
Abstract
Background:
During the COVID-19 pandemic, use of symptom-screening tools to limit attendance of infected workers has been widespread. However, it remains unknown how the reliability of responses to these tools may be compromised by individual and social factors. We aimed to determine whether personal concern over lost wages impacts responses to COVID-19 symptom-screening questionnaires making them less useful in limiting person-to-person transmission.
Methods:
We utilized an anonymous online questionnaire, administered through personal social media networks and those of two U.S. private colleges between September 16, 2020 and November 2, 2020 and distributed to currently or recently employed individuals 18 years of age or older. Participants considered ambiguous hypothetical scenarios involving possible COVID-19 symptoms or exposure and responded to a COVID-19 symptom screen (N = 219).
Findings:
In response to symptom-related scenarios (i.e., elevated temperature or slight cough), respondents lacking access to paid sick leave were 2.2 to 2.7 times more likely to attend work than those with access to paid leave (p < .05). This was not true for contact-related scenarios. Pay type and income level also significantly influenced screening responses.
Conclusion/Application to practice:
Risk of acute wage loss and overall financial stability appear to influence work-attendance decisions with regard to COVID-19 symptom screens. Broadened availability of paid leave and additional specificity within screening questionnaires would likely improve symptom-screen reliability.
Background
When the novel coronavirus SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2) first swept across the United States in March 2020, symptom questionnaires became a common tool to screen sick employees and limit the spread of coronavirus disease 2019 (COVID-19; Gostic et al., 2020). Attempting to keep infected employees out of the workplace, employers in 44 U.S. states required or recommended that their workers complete a COVID-19 symptom-screening questionnaire, provided by the employer, before attending work (Mendelson, 2020). Symptom screening has been recognized as a potentially useful tool to limit virus transmission during the COVID-19 pandemic; Centers for Disease Control and Prevention [CDC], 2020a), however, their effectiveness is likely reduced by asymptomatic and mildly symptomatic infections, which may be overlooked or confused as symptoms of a less severe condition (e.g., Breslin et al., 2020; Callahan et al., 2020 and personal factors that result in employees ignoring or misrepresenting their risk status.
Fear of stigma (Kadowa & Nuwaha, 2009) and the perceived risk of lost income or work opportunity (DeRigne et al., 2016; Rubin, 2020) have been shown to encourage employees to adopt a “need-to-know” strategy when disclosing health-related information to an employer (Munir et al., 2005; Westerman et al., 2017). As such, the accuracy of symptom-screening questionnaire responses may be influenced by possible negative repercussions, like the threat of economic hardship. Service-sector workers (e.g., in retail and food service) comprise approximately 20% of the American workforce, and about 55% of these lack paid sick leave (Schneider & Harknett, 2020). If the risk of personal monetary loss leads employees to misrepresent their current symptom experience, symptom-screening questionnaires would be less effective toward their aim. Here, we investigate the hypothesis that, when confronted with a risky but ambiguous scenario related to COVID-19 symptoms or contact, individuals without access to paid leave will be more likely to attend work than those with paid leave.
Methods
We utilized an anonymous online questionnaire, administered through Google Forms, and promoted through public Facebook groups with varying demographics (a low-to-medium socioeconomic neighborhood group and two private-college alumni groups), personal Facebook pages (with sharing enabled) of both authors, and the message board for current undergraduate students at the authors’ institution. Participants were required to self-certify informed consent, age ≥ 18 years, and experience completing a symptom screen within the prior 30 days. This limited the sample to those recently or currently employed, but we thought it important for participants to have some prior experience with a symptom screen. Four hypothetical scenarios were presented that suggested the respondent had either mild COVID-19 symptoms or a recent contact with a likely or confirmed case. After reading each scenario, respondents were asked how they would respond to a specific related question on their hypothetical employer’s COVID-19 screening questionnaire with implications for attending work or not clearly indicated. Responses were collected from September 16, 2020, through November 2, 2020. In total, there were 250 participants; however, 30 participants were excluded due to ineligibility. This study was approved by the Aquinas College Institutional Review Board (IRB #2020-339) on September 15, 2020.
