
Abstract
Introduction:
Several reports have emerged describing the long-term consequences of COVID-19 and its effects on multiple systems.
Methods:
As further research is needed, we conducted a longitudinal observational study to report the prevalence and associated risk factors of the long-term health consequences of COVID-19 by symptom clusters in patients discharged from the Temporary COVID-19 Hospital (TCH) in Mexico City. Self-reported clinical symptom data were collected via telephone calls over 90 days post-discharge. Among 4670 patients, we identified 45 symptoms across eight symptom clusters (neurological; mood disorders; systemic; respiratory; musculoskeletal; ear, nose, and throat; dermatological; and gastrointestinal).
Results:
We observed that the neurological, dermatological, and mood disorder symptom clusters persisted in >30% of patients at 90 days post-discharge. Although most symptoms decreased in frequency between day 30 and 90, alopecia and the dermatological symptom cluster significantly increased (p < 0.00001). Women were more prone than men to develop long-term symptoms, and invasive mechanical ventilation also increased the frequency of symptoms at 30 days post-discharge.
Conclusion:
Overall, we observed that symptoms often persisted regardless of disease severity. We hope these findings will help promote public health strategies that ensure equity in the access to solutions focused on the long-term consequences of COVID-19.
Introduction
After more than 20 months of battling a novel coronavirus disease (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the global pandemic seems to be far from over, and many countries are still struggling to curb infection rates. This is despite the rapid development of several currently available vaccines and the ongoing development of numerous treatments. Current COVID-19 statistics from the World Health Organization indicate that as of 17 November 2021, more than 253 million cases have been confirmed and more than 5.1 million have died worldwide. 1 In Mexico, there have been over 3.84 million cases, of which 291,147 patients have died (including 977,911 cases and 40,024 deaths in Mexico City). 2 As the pandemic evolves, a new patient category has emerged among seemingly recovered COVID-19 patients. These patients continue to present some symptoms and may even develop new symptoms past the acute stage (4 weeks) of the infection. The persistent or recurring symptomatology is referred to as post-acute COVID-19 (‘long COVID’) and even patients with relatively mild disease can be affected.3,4 Therefore, it is important to view COVID-19 as more than just an acute disease.
Evidence is growing regarding the long-term effects of COVID-19 on patients’ health; however, evidence regarding the prevalence and pattern of symptoms related to the long-term health consequences of COVID-19 is primarily based on surveys. In some preliminary reports, it has been shown that 8 weeks after diagnosis, the proportion of patients with one or more persistent COVID-19 symptoms ranged from 66% to 87%.5–7 The symptoms are heterogeneous and include alopecia and other skin conditions (e.g. pernio), 8 fatigue, dyspnea, joint and chest pain, 6 impaired pulmonary function, post-exertional malaise, cognitive dysfunction,9,10 headaches, vertigo, anosmia, 6 sleep difficulties, anxiety, and depression. 11 Reportedly, these long-term symptoms severely affect their quality of life, 6 activities of daily living and work, and in some cases, lead to significant disability. 12
On 6 October 2021, the World Health Organization proposed a clinical case definition of the post COVID-19 condition by Delphi consensus. 13 Data on persisting symptoms are still lacking, and therefore, there is a need for further research and long-term follow-up of patients with long COVID-19 to clarify these long-term effects and guide the development of potential management strategies to alleviate these symptoms and improve the overall health and quality of life of these patients. 14 Thus, it is necessary to promote research that improves our understanding of the pathophysiology and epidemiology of the post-acute phase as well as promote public health strategies and clinical algorithms that ensure equity in the access to these solutions. 15 Therefore, this study aimed to report the prevalence and associated risk factors of long-term health consequences of COVID-19 by symptom clusters in patients discharged from the Temporary COVID-19 Hospital (TCH) in Mexico City.
