
Abstract
Background:
Many workers shifted to working from home due to the COVID-19 pandemic. This review aims to investigate if this sudden change caused an increase in TElewoRk-RelAted stress (TERRA) which is defined as physical and mental stress caused by telework.
Methods:
A systematic review using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines was performed of three scientific databases (PubMed, ISI Web of Knowledge, and Scopus), which also included a quality assessment. Articles measuring stress, psychological or physical, in remote workers, published from December 2019 through August 2021 were included in the review. Results were extracted by reporting: authors, country, study design, type of workers, sample, questionnaires and measurements, and outcomes. Data were synthesized quantitatively for country, type of workers, and outcomes.
Results:
Out of the 518 articles found in the three databases, 19 articles were included in the systematic review (10,012 participants overall), and 78.9% of these highlighted an increase in TERRA levels in remote workers. Among 85.7% of the studies considering gender as a variable, TERRA levels were higher in female workers. Twelve (63.2%) of the studies investigated psychological well-being, two (10.5%) focused on the physical well-being of remote workers, three (15.8%) investigated both, and two studies had other outcomes (10.5%).
Conclusions:
Considering the redefinition of workplaces dictated by the COVID-19 pandemic, this review highlights the emerging issue of remote work and the use of technology in working from home, emphasizing a rapidly growing occupational health problem. Remote workers need to be provided with emotional and technical support to prevent TERRA in remote workers.
Background
During the first months of 2020, the rapid spread of the SARS-CoV-2 virus and the resulting COVID-19 pandemic caused a profound shift in the lives of people all over the world. To prevent further spread of the virus, many countries adopted quarantine and isolation measures, and many workplaces shifted from the usual workplace to remote working. Subsequently, many studies were carried out to assess the effect of working from home (WFH) on remote workers’ stress, anxiety, and general well-being—both mental and physical. For example, Bijulakshmi et al. (2021), conducted a study on a sample of 912 Indian teachers and IT professionals and reported that 63.9% of the participants were stressed (8.6% having severe stress), 62.5% were suffering from anxiety (6.9% from severe anxiety), and 31% of were suffering from depression (1.2% having severe depression). This study highlighted differences in stress, anxiety, and depression levels, depending on occupation, age, gender, and having at least one child. As far as the physical well-being aspect is concerned, an Italian study, conducted by Moretti et al. (2020), was performed on a sample of 51 participants, to test if muscular pains improved, worsened, or remained equal during WFH. Results showed that WFH worsened muscular pain in some of the participants suffering from back pain, neck pain, elbow pain, shoulder pain, and hip pain.
WFH became possible due to the improvement and diffusion of information and communication technologies (ICTs). However, the diffusion of ICTs on a large scale also caused new mental health problems to emerge among users who were unable to keep up with the rapidly changing technologies. Brod (2007) defined technostress as “a modern disease of adaptation caused by an inability to cope with the new computer technologies in a healthy manner.” Later, Ragu-Nathan et al. (2008) developed and validated a new scale to measure technostress. The Technostress Creators Scale consisted of five items: techno-overload, techno-invasion, techno-complexity, techno-insecurity, and techno-uncertainty, each one measured with a 5-point Likert-type scale (Ragu-Nathan et al., 2008). In 2014, technostress was defined further as “the stress that users experience as a result of application multitasking, constant connectivity, information overload, frequent system upgrades, and consequent uncertainty, continual relearning and consequent job-related insecurities, and technical problems associated with the organizational use of ICT” (Tarafdar et al., 2014).
Stress, anxiety, and mental well-being were not the only factors associated with technostress, recent studies have shown that technostress is responsible for other disturbances including mental fatigue, memory disturbances, poor concentration, irritability, feelings of exhaustion, insomnia, lack or reduction of productivity and job satisfaction, and work-family life balance disturbances (Molino et al., 2020).
