
Abstract
Background:
Employment is an important social determinant of health, and supporting individuals’ return to the workforce is likely to have robust impacts on their health and well-being. The aim of this study was to identify (a) the self-perceived employment needs and expectations of users of community employment services; (b) the assets, needs, and barriers to reemployment among users of community employment services; and (c) areas of priority for programmatic development, including implications for patient–worker needs assessment and care coordination in clinical settings.
Methods:
We conducted structured interviews with 71 adults recruited from three workforce development programs located in the Chicago metropolitan area serving vulnerable workers. Topics of discussion included job histories, financial and social assets, and the respondents’ motivation and expectations for their return to the workforce. We used descriptive statistics to analyze quantitative responses and performed content analysis for qualitative data.
Findings:
Users reported discrimination, legal barriers, family responsibilities, physical or mental health concerns, and needs related to transportation and housing as common challenges to reemployment. Concerns regarding navigating complex social support programs to meet individual and family needs, as well as uncertainty regarding what would qualify as sufficient employment in order to not be reliant on these programs in the future, were expressed.
Conclusion/Application to practice:
Health care providers have opportunities to identify those that may benefit from comprehensive referrals to reemployment programs and social services. Occupational health providers are also in a unique position to enhance workforce development programs through collaborations to better educate and support workers.
Background
The relationship between employment and health is well documented in the literature, and work is included among the recognized social determinants of health (Gevaert et al., 2021; Schaap et al., 2018). The literature demonstrates a correlation between unemployment and ill-health (Krug & Eberl, 2018; Schmitz, 2011). The relationships between underemployment, as well as precarious employment, and ill-health are increasingly scrutinized, with evidence of a strong association between employment quality and workers’ self-reported health (Vanroelen, 2019). Policies and programs designed to support individuals’ return to the workforce, along with programs to bolster workers’ skills to promote employability and potential for advancement, are likely to reduce employment-related health inequalities and have robust impacts on individuals’ physical and mental health and well-being (Benach et al., 2010). There is an opportunity for assessment of patients’ comprehensive needs in many clinical settings, including needs for reemployment services and supports for attaining and retaining employment, to facilitate improvement in overall health outcomes.
Many agencies and organizations provide reemployment services to unemployed or underemployed populations that have often experienced incarceration, substance abuse, mental illness, disability, homelessness, or any combination of these concerns. Individuals who experience these phenomena often have large gaps in their employment histories, adding challenges when they attempt to reenter the labor force (Hahn et al., 2018; Holzer et al., 2003; Massoglia & Remster, 2019). These same individuals often struggle to meet basic needs, such as finding and maintaining housing and child care, or accessing safe and reliable transportation, which are likely to further compound the challenge of workforce reentry. These factors exacerbate individuals’ own perceptions of employability pre-employment, and job security once employed (Shier et al., 2012). Notably, these same struggles may prohibit individuals from entering workforce development or job training programs. Despite these limitations, many programs advertise themselves as specifically dedicated to providing reemployment services to populations who experience the aforementioned phenomena without having comprehensive mechanisms to address them. Occupational health professionals may want to be prepared for these additional challenges affecting unemployed workers and those engaged in low-wage, precarious work.
At their core, workforce development programs are designed to improve worker skills and thus increase workers’ labor market earnings (Holzer, 2008). However, while a worker’s skills are a key determinant of their labor market earnings, fundamental barriers to entry into workforce development programs make skill attainment challenging for those who do not have basic needs met. There is evidence that programs that provide vocational skills training help workers reenter the workforce following a long-term absence; however, many reemployment programs focus primarily on job-specific skill training without addressing other needs, such as transportation, that may affect an individual’s ability to maintain employment in the long term (Graham et al., 2010; Hodgson & Turner, 2003). This gap presents an opportunity for collaboration between occupational health practitioners, public health practitioners and agencies, and reemployment programs to do a comprehensive needs assessment and subsequent referral to support services that will collectively support a worker’s health and well-being.
In the United States, there are efforts at the federal and state levels to prioritize populations for workforce development programs and to ensure that they have standards for training and apprenticeship, but these efforts are limited in their impacts related to other determinants and services. There is little evidence that workforce development programs assess individual participants’ perceptions of employability or needs for services and supports before or upon entry into these programs (Wright et al., 2014; Zweig et al., 2011). Furthermore, programs that do complete evaluations are unlikely to ask participants about the use of other services that are unrelated to their program offerings, even though these services may be key to a participant’s successful reentry into the workforce (Olson, 2013; Zweig et al., 2011). There is an opportunity for all clinicians, but especially primary care, community/public health, and occupational health providers, to understand individuals’ comprehensive needs, including needs for reemployment services and other employment-related supports, to enhance their goals of improving health outcomes through broader service coordination.
The aim of this study was to evaluate the need for a comprehensive reemployment program among users of community programs in the Chicagoland area that emphasize workforce development and job placement by (a) assessing the self-perceived past, present, and future employment needs and expectations of users of community employment services; (b) evaluating the assets, needs, and barriers to reemployment among users of community employment services; and (c) identifying areas of priority for programmatic development. Furthermore, we examine study findings and discuss their implications for worker needs assessment and care coordination in clinical settings.