Methods
Study setting and design
This was an observational, prospective, longitudinal, single-center study. Patients discharged from the TCH at the Citibanamex Convention Center in Mexico City between September 2020 and January 2021 were followed up by physicians with a telephone survey for up to 90 days (telephone numbers were provided by patients on admission). Self-reported clinical symptom data collected via telephone follow-up were analyzed and summarized for 30 and 90 days post-discharge.
As part of routine clinical practice at the TCH, all patients received an oximeter and were trained in its use at discharge from the TCH. All patients discharged from the TCH underwent follow-up by telephone to assess their health status and recovery (see Supplementary Text 1).
The Research Ethics Committee of the Faculty of Medicine of the National Autonomous University of Mexico (FM/DI/094/2020) approved the study. This study also adhered to the Declaration of Helsinki, as well as local laws and regulations. All patients provided verbal informed consent before participation in the survey.
Patients
Male or female patients aged ⩾18 years, admitted to the TCH, with a confirmed diagnosis of COVID-19 by polymerase chain reaction (PCR); treated, discharged, and considered to be recovered from COVID-19, who were followed up for at least 90 days since discharge from the TCH; and who had answered at least three follow-up calls were included in this study.
Excluded patients were those who died in the hospital, had a severe underlying disease, had no telephone, denied participation in the follow-up, were unable to respond to the questionnaire, provide the necessary detailed information, or perform the required measurements (i.e. oximetry or temperature), and women who were pregnant or breastfeeding.
Outcomes
The main outcomes were the prevalence of the most frequently reported symptoms, by symptom clusters, that persisted or developed anew at 30 and 90 days post-discharge; the associations of symptoms at 30 and 90 days post-discharge by sex, comorbidities (diabetes, hypertension, and obesity), biomarkers, and treatment during hospitalization; and risk factors for the persistence of the most frequent symptoms at 30 and 90 days post-discharge.
Follow-up and data collection
Ten follow-up calls were made to each patient during the 90-day follow-up period. Follow-up telephone calls were systematically distributed throughout the follow-up period as follows: days 1, 3, 7, 14, 21, 30, 45, 60, 75, and 90 after discharge.
During the ongoing telephone call, each patient was asked to measure their oxygen saturation and body temperature during the first 21 days post-discharge. This follow-up period of 21 days was designed to provide rapid access to remote assistance if necessary. In addition, patients were asked to complete a questionnaire related to persistent COVID-19 symptoms.
The questions asked included the following: presence or absence of 45 clinical symptoms; the clinical course of reported symptoms; current health status compared with pre-COVID health status; presence of any breathing difficulties overall, at rest, or during physical exertion; and whether patients were receiving any type of pulmonary rehabilitation. Data were captured using RedCap (https://www.project-redcap.org/).
Demographic and clinical background, clinical course during the acute illness, and relevant laboratory data were obtained from the electronic medical records of the TCH digital health platform.
Statistical analysis
Owing to the nature of the study, sample size calculations were not performed. Efforts to minimize bias consisted of training physicians (n = 15) before conducting the follow-up questionnaire to minimize information bias and adjusting for confounders in our multivariable analyses. The training of physicians included a 10-day induction course, which involved an induction on COVID-19-related topics as well as learning and practicing the call dialogue. Physicians were also monitored at the start to ensure the process was followed appropriately.
Descriptive statistics were used, with n (%) for categorical variables and mean ± standard deviation or median (interquartile range (IQR)) for continuous variables. For comparisons between groups, chi-square or Fisher’s exact test were used. The groups for comparison were (1) patients who reported a specific symptom versus those who did not and (2) males versus females.
Bivariate analysis was used to identify the characteristics associated with a specific symptom. To identify risk factors associated with persistence of COVID-19 symptoms, adjusted multiple logistic regression models were used to estimate the odds ratios (ORs) and 95% confidence intervals (CIs) for the association between factors including sex, age, education level, treatment with steroids, comorbidities, biomarkers, need of high-flow nasal cannula (HFNC) or invasive mechanical ventilation (IMV), and occurrence of persistent symptoms.
