
Abstract
Objectives:
This study aims to estimate the prevalence of sinus tachycardia in hospitalized patients with mild COVID-19 infection and to identify the clinical, radiological, and biological characteristics associated with sinus tachycardia.
Methods:
A retrospective cohort study was conducted on patients with mild COVID-19 infection and sinus tachycardia during hospitalization. Outcomes measured included incidences of venous thromboembolism, high-dependency/intensive care unit admission, laboratory parameters, and radiological findings.
Results:
A total of 236 COVID-19 positive patients admitted to Singapore General Hospital isolation general wards from 1 June 2020 to 30 June 2020 were included in this study. Ninety-seven (41.1%) patients had sinus tachycardia on or during their admission. All patients were monitored in general wards and discharged to community quarantine facilities. None required oxygen support or high-dependency/intensive care unit admission. Sinus tachycardia was associated with increased C-reactive protein level (odds ratio = 1.033, 95% confidence interval = 1.002–1.066), abnormal chest X-ray findings (odds ratio = 3.142, 95% confidence interval = 1.390–7.104), and longer hospitalization (odds ratio = 1.117, 95% confidence interval = 1.010–1.236). There was no significant statistical association between sinus tachycardia and incidences of venous thromboembolism.
Conclusion:
This study suggests that patients with mild COVID-19 infection and concurrent sinus tachycardia are more likely to have higher inflammatory marker levels, abnormal imaging, and prolonged hospitalization. However, no significant association between sinus tachycardia and thromboembolism is identified in mild COVID-19 infection.
Introduction
The Coronavirus disease of 2019 (COVID-19) caused by severe acquired respiratory syndrome coronavirus-2 is a global health emergency, characterized by various grades of lung damage and acute respiratory distress syndrome. Although a majority of COVID-19 mortality and morbidity are caused by pulmonary injury, cardiovascular manifestations and complications have also been extensively reported in COVID-19 patients.1–3
Sinus tachycardia is the most common type of cardiac arrhythmia because it may be either pathogenic or a normal physiological response to emotional or physical stimulation. Possible causes of sinus tachycardia in patients with COVID-19 infection are numerous, ranging from impaired pulmonary function, venous thromboembolism (VTE), myocardial injury, thyroid dysfunction, anemia, autonomic dysfunction, and anxiety state.4,5 Clinical observations have found sinus tachycardia to be the most common cardiac arrhythmia reported in COVID-19 pandemic.6–8 However, despite the increased prevalence of sinus tachycardia among COVID-19 patients, the medical implications and underlying causes have not been well-addressed in current literature.
Among the possible causes of sinus tachycardia, VTE is reported frequently early in the COVID-19 pandemic, initially focusing on the critically ill patients, followed by similar studies in non-critically ill patients.9–16 The increased thrombotic risk in COVID-19 patients have led to both the American Society of Hematology and International Society on Thrombosis and Hemostasis recommending VTE thromboprophylaxis in all hospitalized patients regardless of the severity of COVID-19 disease.17,18 While the earlier reports have shown significantly increased incidences of VTE in COVID-19 patients, emerging studies demonstrate the opposite clinical observations, finding no significant differences between thrombotic risk in COVID-19 patients and non-COVID-19 patients, especially among patients with milder COVID-19 infection and with less comorbidities. 19
In this study, we aim to investigate the prevalence of sinus tachycardia in patients with mild COVID-19 infection and to identify the clinical, radiological, or biological characteristics associated with sinus tachycardia, to better understand and optimize management for this patient population.
Methods
Study design
We conducted a single-center retrospective cohort study on 236 adult patients with confirmed COVID-19 infection in Singapore General Hospital, a 1700-bedded tertiary academic medical center. The ethics review for this study was waived by the SingHealth Institutional Review Board (IRB reference # 2020-2710).
