
Abstract
Background:
Sleep health disturbances can increase risks for workplace injury, error, and poor worker health. Essential workers have reported sleep disturbances since the COVID-19 pandemic onset, which may jeopardize their health and safety. The aims of this project were to assess sleep health among Continuing Care Retirement Community (CCRC) workers, examine potential differences between worker types, and describe the self-perceived impact of COVID-19 on workers’ workload and sleep.
Methods:
Through an academic–practice partnership, this needs assessment used a cross-sectional design that collected self-report data during fall 2020 from CCRC workers. Guided by the Workplace Health Model, survey questions included work characteristics, sleep health, and COVID-19 impact on sleep and workload.
Findings:
Ninety-four respondents completed the survey across multiple departments. Respondents (n = 34, 36.2%) reported sleeping below recommended hours on workdays. The majority scored above the population mean on Patient-Reported Outcomes Measurement (PROMIS) measures of sleep disturbance (n = 52, 55.3%), sleep-related impairment (n = 49, 52.1%), and fatigue (n = 49, 52.1%). Differences in workday total sleep time and fatigue were noted among shift workers versus nonshift workers, with shift workers reporting less sleep and more fatigue. Shorter sleep duration was noted among respondents working shifts 10 or more hours compared with those working 8 hours. Pandemic-related workload increase was reported by 22.3% (n = 21) of respondents, with 17% (n = 16) noting more than one type of workload change. Since COVID-19 onset, 36.2% (n = 34) reported no sleep changes and 35.1% (n = 33) reported sleeping less. A medium, positive relationship was found between increased changes in work due to COVID-19 and increased difficulties sleeping (r = .41, n = 73, p = .000).
Conclusion/Application to Practice:
Proper sleep health is essential to workplace safety and worker health. By assessing sleep health during a crisis, occupational health nurses can identify opportunities to support worker health and safety, through sleep education, monitoring for sleepiness and fatigue, ensuring countermeasures are available (e.g., caffeine), and assessing for opportunities to change organizational policies.
Background
As with many aspects of people’s lives, the COVID-19 pandemic has changed the way individuals in the workforce sleep. Some Americans have reported improved sleep due to a decrease in societal intrusions on sleep/wake times (Gao & Scullin, 2020). Other workers have found sleep has worsened since before the pandemic as a result of more stress and changes to their life (i.e., family member test positive and workload changes; Gao & Scullin, 2020; Sagerman et al., 2020). Providing patient care during the pandemic seems to have contributed to healthcare worker’s sleep problems such as sleep quality or poor sleep duration (Herrero San Martin et al., 2020). A recent meta-analysis found slightly higher pooled prevalence rates of sleep problems for healthcare workers (36.0%) versus the general public (32.3%) (Jahrami et al., 2021). Frontline healthcare workers, including those working in Continuing Care Retirement Communities (CCRC), have described contributing work conditions, including heavier workloads, longer work hours, and higher levels of stress and anxiety since the onset of the COVID-19 pandemic (Sagherian et al., 2020; White et al., 2021; Zhuo et al., 2020). As a result, CCRC workers experiencing sleep changes may be at an increased risk of occupational injuries and decreased health and well-being (Lerman et al., 2012; Luyster et al., 2012). During times of crisis, it is vital for occupational health nurses working with CCRCs to assess workforce sleep health among all staff when evaluating workplace health promotion and injury prevention programs (Price et al., 2017).
CCRCs provide a wide variety of services for elderly and disabled individuals, such as independent living, assisted living, and full-time nursing care (U.S. Department of Health and Human Services, 2020). Because of the various care options, the workforce type is diverse, including shift workers required for 24/7 care (i.e., nurses, nursing assistants, and custodial staff) and nonshift workers (i.e., office workers, administrative staff, and management) who work more traditional 9 to 5 work hours. Meeting the health and safety needs of a workforce with widely differing job types can be challenging, particularly as nursing assistants, registered nurses, maintenance workers, and janitorial staff are occupations most at risk of injuries (Bureau of Labor Statistics, 2020). Although nonshift working CCRC staff such as administrative and business departments may not be as prone to physical occupational injuries, work–family and family–work conflicts can contribute to stress and psychological distress (Mutambudzi et al., 2017).
Regardless of work type, when sleep health such as sleep duration, sleep quality, and daytime alertness (Buysse, 2014) is poor, workers can experience fatigue, poor coordination, decreased attention, attitude, and mental health issues (Lerman et al., 2012; Pigeon et al., 2017; Stepan, 2020; Vandekerckhove & Wang, 2017; Van Dongen et al., 2003). Researchers conducting a meta-analysis of sleep and occupational injuries found workers experiencing poor sleep health had a 62% increased risk for an occupational injury or illness (Uehli et al., 2014). Unfortunately, more than one-third of all U.S. workers failed to meet recommended standards of 7 to 9 hours in a 24-hour period, with rates higher for those working shift work (Hirshkowitz et al., 2015; Khubchandani & Price, 2019). In the CCRC setting, this could translate to increased risks for occupational health and safety concerns across the broad spectrum of workers. Because of these risks, occupational health experts are increasingly calling for sleep health to be recognized as an important component of workplace health and safety and for sleep-promoting and fatigue mitigation strategies to be put into place (Caruso et al., 2017; Howard, 2020; Wong et al., 2019).