A p value < 0.05 indicated statistical significance, and all tests were two-sided. The statistical software used for statistical analyses was STATA, version 15 (Stata Corp., College Station, TX, USA) and R 1.3.1073.
Results
Patients
By January 2021, a total of 5000 patients had been admitted to the TCH, of which 4884 had been discharged. Of these, 4670 patients who agreed to participate in the follow-up survey and met the inclusion criteria were followed up by telephone. In total, 21,553 follow-up calls were performed between September 2020 and January 2021. The number of responders declined progressively with 3914 responses on day 1, 1303 responses on day 30, and 928 responses on day 90.
The main demographic characteristics of patients are shown in Table 1. Patients had a median (IQR) age of 48 (37–58) years, 50.5% were female, 21.2% had type-2 diabetes, 23.1% had hypertension, 38.7% were overweight, and 37.5% were obese.
Characteristics of patients enrolled in this study.

BMI, body mass index; IQR, interquartile range.
Over 75% of patients met the criteria for the green NEWS score category at admission (Table 2). During hospitalization, 15.2% required HFNC, and only 4.6% of patients were admitted to the intensive care unit (ICU). The median (IQR) hospitalization stay was 8 (6–12) days, and 99.4% of patients were discharged from the hospital. While over 80% of patients maintained normal hemoglobin levels during hospitalization, 13.2% had increased D-dimer levels (>1500 ng/mL), 31.2% had increased levels (336.2 ug/L) of ferritin, 30.7% had high levels (>233 U/L) of lactic dehydrogenase, and 31.6% had a low absolute lymphocyte count (<1000 × 103 cells/μL; Table 2).
Frequency of symptoms and main clinical conditions at admission.

CALL, comorbidity, age, lymphocyte count, and lactate dehydrogenase; ICU, intensive care unit; NEWS, National Early Warning Score.
Data are presented as median (interquartile range) unless otherwise stated.
Data on pulse oximetry from patients who did not require oxygen at discharge were available for the first 21 days. Of note, the median oxygen saturation was 94%, and the mean saturation remained similar throughout the 21 days (93.6% on day 1% to 94.1% on day 21). Saturation remained below 90% in 2.6% (56) of patients. Temperature measurements yielded a median temperature of 36.2°C, and the mean temperature remained mostly unchanged for 21 days.
Symptoms
We identified 45 symptoms attributed to COVID-19 and classified them into eight body system clusters (neurological; mood disorders; systemic; respiratory; musculoskeletal; ear, nose, and throat; dermatological; and gastrointestinal) (see Supplementary Figure 1 online).
The change in symptoms over time is shown in Figure 1(a). The symptoms with a significant decrease in frequency from day 30 to day 90 were fatigue (difference in frequencies: −9.5%, p < 0.0001), cough (−7.1%, p < 0.0001), chest pain (−4.9%, p < 0.0001), tremors (−3.8%; p < 0.0001), muscle pain (−3.2%; p = 0.01), sore throat (−3.6%; p = 0.03), dizziness (−2.8%; p = 0.04), and diminished exercise capacity (−2.5%; p = 0.04). Most symptoms tended to decrease in frequency between day 30 and day 90, except for alopecia (difference in frequencies: +12.6%, p < 0.00001), rhinorrhea (+1.8%, p = 0.25), lacrimation (+1.2%, p = 0.71), lack of concentration (+0.79%, p = 0.41), paresthesia (+0.78%, p = 0.56), arthralgia (+0.61%, p = 0.54), and memory loss (+0.49%, p = 0.53), all of which showed increases in frequency over that period. Headache and insomnia were the most common neurological complaints, while sadness, desire to cry, anguish, anger, and anhedonia were the most common complaints in the mood disorder cluster (Figure 1(b) and (c)). Fatigue, cough, back pain, throat pain, hair loss, nausea, and diarrhea were the other major complaints in the remaining clusters.