Patient population and data collection
We identified 238 COVID-19 patients consecutively admitted to Singapore General Hospital isolation general wards from 1 June 2020 to 30 June 2020. At the time of study, all COVID-19 patients in Singapore, regardless of disease severity, were required by the Singapore Ministry of Health to be admitted to tertiary hospitals for medical assessment and triage, prior to transfer to community quarantine facilities. Inclusion criteria were as follows: patients who had positive COVID-19 reverse transcription polymerase chain reaction (RT-PCR) test results on a nasopharyngeal or oropharyngeal swab or positive serology for severe acquired respiratory syndrome coronavirus-2, patient who were more than 18 years of age, and patients who did not have known chronic illnesses. Patients were excluded from this study if they fulfill any of the following: (1) patients who were admitted for more than once during the study period, (2) patients who were transferred out from High Dependency (HD) or Intensive Care Unit (ICU), (3) patient who required oxygen therapy, and (4) patient who presented with significant abnormal electrocardiogram (ECG) changes indicating myocardial ischemia, high-grade atrioventricular blocks or non-sinus cardiac arrhythmia. Patients were defined to have mild COVID-19 infection if they did not require oxygen support nor HD/ICU care and were able to perform activities of daily living independently during admission. A total of 236 patients were included in this study.
The patients were further categorized based on their maximum heart rate (max. HR) into two groups. Tachycardia was defined as a heart rate >100 beats/minute (bpm) in accordance with the American Heart Association and Advanced Cardiac Life Support guidelines.20,21 Patient with max. HR more than 100 bpm during admission were classified into tachycardia cohort and patients with max. HR less than 100 bpm were classified into non-tachycardia cohort (control cohort). All ECGs performed in the ward were viewable on the hospital’s electronic health record system (Allscripts Sunrise™) and were reviewed to ensure each patient’s eligibility in this study. Data points were manually collected and coded for each patient.
Hospital course, treatments, and outcome
The main outcomes for this study were development of VTE (inclusive of both deep vein thrombosis and pulmonary embolism) during hospitalization, hypotension, oxygen therapy requirement, HD/ICU admission, length of stay (LOS), and inpatient mortality.
Blood pressure, heart rate (HR) and oxygen saturation (SpO2) were measured at least every 4 h during hospitalization, to detect tachycardia, desaturation to SpO2 <95% which will trigger initiation of oxygen therapy, and hypotension. Hypotension was defined as systolic blood pressure <90 mm Hg and/or diastolic blood pressure <60 mm Hg.
Demographic data collected included age and gender. In addition, routine laboratory and radiological data were reviewed and collected. Routine investigations performed for all patients admitted included a full blood count (FBC, inclusive of hematocrit, and absolute lymphocyte count), renal panel (RP, inclusive of urea), lactate dehydrogenase (LDH), C-reactive protein (CRP), and chest X-ray (CXR). Other investigations such as free T4 (fT4), thyroid-stimulating hormone (TSH), D-dimer, venous duplex ultrasound of the lower limb (US LL), transthoracic echocardiogram (TTE), and computed tomography pulmonary angiogram (CT PA) were performed at primary physician’s discretion, directed by patients’ clinical condition. All patients included in the study had a documented discharge status (inpatient mortality vs discharged) at the time of data collection.
Statistical analyses
Categorical variables were described as frequency and percentages. Continuous variables were expressed in mean values and standard deviations (SD) if they were normally distributed or median and interquartile range (IQR) if they were not. For comparison between cohorts, Pearson’s χ2 test and Fisher’s exact test were used for categorical variables, while Student’s t-test and binary logistic regression were used for continuous variable. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated to evaluate the strength of association. All statistical tests were two-tailed, and p < 0.05 was considered statistically significant. Statistical analyses were completed using IBM SPSS Statistics software (version 26).
