
Abstract
Background:
Sleepiness during the night shift is associated with errors, accidents, injuries, and drowsy driving. Despite scientific evidence that supports brief naps to reduce sleepiness, and guidance documents from policy organizations, napping has not been widely implemented.
Methods:
An initiative to translate scientific evidence about napping was implemented in one hospital over one year. The initiative included garnering leadership support and resources, building a translation team, evaluating the evidence, responding to operational concerns, developing an implementation strategy, and then implementing and evaluating the results. Night shift nurses were surveyed pre and post nap implementation for drowsy driving, sleepiness, and work and coworker relationships. Qualitative data documented the nurses’ perceptions about napping.
Findings:
Three-fourths of the units that were eligible to nap successfully implemented and sustained napping. Most nurses felt refreshed by a brief nap and felt safer on the drive home, but one-fourth worried about or had sleep inertia symptoms. Drowsy driving remained unacceptably high.
Conclusion:
The initiative was successfully implemented on most nursing units. The mixed reaction to napping, and the unfavorable drowsy driving outcome point to the need for additional interventions to reduce sleepiness.
Keywords
Background
Sleepiness during the night shift is a well-documented phenomenon and is known to be associated with errors, accidents, injuries at work, and drowsy driving on the way home from the night shift (Caruso et al., 2015). In high-quality experimental studies, the evidence supports brief naps to reduce decrements in neurobehavioral functioning and performance, including a reduction in drowsy driving (Ruggiero & Redeker, 2013). Numerous position and policy statements from federal and trade organizations, some from nearly two decades ago, support napping as a fatigue reduction measure (American Nurses Association [ANA], 2014; Caruso et al., 2017; Joint Commission, 2011; Lerman et al., 2012; Page et al., 2004). Yet napping has not been implemented to protect nurses and the patients who they serve in most acute care hospitals.
Prior investigators have reported difficulty implementing napping on patient care units (Edwards et al., 2013; Scott et al., 2007) despite research evidence of reduced sleepiness and fatigue. Translating evidence about napping into one hospital’s practice took more than one year and required a deliberate and systematic approach at multiple levels of the organization where nursing leadership and the nursing staff, committed to follow the evidence, took operational needs into account and evaluated the outcome (Mittman, 2012). The impetus for this initiative was the research finding of a two-hospital implementation study of fatigue risk reduction strategies (Geiger-Brown et al., 2016) where napping was successfully implemented and sustained on one of this hospital’s 14 nursing units and for the air and ground transport team members. There were no adverse events due to napping in the three years where napping was sustained. Subsequently, staff nurses wanted to extend the napping initiative onto other nursing units. The purpose of this initiative was to extend implementation of a brief night shift nap opportunity for nurses hospital-wide. In this quality improvement report, we described quantitative data collected pre- and post-nap implementation for drowsy driving, drowsiness during work, and coworker sleepiness. We also provided analysis of free-form comments about the benefits and drawbacks of the nap experience collected post-implementation.
Methods
The goal of this multiphase quality improvement project was to review the napping literature, assess the need for nap implementation at this hospital, present the evidence to management, receive their decision about moving forward with implementation, implement a napping initiative on nursing units if and once management approved, and assess the results of nap implementation.
Implementation Process
Pre-Implementation Phase
In the pre-implementation phase, a translation team (hereafter, the “team”), comprised largely of night shift staff nurses, was created to conduct the knowledge translation process. Knowing that significant time would be needed from many nurses, the team wanted to ensure that this project was worthwhile. A 22-item nurse-report survey was created based on team discussions of their experience of their own night shift sleepiness and fatigue, and observations of other nurses (items shown in Table 1). Domains included drowsy driving, drowsiness at work and its sequelae, and coworker relationships. All were measured on a 4-point Likert-type scale (never/nearly never to 3–4 times per week). Drowsy driving items included “hard time keeping eyes open,” “nod off or fall asleep even for a second or two,” “no recall of portion of the ride,” “nod off at stop sign or red light.” Because any drowsy driving poses a risk, an indicator variable was created to reflect “any” drowsy driving (1–2 times per month or more often) on one or more of the four items. As frequent drowsy driving reflected elevated risk of harm, a second indicator was created to show “frequent” drowsy driving (1–2 times per week or more) on at least one of the four items. A similar classification strategy (any and frequent) was used on the remainder of the individual survey items. The post-implementation survey offered an open-ended item, “Please describe here the benefits and the drawbacks of napping on the night shift.”