Frequently reported symptoms and symptom changes over time (a) frequency of symptoms by cluster after 30 days post-discharge (b), and frequency of symptoms by cluster after 90 days post-discharge (c).
Significant differences in the frequency of all symptom clusters were observed between 90 and 30 days post-discharge (Figure 2). At 90 days post-discharge, there were slight decreases in the frequency of symptoms across all clusters, except for the dermatological symptom cluster, in which the frequency of symptoms had significantly increased from 22.4% to 33.5% (p < 0.0001). However, persistent symptoms were still markedly high in the neurological, mood disorder, systemic, musculoskeletal, and ear, nose, and throat symptom clusters. At 30 days post-discharge, the proportions of patients with and without symptoms were 76.2% and 23.8%, respectively, while at 90 days the proportions of patients with and without symptoms were 68.0% and 32.0%, respectively. Furthermore, over 16% and 22% of patients still had at least one symptom after 30 and 90 days, respectively.

Persistence of symptoms by symptom cluster over time.
When comparing symptom persistence in patients who had or had not undergone IMV, the use of IMV increased the frequency of symptoms by over 13% at 30 days post-discharge (75.5% (936/1239) and 88.7% (55/62); however, this was non-significant (p = 0.31). The difference in the proportion of patients with persistent symptoms at 90 days among those who underwent IMV and those who did not was also non-significant (69.2% (612/884) and 68.9% (31/45) p = 0.27). By symptom cluster, the majority of complaints of patients who underwent IMV at 30 days were in the neurological, systemic, mood disorder, and respiratory clusters (Figure 3). Although neurological symptoms remained the most frequent at 90 days, there was a shift to dermatological symptoms as the second-most frequent symptom cluster. Furthermore, at 90 days, the trend in frequency across symptom clusters resembled that of patients who did not undergo IMV.