Technostress as defined by Tarafdar et al. (2014) was not specifically used to define stress caused by ICTs in the workplace, although they aimed to assess technostress in workers. Therefore, we have decided to use the term “TElewoRk-RelAted stress” (TERRA) to define technostress, and include both physical and mental stress, caused by ICTs specifically in workers, while WFH. As the pandemic exacerbated technostress in workers while WFH, the authors used the new term to frame a new occupational health issue arising from the rapid change of the workstation from an office-provided one to a home station, with all the consequent mental (i.e., inability to disconnect from work even after working hours because it is not physically possible to leave the office) and physical (i.e., having to use a home setup for work, including a new workstation that could be less ergonomic) health problems it may cause.
This systematic review aims to investigate how TERRA levels affect workers’ everyday life, their well-being, and their work-family life balance during the COVID-19 pandemic.
Methods
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement (Page et al., 2021), a systematic review was performed using PubMed, ISI Web of Knowledge, and Scopus. In order to perform the bibliographic search, the following query was used: [(“remote work*” OR “smart work*” OR telecommu* OR telework* OR “home work*” OR smartwork* OR “smart-work*” OR “work from home” OR “flexible work*” OR “mobile work*”) AND (stress OR technostress OR “occupational stress” OR “work related stress” OR “work-related stress” OR burnout OR exhaustion OR overwork* OR (stress AND tech*)) AND (Covid19 OR “Covid-19” OR “Sars-CoV-2” OR Covid OR Coronavirus)]
Duplicate removal was consequently done through Mendeley, a final check was then performed manually to ensure no duplicates remained. Title and abstract screening was performed in triple blind through the website Rayyan (www.rayyan.ai), which allowed for articles to be screened blindly by three researchers, to reduce selection bias. The articles unanimously included or excluded were not discussed further; however, the articles for which the website showed conflict were openly discussed, and a unanimous decision about inclusion or exclusion was eventually reached. A quality assessment for the included studies was performed using the Newcastle-Ottawa Scale (Wells et al., n.d.).
Inclusion Criteria
The research was restricted to Italian or English articles, published from December 2019, when the COVID-19 Pandemic started, and up to August 2021. Inclusion criteria concerning title and abstracts were met if WFH during the COVID-19 pandemic was mentioned. To screen full-text articles, stricter inclusion criteria were used: The article had to mention physical (ergonomic) or mental stress while working, not caused by external factors (family, children, house chores, etc.), but specifically by an overuse or misuse of technology. These articles were therefore classified as concerning TERRA and included in the review.
Exclusion Criteria
Articles that did not mention WFH, work-related stress, the use of technology while working, or did not include the working population, were excluded. Exclusion criteria also encompassed the absence of full text or article type not consistent with the purpose of this research (conference acts, vignettes, etc.).
Data Extraction and Synthesis
Results were extracted by reporting, for each included study, in an excel sheet: authors, country, study design, type of workers, sample, questionnaires and measurements, and outcomes. Data were synthesized quantitatively for country, type of workers, and outcomes.
Results
The systematic search resulted in 518 relevant articles from the three databases (PubMed, ISI Web of Knowledge, and Scopus). After removing duplicates, the initial search resulted in 294 eligible articles. Three researchers screened the articles by title and abstract: 210 were excluded based on the addressed topics; five articles were not relevant to the COVID-19 pandemic; four articles were excluded according to the type of publication; one article was excluded because of the considered population (the study did not consider workers).
The remaining 74 articles were screened by full text. For two of the articles, the full-text was not freely accessible, therefore the articles were excluded. Out of the remaining 72 articles, 34 articles were included based on full text: two were literature reviews, 13 were validation studies for questionnaires or methodologies, and the other 19 were articles included in our systematic review (Figure 1). Any conflict about the inclusion or exclusion of the articles was resolved by internal discussion between the researchers. A quality assessment was performed on all the included studies using the Newcastle-Ottawa Scale; three of the included studies showed fair quality (5 points), while the other 16 studies showed good quality (6 or 7 points).