To incorporate these recommendations, occupational health nurses working with staff in the CCRC setting would need to assess the status of worker sleep health. Occupational health nurses can use assessment data obtained from a focused and formal evaluation to determine strategies most helpful to employees for achieving a healthy lifestyle (Price et al., 2017). There are multiple ways to gather sleep data from workers, including interviews, surveys, and wearable devices. For specific sleep needs assessments, workers can be screened for sleep disorders, such as insomnia, obstructive sleep apnea, restless leg syndrome, and shiftwork sleep disorder, with workers reporting positive screenings referred to sleep medicine specialists. Post data collection, it is necessary to analyze data to discern any patterns. Data patterns can help to prioritize the highest risk or needs to be addressed.
Conceptual Framework
To guide the evaluation, this needs assessment project used The Centers for Disease Control and Prevention’s (CDC) Workplace Health Model as a process model to steer the team toward success (CDC, n.d.). The Workplace Health Model includes four steps: (a) assessment, (b) planning and management, (c) implementation, and (d) evaluation. The model recommends evaluators consider the individual, organizational, and environmental domains as influential on sleep health. Expanding on the CDC’s Workplace Health Model, Price et al. (2017) define steps for a needs assessment as gathering data from the influential domains through surveys and/or interviews, analyze the data for significant patterns, and report the findings. As such, this assessment survey incorporated questions about the individual, workplace, and community factors that can intersect with sleep. Due to state-imposed CCRC visitor restrictions during the pandemic, project partners external to the organization were prevented from being on-site; therefore, this project focused only on the assessment step.
The purpose of this project was to conduct a health needs assessment of sleep with CCRC employees in the context of the COVID-19 pandemic. This needs assessment allowed for (a) descriptive statistics for comparisons to determine where CCRC sleep health may be below recommendations for health and safety; (b) comparison of sleep health among worker groups (i.e., shift working vs. nonshift worker, 8-hour vs. ≥10-hour shifts, and daytime vs. evening/night/rotating) to assess where targeted strategies for improvement may be necessary; and (c) description and examination of the self-perceived impact of COVID-19 on work factors, such as work hours or workload and sleep.
Methods
This needs assessment was conducted to determine the sleep health status of workers in a CCRC in the fall of 2020 during the COVID-19 pandemic. Gaining insight into the employees’ current sleep health status may help to identify gaps where occupational health staff can provide additional workplace support or further investigation. This needs assessment used a cross-sectional design, collecting self-report data via an anonymous online or paper survey (based on employee preference).
Setting and Sample
This project was developed through an academic–practice partnership between the University of Cincinnati, College of Nursing, and Maple Knoll Communities, Inc., both located in Southwest Ohio. The retirement center includes several campuses with facilities equipped to provide older adults care at varying degrees, including retirement living, assisted living, and skilled nursing. Approximately 25% of staff have positions that require evening or night shift hours, with the rest of the staff working during the day. All staff (N = 490) were invited to complete the survey.
Instrumentation
The survey had 25 questions and took approximately 10 to 15 minutes to complete. Face validity of the survey was assessed through consultation with five experts in the field. These experts were occupational health nursing students, registered nurses, and a human resource representative from the center. Data collected included demographics (age, race, ethnicity, gender, sex), sleep health measures (sleep duration, sleep quality, sleepiness, and fatigue), work characteristics (timing of shift, shift length, work tenure, work department, and weekly number of work hours), and questions related to work and sleep changes since the onset of COVID-19. COVID-19 questions were adapted from the COVEX questionnaire (Fisher et al., 2020). Sleep duration was measured using the Micro Munich Chronotype Questionnaire (µMCTQ; Ghotbi et al., 2020), a shortened version of the Munich Chronotype Questionnaire (Roenneberg et al., 2003), where workers were asked to report sleep times on workdays and work-free days. The four µMCTQ measures (sleep onset/offset on work and work-free days) correlated well with the full Munich Chronotype Questionnaire (r = .89–.95, p < .001), both of which have been validated with actigraphy (Ghotbi et al., 2020; Roenneberg et al., 2007).
Sleep quality, sleepiness, and fatigue were determined using Patient-Reported Outcomes Measurement Information System (PROMIS) measures. PROMIS (Ader, 2007) measures were developed through a National Institutes of Health initiative to establish common measurements of multiple outcomes and are available for public use. Raw scores were converted to a common T-score scale, where a T-score of 50 (SD = 10) was representative of the average U.S. general population. Scores above 50 represent more sleep disturbance, sleepiness, and fatigue and were used as the cutoff for this study. All three PROMIS instruments used in this study measured respondent answers from the past 7 days using a 5-point Likert-type scale. Sleep quality was measured using the PROMIS Sleep Disturbance 8-a Short Form (Yu et al., 2011), which has a high correlation (r = .90) with the 27-item PROMIS Sleep Disturbance long-form (Buysse et al., 2010; Yu et al., 2011) and high convergent validity (r = .83) compared with the gold-standard measure of sleep quality, the Pittsburgh Sleep Quality Index (Buysse et al., 1989). Sleepiness was measured using the PROMIS Sleep-Related Impairment (SRI) 8-item short form (Yu et al., 2011). The reliability of the SRI short form was strong (r = .90) when compared with the 16-item PROMIS SRI (Buysse et al., 2010). Convergent validity with the Epworth Sleepiness Scale (Johns, 1991) was adequate (r = .46). The PROMIS fatigue short form 8a measured a continuum of fatigue from tiredness to exhaustion, which can impact activities of daily living. Fatigue was one of the first PROMIS measures to be developed (Cella et al., 2007). Although the short fatigue form was designed for a universal population, it has been used with a wide variety of disease-specific populations as well as shift working nurses (Imes & Chasens, 2019).