Persistence of symptom clusters stratified by patients who underwent IMV versus no IMV at 30 and 90 days post-discharge.
We also compared the frequency of symptoms by sex (Figure 4). Of note, in both women and men, the frequencies of symptoms such as alopecia, joint pain, paresthesia, lack of concentration, rhinorrhea, and memory loss were higher at 90 days than at 30 days post-discharge. Women seemed to be more affected than men for most of these symptoms, particularly alopecia. At 90 days, the frequency of dermatological symptoms in women was 45.9%, compared with 21.2% in men.
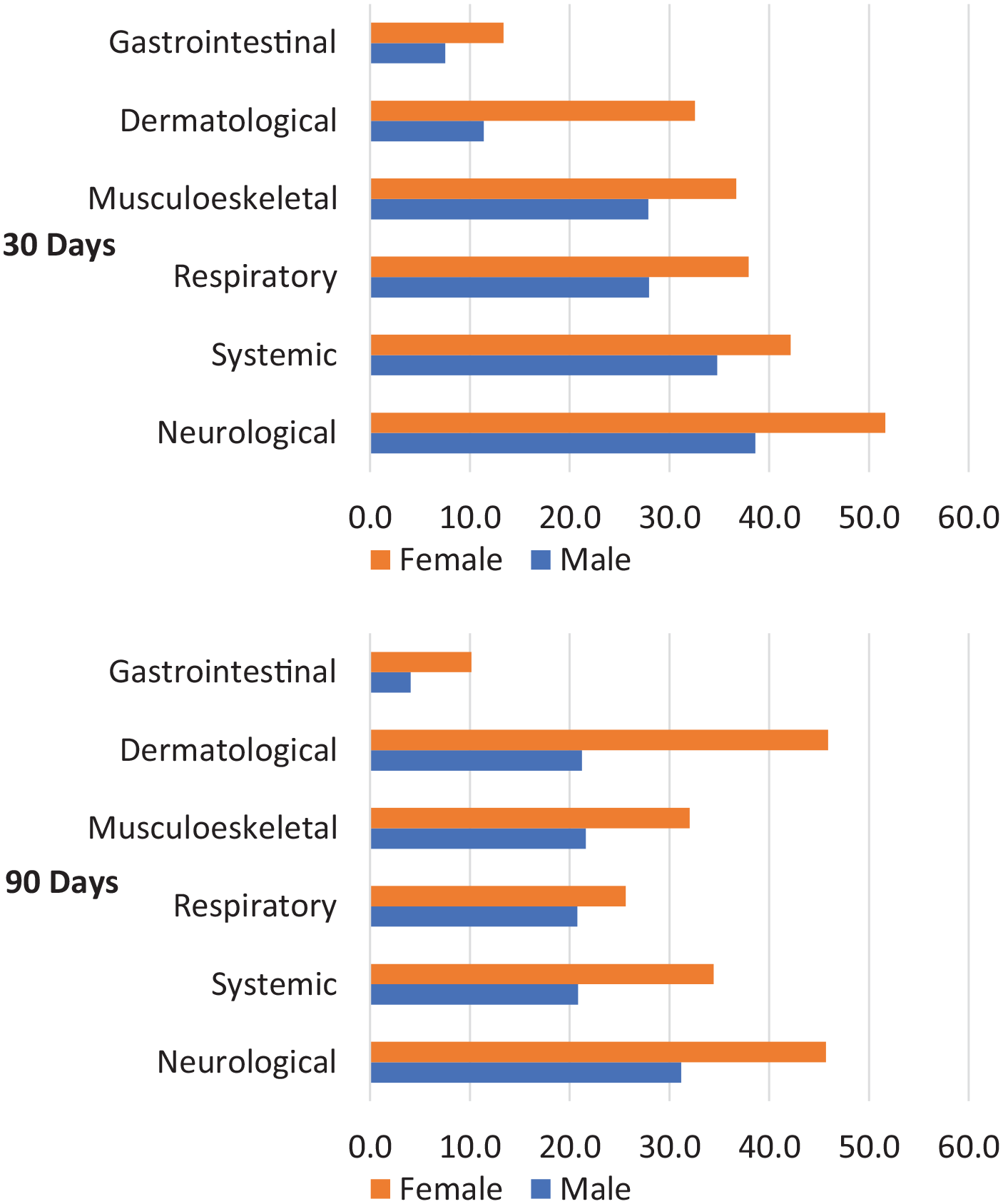
Persistence of symptom clusters stratified by sex at 30 and 90 days post-discharge.
Multiple logistic regression models
Table 3 and Supplementary Figure 2a−d show the multiple logistic regression analyses for relevant background factors and symptom clusters. After 30 and 90 days, significant associations were observed with male patients compared with female patients, including a lower risk shown for neurological (OR: 0.59 (95% CI 0.43−0.81), p < 0.01% and 0.38 (95% CI 0.24−0.62), p < 0.001, respectively), mood disorder (OR: 0.57 (95% CI 0.41−0.78), p < 0.001% and 0.42 (95% CI 0.25−0.70), p < 0.001, respectively), musculoskeletal (OR: 0.59 (95% CI 0.42−0.82), p < 0.01% and 0.50 (95% CI 0.30−0.84), p < 0.01, respectively), and dermatological (0.27 (95% CI 0.18−0.41), p < 0.001% and 0.27 (95% CI 0.16−0.45), p < 0.001, respectively) symptoms. Compared with the male sex, female sex was also associated with a lower risk of presenting with respiratory symptoms at 30 days and systemic symptoms at 90 days.
Results of bivariate and multivariate analysis.

HFNC, high-flow nasal cannula; IMV, invasive mechanical ventilation; LDH, lactate dehydrogenase.