The first scenario stated that the participant was coughing “slightly more than usual” (cough scenario); the second involved taking their temperature and having a fever or a borderline fever before work (temperature scenario). In the third scenario, the participant attended a socially distanced but unmasked gathering with someone who later presented COVID-19 symptoms and was awaiting test result (gathering scenario). In the fourth scenario, the participant dined at a restaurant and then learned that a server there tested positive for COVID-19 (server scenario). All scenarios ended with, “You think it’s unlikely, but not impossible, that you have been exposed to COVID-19.”
At the time of our study, close contact was defined as being “within 6 feet of someone who has COVID-19 for a total of 15 minutes or more,” having “direct physical contact,” or getting “respiratory droplets on you” (CDC, 2020b). Common recognized symptoms of COVID-19 include a fever (variably defined as ≥100.4°F or above 98.6°F), chills, and/or a dry cough (CDC, 2020c). An individual with close contact with a COVID-19-positive individual or any common symptoms was advised to isolate for 14 days from the date of contact/onset (CDC, 2020b).
After reading the scenarios, participants had the option to identify their access to paid time off, wage type, and income level. The four options for leave availability were as follows: “My employer has offered additional sick leave due to COVID-19”; “I have enough PTO and/or sick days to take paid time off”; “If I take time off, it would be unpaid”; and “If I take time off, I would worry about losing my job.” Income level was delineated as less than US$15,000, US$15,000 to US$29,999, US$30,000 to US$44,999, US$45,000 to US$59,999, and more than US$60,000 (Levels 1 and 5, respectively). The lowest category represents individuals earning below the federal poverty line, while the top represents above-average earners in the researcher’s locality (Semega et al., 2020). The options for compensation type were “Salary” and “Hourly”.
Statistical Analyses
We considered each independent predictor variable (availability of paid leave, income level, and compensation type) separately in the context of each scenario (cough, temperature, gathering, and server). Levels for “availability of paid leave” were grouped into participants with some form of available leave and those without this option. For each scenario and predictor level, we calculated the percentage of the respondents choosing each response on the symptom screen (e.g., proportion “yes”/“no” among respondents with paid leave). Using logistic regression with binomial error distribution, we considered the influence of each predictor on responses to each of the four scenarios. Reference groups for these variables were set as paid leave available, income less than US$15,000, and salaried compensation. The dependent or outcome variable was work attendance. Post hoc power analyses indicate that all tests reporting a significant result were sufficiently powered (range = 0.64–0.99, average = 0.818). Statistical analyses were performed in R version 3.3.0 (R Core Team, 2016).
Results
Usable responses for at least one comparison were provided by 219 respondents. Some participants declined to respond to demographic questions about paid leave availability, income level, and/or income type, and one declined all three questions (number declining = 22, 8, and 9, respectively). One respondent declined one scenario response. Seventy-five percent reported having some form of employer-provided sick leave (Table 1). The proportion of respondents in each income category (lowest to highest) was as follows: 17%, 16%, 14.6%, 21.7%, and 30.7%, respectively. Income types were evenly represented (salaried = 53%).