Results
Patient population and baseline characteristics
This study included 236 patients admitted to Singapore General Hospital isolation general wards with positive COVID-19 PCR swab test and/or COVID-19 IgM serology from 1 June 2020 to 30 June 2020. Out of the 236 patients, 235 were males (99%) and 1 was female (1%). The mean age of patients was 44.6 years (SD = 7.64). The median LOS was 5.43 days (IQR = 3–6). Majority of these patients were dormitory-dwelling migrant workers admitted for medical assessment before transferring to community quarantine facilities (Table 1).
Demographics, baseline characteristics, and clinical outcomes of study participants.

SD: standard deviation; IQR: interquartile range; LOS: length of stay; HR: heart rate; LDH: lactate dehydrogenase; CRP: C-reactive protein; Hct: hematocrit; L. Abs: absolute lymphocyte count; fT4: free T4; TSH: thyroid-stimulating hormone.
Sinus tachycardia was detected in 97 patients (41%). None of the patients developed new VTE, or hypotension, required oxygen support, or required admission to HD/ICU during their hospitalization. All the patients were admitted directly to general wards and were discharged to community quarantine facilities. Suitability for discharge to community quarantine facilities was dependent on patient’s COVID-19 disease severity and symptoms, day of illness, age, presence of concurrent acute medical conditions, and bed availability at community quarantine facilities. There was no mortality during admission.
Comparison between patients with versus without sinus tachycardia
Sinus tachycardia correlated to prolonged LOS (OR = 1.117; 95% CI = 1.010–1.236; p = 0.002). Mean max. HR was greater in patients with sinus tachycardia by 21 bpm, and the mean difference of mean HR was 12 bpm higher in the sinus tachycardia group. No correlation was found between sinus tachycardia and age (Table 2).
Demographics and baseline characteristics of sinus tachycardia versus control cohorts.

OR: odds ratio; 95% CI: 95% confidence interval; SD: standard deviation; IQR: interquartile range; LOS: length of stay; HR: heart rate.
Comparison between laboratory parameters
Sinus tachycardia was associated with increased CRP level (OR = 1.033; 95% CI = 1.002–1.066; p = 0.002). No correlation between sinus tachycardia and LDH, urea, hematocrit, absolute lymphocyte count, fT4, TSH, and D-dimer levels were found (Table 3). None of the thyroid function tests were suggestive of thyrotoxicosis. All D-dimer values were <0.50 in both groups.
Laboratory parameters of sinus tachycardia versus control cohorts.

OR: odds ratio; 95% CI: 95% confidence interval; SD: standard deviation; LDH: lactate dehydrogenase; CRP: C-reactive protein; Hct: hematocrit; L. Abs: absolute lymphocyte count; fT4: free T4; TSH: thyroid-stimulating hormone.
Comparison between radiological findings
All patients had a CXR performed during hospitalization. Sinus tachycardia in patients was associated with abnormal CXR findings, defined as consolidation changes (OR = 3.142; 95% CI = 1.390–7.104; p = 0.008). Neither US LL nor TTE was performed in this study. Only one CT PA was performed in the sinus tachycardia cohort, which was negative for pulmonary embolism (Table 4).
Radiological finding of sinus tachycardia versus control cohorts.