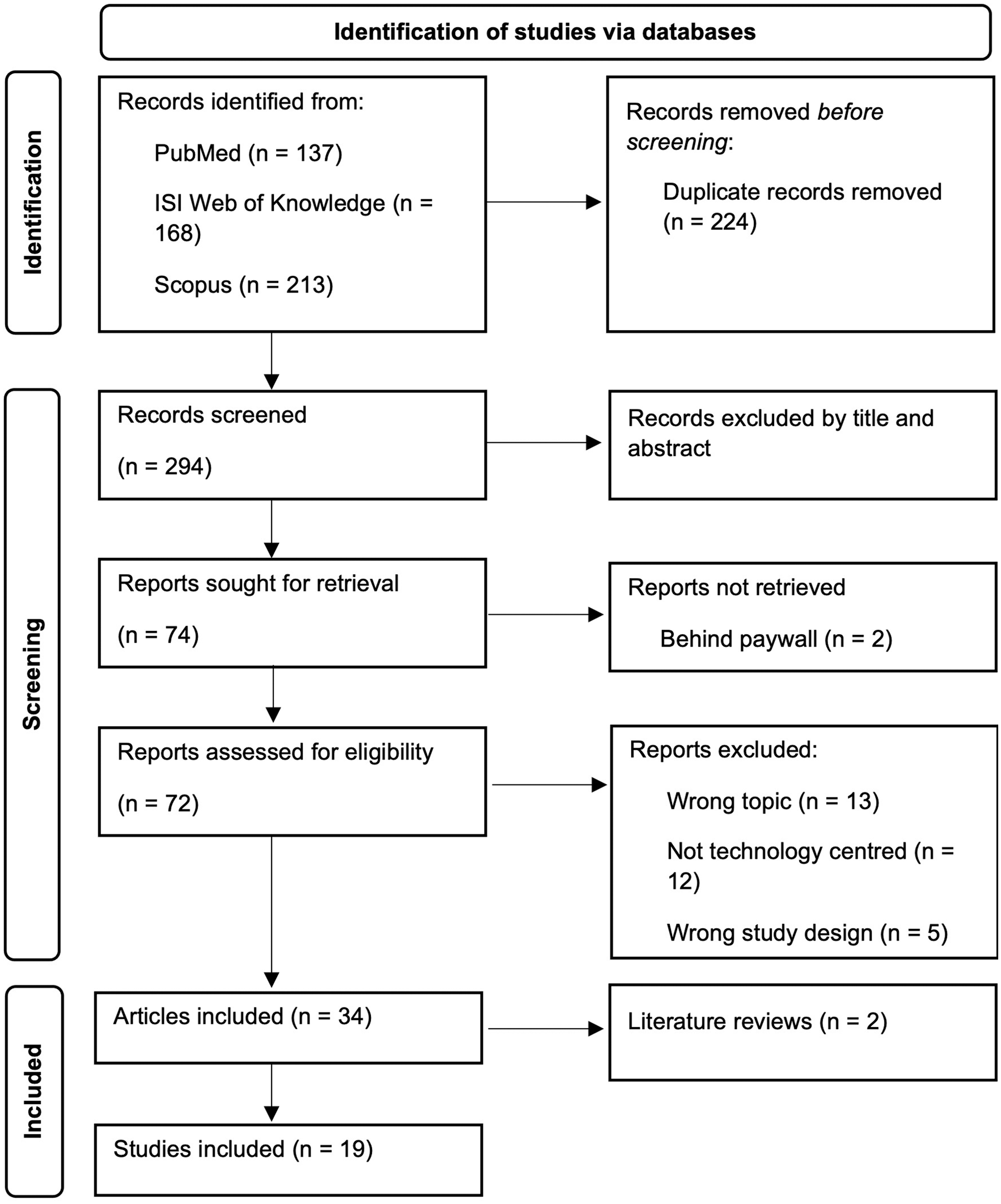
PRISMA flowchart of the inclusion process.
Study Characteristics
Out of the 19 studies included in the review (Table 1), 6 (31.6%) were conducted in Italy, 3 (15.8%) in India, two (10.5%) in Finland, one (5.3%) in the Philippines, one in Germany, one in Mexico, one in Egypt, one in Canada, one in the United States, and two (10.5%) studies were performed in more than one country. Concerning study design, 16 (84.2%) were cross-sectional studies, while three (15.8%) were longitudinal studies. All the studies included in the review were conducted by administering a survey to the participants. Only three (15.8%) studies had more than 1,000 participants, while most studies, 11 (57.9%), had under 500 participants, and five (26.3%) had between 500 and 1,000 participants.