Frequency of Drowsy Driving, Drowsiness at Work, and Coworker Relationships, Pre- and Post-Napping Implementation in Nurses (Pre N = 166, Post N = 177)
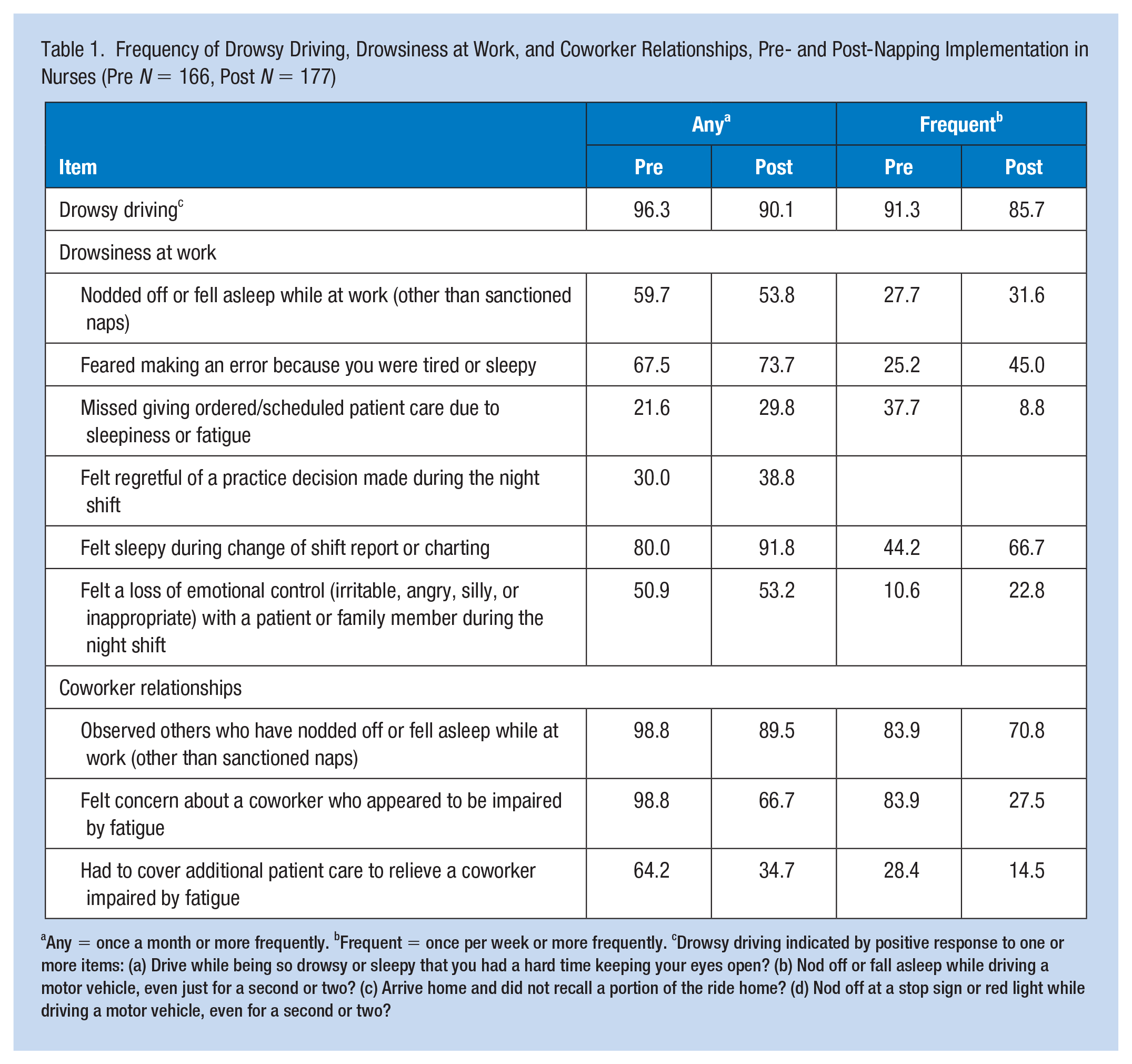
Any = once a month or more frequently. bFrequent = once per week or more frequently. cDrowsy driving indicated by positive response to one or more items: (a) Drive while being so drowsy or sleepy that you had a hard time keeping your eyes open? (b) Nod off or fall asleep while driving a motor vehicle, even just for a second or two? (c) Arrive home and did not recall a portion of the ride home? (d) Nod off at a stop sign or red light while driving a motor vehicle, even for a second or two?