Characteristics of Participants and Summary of Responses to COVID-19 Symptom Screen After Considering Each of Four Scenarios Related to Symptom Development and Potential Contact (Total N = 219)
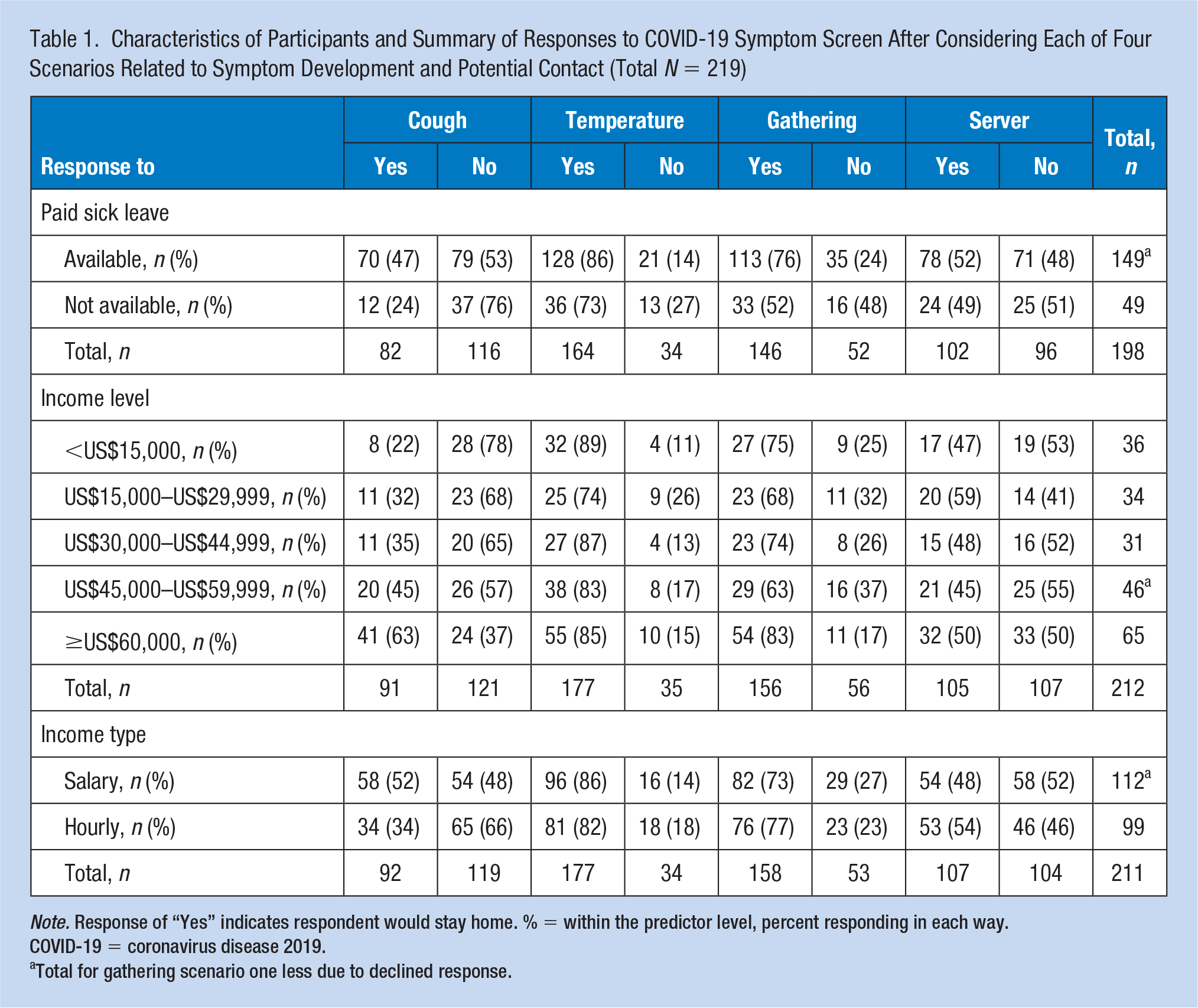
Note. Response of “Yes” indicates respondent would stay home. % = within the predictor level, percent responding in each way. COVID-19 = coronavirus disease 2019.
Total for gathering scenario one less due to declined response.
Among the 20 possible combinations for the three predictors, the most-populated categories were leave-eligible/Level 5/salaried employees, leave-eligible/Level 4/salaried employees, and leave-ineligible/Level 1/hourly employees (25%, 15%, and 11% of respondents, respectively; Table 2). Salaried employees were minimally represented among those lacking paid leave or those in the lowest two income levels.