Procedures
Staff were invited to participate in an online survey starting in September 2020. Invitations were sent via an internal company email from the retirement center study team member. The survey was available online for 4 weeks, with emailed invitations sent weekly for 3 weeks. With <10% response rate, the survey was made available again in November for 3 weeks. In addition to the emailed invitation, the online survey link was publicized via an app used by the organization as well as paper survey copies made available at employee entrances. Two respondents completed paper surveys. All data were submitted in REDCap, a secure web-based platform for data collection and management hosted by the University of Cincinnati and Cincinnati Children’s Hospital Medical Center (Harris et al., 2009). No incentive was offered to complete the survey.
Data Analysis
Data were analyzed using SPSS version 26 (IBM Corp., 2019). Data analysis included descriptive statistics (means, standard deviations, and frequencies) to define the respondent sociodemographics and prevalence of sleep health among the project cohort. Group comparisons (correlation and independent-sample t-test) were used to explore differences in sleep measures across groups (shift workers vs. nonshift workers, shift length, and shift timing). Significance was set at p value <.05. Nursing and Environmental Services were departments identified by the CCRC representative as areas workers were needed to be on-site during irregular work hours, such as night shift, evening shift, early morning work start times. As such, respondents self-reporting as working in these departments were categorized into shift workers. Respondents from all other departments (Activities, Business, Marketing/Development, and Outreach Services) were deemed nonshift workers, as their work hours were closer to traditional 9 to 5 hours. Other groups (8-hour vs. ≥10-hour shifts and daytime work vs. evening/night/rotating work) were determined based on self-reported responses to survey questions regarding shift length and shift timing. The needs assessment was deemed to be nonhuman subjects research by the University of Cincinnati, Institutional Review Board.
Results
A total of 94 (19.2%) participants from the study site completed the online or paper survey. Of the 94 participants, 74 had no missing data on all variables and were complete cases. The largest proportion of the respondents were within the age group of 46 to 60 (n = 37, 39.4%), White (n = 76, 80.9%), and female (n = 78, 83%). See Table 1 for demographic information. Most of the sample (n = 60, 63.8%) reported being partnered in a relationship. More than 50% of the respondents were nonshift and daytime workers, respectively. Of the sample, 60 (63.8%) worked 8 hours per day, and 53 (56.4%) had worked 6 years or more in their current job.
Participant Sociodemographic Categorical Data (N = 94)
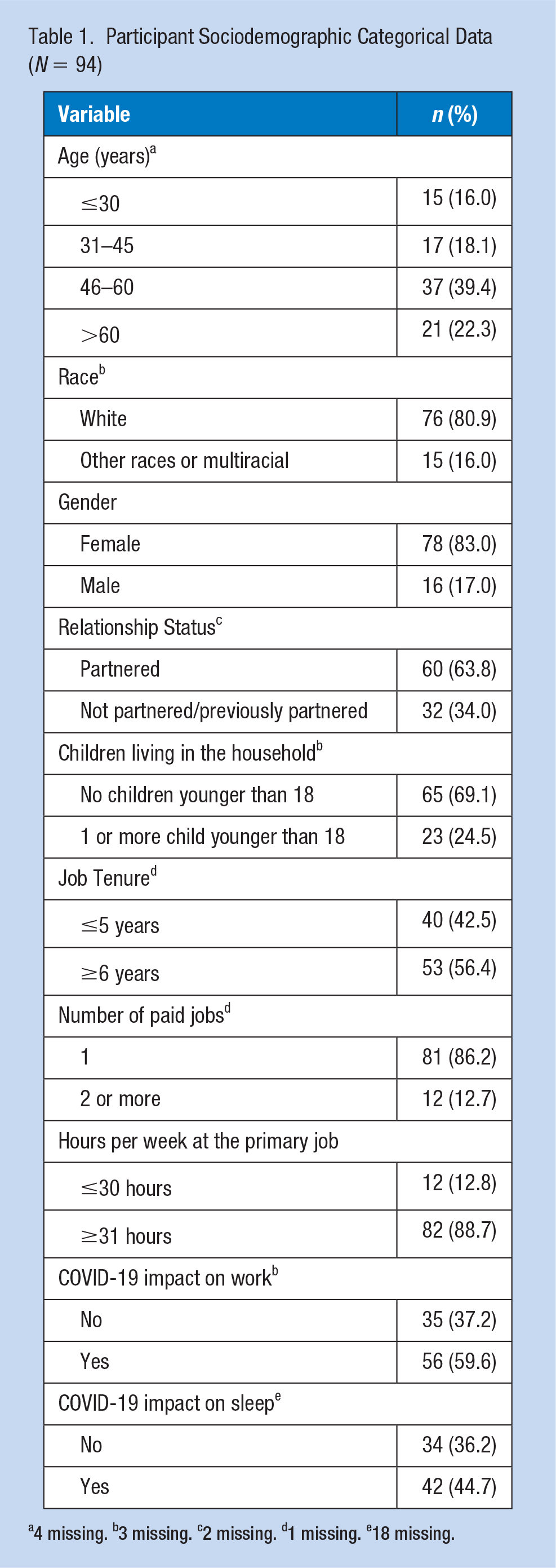
4 missing. b3 missing. c2 missing. d1 missing. e18 missing.