An “opt out” response was provided for questions that were highly sensitive in nature (e.g., frequency of missed care and errors). On a usual weeknight, the registered nurse (RN) complement on all units was about 140. The survey was offered to RNs who worked on the night shift during a 2-week period, and the team was able to reach 87% of nurses who worked during this period. No personal or nursing unit data were collected, and the anonymous nature of the survey was stressed.
Once the pre-implementation survey phase was completed, the team reviewed and summarized the literature to document the scientific evidence basis for implementing napping and to present these data to nursing management to supplement the pre-intervention survey data with the scientific basis for implementation of napping. Fourteen clinical and laboratory experimental studies included the following outcomes: subjective and objective sleepiness, subjective and objective drowsy driving, cognitive and neurobehavioral functioning, and other noncognitive performance measures and satisfaction with naps. The Oncology Nursing Society’s (ONS) evidence rating scale was used to rank the likelihood of this intervention being effective if implemented (Johnson, 2014).
The team also examined the precedent-setting initiative of napping on this hospital’s hematology-oncology unit and the napping used by the safety time-out program of the transport team. In both cases, no operational problems had been associated with napping. No transports of sick children had been delayed or aborted, and patient care on the hematology-oncology unit had not been adversely influenced by nurses’ napping.
Policy and position documents from trade organizations and government reports were reviewed. These included a Sentinel Event Alert from the Joint Commission (2011), a Position Statement on nurse fatigue by the ANA (2014) and the American Academy of Nursing (Caruso et al., 2017), a guidance statement by the American College of Occupational and Environmental Medicine (Lerman et al., 2012), and the landmark report of the Institute of Medicine Committee on the Work Environment for Nurses and Patient Safety (Page et al., 2004). In addition, the team reviewed the National Institute of Occupational Safety and Health (NIOSH) evidence-based educational materials about shift work and long work hours (Caruso et al., 2015). A summary of the research evidence and survey data described above was presented to nursing leadership, the collective bargaining unit leadership, and the human resources department.
This was a quality improvement initiative that was reviewed by the institutional review board (IRB) and deemed as not human subjects research. The pre- and post-implementation surveys of night shift nurses were voluntary, anonymous, and results were aggregated and not reported by the nursing unit.
Results
Implementation of a Planned Nap Option
The team made seven specific recommendations based on the evidence (Figure 1). Operational questions were raised by unit managers and directors (Figure 2). Nurses who worked the night shift responded to the operational questions. The chief nurse officer, having heard the evidence, and the responses to the operational questions, gave the charge to implement a napping initiative according to recommendations made by the team.
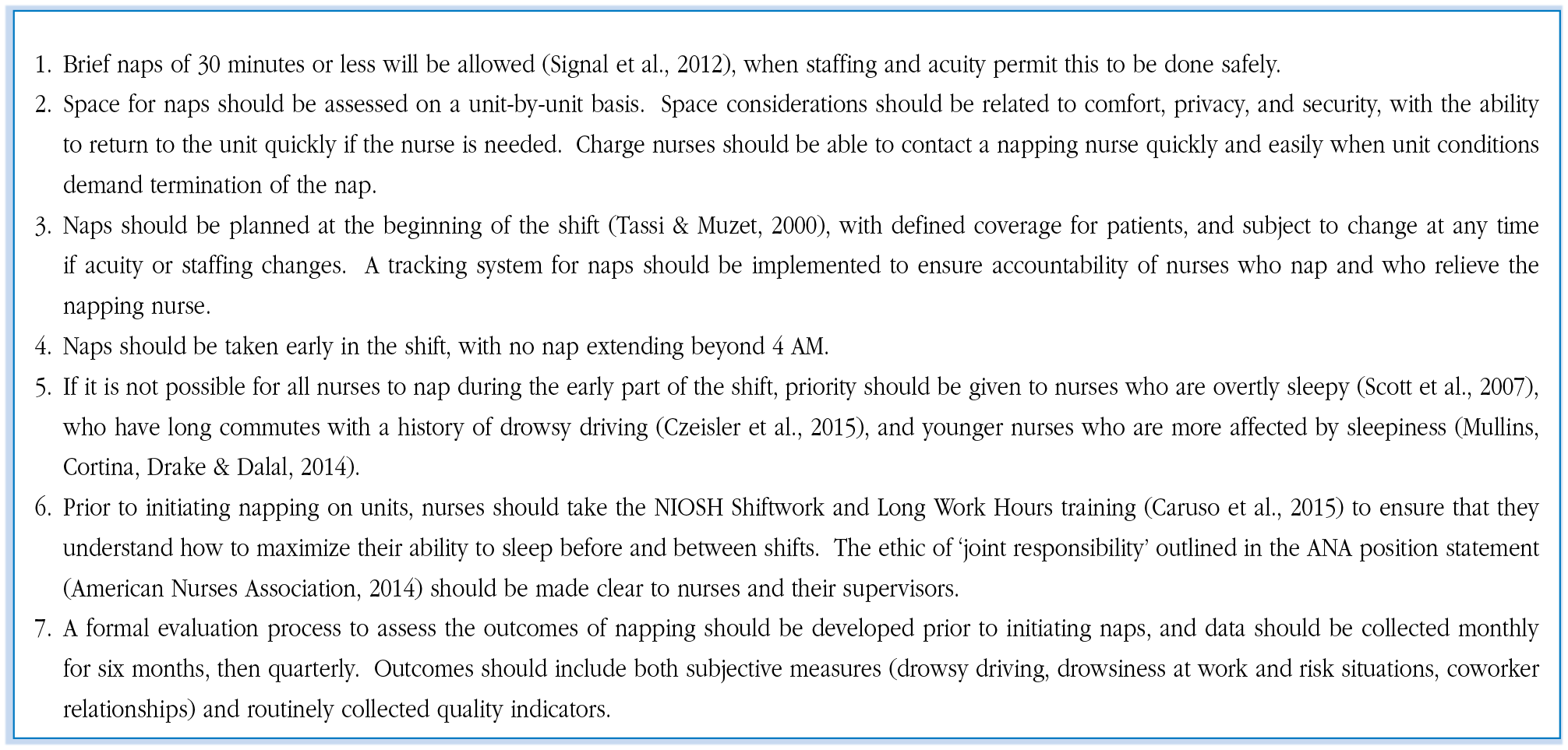
Translation team napping recommendations to nursing leadership.
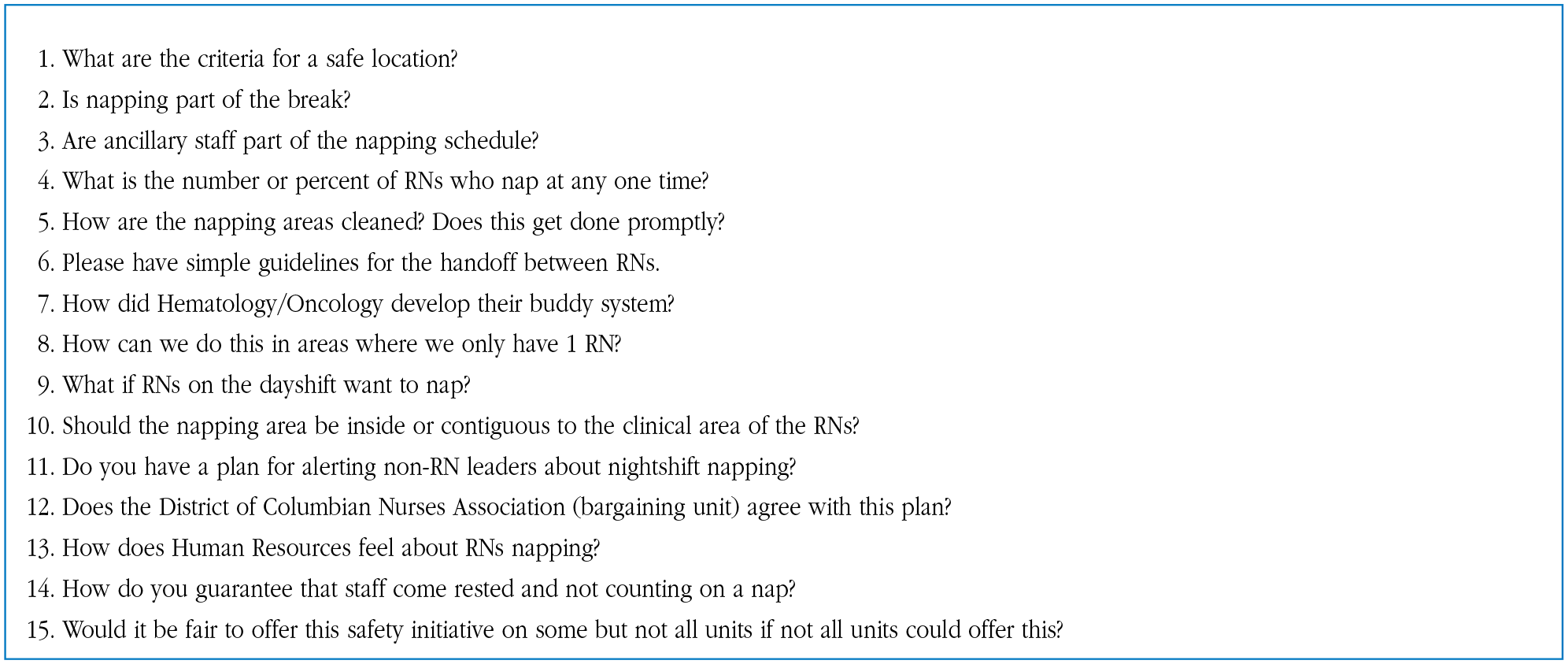
Operational concerns of nurse managers and directors.