Studies Included in the Systematic Review: Authors, Country, Study Design, Sample Size, and Questionnaires Used
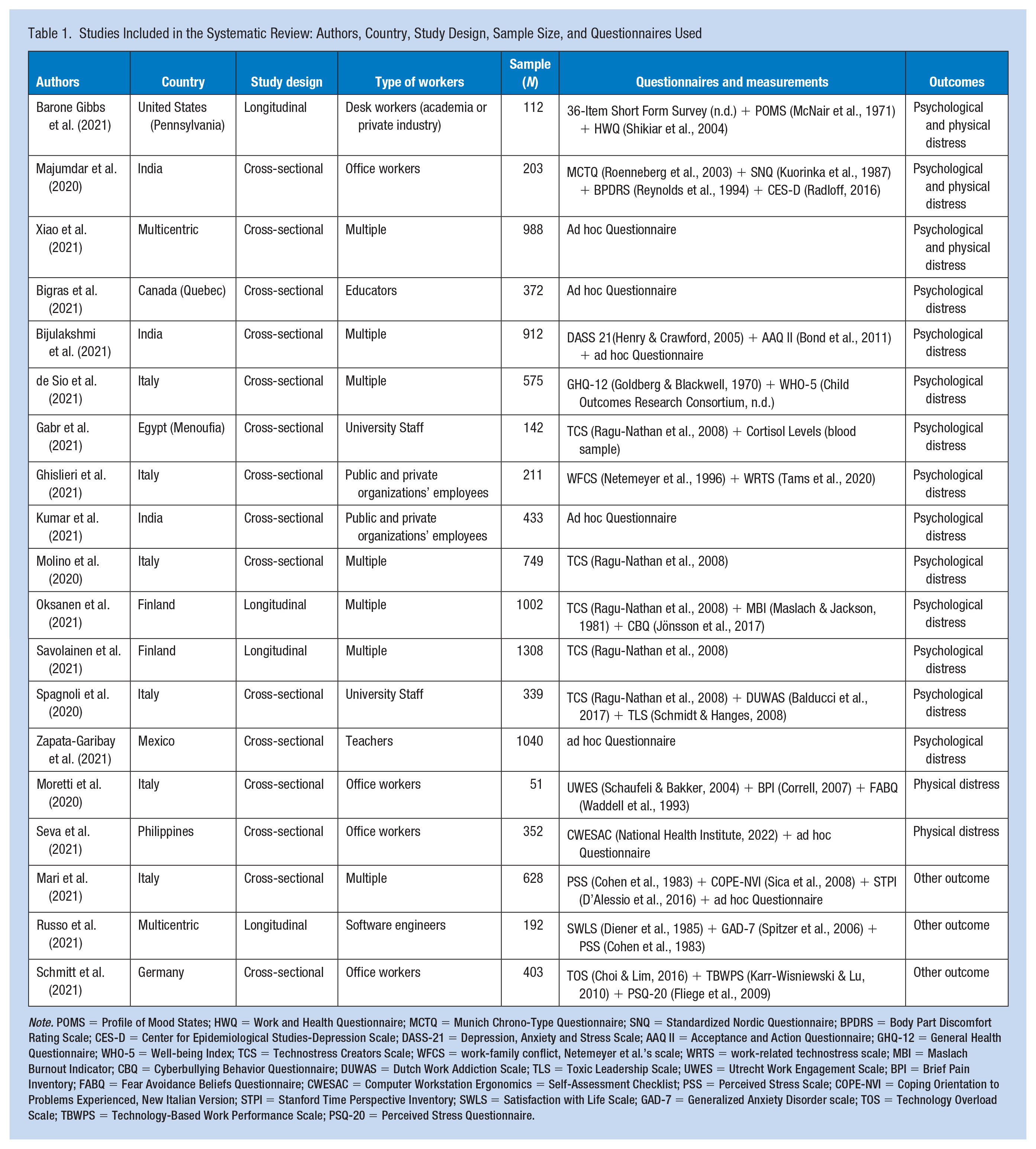
Note. POMS = Profile of Mood States; HWQ = Work and Health Questionnaire; MCTQ = Munich Chrono-Type Questionnaire; SNQ = Standardized Nordic Questionnaire; BPDRS = Body Part Discomfort Rating Scale; CES-D = Center for Epidemiological Studies-Depression Scale; DASS-21 = Depression, Anxiety and Stress Scale; AAQ II = Acceptance and Action Questionnaire; GHQ-12 = General Health Questionnaire; WHO-5 = Well-being Index; TCS = Technostress Creators Scale; WFCS = work-family conflict, Netemeyer et al.’s scale; WRTS = work-related technostress scale; MBI = Maslach Burnout Indicator; CBQ = Cyberbullying Behavior Questionnaire; DUWAS = Dutch Work Addiction Scale; TLS = Toxic Leadership Scale; UWES = Utrecht Work Engagement Scale; BPI = Brief Pain Inventory; FABQ = Fear Avoidance Beliefs Questionnaire; CWESAC = Computer Workstation Ergonomics = Self-Assessment Checklist; PSS = Perceived Stress Scale; COPE-NVI = Coping Orientation to Problems Experienced, New Italian Version; STPI = Stanford Time Perspective Inventory; SWLS = Satisfaction with Life Scale; GAD-7 = Generalized Anxiety Disorder scale; TOS = Technology Overload Scale; TBWPS = Technology-Based Work Performance Scale; PSQ-20 = Perceived Stress Questionnaire.
Concerning the occupation type, seven of the included studies (36.8%) included multiple types of workers and occupations (because the surveys in these studies were distributed online and included many occupational types), five studies (26.3%) focused on desk or office workers, four studies (21.0%) focused on teachers, educators or university staff, two studies (10.5%) included public and private organizations’ employees (not otherwise specified), and one study (5.2%%) included software engineers.
Psychological Distress
Fifteen of the 19 studies included in our review investigated psychological distress.