The summary of the participants’ sleep health characteristics is presented in Table 2. Of the 76 participants, the mean total sleep time on workdays was 6.7 (SD 1.3) hours and work-free days was 7.5 (SD 1.6) hours. As a result, 36.2% (n = 34) participants were reported as sleeping below the recommended 7 to 9 hours of sleep in 24 hours, and 19.1% (n = 18) slept below the recommended 7 to 9 hours of sleep on the days they were off from work. None of the participants slept above the recommended hours of sleep on the days they worked, but 8.5% (n = 8) slept more than the recommended 7 to 9 hours of sleep on the days they were off from work. For the PROMIS measures, participants reported an average sleep disturbance score of 53 (SD = 8.3), sleep-related impairment score of 51.5 (SD 9.7), and fatigue score of 52.3 (SD 9.3). Most of the sample had a score >50 in their sleep disturbance (55.3%), sleep-related impairment (52.1%), and fatigue (52.1%) total scores, which indicated they were experiencing worse sleep disturbance, sleep-related impairment, and fatigue than the average American adult.
Participant Sleep Health Characteristics Data (N = 94)
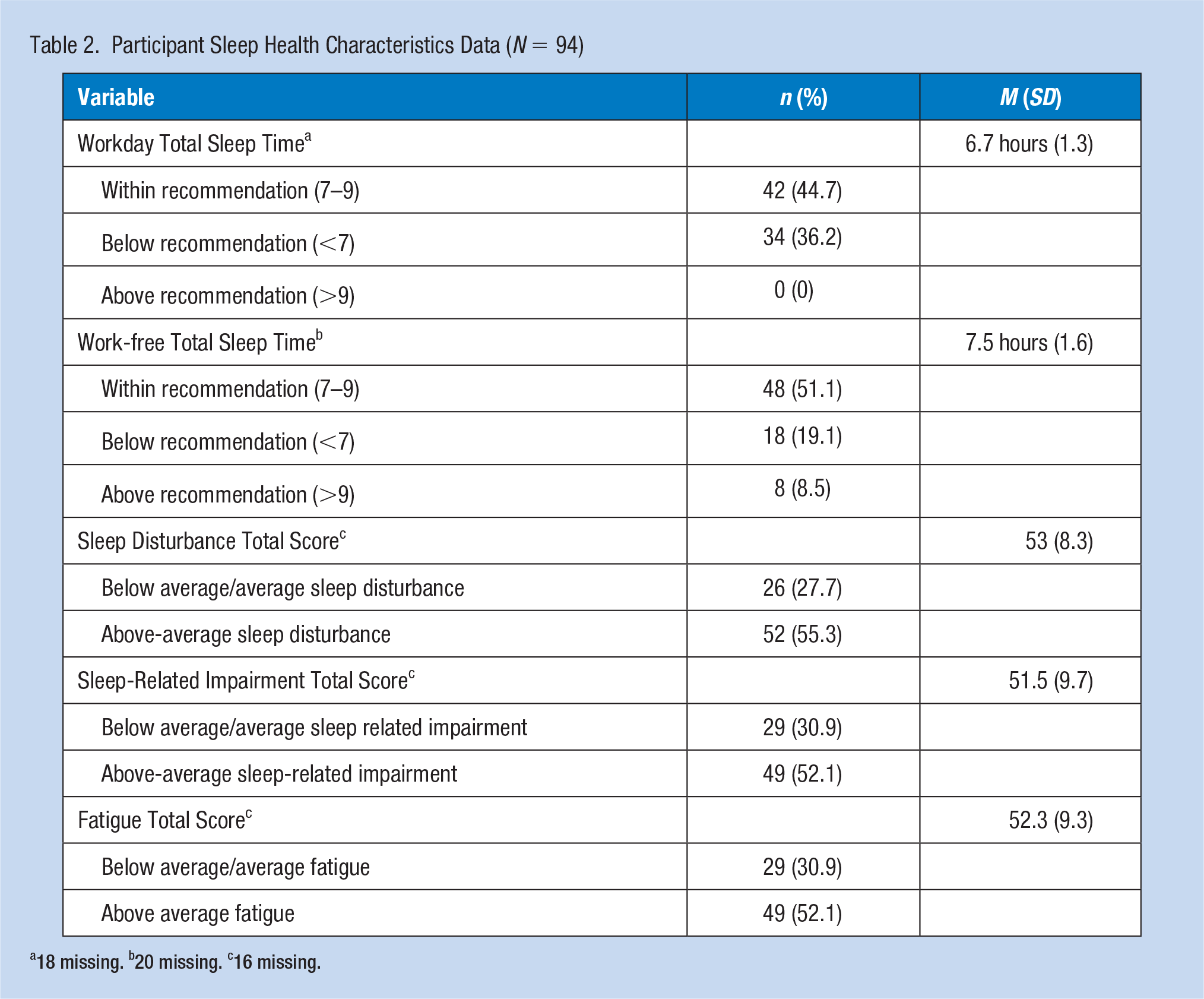
18 missing. b20 missing. c16 missing.