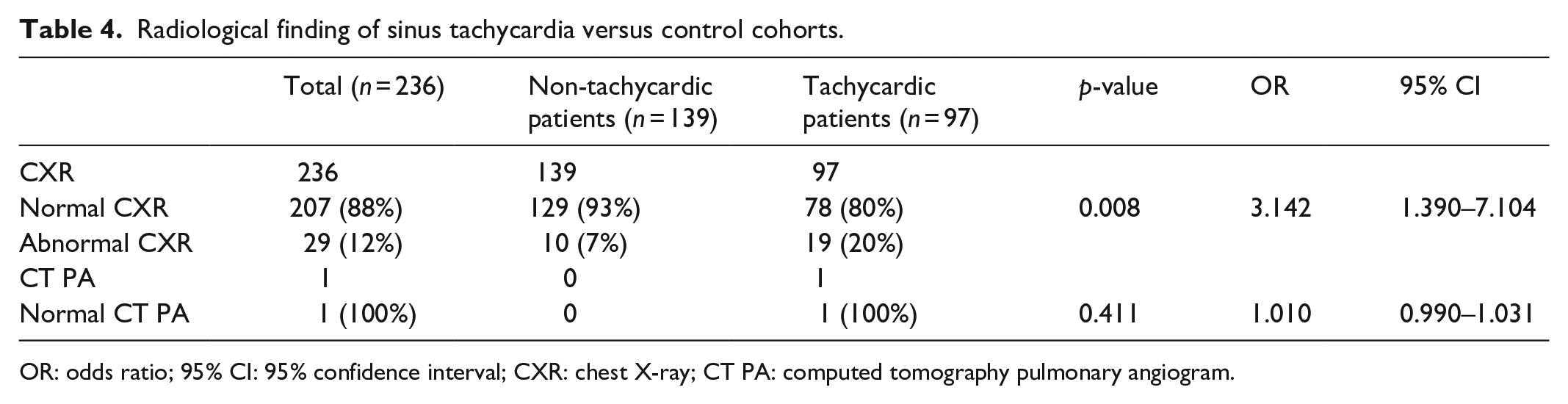
OR: odds ratio; 95% CI: 95% confidence interval; CXR: chest X-ray; CT PA: computed tomography pulmonary angiogram.
Discussion
A variety of cardiac arrhythmias and ECG abnormalities have been observed in patients with COVID-19 infection and sinus tachycardia is reported as the most common ECG finding in COVID-19 patients in several studies.22–24 Sinus tachycardia in febrile viral illness is known to be caused by multiple factors, including fever, hypoxia, hypotension, anemia, inflammatory response, and anxiety. Many other mechanisms may also explain a persistent elevated heart rate and blood pressure in COVID-19 patients, such as activation of the renin–angiotensin–aldosterone system and sympathetic system, endothelial dysfunction, vasculitis, ischemia, hyperreninemia secondary to volume overload and intravenous saline use, vasopressors use, and mechanical ventilation.25,26
This retrospective study explored the significance of sinus tachycardia on the clinical course of patients with mild COVID-19 infection, who did not require oxygen support or HD/ICU admission. Cohort analysis of sinus tachycardia demonstrated statistical significance for sinus tachycardia to increased CRP, abnormal CXR findings and prolonged hospitalization. Both raised CRP and abnormal CXR were associated with clinical deterioration and worse outcomes in COVID-19 patients, implying that sinus tachycardia may indicate excessive inflammatory stress associated with critical illness.27–29 Overall, our findings suggest that sinus tachycardia may be a significant prognostic factor in patients with mild COVID-19 infection.
However, no significant correlation was established between sinus tachycardia and various laboratory and radiological results, including LDH, urea, hematocrit, absolute lymphocyte count, fT4, TSH, D-dimer levels, and CT PA, to suggest any underlying pathologies. Other studies have also found similar negative association between sinus tachycardia and casual physiological changes. An epidemiological study on COVID-19 patients has concluded that sinus tachycardia is not always correlated to fever and hypoxia in COVID-19 infection. 4 Another observational study of sinus tachycardia in COVID-19 patients with myocardial injury has also demonstrated the acceleration of heart rate is not correlated with raised body temperature. 30
Although our results suggest that sinus tachycardia reflects a longer and possibly more inflammatory clinical course among mild COVID-19 infection, in the absence of significant pulmonary, thyroid, and hematological dysfunction found in this study, we believe that sinus tachycardia in mild COVID-19 infection may be attributable to reversible physiological changes including dehydration and mild inflammatory response and contributed by impaired psychological well-being that have been frequently observed in COVID-19 patients, rather than underlying detrimental complications such as VTE. 31 The investigation and management of this group of patients should focus on enhancing recovery of physical and psychological fitness, selecting non-routine investigations carefully and avoiding premature anticoagulation without clinical evidence of other concomitant underlying illness.