Two factors led the vice president for nursing to the decision to move forward with nap implementation. Nearly all the napping studies reviewed during the literature review fell into the “likely to be effective” category on the ONS rating scale. Results of the pre-implementation survey showed that, among nurses who drove, 91.3% of nurses had frequent drowsy driving experiences (at least once per week); more than half of nurses nodded off or fell asleep at least once per month while at work (other than sanctioned naps); two thirds feared making an error because of sleepiness; and more than half felt sleepy during change of shift report or charting. Furthermore, nearly all participants had observed a coworker fall asleep while at work (other than sanctioned naps) and felt concern about a coworker who appeared to be impaired by fatigue.
The napping initiative recommended that nurses be allowed to take a brief (30 minutes or less) planned nap at a unit-designated specific location, before 4:00 a.m., and only when staffing and acuity permitted this to be done safely. The team developed a tool kit that included napping guidelines, a checklist of steps to consider when implementing napping on the night shift, the ANA Position Statement on Addressing Nurse Fatigue to Promote Safety and Health, a list of frequently asked questions, a link to the NIOSH educational modules for nurses on shift work and long work hours, and a statement about measuring the processes and outcomes of implementing napping on the night shift. Team members reviewed the tool kit materials with unit nurses and assisted units to implement the napping initiative.
During the nap implementation phase, barriers to napping implementation varied by unit. Staffing and space were the two most difficult obstacles to napping. Units that overcame these barriers developed a process for handoffs while the nurses napped, decision rules for who should nap when napping opportunities were limited, and whether to include ancillary personnel in the nap opportunity. Over the course of 15 months, 10 nursing units implemented napping, two units adopted it with plans to implement in the future, and two units decided that there was no feasible path to napping for their night shift nurses. One unit where napping was not feasible was a very small unit with only one to two RNs on duty at night and, for another large unit, the manager felt it would be unwise to adopt napping. The determination of whether napping was possible on a particular night, and which nurses would have the opportunity to nap, was all handled by the staff nurses, not by administrators.
Data Analysis
Pre-implementation, 166 surveys were completed and analyzed. The response rate for those who received a survey was greater than 99% for both pre- and post-implementation surveys. Of the 177 nurses who completed the post-implementation survey, 43% of nurses had tried napping to manage fatigue, 44% had not tried napping either because their unit had not implemented naps or for personal preference, and 12% were “thinking about it.”
Prior to napping, more than 90% of nurses who drove to work experienced drowsiness on the drive home once a week or more often (Table 1). After napping was implemented, the frequency of drowsy driving remained high, with 85% of nurses still driving while drowsy.
Prior to napping implementation, more than half of the nurses nodded off or fell asleep (other than sanctioned naps) while at work at least once per month. Two thirds feared making an error because of sleepiness, and 80% felt sleepy during change of shift report or charting. After nap implementation, change was inconsistent, with some items showing improvement and some decrements after naps were initiated. Frequent (once per week or more often) drowsiness at work was less than half of the “any” values, suggesting that there may be a subset of nurses for whom night shift drowsiness is a persistent condition.
Nearly all participants had observed a coworker fall asleep while at work (other than sanctioned naps) and felt concern about a coworker who appeared to be impaired by fatigue. Two thirds had needed to cover additional patient care to relieve a coworker impaired by fatigue. After nap implementation, a substantial proportion of nurses still observed a staff member who nodded off during the night.