Table 3 presents the comparison of work schedule, shift working status, and shift length with their sleep health characteristic using independent samples t test (p value set at <.05). There was a statistical difference in the workday total sleep time and shift work status with a medium effect size, t(72) = 2.37, η2 = 0.07, p = .021, 95% confidence interval [CI]: [0.11, 1.29]. Reports showed that nonshift worker respondents (e.g., those working more typical 9–5 work hours) had on average 7 hours of sleep/24-hour period, while shift worker respondents reported an average of 6.3 hours of sleep on the days they worked. Despite both groups averaging fatigue scores above 50 (indicative of fatigue), analysis of shift work and nonshift work staff did demonstrate a significant difference with a medium effect size, t(74) = −2.24, η2 = 0.07, p =.028, 95% CI [0.51, 8.76]. Shift working staff (e.g., those working in areas requiring staff 24/7) reported an average fatigue score of 55.2, while nonshift worker respondents had an average fatigue score of 50.6. When shift length was compared with the workday total sleep time, a significant difference was observed, and a large effect size was reported, t(71) = 3.4, η2= 0.14, p = .001, 95% CI: [0.44, 1.69]. Staff who worked 8-hour shifts had an average of approximately 7 hours of sleep/24-hour period, and those who worked 10-hours, or more were getting closer to 6 hours of sleep/24-hour period on the days they had to work. No statistical significance was found among respondents identifying as having daytime schedules versus evening/night/rotating schedules. Despite the nonsignificance, trends were noted where respondents with evening/night/rotating schedules reported shorter workday sleep time, longer work-free sleep time, and higher scores were noted for sleep disturbance, sleep-related impairment, and fatigue scores when compared with respondents with daytime work schedules.
Sleep Health Characteristics by Work Schedule, Shift Working Status, and Shift Length (n = 78)
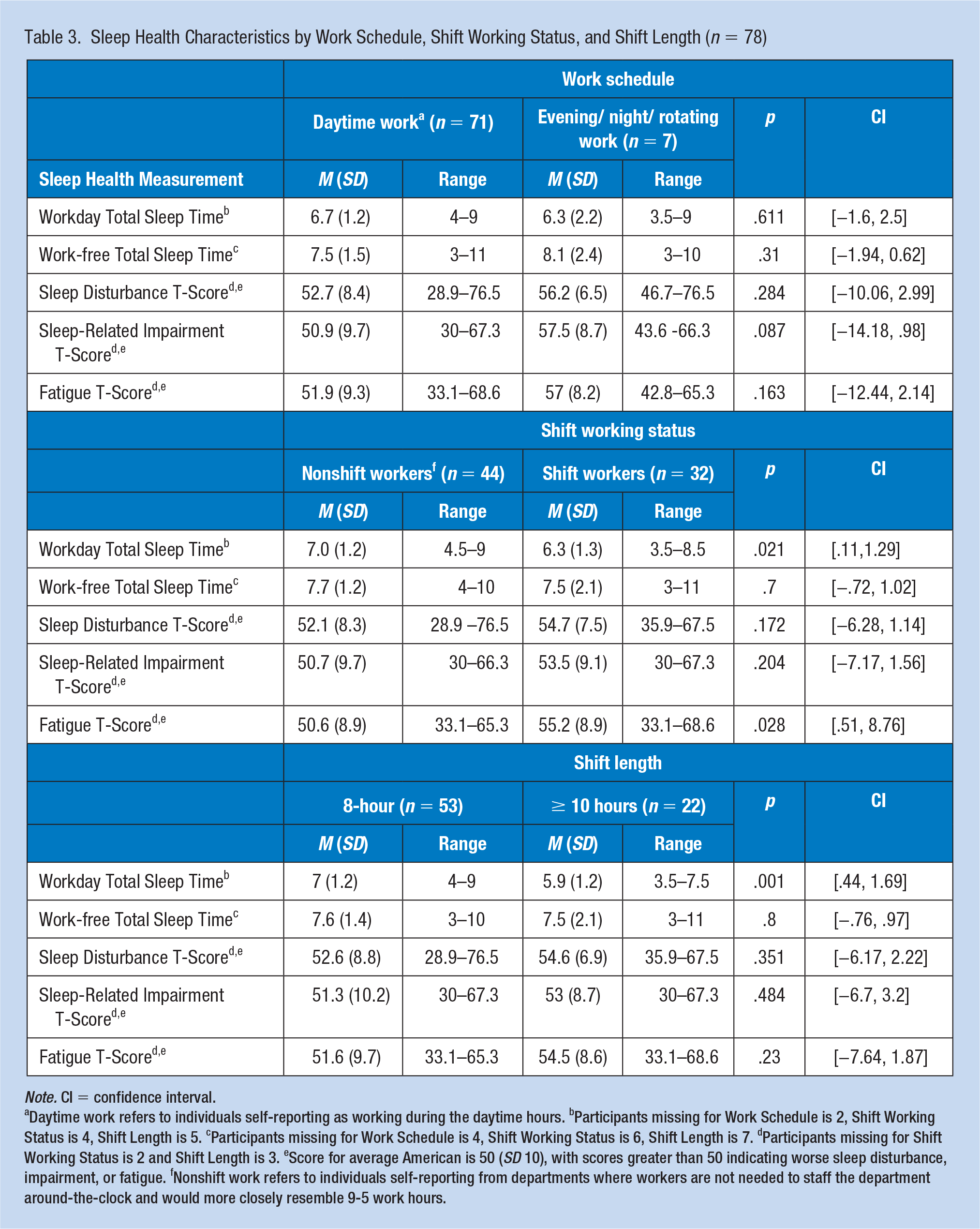
Note. CI = confidence interval.