Distribution of Respondents (N = 219) Among the Possible Combinations of the Three Independent Variables
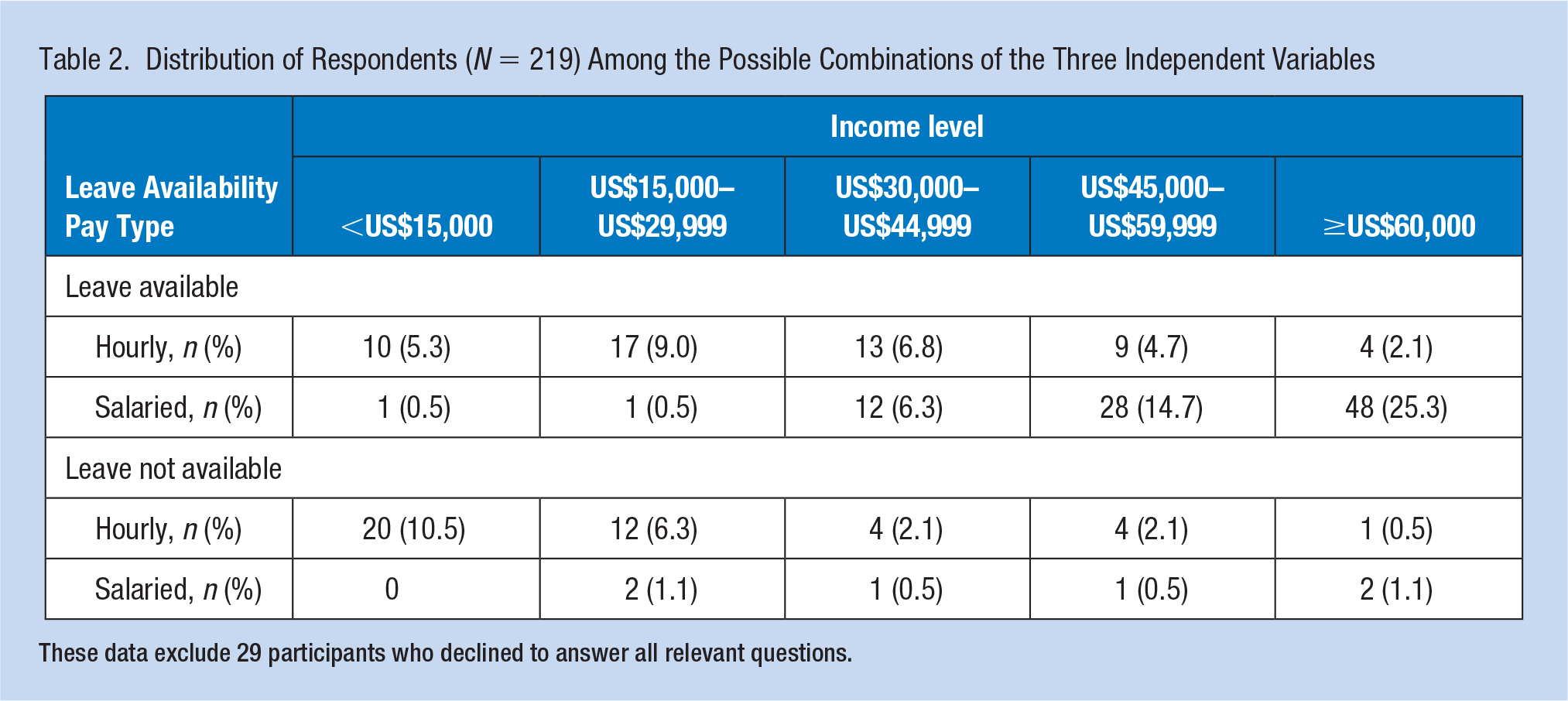
These data exclude 29 participants who declined to answer all relevant questions.