Qualitative Analysis
A total of 98 participants (56.3%) offered written comments to the open-ended prompt. The unit of analysis to this prompt was the phrase and 256 phrases were coded. A second survey prompt invited additional comments; 53 nurses offered comments and 67 phrases were coded. Two members of the original team reviewed the written comments jointly and 17 codes resulted and were defined to comprise the coding dictionary. Two additional members reviewed all written comments using the coding dictionary. As a result of their reviews and coding, three possible combinations of two codes each were recommended because of overlapping meaning of the involved codes. Subsequent discussion with the team leader confirmed the conceptual merit of combining the identified codes, thereby reducing the number of codes to 13. The number of times that a code was identified and the number of nurses whose comments reflected each code were also counted (Table 2). The most frequently occurring codes were “feeling refreshed as I return to my shift,” “feeling safer driving home, “worrying about or actually feeling more tired upon awakening,” and “feeling too worried about patients to sleep.”
Frequency of Benefits and Drawbacks of Napping by Nurses (N = 98)
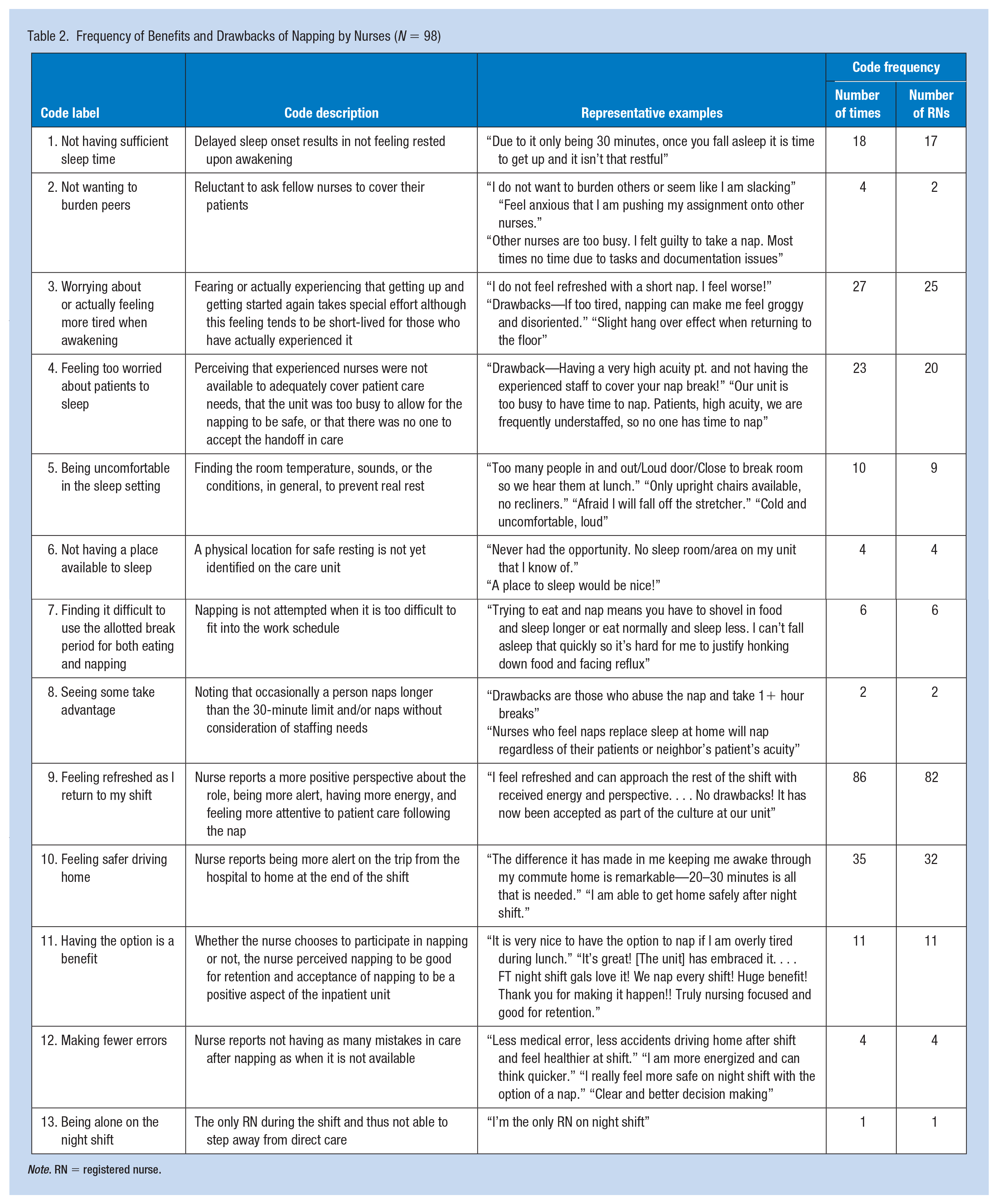
Note. RN = registered nurse.