Daytime work refers to individuals self-reporting as working during the daytime hours. bParticipants missing for Work Schedule is 2, Shift Working Status is 4, Shift Length is 5. cParticipants missing for Work Schedule is 4, Shift Working Status is 6, Shift Length is 7. dParticipants missing for Shift Working Status is 2 and Shift Length is 3. eScore for average American is 50 (SD 10), with scores greater than 50 indicating worse sleep disturbance, impairment, or fatigue. fNonshift work refers to individuals self-reporting from departments where workers are not needed to staff the department around-the-clock and would more closely resemble 9-5 work hours.
Table 4 presents the self-reported impact of COVID-19 on workload and sleep. Of the 91 participants who completed the COVID-19 workload survey item, 22.3% (n = 21) reported an increase in workload and 17% (n = 16) had more than one change (i.e., reported increased workload and increased work hours), while 37.2% (n = 35) had no changes in their workload. Regarding sleep changes due to COVID-19, 36% (n = 34) self-reported no sleep changes, and 35.1% (n = 33) slept less than usual. The relationship between reported changes in work and sleep due to COVID-19 was investigated using Pearson Correlation. A medium, positive correlation was found (r = .41, n = 73, p = .000), indicating as workers experienced significant changes in their job due to COVID-19, they also experienced changes in their sleep.
Impact of COVID-19 on Workers (N = 94)
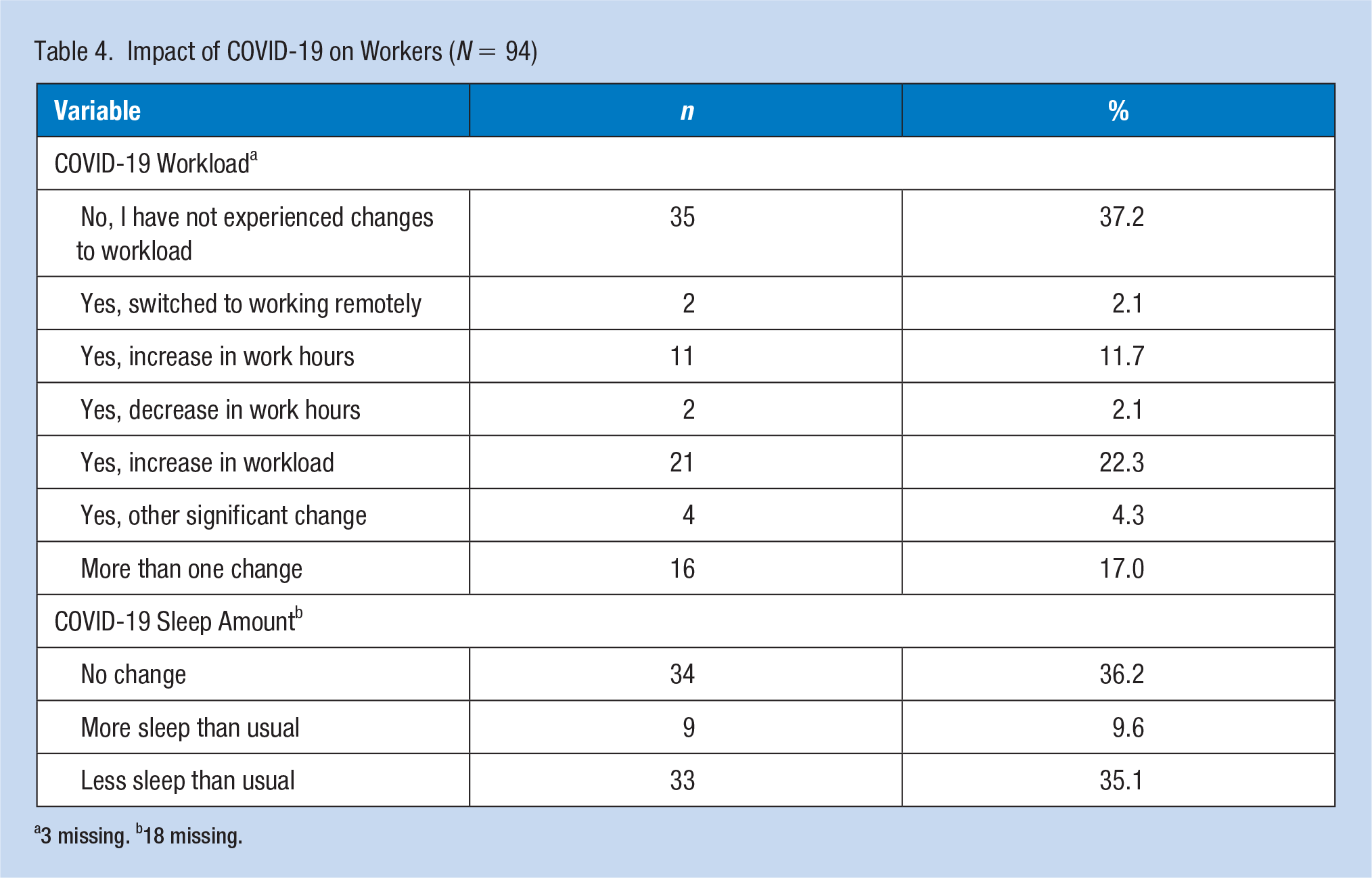
3 missing. b18 missing.