Methods
Study Population
In this concurrent mixed-methods study, we recruited participants from three reemployment programs in Chicago to participate in face-to-face interviews. Participants in the first of these programs, Program A, were unpaid and participated in various seminars and coursework that addressed topics related to securing employment (such as resume and interview skills), job skills development, and personal growth (such as self-esteem building exercises). Program participants were generally able to select which seminars and coursework they took as long as they committed to program and job-seeking activities full-time. Participants were also able to participate in a transitional job program, which included businesses owned by the program and several corporate partnerships. We recruited Program A participants at two separate locations. Program B is a public–private partnership that paid participants an hourly wage and provided both work experience and coursework to participants, resulting in marketable certifications and employment-related wraparound services (such as obtaining high school diploma equivalents and a driver’s license) over the yearlong program. All Program B participants were recruited from the same location. Program C enrolled participants in a multi-week workforce education and training program, designed to confer specific skills and certifications for application in specific industries. We recruited participants from three separate cohorts from Program C, only one of which included a stipend for participants.
Participants came to each of these programs via different pathways, including the criminal justice system, referral from other social services and charities, and self-referral. While not a requirement, many of these participants have experienced poverty, language or cultural barriers, precarious housing, incarceration, unemployment, and other life stressors before joining the program. These programs vary in length but generally lasted about 2 months or more and required attendance that was similar to full-time employment.
We employed purposive sampling to recruit adults who were fluent in English and had been in their respective program for at least 2 weeks. We assumed that very few program participants would not be fluent in English, as this was the language of instruction and assessment in these programs. In consultation with program directors, we determined 2 weeks to be sufficient time for participants to be familiar with the program and expectations, and understand that participation in these interviews was not required to continue to receive services.
The Institutional Review Board (IRB)–approved (University of Illinois at Chicago Protocol) consent document and initial parts of the recruitment process and interviews clearly articulated that qualification for services from their program was not contingent on their participation in this study. Participants were compensated US$20 for their participation.
Interview Instrument
The interviewer-administered questionnaire was based on the known needs of those with unstable or a lack of housing, as well as the general population, when seeking future employment. It queried information regarding job histories, financial and social assets, and the respondents’ motivation and expectations for their return to the workforce using both open-ended and closed-ended questions with prompts to add more information for the closed-ended responses. This questionnaire has been used in previous studies (Madigan et al., 2020) and required only slight modifications to ask about technical skills preparation and remove elements specific to residential rehabilitation programs.
All interviews were conducted in-person and audio-recorded by one of three interviewers between November 2017 and June 2018 until response saturation was reached. Two interviewees declined recording (one each in Programs A and C), so responses were written on the questionnaire by the interviewer as the interview took place. Interviews were conducted at the program facilities in private rooms. Any additional information offered by the respondent to contextualize answers was also recorded, and the interviews were not time limited. The interviewers had no affiliation with the programs.
Analysis
The interviews were transcribed by a research assistant and organized by responses to each questionnaire item in Excel. Responses were read and reread by two interviewers. Data were analyzed descriptively comparing the three different programs. The closed-ended responses were analyzed using SAS 9.4, while the open-ended responses were assessed in Microsoft Excel using content analysis. Content analysis allows for descriptive analysis of qualitative data similar to thematic analysis, while also considering a quantification of the qualitative data (Vaismoradi et al., 2013). The authors developed a codebook with literature-based a priori codes prior to the analysis and subsequently added emergent codes after an initial reading of all transcripts. Coding was completed by one author and the other author verified coding. As the interviews were structured, most responses fell within the code assigned each question. Discrepancies between reviewers were discussed until both reviewers agreed on the final interpretation. This analysis primarily complemented the quantitative data and provided additional context for participants’ responses to closed-ended questions. Responses were left in the participants’ words rather than recoded to reflect external definitions of variables, such as housing status.
Results
A total of 71 individuals across the three programs completed the interviews and were included in the analysis: 30 interviews with participants from Program A, 13 interviews with participants from Program B, and 28 interviews with participants from Program C. Two interviews were not included in the analysis: One participant unexpectedly needed to leave the interview during the initial questions for personal reasons unrelated to interview content and one participant stated he would not answer questions and was only there for the compensation. Overall, 69 interviews (97.2%) were audio-recorded, and interviews lasted 34 minutes on average (range = 16–75 minutes).