Barone Gibbs et al. (2021) found that stress levels were higher in workers always working remotely; Xiao et al. (2021) reported that 73.6% of respondents had new mental health issues, and Majumdar et al. (2020) highlighted that depressive symptomatology increased while WFH. Molino et al. (2020) also found technostress levels to be higher while WFH and Kumar et al. (2021) reported that 48% of female and 41% of male workers had been experiencing distress. Schmitt et al. (2021) reported an increase in overload related to the use of text-based tools. de Sio et al. (2021), Spagnoli et al. (2020) and Zapata-Garibay et al. (2021) reported technostress to be present while WFH.
Bijulakshmi et al. (2021) and Gabr et al. (2021) reported that older participants (over 60 years of age in Bijulakshmi’s study, not specified in Gabr’s) had the highest percentage of stress, anxiety, and depression and higher technostress levels, respectively.
Two studies in our review were conducted with data from the “Social Media at Work in Finland” survey: Oksanen et al. (2021) and Savolainen et al. (2021). Oksanen et al. (2021) highlighted that 17.09% of workers reported a substantial increase in technostress, 69.72% reported little or no change, and 13.19% reported a significant decrease in technostress; young age was a protective factor for technostress, while victimization from cyberbullying at work, use of social media for work communications, and neuroticism, were predictors of higher technostress. Savolainen et al. (2021) highlighted that technostress correlated with COVID-19 anxiety.
Only two of the studies we have identified did not report a higher stress level while WFH. Bigras et al. (2021) showed that educators’ WFH reported higher well-being than those who worked on-site, and stress levels were lower while WFH. Ghislieri et al. (2021) also reported that levels of perceived cognitive demands, work interference, and stress, caused by ICTs in public and private organizations’ employees were low, but stress was related to the use of ICTs to stay connected with others.
Physical Distress
Only 5 studies out of the 19 included in this review investigated physical distress while WFH.
Barone Gibbs et al. (2021) reported that changing to WFH caused an increased level of sedentariness during non-work days and a worsening in quality of life and overall work health; a decrease in physical functioning was reported in the “always remote” group. Xiao et al. (2021) also reported that 64.8% of respondents had new physical health issues.