Discussion
Sleep health is a burgeoning topic and the importance of health and safety is gaining recognition within the field of occupational health. As such, this project was designed to assess the sleep health needs of CCRC employees at one organization while accounting for the assessment occurring during the COVID-19 pandemic. This needs assessment was designed for workers to self-report facets of their sleep health, allowing for an opportunity to identify areas for sleep health improvement and to distinguish changes resulting from the COVID-19 pandemic. The assessment results demonstrated on workdays, more than 36% of respondents were sleeping below the recommended 7 to 9 hours of sleep considered optimal for health and safety. This is comparable to national statistics among all worker populations, where the prevalence rates for workers sleeping below 7-hour/24-hour period increased from 30.9% in 2010 to 35.6% in 2018 (Khubchandani & Price, 2019). As sleep health is more than just sleep duration (Buysse, 2014), this assessment also included measures of poor sleep quality, daytime sleepiness, and overall fatigue scores. More than half of the respondents self-reported scores above the national average for all measures, indicating poor sleep health.
Multidimensional measures of sleep health have been evaluated in recent years and found to be associated with long-term implications in health and safety. In a nationally represented cohort of middle-aged men, higher multidimensional sleep health scores (daytime alertness, sleep quality, duration, regularity, efficiency, and timing) were statistically associated with lower cardiometabolic morbidity (Brindle et al., 2019). Similar results of sleep health measures (sleep satisfaction, wake after sleep onset, and minimal daytime sleeping) and cardiometabolic risk scores were reported among workers in extended care facilities (Buxton et al., 2018).
Educating workers on the health merits of all sleep dimensions, beyond sleep duration and sleep quality, may be helpful in future disease prevention. Sleep health education has the potential of improving sleep health. In a systematic review, Redeker et al. (2019) reported employer-sponsored interventions designed to improve sleep health, including educational programs, did result in positive sleep changes among workers. Although effective, the heterogeneity of intervention types and outcomes resulted in the researchers determining the evidence weak. Similar results were found in a systematic review of sleep health education among shift workers (Patterson et al., 2018). Despite the promising impact, <10% of workplaces surveyed nationally offered any sleep-promoting programming for workers (Meaklim et al., 2020). In addition to education, occupational health nurses could incorporate sleep disorder screenings into their worker assessments, monitor workers for sequelae of poor sleep health with sleepiness and fatigue surveys and ensure countermeasures to sleepiness and fatigue are available to workers. It is important to address the sleep deficit of staff in long-term care facilities by investigating resources to support staff during the pandemic and beyond.
When reviewing sleep health differences among worker groups, those designated as shift workers reported more fatigue and almost 40 minutes less sleep on average as compared with nonshift working colleagues. Workers reporting longer work hours were, on average, sleeping <6 hours/24-hour period on workdays. These findings were consistent with other studies, demonstrating long work hours encroach on time normally set aside for sleep (Mireku & Rodriguez, 2021). Due to these working conditions, shift workers and those working long work hours often lacked the opportunity for sleep and were needing to sleep at times outside the normal bedtime hours. This can disrupt sleep–wake cycles, increasing the risks for poor health and safety outcomes. Several researchers suggested that although shift work and long work hours contributed to worker fatigue, decreased well-being, and burnout, some work factors, such as regularly scheduled breaks and job control, can protect workers from these poor outcomes (Dall’Ora et al., 2016; Gifkins et al., 2020; McElroy et al., 2020).