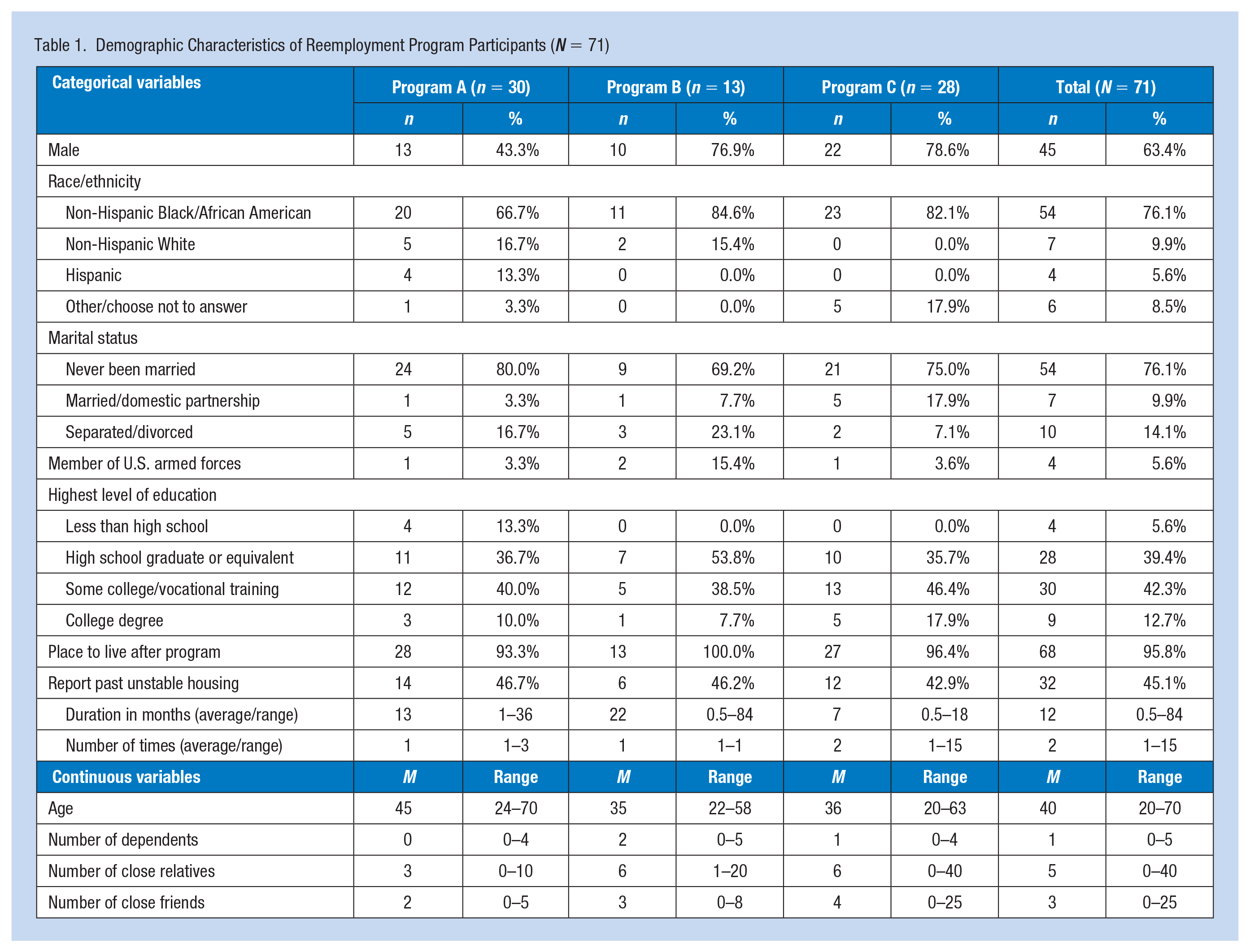
Demographic characteristics for the samples from each program are included in Table 1. Respondents were predominantly male (with the exception of Program A which was only 43.3% male), Black, and were on average approximately 35 years old (with the exception of Program A, which had a mean age of 45). Of note, over half of the participants had attained education past high school or a GED and had social support networks of five close relatives and three close friends. Despite almost half (45.1%) of the participants reporting previous unstable housing, with an average of 2 times and a year in duration, almost all reported having a place to live after the program (95.8%). This is likely an overestimate, as people reported living arrangements that would fit criteria for precarious housing as defined by U.S. law (U.S. Code, 2012). Several participants described the challenge of maintaining housing, even with family members, while they were unemployed or searching for work, as summarized by this 43-year-old male participant in Program A: I’ve had some issues with my siblings at home and last year because I have not been able to find work . . . one of my siblings was threatening to kick me out of the house and make me homeless.
Another participant, a 20-year-old male in Program C, summarized his feelings of incomplete independence given his lack of permanent housing, which was echoed by other participants: I’m currently homeless right now, not homeless sleeping on the streets but I don’t have my own place . . . makes you get a feel of I’m half way there I just need that extra push, working for your house and your own car you feel untouchable.
Demographic Characteristics of Reemployment Program Participants (N = 71)
Attitudes Toward Future Employment
Getting a job was a priority for most participants (91.5% extreme or important priority; Table 2). Similarly, most participants noted that having a job is extremely or very important for their future (95.8%) and felt extremely or very confident they would get a job within the following year (93.0%) reporting, on average, that it would take less than 2 months to secure employment. Nobody reported feeling unprepared to get a job, which is reflected in their self-assessment of having sufficient skills for the job they want. Overwhelmingly, participants reported being confident in their skills but were most likely to report a lack of confidence in their computer skills (11.3%) followed by their math (8.5%) and technical (8.5%) skills.