Nurses were asked about their willingness to hand off their patient assignment to another nurse to take a nap. Those nurses who favored napping said that their unit culture supported nurses taking their break time, and that napping during break was no different than using the break for other activities. Other nurses stated they would only nap if they knew that their patient was being well cared for, only if they were able to complete all their patient care tasks and they were fatigued, and that they would keep their phone handy so that they could be reached and would answer any calls that came in. Some also set the condition that the nurse who was relieving the napping nurse would have to be a trusted and competent nurse to deliver care and have time to deliver care to the patients of the napping nurse. They would not elect to take a nap if their patient was very acute, or if they perceived staffing to be inadequate to permit the nap. Some nurses would not hand off their patients under any circumstance to take a nap. These nurses expressed concern that the units were too busy to permit napping, and that each nurse was too busy to take on additional patients while the napping nurse rests. The sense of responsibility for patients did not permit some nurses to take naps, including both staff and charge nurses. Others had more internal reasons for not napping, including long sleep latency (so no benefit), rumination about patient tasks, feelings of discomfort about napping, and concern about burdening others.
More than two thirds of nurses felt that napping benefited their nursing practice. Positive benefits included being more alert for the drive home, able to communicate more clearly and efficiently during shift changes, no longer asleep when charting, more refreshed and able to focus, more energized, more confident to accomplish tasks without error, less stressed, able to think more quickly, and able to wind down and regroup. These nurses reported that even 30 minutes made a difference and having the option to nap was very satisfying.
Nurses who expressed negative sentiments had a variety of reasons for not being in favor of napping. One nurse expressed a concern that coworkers might feel that naps replace sleep at home and would nap regardless of their patient or unit needs. Others had discomfort about the sleep itself, such as feeling drowsier on arising, having a headache, having long sleep latency, and not able to think clearly upon awakening if they had been exhausted at the beginning of the nap. Other nurses reported that the nap opportunity was too short; they were not able to get enough rest in that short period of time and preferred to use the time to eat rather than sleep. Nurses also reported that the sleeping accommodations were uncomfortable.
The physical space for napping was an issue for some nursing units. Two thirds of the nurses said that their napping space was comfortable. Of those who were dissatisfied with the space, complaints were of excessive noise, physical discomfort (sitting up in a chair), lack of a door lock, others using the room for other purposes, and interruptions while napping, which were a deterrent to restful napping. Yet only one third of napping nurses complained of interruptions during the nap, whereas more than 80% said that the napping space was safe.
Discussion
The problem of fatigue-related errors, accidents, and injuries was a persistent problem in health care despite attempts to reduce workplace fatigue and sleepiness through work schedule manipulation. Research suggested that brief naps on the night shift were an effective way to reduce fatigue and sleepiness (Ruggiero & Redeker, 2013). This quality improvement initiative showed that a systematic approach to implementing night shift naps was successful on 10 out of 14 units and napping was sustainable in one acute care hospital. This contrasted with the observation by Edwards et al. (2013) that napping was difficult to implement. We believe that the experience of napping implementation in this single hospital can be generalized to other settings because each nursing unit had to solve unique problems (e.g., space, staffing, and handoffs) in the adoption and implementation process. This team’s approach included keeping leadership informed of the team’s intentions and progress and used the accumulated wisdom of night shift nurses to craft a unit-based strategy. Responding to operational concerns of managers prior to implementation was important to gain their support. By providing a step-by-step plan for napping implementation and a tool kit, this quality improvement initiative can be replicated by other hospitals who desire to use this method to reduce sleepiness on the night shift.
Our data showed that drowsy driving was a clear risk and was reduced by only 5% when measured subjectively post-implementation. These data contrasted with experimental literature, using objective driving measures, which showed drowsy driving to be reduced by a brief nap (Sagaspe et al., 2007; Smith-Coggins et al., 2006; Signal et al., 2012). Our data may differ because napping had lower than expected night-to-night penetration due to staffing and acuity, or nurses’ reluctance to nap. It may also be because a brief nap was not powerful enough an intervention to overcome the biologic propensity toward sleepiness from a high level of sleepiness and a low circadian alerting signal at 7:00 a.m.