Interestingly, we did not observe any incidences of newly diagnosed VTE in our cohort of patients with mild COVID-19 infection, regardless of their maximum heart rates. This finding is in contrast to the currently estimated 8% incidence of VTE in all COVID-19 patients and up to 69% in critically ill patients.10,12,14,32–34 Other case studies have shown that patients with mild COVID-19 infection are at risk of developing myocardial infarction due to microvascular obstruction by thrombi that can be only detected by cardiac magnetic resonance imagining. 35 These differences in thrombotic event incidence may be accounted for by a few factors specific to this study’s population. The majority of this study population consisted of migrant workers residing in dormitories who were otherwise healthy, ambulant, younger males with less severe infection, compared to the global COVID-19 population, hence reducing their risks for developing thrombotic events. 36 Also, this study excluded patients who presented with significant abnormal ECG changes indicating myocardial ischemia, high-grade atrioventricular blocks, or non-sinus cardiac arrhythmia. In addition, cardiac markers such as troponins and pro-B-type natriuretic peptide (BNP), coagulation studies such as prothrombin time (PT), activated partial thromboplastin time (aPTT) and international normalized ratio (INR), and imaging studies were only performed in symptomatic cases for confirmatory purpose, instead of routine screening for all patients in our cohort. Our protocol on investigations may have decreased the detection rate of thrombotic events in our center; however, zero thrombotic event observed in our cohort of more than 200 hospitalized patients is nonetheless a striking departure from the reported incidences despite our conservative investigation protocol.
Worldwide, anticoagulant treatment has been associated with decreased mortality in patients with severe COVID-19 disease and guidelines have recommended to start anticoagulant at prophylactic dose for all hospitalized COVID-19 patients and at therapeutic dose for all critically ill-hospitalized COVID-19 patients.37,38 While most literature reports a significantly higher rate of thrombotic events in COVID-19 patients, which validate current recommendation for thromboprophylaxis, our results suggest a more prudent approach and careful risk–benefit assessment for the use of anticoagulation in patients with mild COVID-19 infection and no significant comorbid illnesses. Because anticoagulation is not risk-free in any population, the recommendation to thromboprophylaxis all hospitalized COVID-19 patients may not be universally suitable and the recommendation may require further adjustments in different populations, taking the inherent thrombotic risk into account.
We acknowledge that this study has several limitations. First, we have conducted a retrospective, single-center cohort study comprised mostly of otherwise healthy young male dormitory-dwelling migrant workers; therefore, the results may not be widely extrapolatable. Second, we did not perform power analysis on our retrospective cohort sample sizes. Third, this study focused on patients with mild COVID-19 infection, which may not be representative of the hospitalized COVID-19 population globally, although this is likely more representative of the overall COVID-19 population. Finally, investigation for possible thrombotic events was conducted at each physician’s clinical discretion, and no active surveillance on the clinicians’ approach was systematically performed during the study period. Therefore, VTE may be underdiagnosed and more studies with a large sample size and standardized investigations are needed before any conclusive inference can be made in this regard. We believe that further studies of larger scale will provide a better understanding of the possible implications of sinus tachycardia and prevalence of VTE in mild COVID-19 patients.
Conclusion
Recent clinical and epidemiological studies have suggested that sinus tachycardia is frequently seen in COVID-19 patients. However, the exact underlying mechanism is still unclear. In this study, we demonstrate that patients with mild COVID-19 infection and sinus tachycardia are more likely to have elevated CRP level, abnormal CXR findings, and prolonged hospitalization. There are no significant associations between sinus tachycardia and development of thromboembolism in patients with mild COVID-19 infection.
Footnotes
Acknowledgements
The author thank Dr Mei Ling Kang for her encouraging guidance on this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was waived by the SingHealth Institutional Review Board (IRB reference # 2020-2710).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent for this study was waived by the SingHealth Institutional Review Board (IRB reference # 2020-2710).