Number and Percent of Self-reported Job Preparedness Characteristics of Reemployment Program Participants (N = 71)
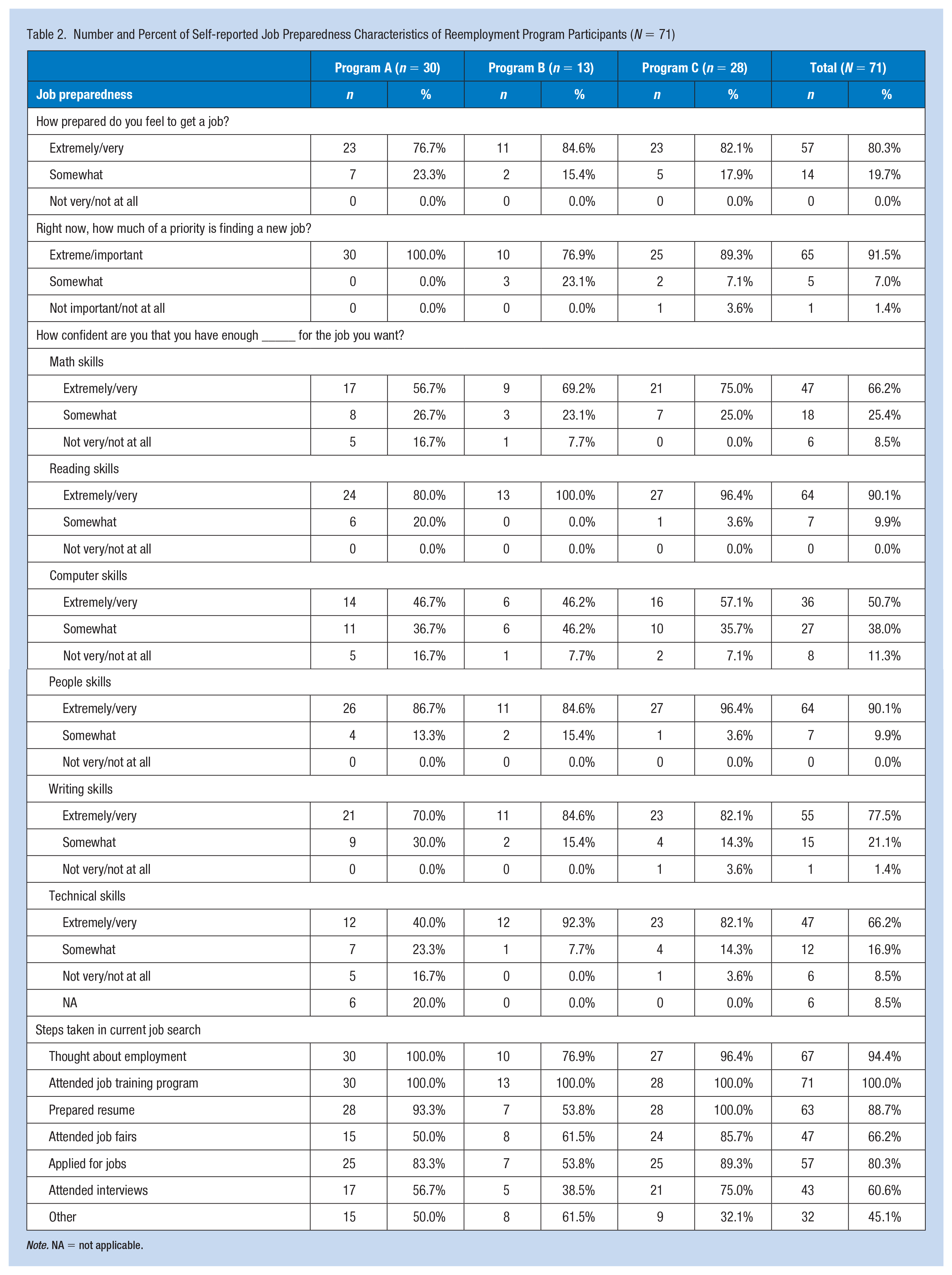
Note. NA = not applicable.
Participants reported taking various steps in their current job search with over half of participants in all programs having already applied for jobs. Many participants reported previous experience with reemployment programs and 91.5% identified them as being helpful. A small portion (12.7%) reported participating in employment programs that were not helpful.
More than a third (39.3%; n = 11) of Program C participants reported having a job offer and an additional 14.3% (n = 4) reporting a possible job offer. A 40-year-old male participant from Program C noted that Program C was particularly helpful in conferring desirable job skills and noted that he had a job offer as result of his participation in the program: I, actually, I already had a job offer the first day out of our job forum . . . so the guy just actually just called me today and try to set up an interview with me today or tomorrow so yeah the program was outstanding for me.