In organizations requiring workers to fill shifts around the clock, ensuring organizational factors, such as shift length, breaks during and between shifts, and the number of successive shifts scheduled is not contributing to worker sleep deficits is key (Wong et al., 2019). Controlling these types of organizational factors is the first line of defense in a fatigue risk management system, a workplace health and safety program designed to mitigate fatigue risks in operational settings. Determining which factors were contributing most to poor sleep and if there were any protective work factors which could be employed to assist this CCRC worker population will require further evaluation.
Although COVID-19 has resulted in additional workload and sleep disturbances for essential and frontline healthcare workers, including this group of CCRC workers, the potential for continued sleep issues post-pandemic needs to be monitored. The pandemic has created increased stress and symptoms of psychological distress for frontline workers, which has been associated with disturbed sleep (Adamson et al., 2020). The implications of which have researchers suggesting a need for longitudinal monitoring of these effects (Marco et al., 2020; Sheraton et al., 2020). As a result, occupational health nurses will likely need to continue to monitor for sleep health disturbances associated with mental health issues to provide supportive measures as pandemic conditions evolve.
This needs assessment was limited by COVID-19 restrictions, preventing the research team from engaging directly with the CCRC staff to describe and promote the assessment. As a result, only about 20% of workers responded. This low response rate does increase the risk for sampling bias. Eleven respondents self-identified as evening or night shift staff, far below the approximately 122 workers employed to work these shifts. This worker population can be most at risk for sleep difficulties, so finding ways to further engage is important. Some respondents answered only a portion of the survey questions, including those related to sleep health. The PROMIS measures were designed to capture respondent information from the past 7 days. As this relates to the current assessment, PROMIS measures are indicative of a week of workdays and non-work days, not allowing for distinction. Finally, this was a sleep assessment of a single CCRC and cannot be generalized to other facilities.
Despite these limitations, the results of this needs assessment indicated some workers were not meeting the necessary sleep requirements for optimal health and safety. The prevalence of sleep problems was similar to what was found in the general worker population. Based on the Workplace Health Model, the next steps for an occupational health nurse would be planning and management (CDC, n.d.). Considering this assessment was limited by COVID-19 restrictions, engaging a wide variety of worker stakeholders in a full assessment of worker sleep would be essential in successfully planning any future educational or intervention strategies. Currently, leadership at the study site had expressed interest in a continuation of the academic–practice partnership. Collaboration from unit management also would have provided further support for effective planning and management strategies.
Conclusion
Sleep health is important for healthy living and can affect staff at work. It has become more pertinent since the onset of the COVID-19 pandemic, especially relating to staff at this CCRC. Considering the potential long-term impact of COVID-19 on worker sleep and the importance of sleep to disease prevention, occupational health nurses should consider assessing for sleep deficits in workers. CCRC workers would benefit from occupational health nurses providing education or implementing organizational changes to support sleep health as an integral part of the occupational health nurses’ health and safety practice.
Applications to Professional Practice
This sleep health needs assessment was conducted with staff at a CCRC during the COVID-19 pandemic. Although the pandemic limited the ability of the occupational health nursing research team to fully engage with the staff, results provided a preliminary indication of poor sleep health among 30% to 50% of the workforce. The pandemic had increased occupational health and safety exposures for frontline health care, including poor sleep health outcomes. Poor sleep health can further exacerbate mental health disturbances, increase risks for health outcomes (such as cardiometabolic disease), and place workers at risk for occupational injuries and errors. Due to the growing evidence regarding the importance of sleep to health and occupational safety, occupational health nurses can evaluate frontline workers for poor sleep health, regardless of the status of the pandemic. Evaluations would benefit from using an established evaluation model for guidance.
Footnotes
Acknowledgements
The authors acknowledge Dr. Gordon L. Gillespie and Dr. Carolyn R. Smith for their review of this manuscript and the support of the CCHMC Division of Biomedical Informatics and CCTST for supporting the REDCap clinical data capture service as a research resource at the University of Cincinnati.
Conflict of Interest
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B.M.H. and R.M.N. are funded by the National Institute for Occupational Safety and Health.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: R.M.N. is funded by National Institute for Occupational Safety and Health through the University of Cincinnati Education and Research Center, grant T42OH008432. The CCTST at the University of Cincinnati (provider of the REDCap services) is funded by the National Institutes of Health (NIH) Clinical and Translational Science Award (CTSA) program, grant 2UL1TR001425-05A. The CTSA program is led by the NIH’s National Center for Advancing Translational Sciences (NCATS). The content of this website is solely the responsibility of the CCTST and does not necessarily represent the official views of the NIH.
Human Subjects Review
This study was determined to be non-human subjects research by the University of Cincinnati, Institutional Review Board.
Author Biographies
Beverly M. Hittle is an occupational health nurse scientist with a special focus on sleep and shift work. Her contribution to this study included conception, acquisition, analysis, interpretation, drafting of the manuscript.
Ruth M. Norrell is a master’s student in Occupational Health Nursing at the University of Cincinnati with 30 years of nursing experience. Ms. Norrell’s contribution to this study included data acquisition, interpretation of the data, and drafting of the manuscript
Shammah Omololu’s contribution to this study included data cleaning, analysis, interpretation, and drafting of the manuscript.
Megan Gresham-Ulrich’s contribution to this study included data acquisition, interpretation of the data, and revising the manuscript.