guidelines for anxiety, the nurse asked targeted screening questions. These questions were, “During the past two weeks, how much have you been bothered by the following problems: 1) feeling nervous, anxious, frightened, worried, or on edge, 2) feeling panic, or being frightened, and 3) avoiding situations that make you nervous?” (Katzman et al., 2014). Positive responses lead to screening questions for generalized anxiety disorder (GAD), panic disorder (MACSCREEN), and social anxiety disorder (Mini-SPIN). No significant findings were found at the time of the interview on these screening tools.
Therapeutic Intervention
The lack of immediate danger to self or others allowed the nurse to recommend a referral to the employee assistance program (EAP) counselor (licensed clinical social worker [LCSW]). The LCSW focused on those moments that historically demonstrated an increased heart rate. The employee and LCSW practiced interventions (cognitive behavioral therapy meditation, breathing) to decrease anxiety over the allocated six sessions. The ability of the Fitbit™ to alert a high heart rate allowed the employee to see an elevated heart rate as a prompt for self-intervention.
The Fitbit™ showed a continual heart rate that should be a lower heart rate following a successful self-intervention. The ability to focus and receive immediate biofeedback via the heart rate provided a measurable outcome associated with the EAP referral.
Follow-Up and Outcomes
A 1-year follow-up visit was conducted between the nurse and the patient. During this period, the COVID pandemic occurred forcing many others to also work at home. Even with the added onus of COVID, the patient remained at a lower average daily heart rate. The employee identified days with stressful meetings or events. On those days, an increase in heart rate could be observed for a few minutes. However, there was little to no differences in the average daily heart rate, suggesting the employee was able to bring the heart rate back to baseline. The patient reported that when the watch indicated an increase in heart rate, he could perform deep breathing exercises (e.g., Breathe on the Apple watch) and watch his heart rate decrease in real time.
Discussion
This case study demonstrated that the occupational health nurses can continue to provide essential employee safety functions even during periods when the workplace or clinic is closed.
Occupational health nurses identified and managed risks of remote employees globally, at least since the onset of widespread adoption of globalization (Tompkins et al., 2005). Initially, the focus on the health of traveling (remote) workers was an itinerary specific to exogenous risk factors and reducing the risk of environmental exposure (Tompkins et al., 2005). However, there was little follow-up after an uneventful trip. The focus on more psychosocial aspects of remote work means that occupational health nurses could expand the assessment of remote workers to include the stress of work-from-home remote workers (Hoying et al., 2020; Martin & Giallo, 2016; Sanchez et al., 2017). Some estimates indicate up to a quarter of employees have undiagnosed stress or global discomfort (Barrech et al., 2018; Kuehnl et al., 2019; Rundle et al., 2018). The lack of face-to-face interaction, or clinical assessment for stress, presented a challenge for the occupational health nurse. Conversely, it was economically unfeasible to test all employees for stress related to the long-term reactions to remote work.
Technology such as movement and heart rate tracking watches (Fitbit™, Apple watch) may provide a cost-effective real-time screening tool. Studies show that interventions to encourage employees to move more during work have been successful (Guitar et al., 2018). Other studies have tracked mood and provided financial incentives to engage in remote monitoring (Losina et al., 2017; Mark et al., 2016; Padmaja et al., 2019). These studies, as well as others, have shown that smartwatch accuracy in tracking is sufficient for baseline screening (Benedetto et al., 2018; Feehan et al., 2018; Reingle Gonzalez et al., 2019). Heart rate is a suitable variable to capture on the smartwatch, and heart rate can be used as a proxy for times of increased stress (Nakayama et al., 2018; Padmaja et al., 2019).
The implementation of a smartwatch program to monitor heart rate as a proxy for worker stress associated with remote work offers additional advantages of cost and comprehensiveness. Between 20% and 30% of Americans already own a smartwatch, with a higher percentage of users in the higher annual income levels above US$70,000 (Vogles, 2020). For those who already own a watch, heart rate data may already be captured and stored, thus not requiring any upfront cost from the occupational health department. Furthermore, the always monitoring of the heart rate means the comprehensiveness of the heart rate monitoring can match or exceed any clinical one-time or even 24-hour Holter monitoring. Following a research design of an “n of 1,” the patient’s baseline (even given any variance in the ability of the watch to record the heart rate) heart rate served as a robust control for periods of increased heart rate (Yoon et al., 2018). The nurse only needed to record the historical heart rate data from the watch and compare the elevated average daily heart rate with the employee’s calendar to make a preliminary assessment, and determine if more intervention was needed.
An employee identified with increased heart rate and stress can then proceed to a more formal (or virtual) assessment and interaction with the occupational health nurse. Better patient selection means that the limited resources of the occupational health nurses will have a greater measurable impact. For example, the occupational health nurse link increased heart rate in specific circumstances and a positive screening test on web-based screening tools such as MACSCREEN or MiniSpin (Van Ameringen et al., 2010). These assessment tools suggest a referral to mental health will be cost-effective for the 3% to 12% of employees who are at risk of suicide or burnout (Hoying et al., 2020; Melnyk, 2020)
Conclusion
The occupational health nurse needs tools to manage the health challenges associated with employees who are working from home. The COVID pandemic has forced many employees to work from home. Sixteen percent of these workers may work from home permanently (although this percentage will vary among industries; Bartik et al., 2020). The occupational health nurse will need new support and tools to monitor these long-term work-from-home employees. Telemedicine, smart devices, and connected homes need to consider issues of privacy, too much data, and false positive screening. The occupational health nurse may also look at customer service work that screens for angry customers as a proxy for stressed work-from-home employees (Gupta et al., 2010). Mental health has always been challenging to screen for, and working remotely makes those assessments more difficult. Complaints about workers to human resources, or employees with a sudden change in performance, may warrant screening. Leveraging technology to provide a free longitudinal report on heart rate as a proxy for stress can identify employees needing future screening. Three questions asked by the occupational health nurse coupled with three to five online questions on web tools, may effectively identify the 3% to 12% of employees who need professional mental health assistance to prevent burnout, depression, homicide, and suicide in the workplace (Harvey, 2019; Tran et al., 2019).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Alexander M. Gleason’s research focuses on oversea foreign worker wellness in Southeast Asia and the Middle East. He is currently a head of Department for Nursing at Fatima College in Abu Dhabi.