Moretti et al.’s (2020) results showed that lower back pain was worse in 38.1% of participants, and neck pain was worse in 50% of participants since starting WFH. A significantly (p = .009) higher job satisfaction was reported by workers with no muscle-skeletal pain (MSK). Majumdar et al. (2020) reported that sleep duration worsened while WFH (ranging from 4 to 8 hours); this worsening in sleep duration might have been related to an observed increase in screen time usage in office workers. They also highlighted that office workers reported MSK pain in the neck, shoulders, wrists, upper back, and hips/thighs; these results were in accordance with Seva et al. (2021) findings (74.1% of participants reported lower back pain, 67.9% neck pain, and 67.3% of participants reported shoulders pain, and 22.6% reported ankle or feet discomfort).
Gender Differences
Seven studies included in this review investigated gender differences.
De Sio et al. (2021), Gabr et al. (2021) and Spagnoli et al. (2020) reported that female participants had significantly higher technostress levels, and Kumar et al. (2021) reported that distress levels were higher in female workers. Yet, to date, only five studies examined MSK pain during this time frame. Xiao et al. (2021) reported that being female increased the risk of new health problems while WFH; the authors highlight that this difference might be influenced by women’s tendency to be more responsible for household chores and child care. Bijulakshmi et al. (2021) reported that moderate stress was higher in male teachers, while depression was higher in female teachers; on the contrary, stress, anxiety, and depression, were higher in female IT workers.
Zapata-Garibay et al. (2021) reported that 86.2% of female teachers felt that working days were more strenuous because of the increase in work they had to do at home, highlighting that work-family life balance could be a confounding factor in female workers, adding to the stress of WFH not related to technology; 35.9% of female teachers had difficulties concentrating on teaching practice. Depression indicators related to feelings were more prominent in female teachers, while indicators associated with the lack of motivation and desire were more common in male teachers.
It is important to highlight that Gabr et al. (2021) and Spagnoli et al. (2020) did not investigate confounding factors related to family status, such as having children, which could influence the gender difference in technostress highlighted by these studies. Furthermore, de Sio et al. (2021), Kumar et al. (2021), and Bijulakshmi et al. (2021) reported that being a parent was related with higher technostress levels but did not investigate if this factor had a different role in male and female workers.
Other Outcomes
In Bigras et al.’s (2021) study, a small percentage of participants (6.42%) reported technical difficulties due to technology use while WFH. Xiao et al. (2021) highlighted that physical and mental well-being were significantly lower in workers who did not know how to adjust their workstations or did not have a good workstation setup. Russo et al. (2021) reported that stress and anxiety negatively affected well-being, and there was a positive correlation between productivity and well-being. Mari et al. (2021) reported that teachers had a worse attitude, emotional response, and coping mechanisms, toward smart working than practitioners, managers, and executive employees. Spagnoli et al. (2020) reported that the interaction between workaholism and authoritarian leadership was significantly related to technostress, and these factors’ interaction with WFH was also related to technostress.
Discussion
The SARS-CoV-2 pandemic caused a drastic change in the work lives of people all around the world, as many workers were forced to stay at home to reduce the risk of contagion. These workplaces thus shifted from the office to WFH; in this systematic review, we investigated the consequences of this sudden shift on workers’ health, both mental and physical, and on the effect this change had on workers’ technostress.
Psychological Distress
Fifteen of the 19 studies included in our review investigated psychological distress due to the shift to WFH; 12 of these studies (80%) highlighted a worsening in technostress while WFH or the development of new mental health issues (i.e., anxiety, depression, stress).
These results could be partially due to the sudden shift to WFH due to the COVID-19 pandemic, as many workers were forced to switch to WFH without having a proper workstation or the proper ICTs. Furthermore, COVID-19 anxiety and stress caused by the pandemic itself could have affected psychological well-being outcomes (Yang et al., 2020). However, technostress has been identified as a problem in previous studies, as highlighted in La Torre et al.’s literature review performed in 2019, before the pandemic started (La Torre et al., 2019).
As technology becomes more and more specialized in the workplace, these findings suggest that technostress could be evaluated by occupational health clinicians during medical surveillance, especially for workers at risk (i.e., workers using ICTs, particularly female workers).