In response to the cough scenario, respondents with paid time off (which includes those with special COVID-19-related provisions) were similarly likely to attend work or stay home (Table 3). Respondents without access to paid leave were significantly more likely to attend work than those with paid leave (odds ratio [OR] = 2.73, 95% confidence interval [CI] = [–1.77, 0.31]). In response to the temperature scenario, respondents with paid leave were significantly more likely to stay home than to attend work (OR = 0.16, CI = [1.39, 2.31]). Respondents without access were significantly more likely to attend work than the former group (OR = 2.2, CI = [–1.58, –0.003]). After the gathering scenario, respondents with paid leave were more likely than not to stay home (OR = 0.32, CI = [0.80, 1.55]). For those without access to paid time off, the OR of attending work was greater than one but not significantly different from the baseline group (OR = 1.52, CI = [–1.13, 0.28]). No significant differences within or between leave-availability groups were found for the server scenario.
Odds and ORs of Attending Work Within Each of Four Scenarios Related to COVID-19 Symptom Development or Contact (Total N = 219)
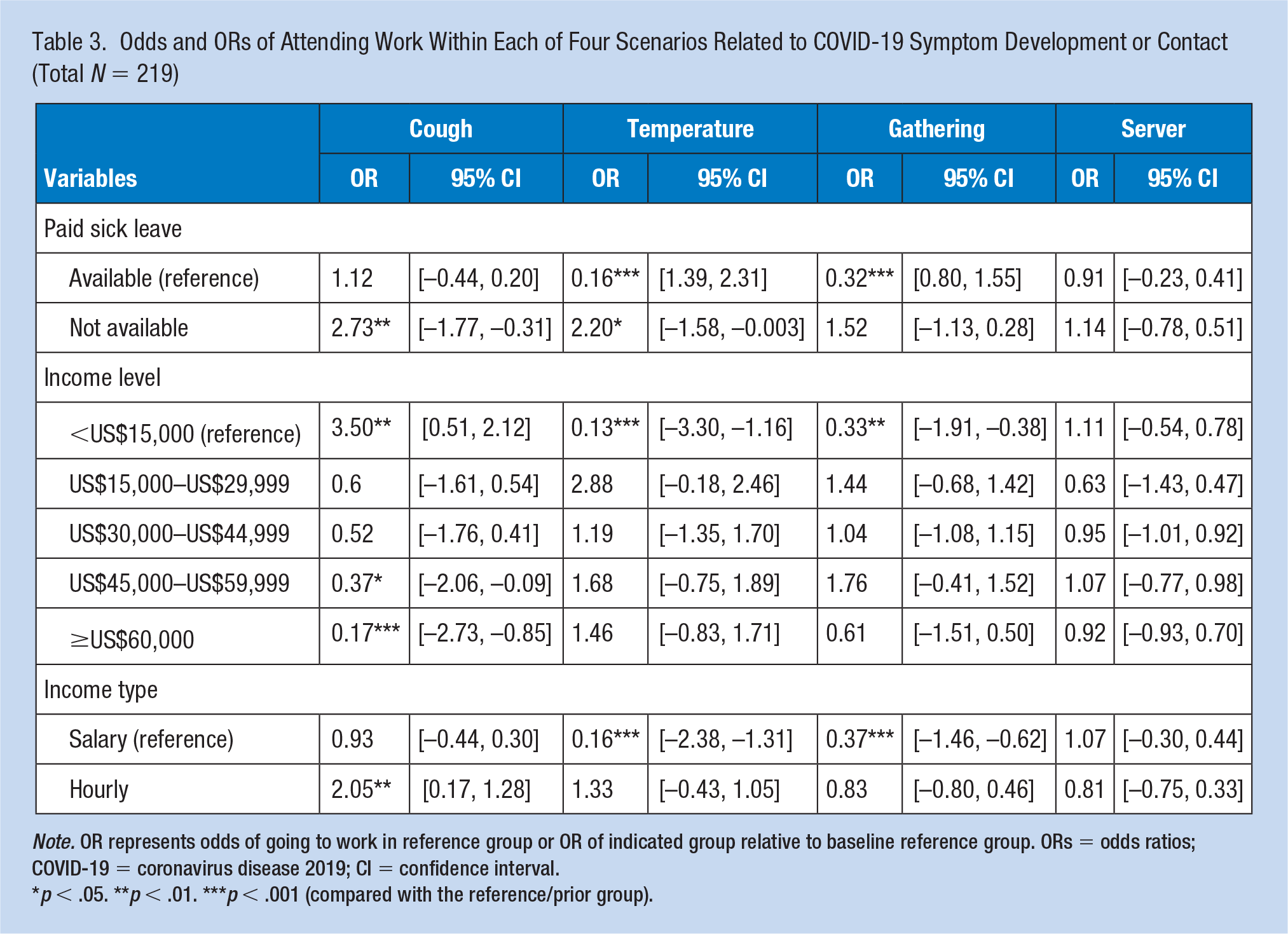
Note. OR represents odds of going to work in reference group or OR of indicated group relative to baseline reference group. ORs = odds ratios; COVID-19 = coronavirus disease 2019; CI = confidence interval.