Programs A and B were less likely to report firm or possible job offers (Program A: 20% reported having a job offer, 23.3% reported a possible offer; Program B: 7.7% reported having a job offer, 15.4% reported a possible offer). However, these job offers were not necessarily for full-time, permanent positions that offered the compensation participants felt was necessary to meet their basic needs, particularly in the long term. Some of these were secured through the program, but others were jobs held before entering the program that did not provide enough stability.
Reflections on Past Employment and Previous Injuries at Work
On average, participants in all programs reported having five (range = 1–25) previous jobs that they would put on their resumes, but the average time that had elapsed since their last job varied with Program A reporting 30 months (range = 0–168 months), Program B reporting 17 months (range = 0–144 months), and Program C reporting 10 months (range = 0–60 months). Past employment aligned with future employment, both in the present and long-term aspirations.
Participants in all programs (n = 14, 19.7%, range = 15.4%–23.3% within each program) reported suffering an injury at one of the five most recent jobs they would put on their resumes. No participant reported more than one injury that resulted in seeking medical care. Of those, eight (57.1%) reported receiving disability or workers’ compensation for those injuries; however, in further description, some participants only described receiving paid time off or receiving compensation from insurance because of vehicular involvement. At least one of the individuals reporting no compensation for their injuries was self-employed. In addition, two of the participants expressed having additional concerns about their injuries as they were pregnant at the time. At least one participant, a 46-year-old female in Program B, noted that their injury contributed to their current unemployment and described the challenge of maintaining work while injured: I mean recently, my injury, me getting hurt and I couldn’t, I left, yeah it was my last job, well I would say that they kind of forced me cause they kept me on the job that was kind of hindering my ability to complete because of my injury so I left . . .
Barriers to Reemployment
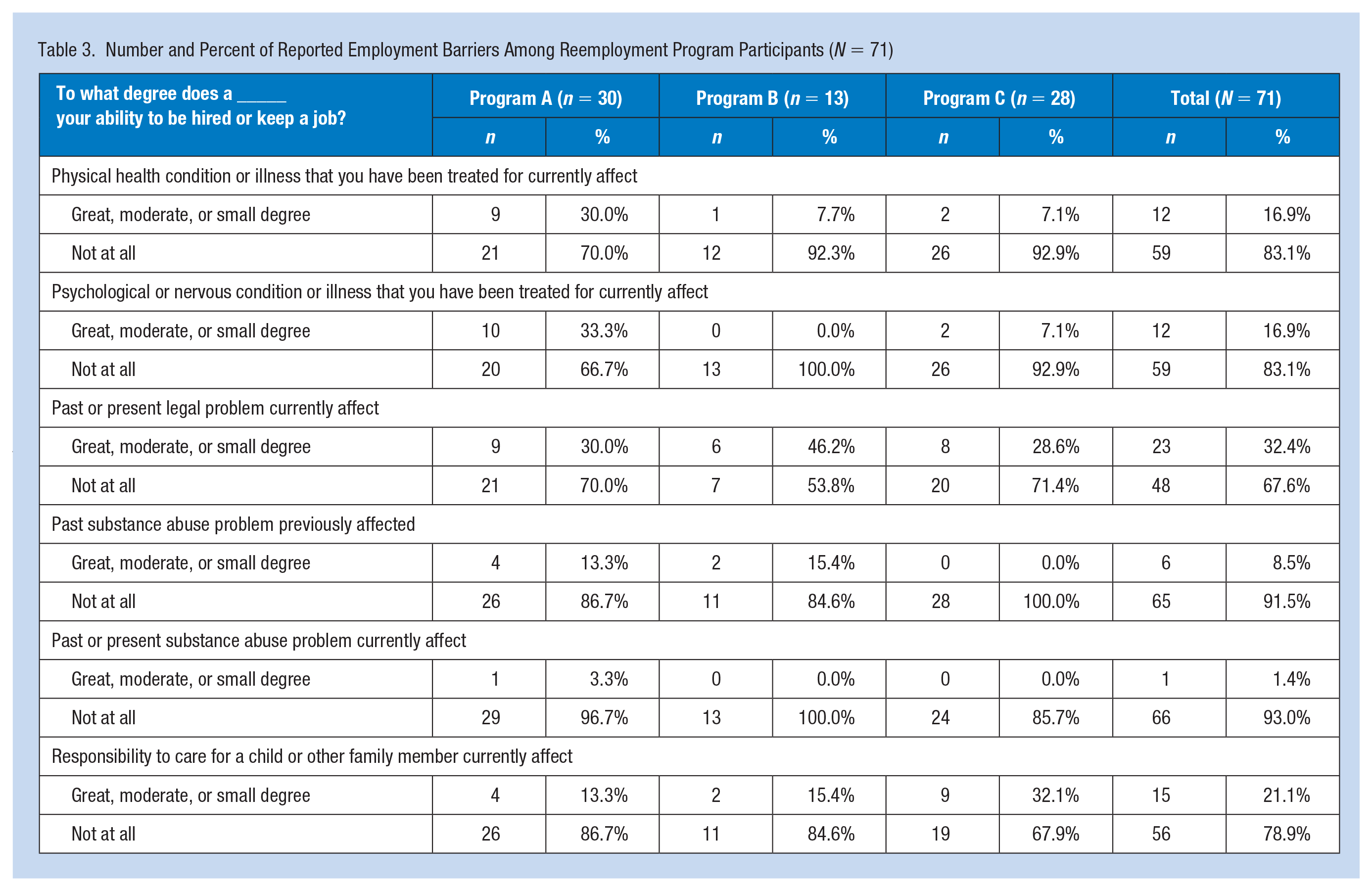
Participants described a variety of barriers to employment, including lack of control over the reasons for their recent unemployment (46.5%), physical health issues (16.9%), mental health issues (16.9%), legal problems (32.4%), substance abuse problems (8.5%), family responsibilities (21.5%), discrimination (46.5%), and lack of desire to seek new employment (11.3%) (see Table 3). Physical health concerns were related to the ability to keep up with speed and mobility demands, side effects of medications like fatigue, or exacerbation of chronic conditions no longer controlled by their current treatment that can impair breathing and mobility. Mental health concerns were primarily from sleep, attention, and anxiety disorders that were being managed by a health care professional. Participants were concerned that they would not be able to perform the work expected of them long term, that work would exacerbate their symptoms and conditions, and work structure could diminish their ability to maintain their health due to reasons such as not being able to take medications as scheduled.