Gender Differences
Out of seven studies investigating gender differences, six (85.7%) highlighted female gender as a risk factor for psychological distress, reporting higher technostress levels in female workers. These findings are consistent with the scientific literature. Higher technostress levels in women could be related to gender imbalance in technology use at work (Brussevich et al., 2018); as women in science, technology, engineering, and mathematics fields are outnumbered by men to this day, and only recently efforts were put in place to reduce this gap (Hunt et al., 2021). Morris et al. (2005) highlighted that the gender gap where technology usage and knowledge in the workplace are concerned, is more prominent in workers older than 40 years of age. This is also consistent with our findings. All the studies included in this review that considered age differences highlighted higher stress levels in older participants.
Physical Distress
All five studies investigating physical distress highlighted either the presence of MSK pain (Majumdar et al., 2020; Moretti et al., 2020; Seva et al., 2021), a worsening in the overall work health (Barone Gibbs et al., 2021), or new physical health issues (Xiao et al., 2021), in at least some of the participants. Ergonomics were being investigated to ensure that MSK pain in office workers is prevented and its causes were swiftly identified (Sama’ An Shahwan et al., 2022; Tahernejad et al., 2021). MSK pain is generally related to the workstation’s setup: ergonomic chairs, an adjustable workstation, and a fitting mouse or screen, are just a few of the commodities needed in order to ensure MSK pain prevention. An evaluation of home workstations should be performed to ensure appropriate safety conditions are being met (Sama’ An Shahwan et al., 2022).
Strengths and Limitations
One of the strengths of this review is that, by introducing the TERRA definition, it attempts to better frame the emerging issue of technostress. A systematic approach was used to search three databases following the PRISMA Guidelines, and the article screening was performed by three researchers using a blind methodology. However, only articles in English or Italian were included in the review, and articles not freely accessible were discarded. It is important to note that the use of many different questionnaires to measure stress or other psychological well-being indicators, as well as the use of ad hoc questionnaires, has made the harmonization of the result challenging. A quantitative summary of the findings was not possible to obtain, due to the high heterogeneity of assessment, so a meta-analysis was not performed. Furthermore, factors such as isolation, child care, house chores, may have influenced mental and physical stress during the COVID-19 pandemic but could not be evaluated as confounding factors due to the heterogeneity of included studies.
Implications for Occupational Health Practice
Overall, 15 (78.9%) out of the 19 included studies highlighted high TERRA levels while WFH; TERRA levels were higher in female and older workers.
These results showcase the need to prevent technostress and techno-overload while WFH, by implementing prevention strategies focused both on emotional as well as technical support (for workers with poor Wi-Fi signal, outdated software, low technology knowledge). Furthermore, appropriate equipment should be provided to reduce MSK pain in workers, such as adjustable and ergonomic workstations and other tools used while WFH. From an occupational health standpoint, technostress and its impact has on workers’ health should be addressed during medical surveillance, and prevention evidence-based strategies should be put in place.
Furthermore, during hazard assessment, exposure to ICTs should be taken into account when classifying an employee and their work-related risks; employees should be trained and informed about TERRA and the health consequences that technostress may have on workers; medical surveillance, as stated, should address this issue and a screening for technostress could be performed for at-risk workers. As the workplace is changing, the risk assessment and medical surveillance programs should take into account that technology, as an integrated and active tool for workers, has many repercussions on health that should be closely monitored.
In conclusion, this review should be a starting point for further research to implement prevention strategies and, as technology becomes an ever-growing presence in workers’ lives, to develop a standardized method to measure TERRA levels in workers, to assess its effect on remote workers’ well-being, and to develop a prevention plan to limit its impact.
Summary
78.9% of the studies included in this review highlighted high technostress levels in remote workers (higher in female and older workers).
There is a need to prevent technostress and techno-overload in remote workers, and the right equipment should be provided to ensure physical health in workers.
From an occupational health standpoint, the effects technostress has on total workers’ health should be addressed during medical surveillance, and prevention strategies should be put in place.
Footnotes
Author Contributions
M. R. G. and P. E. S. conceived the idea; M. R. G., M. F. R., C. A., and A. D. selected the articles; M. R. G. and M. F. R. led the writing; M. R. G., P. E. S., I. B., and U. M. revised and structured the manuscript; U. M. supervised the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.