Red cells indicate a higher association. Green cells indicate a lower association.
p < 0.05, **p < 0.01, ***p < 0.001
Compared with normal weight, obesity was significantly associated with respiratory symptoms, and HFNC use versus no use during hospitalization was associated with musculoskeletal and dermatological symptom clusters at 30 days post-discharge. Dexamethasone treatment versus no dexamethasone use was significantly associated with respiratory, musculoskeletal, and dermatological symptom clusters at 30 days post-discharge. Compared with normal levels, elevated D-dimer levels were associated with ear, nose, and throat symptoms at 30 days post-discharge and with respiratory, musculoskeletal, and dermatological symptom clusters at 90 days post-discharge. Significant associations were noted between 1-day increases in hospital stay duration and neurological (30 days post-discharge) and respiratory symptom clusters (30 and 90 days post-discharge).
Discussion
This longitudinal, prospective, observational, single-center study analyzed the most frequent symptoms that persisted in patients with COVID-19 at 30 and 90 days post-discharge from the TCH in Mexico City. Notably, 76.2% had at least one of the 45 identified COVID-19 symptoms at 30 days post-discharge, with 68.0% of patients having at least one of these symptoms persist to 90 days post-discharge. When grouped in clusters by body systems, we identified eight symptom clusters. Among these, the most relevant symptom clusters that persisted in >30% of patients at 90 days post-discharge were the neurological, dermatological, and mood disorder symptom clusters. The changes in symptom cluster frequency over time indicate that COVID-19 is not only a viral disease with an acute phase, but that it can develop into a chronic condition with long-term consequences that are frequent and disabling. Some moderate associations were also observed between long-COVID symptom clusters and obesity, dexamethasone use, increased D-dimer levels, and hospital stay duration. Although the early symptoms of COVID-19 have been amply characterized, further evidence of long or post COVID-19 is needed to offer these patients the appropriate clinical management, rehabilitation, and support via public health strategies after the acute phase of the disease.
The present proportions of patients reporting long-term symptoms are similar to those reported in a cohort of patients discharged from a temporary hospital in Wuhan. 11 In that cohort, 76% of patients discharged from that hospital had at least one symptom at the 6-month follow-up. Meanwhile, an Italian post-acute outpatient service reported that 87.4% of patients had at least one persistent symptom at 60 days. 6 In contrast, we report a higher incidence than what was reported in a single-center study in Wuhan at 3 months after discharge, in which 49.6% had at least one general symptom after discharge. 16 Furthermore, a multicenter study in Michigan, USA, showed that persistent symptoms remained in 32.6% of patients 60 days after discharge when using a telephone survey. 17
Previous coronavirus epidemics, namely SARS and Middle East respiratory syndrome (MERS), have also resulted in long-term sequelae, 18 including fatigue, shortness of breath, myalgia, depression, alopecia, insomnia, and mental disorders such as anxiety and post-traumatic stress disorder that lasted from 3 months to over 1 year after the acute illness. During the current pandemic, concerns were raised early on that this could happen with COVID-19. 19 Recently, a large retrospective database study followed 236 379 patients for 6 months after a COVID-19 diagnosis and compared symptoms against patients who had influenza or a respiratory tract infection during the same period. 20 They reported that the presence of COVID-19 was significantly associated with neurological and psychiatric symptoms with an estimated incidence of 33.62% at 6 months. The neurological and psychiatric consequences of COVID-19 that were identified in that study included ischemic stroke, intracranial hemorrhage, psychotic disorders, anxiety and mood disorders, insomnia, and substance use disorders. These symptoms, which we also identified in our study, are usually chronic or recurring conditions that may persist beyond 3 and 6 months, and as such add further support to the notion of the chronicity of COVID-19.
The 10 most frequent individual symptoms at 30 and 90 days post-discharge were fatigue, headache, sadness, alopecia, insomnia, desire to cry, anguish, anger, anhedonia, and back pain, which are similar to those described in previous reports.6,12,16,21 Most recently, a study on the attributes and predictors of long COVID-19 also reported similar individual symptoms (i.e. fatigue, headache, dyspnea, and anosmia) that persisted for 12 weeks. 4 Although symptoms like fatigue, cough, and chest pain decreased over time in our study, patients who were discharged from the TCH reported higher frequencies of alopecia, rhinorrhea, lacrimation, lack of concentration, paresthesia, arthralgia, and memory loss at 90 days compared with 30 days.