Number and Percent of Reported Employment Barriers Among Reemployment Program Participants (N = 71)
A few participants noted that these barriers were significant contributing factors to their decisions to attend a reemployment program. One 26-year-old male in Program B shared that their background led to their decision to attend, saying, “My background, I have a felony. No that’s pretty much it, like if I didn’t have the felony then I wouldn’t even be here today to be honest.”
Several participants who listed family responsibilities as barriers to employment described the particular challenge of finding available and reliable child care, summarized by this 33-year-old female in Program A: . . . so many people need childcare, like with my kids being different ages it would have to be a slot being filled it would have to be available you know and then they maybe have no open slots till next year or next 5 or 6 months and you’re like waiting so it’s like that.
Participants also reported feeling underqualified (21.1%) and overqualified (32.4%) for the jobs to which they were applying. Of those who reported feeling overqualified, approximately half (46.8%) reported this as a barrier to reemployment. A 61-year-old female in Program A described their level of education as a barrier compared with others in their program, saying, “I have a college degree and some people don’t here, but they’re getting jobs and I’m not.”
Another participant, a 62-year-old female in Program A, shared that they felt both overqualified for some jobs, given their skillset and experience, but underqualified for others due to the gap in their employment, saying, “I’m overqualified for clerical work, underqualified for the work I was doing because I was off; so therefore, you can’t keep up with business and what’s going on with technology and stuff if you’re not there.” Program A reported being underqualified and overqualified with the same frequency, while the other programs were more likely to report being overqualified and reported being underqualified less frequently than in Program A.
Comprehensive Needs
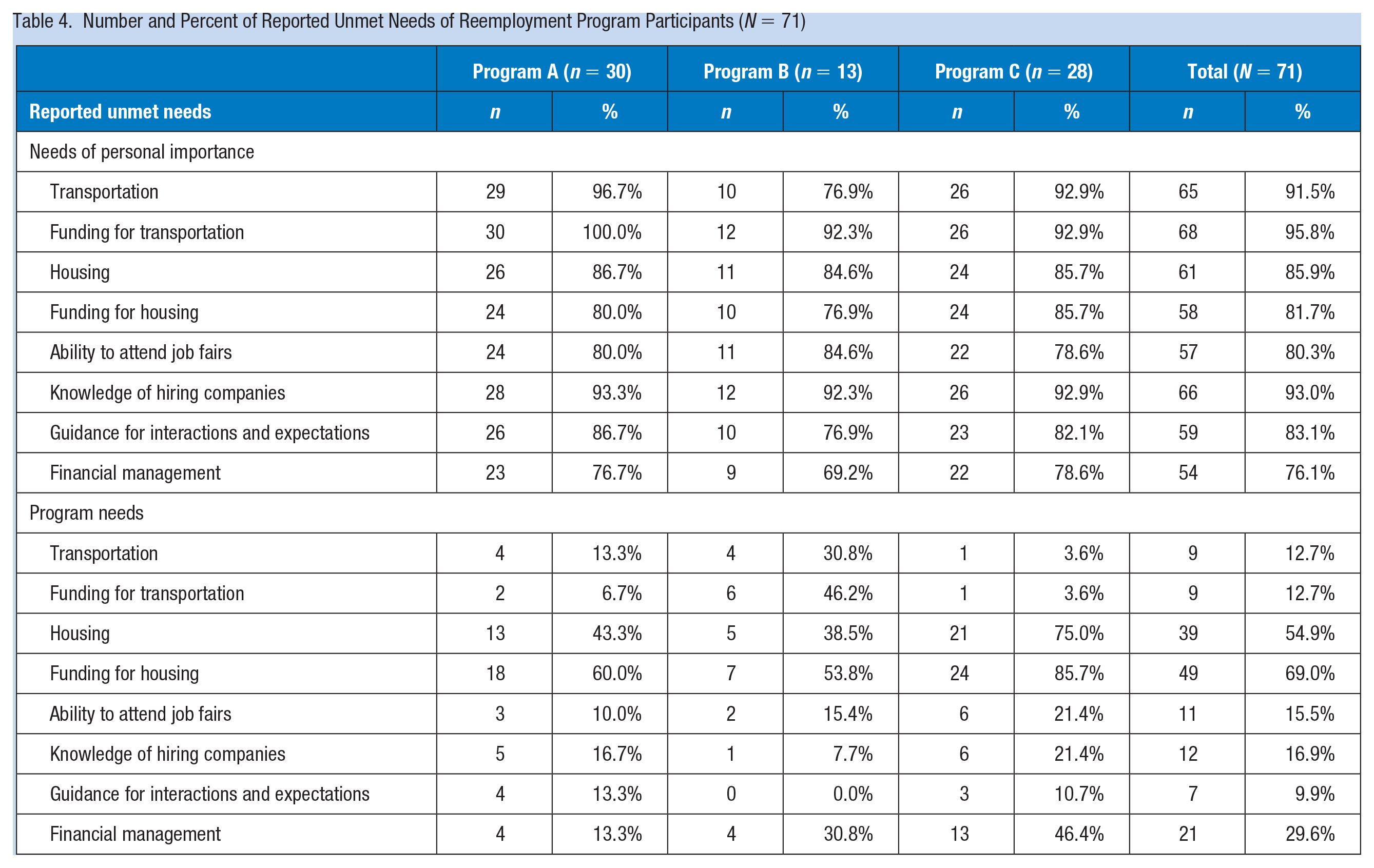
Participants described a variety of personal needs that affected their search for and retention of employment, including transportation (91.5% needed access to, 95.8% needed funding for), housing (85.9% needed access to, 81.7% needed funding for), financial management advice (76.1%), guidance for interacting with potential employers (83.1%), and knowledge of and access to employers who are hiring (93.0%) (Table 4). While acknowledging that reemployment programs cannot and are not expected to provide all needed services, particularly as individuals transition out of a program, participants described unmet needs that would support reemployment. Housing was the most frequently cited area of needed support, with 69% of respondents indicating that funding for housing was needed and 54.9% indicating that access to housing was needed. A 48-year-old male in Program B summarized these sentiments: I think it should be like some kind of transitional housing that not only are you transitioning people to go out in the work force, you should be transitioning people in bad situations to be able to take care and be on their own and be more independent. Cause it’s a lot of people here from conversations I hear that are in different situations . . . people can be successful and get employment but the things that’s going on in their life can stop that cause you’re not independent.