p < .05. **p < .01. ***p < .001 (compared with the reference/prior group).
In response to the cough scenario, odds of attending work were high among the baseline income Level 1 (OR = 3.5, CI = [0.51, 2.12]). No significant differences were present between Income Levels 1 and 2 or between Income Levels 2 and 3. However, a significantly increasing likelihood of staying home was present as income increased from Level 3 to 4 and from Level 4 to 5. In response to both the temperature and gathering scenarios, odds of attending work for respondents in Income Level 1 were low (temperature: OR = 0.13, CI = [–3.30, 1.16]; gathering: OR = 0.33, CI = [–1.91, 0.38]), and no significant differences were found among the income levels. No significant differences within or between income levels were found for the server scenario.
In response to the cough scenario, salaried respondents were similarly likely to attend work versus stay home. Hourly respondents were significantly more likely to attend work than salaried workers (OR = 2.05, CI = [0.17, 1.28]). In response to both the temperature and gathering scenarios, odds of attending work among salaried respondents were low (temperature: OR = 0.16, CI = [–2.38, –1.31]; gathering: OR = 0.37, CI = [–1.46, –0.62]), and hourly respondents did not differ significantly from this baseline group. No significant effects of income type were found for the server scenario.
Discussion
Managing the spread of communicable diseases such as COVID-19 requires an understanding of individual willingness to accept risk for themselves and others, especially when societal influences and vulnerabilities to infection overlap. The influences of societal inequalities on this risk-taking behavior must be considered in the design and deployment of public health measures. In this study, we presented individuals with ambiguous scenarios about symptoms of and exposure to COVID-19 and considered the influence of job and income security on responses to a simulated symptom-screening tool. Availability of paid sick leave, pay type, and income level all significantly influenced responses to scenarios. Willingness or intention to attend work despite potential risks was stratified across socioeconomic levels.
For respondents lacking access to paid leave, willingness to attend work after scenarios involving the development of mild COVID-19 symptoms was 2.2 to 2.7 times greater than for those with available leave (temperature and cough, respectively). This outcome for the temperature scenario is particularly notable as respondents with paid leave were significantly more likely to stay home (a 14% probability of attending work). These findings support our hypothesis that concern over lost wages may influence willingness to accept risk during a pandemic and could influence greater infection and transmission rates among already vulnerable populations.
Potential indicators of the participant’s overall financial security also affected responses to the cough scenario. Here, participants in the lowest income level were 3.5 times as likely to attend work as to stay home. In contrast, the two highest income levels were significantly less likely to attend work than participants in the levels below. Salaried respondents showed no significant preference; however, hourly respondents were twice as likely to attend work. For the temperature scenario, no significant influence of income level or pay type was present; all respondents coalesced around the choice to stay home. Income level and income type may be less impactful on individual decision making than the influence of lost daily wages.
Although the contact scenarios did not directly support our hypothesis, they reveal an interesting phenomenon. For the gathering scenario, respondents were consistently unlikely to attend work. This suggests general societal consensus regarding the appropriate response to a contact scenario involving personal acquaintances. In contrast, responses to the server scenario show a notable lack of consensus. No significant signal was present among respondents in the baseline group (47%–48% probability of attending work), and no significant differences were present among levels of the predictor variables.