Of note, dermatological manifestations such as alopecia have been reported in approximately 20% of patients 11 and Xiong et al. 16 discuss in their paper that alopecia may be a distinctive long-term feature of COVID-19 survivors and that it almost exclusively affected women. We also found that alopecia increased over time that it mainly affected women, and at 90 days, the proportion of women who suffered alopecia was double that of men. Possible reasons for alopecia in women include inflammation and immunity22,23 and a possible association with emotional distress, 24 which seems plausible given the high proportion of patients in our population who reported sadness and anxiety. These findings indicate that healthcare systems must develop strategies to provide mental health support to COVID-19 survivors with persistent symptoms. 25
In this study, women reported having persistent COVID-19 symptoms more often than men, which is consistent with the reports of two previous single-center cohort studies at COVID-19 hospitals in Wuhan, 11 and a 12-week follow-up study in the United Kingdom. 4 Furthermore, the association between female sex and long-COVID-19 symptoms was clearly observed across several symptom clusters, including the neurological, mood disorder, musculoskeletal, and dermatological clusters. Of the biomarkers evaluated, increased D-dimer levels (>1000 or 1500 U/L) were significantly associated with ear, nose, and throat, respiratory, musculoskeletal, and dermatological symptom clusters. More recently, D-dimer levels were also shown to be elevated (>500 ng/mL) for up to 4 months post-infection in more than 25% of patients. 26 These elevations contrasted with other coagulation and inflammatory markers, which had all returned to normal levels across more than 90% of patients.
In contrast with the cohort study by Huang et al. 11 in China, where the presence of persisting symptoms was linked with the severity of the initial COVID-19 illness, we found that patients tended to present long-term health consequences of COVID-19 regardless of their initial disease severity. However, we cannot rule out selection bias as the TCH admitted many patients with mild or moderate disease. When we compared symptom persistence between patients who had undergone IMV versus those who did not, IMV increased the frequency of long-COVID-19 symptoms by 13% at 30 days post-discharge. Interestingly, at 90 days post-discharge, the frequency of symptoms was similar to those of patients who did not receive IMV. Our findings are also broadly aligned with a recent study focusing on persistent neurological symptoms at 6 months. The incidences and risk of presenting such persistent symptoms were greater, but not limited to patients who were hospitalized. Of note, in that study, these outcomes were even more marked among patients who had required intensive care or had developed encephalopathy during their hospital stay. 20
Some studies have suggested that post-COVID-19 symptoms resemble fibromyalgia, post-viral fatigue syndrome, or chronic fatigue viral syndrome.27–30 Of note, a recent web-based cross-sectional survey identified that 30.7% of patients met the criteria for fibromyalgia 6 months after their COVID-19 diagnosis and that obesity and male gender were the strongest risk factors. 28 However, further research is needed to clarify the underlying pathophysiology of long COVID-19 and whether applying similar clinical management strategies would be beneficial.
This study’s main limitation was that many patients were lost to follow-up by the end of the observation period. In addition, the results depended on a self-reported questionnaire. Patient responses may have been subject to recall bias, which could have affected the accuracy of the information obtained by the telephone follow-up. Furthermore, patients did not undergo a physical examination or in-person interview during follow-up to validate their responses. However, the electronic medical records at the TCH were considered a reliable source of data.
Conclusion
In conclusion, a large proportion of patients who experienced COVID-19 and who were discharged from the hospital presented long-term health consequences of COVID-19 at 30 and 90 days post-discharge. Our observations suggest that COVID-19 is a chronic illness that affects several organs and systems and that the presence of these persisting symptoms is not limited by the severity of the initial COVID-19 disease. We propose that the management and rehabilitation of COVID-19 patients should include strategies that include neurological, mood disorder, and dermatological symptoms.