A 50-year-old female in Program A noted that simply providing a list of resources and expecting the participants to sort through available supports was insufficient: . . . she just gave me information and listings about for the low-income housing . . . I need more assistance with that cause it’s kinda hard, because, I don’t know, some of them want you to be working or already have an income. I just want to get a place; I know I don’t have an income but if I can get a place . . . even though I don’t have a job right now I’m working towards getting one.
Number and Percent of Reported Unmet Needs of Reemployment Program Participants (N = 71)
Discussion
The findings from this study highlight the multitude of challenges that under-resourced individuals face when seeking to return to the workforce and maintain stable employment. Data from this study suggest that these three reemployment programs—though targeted at individuals who experience particular challenges to employment, including previous incarceration, homelessness, and other contributors to gaps in employment histories—are unable to meet the comprehensive needs of their participants that would facilitate job attainment and retention. While some reemployment programs may have the agility and resources to fully support their participants with comprehensive services, it is likely that many programs, similar to those included in this study, are unable to meet the range of unique and complex needs of their individual participants.
Despite participants’ assessments that these programs conferred the knowledge and skills required to reenter the workforce, many had enrolled in similar programs on more than one occasion and had experienced significant employment instability that could be attributed to challenges meeting basic needs. This preparation, if other basic and prerequisite needs are unmet, will leave successful graduates of these programs unlikely to attain stable employment and thus unlikely to realize the health benefits associated with employment.
Both quantitative and qualitative findings elucidate the complexities study participants experienced when navigating auxiliary supports to attain and sustain employment, both prior to and while taking part in a reemployment program. Several participants articulated the cyclical challenges of finding stable housing and maintaining needed safety net benefits while searching for or trying to keep a job, and others noted the challenges associated with child care and other family responsibilities that have contributed to job loss or job insecurity. These phenomena are clear contributors to employment instability and are well documented as chronic contributors to poor health and well-being (Loprest & Nightingale, 2018). This study contributes to this existing body of evidence and showcases a gap in the existing assistance structures and networks for individuals who are likely to benefit from reemployment services but for whom other collateral supports are both needed and lacking.