Our results indicate that both acute loss of wages and overall financial stability may influence willingness to accept risk (to self and others) and therefore influence individual responses to COVID-19 symptom-screening questionnaires. Our results imply that the reliability of COVID-19 screening questionnaires may be significantly hampered by individual tolerances for lost wages, financial instability, and the potential to cause or assume health risks.
Limitations
Our study was limited by exclusion of respondents who lack access to social media, a relatively small sample size (N = 219), and the time period in which responses were collected (September 16, 2020–November 2, 2020). In addition, in not controlling for location, our data may be influenced by varying local positivity rates or social norms. Furthermore, we were not able to calculate a response rate because we had no ability to estimate the sampling frame. Despite our study’s limitations, our findings provide beneficial insight into COVID-19 symptom-screening questionnaires, an area in which there is minimal current research.
Implications for Occupational Health Practice
Our study highlights compelling occupational health considerations related to the spread of SARS-CoV-2. We reason that paid leave availability for all employees would serve dual benefits. Those who utilize leave during illness would be buffered from negative financial consequences. In addition, protection would be afforded to those who might otherwise be in contact with symptomatic coworkers. It is also notable that access to paid leave, income level, and wage type are likely to be confounded with other systemic inequalities. Frontline workers often lack access to paid leave; occupy relatively low-paying, hourly positions (Schneider & Harknett, 2020); and are more likely to be people of color, women, and immigrants (Rho et al., 2020). These conditions, perhaps more than behavioral or preexisting health factors (Raisi-Estabragh et al., 2020), could contribute to the higher rates of COVID-19 seen in minority groups (Bui et al., 2020), making access to paid leave even more critical for frontline workers and those in already precarious financial circumstances. Case studies examining the effects of newly deployed benefits on the spread of common diseases like Influenza or COVID-19 within frontline-worker populations would be illuminating.
Another implication of our work is that risk assessment information from employers, public health authorities, and governmental sources should be as specific and easy to understand as possible to guide employees in evaluating and responding to risk, especially in scenarios involving casual or short-term exposure. Embedding this guidance within the screening tool is recommended. Decisions to stay home from work when it would be safe to attend work increase frustration and/or likelihood of non-compliance at a later time (i.e., decision fatigue; Dai et al., 2015; Muraven & Baumeister, 2000; Simon, 1955). Future studies could investigate the idea of personal “compliance fatigue” during a long-term public health crisis, especially when compliance results in a personal cost.
Applying Research to Practice
This study examined whether societal and personal factors bias responses to COVID-19 symptom-screening questionnaires conducted by employers. When confronted with hypothetical onset of COVID-19 symptoms, respondents lacking paid sick leave were more likely to attend work than those with paid leave. Occupational health practitioners, especially those in high-contact industries such as food service or health care, may consider these findings during contact tracing interviews and clinical encounters with sick employees. These findings suggest that occupational health providers should advocate for paid leave policies to benefit health and safety of employees and their workplace contacts. Increased specificity of screening questions or embedded guidance about best practices is also suggested to improve reliability of symptom-screening tools.
Research Data
sj-xlsx-1-whs-10.1177_21650799211053231 – Supplemental material for Safety Nets Work Both Ways: The Influence of Available Paid Leave on Employee Risk Taking During the COVID-19 Pandemic
sj-xlsx-1-whs-10.1177_21650799211053231 for Safety Nets Work Both Ways: The Influence of Available Paid Leave on Employee Risk Taking During the COVID-19 Pandemic by Teegan R. Galdeen and Rebecca P. Humphrey in Workplace Health & Safety
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received initial financial support through the internal Mohler-Thompson Research Fellowship program.
Human Subjects Review
This study was approved by the Aquinas College Institutional Review Board (IRB #2020-339) on September 15, 2020.
Author Biographies
Teegan R. Galdeen has a BSc in health science and is a master of public health student at Grand Valley State University.
Rebecca P. Humphrey is an assistant professor in the Department of Biology and Health Science at Aquinas College. She has a BSc in biology and a PhD in evolution, ecology, and behavior.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.