As a consensus has yet to be reached regarding the pathophysiology, characteristics, evolution, and treatment for this post-viral syndrome, the present findings are intended to expand on the presently available data and aid the development of appropriate and multidisciplinary strategies to manage symptoms and promote physical, mental, and emotional recovery. However, long-term studies are needed to clarify any association among COVID-19 symptoms, prolonged hospital stay, disease severity, and hospitalization stressors.
Supplemental Material
sj-docx-2-tai-10.1177_20499361211069264 – Supplemental material for Symptom cluster analysis of long COVID-19 in patients discharged from the Temporary COVID-19 Hospital in Mexico City
Supplemental material, sj-docx-2-tai-10.1177_20499361211069264 for Symptom cluster analysis of long COVID-19 in patients discharged from the Temporary COVID-19 Hospital in Mexico City by Rosa María Wong-Chew, Edwin Xchel Rodríguez Cabrera, Carlos Alberto Rodríguez Valdez, Julieta Lomelin-Gascon, Linda Morales-Juárez, Mariana Lizbeth Rodríguez de la Cerda, Antonio Rafael Villa-Romero, Stephanie Arce Fernández, Mariana Serratos Fernandez, Héctor Herrera Bello, Lidia Moreno Castañeda, Mónica Arboleya Avendaño, Jesús Abraham Hernández-Cruz, Nelson Álvarez Martínez, Liza Fernanda Contreras, Luis Rafael González de la Cerda, Arturo Juárez Flores, Luis Alberto Martínez-Juarez, Diego-Abelardo Álvarez-Hernández, Héctor Gallardo-Rincón, German Fajardo Dolci, Roberto Tapia-Conyer and Rafael Ricardo Valdez-Vázquez in Therapeutic Advances in Infectious Disease
Supplemental Material
sj-pptx-1-tai-10.1177_20499361211069264 – Supplemental material for Symptom cluster analysis of long COVID-19 in patients discharged from the Temporary COVID-19 Hospital in Mexico City
Supplemental material, sj-pptx-1-tai-10.1177_20499361211069264 for Symptom cluster analysis of long COVID-19 in patients discharged from the Temporary COVID-19 Hospital in Mexico City by Rosa María Wong-Chew, Edwin Xchel Rodríguez Cabrera, Carlos Alberto Rodríguez Valdez, Julieta Lomelin-Gascon, Linda Morales-Juárez, Mariana Lizbeth Rodríguez de la Cerda, Antonio Rafael Villa-Romero, Stephanie Arce Fernández, Mariana Serratos Fernandez, Héctor Herrera Bello, Lidia Moreno Castañeda, Mónica Arboleya Avendaño, Jesús Abraham Hernández-Cruz, Nelson Álvarez Martínez, Liza Fernanda Contreras, Luis Rafael González de la Cerda, Arturo Juárez Flores, Luis Alberto Martínez-Juarez, Diego-Abelardo Álvarez-Hernández, Héctor Gallardo-Rincón, German Fajardo Dolci, Roberto Tapia-Conyer and Rafael Ricardo Valdez-Vázquez in Therapeutic Advances in Infectious Disease
Footnotes
Acknowledgements
Author contributions
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The Carlos Slim Foundation funded this study. The funding source was involved in the design of the study, analysis, interpretation of data, and in writing the manuscript. R.R.V.V., E.X.R.C., C.A.R.V., M.L.R.C., S.A.F., M.S.F., H.H.B., L.M.C., M.A.A., J.A.H.C., N.A.M., L.F.C., L.R.G.C., and A.J.F. are employees of the Temporary COVID-19 Hospital. J.L.G., L.M.J., L.A.M.J., D-A.A-H., H.G-R., and R.T-C. are employees of The Carlos Slim Foundation. All authors confirm that they had full access to all the study data and accept responsibility to submit for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Carlos Slim Foundation funded this study. The funding source was involved in the design of the study, analysis, interpretation of data, and in writing the manuscript.
Availability of supporting data
The data that support the findings of this study will be made available upon reasonable request to the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.