Given the importance of stable and secure employment as a social determinant of health, we argue that there is an opportunity for clinicians to identify patients who might benefit from reemployment services, assess their needs for other comprehensive services that would support a successful transition to reemployment, and provide comprehensive referrals to appropriate services. Clinicians are likely to interact with individuals who may seek reemployment and related services: Study participants described a range of experiences that contributed to their unemployment or underemployment, including previous work-related injury or illness, physical or mental health issues, substance abuse problems, homelessness, and family-related responsibilities, many of which might precipitate a clinical encounter. In addition, enrollment in these programs is often a condition of being on parole or receiving unemployment or other social benefits. This also makes access to quality programs of greater importance for individuals.
While workers who sustain a serious work-related injury are likely to be seen by a clinician and are perhaps more likely to be connected with appropriate support resources given the nature of the clinical encounter, clinicians are also likely to engage with others who may benefit from reemployment and other comprehensive services that would facilitate improvement in health outcomes. The impacts of work-related injuries can be compounded as clinical services are likely less to be accessible to low-wage workers and the consequence of work-related injuries can be loss of a job. Health care providers and case managers will need to help the worker connect with state workers’ compensation and other programs to receive medical care, wage replacement, and referrals for continued care and rehabilitation that may enable future employment.
While the clinical and care coordination infrastructure may not yet exist or be sufficiently robust to connect individuals to comprehensive services to support a transition to employment, establishing such networks in clinical practice to address social determinants of health continues to gain traction within the medical field (Andermann, 2018). Additional opportunities exist to collaborate with robust health systems already serving these workers, such as the Veterans Affairs centers or managed care groups, that can also provide care coordination and social service referrals. There may also be opportunities for health care providers outside of these systems to refer patients to comprehensive support systems, which may include focused reemployment systems alongside other social services, whether they seek clinical care for an employment-related injury or illness, or whether they see a clinician for concerns that may seem superficially unrelated to employment. In addition, there is some confusion on worker rights, reporting, and compensation for injuries in our study population. This has been seen in other clinical settings and there may be additional opportunities for clinics and health care providers to help educate workers independently or in collaboration with community groups that serve these individuals (Topete et al., 2018).
The subjects of this study were participants of intensive, well-respected programs in an urban setting, which may limit the generalizability of study findings. However, this particular sample offers insight into challenges faced by some of the most comprehensive and well-resourced programs that provide reemployment services to particularly vulnerable subsets of the population. The findings highlight the need for expanded identification of participants’ needs and provision of appropriate supports to ensure their success in attaining and maintaining employment. We also caution that this study captures only the experiences of individuals who were able to commit to programs that require an intensive and long-term commitment, and the needs of marginalized workers who were unable to participate in programs similar to those of focus in this study may have different and more substantial needs to support employment. Future studies could collaborate with community-based supportive services to study the needs of these workers.
Implications for Occupational Health Practice
The link between employment and health is well established, but health and employment challenges are often addressed separately. Reemployment programs, even when well designed, face a number of challenges in holistically supporting the attainment of sustainable employment. Occupational health care providers depending on their work setting may have opportunities to identify those that may benefit from comprehensive referrals to reemployment programs and social services. They should consider the complexities of the challenges facing the individual and their history with these programs when determining where to refer. Occupational health providers, especially those in state or local government and community-based health care systems, are also in a unique position to enhance reemployment programs through collaborations to better educate and support workers.
Applying Research to Occupational Health Practice
Given increased precarity in employment, which is sometimes exacerbated by work-related injury and illness, occupational health care providers will need to be versed in reemployment programs and supports needed for those in these programs. Our study findings suggest that even the most comprehensive programs are unable to meet the demand for basic services that would support employment and health as many participants reported additional needs and barriers in the structured interviews. There are opportunities to provide a more comprehensive support system for individuals that would benefit from stable employment. While directly addressing these needs may not be realistic for traditional onsite occupational health nurses, these considerations could be included in standard referral lists that are commonly used in clinical practice and public health settings.
Footnotes
Authors’ Note
The work is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute for Occupational Safety and Health.
Author Contributions
Dana Madigan and Tessa Bonney made a substantial contribution to the concept and design, acquired and interpreted the data, drafted the article, and approved the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors were supported by the Illinois Education and Research Center, Grant Number T42/OH008672, from the National Institute for Occupational Safety and Health (Centers for Disease Control and Prevention [CDC]).
Author Biographies
Dana Madigan, DC, MPH, PhD, is a research assistant professor in the Division of Environmental and Occupational Health Sciences at the University of Illinois at Chicago and an assistant professor at National University of Health Sciences. Her research explores the relationship between unstable housing, employment, and health.
Tessa Bonney, MPH, PhD, is a postdoctoral fellow at the Great Lakes Center for Occupational Health and Safety and research assistant professor in the Division of Environmental and Occupational Health Sciences at the University of Illinois at Chicago. Her research explores the relationship between precarious employment and health.