Scott et al. (2007) showed that drowsiness during the shift was one of the best predictors of drowsy driving after the shift. Naps do not eliminate the hazards of drowsy driving, and it is still necessary for nurses to receive education to reduce the hazard of driving home from work after the night shift (Caruso et al., 2015). A better solution may be for nurses or hospitals to purchase in-car drowsy driving detection technology to provide real-time alerting to increase the driver’s own awareness of when drowsiness occurs during the drive (Aidman et al., 2015). The shift in emphasis, from reducing fatigue to managing fatigue risk, points to the need for accurate self-detection of fatigue and effective risk-mitigation strategies among nurses (Honn et al., 2019).
Several nurses in this quality improvement initiative had sleep inertia symptoms and avoided napping. Sleep inertia is most common when individuals are already quite sleep deprived at the time that they take a nap (Tassi & Muzet, 2000). Nurses need to self-monitor their sleep and ensure that they are getting adequate rest before coming to work. In a study of neurobehavioral functioning (reaction time to a visual stimulus), Geiger-Brown et al. (2012) found that sleep deficiency-related cognitive impairment was trait-like, with some nurses showing significant slowing of reaction times. In an observational study of nurses who did and did not nap, those who chose to nap had higher levels of fatigue as measured on the Brief Fatigue Inventory (Neville et al., 2017). In nurses for whom napping was successful, it was beneficial both during and after the shift (to reduce drowsy driving on the way home). Identifying nurses who were biologically intolerant to safely perform shift work (such as those with shift work sleep disorder) was not addressed operationally in most settings. Having additional means of preserving alertness during the night shift (e.g., light amplification, timed caffeine doses, and shift scheduling to reduce fatigue risk) may be needed to reduce fatigue and sleepiness (Lerman et al., 2012) for those who cannot or should not nap. Napping should be but one component of a comprehensive fatigue risk management system to reduce the risk for accidents, injuries, and errors during the night shift and drowsy driving after the night shift.
Eighty-two percent of participants felt refreshed by the brief nap. This was consistent with the large experimental literature on subjective and objective measures of sleepiness, with 10 out of 15 studies favorable to the napping condition; however, many used naps longer than 30 minutes, or were conducted in laboratory conditions. Of the six studies where naps were of 30 minutes or less, three favored napping (Lovato et al., 2009; Sallinen et al., 1998; Smith et al., 2007). The two studies performed in a healthcare environment showed less sleepiness (Smith et al., 2007) and less fatigue (Smith-Coggins et al., 2006) after napping. However, most nurses still had some sleepiness despite the opportunity to nap. There was a biological propensity to sleep that was unmasked during the night shift, when circadian pressure for waking was low and there was less environmental stimulation with dimmer light, and less noise and activity.
There were limitations to this quality improvement initiative. The pre- and post-implementation data represent two cross sections where there was unmeasured dependency. A within-subjects approach to design would have been more informative and would have permitted a statistical comparison of outcomes. The hospital administrators and team chose to administer the survey with complete anonymity because the sensitivity of asking questions such as those included in this survey cannot be underestimated. Although the investigators offered a “prefer not to say” option, it was seldom utilized. We reduced our ability to interpret and generalize these data by not collecting demographic or nursing unit information but believe that it provided responses that were more truthful. Future studies should use a within-subjects research design rather than a quality improvement approach to precisely quantify individual differences pre- and post-nap implementation.
Applications to Professional Practice
Implementing brief naps for night shift nurses was possible in many acute care hospital nursing units and has the potential to reduce drowsy driving on the way home from the shift in some nurses. Other benefits of napping were less clear and the problem of sleep inertia deters some nurses from using napping to reduce night shift fatigue. The perspective from nurses who did not use the napping option helped us to learn that napping may not be the best option to reduce sleepiness for all nurses. Napping was but one strategy to reduce night shift sleepiness and may be part of a fatigue risk management system that comprehensively addressed the challenges of shift work. Additional studies are needed to determine the subpopulation of nurses for whom napping works well.
Footnotes
Author Contributions
The authors J.G.-B. and P.S.H. designed and directed the project; A.H., B.B., and K.S. contributed to the conceptualization of the survey measures; A.H., B.B., and P.S.H. collected the data for both waves; J.G.-B. analyzed the quantitative data; A.H., B.B., and P.S.H. analyzed the qualitative data; All the authors contributed to manuscript preparation and review.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Jeanne Geiger-Brown, PhD, RN, FAAN, is the associate dean for research and professor at the George Washington University School of Nursing.
Ashleigh Harlow, BSN, RN, CCRN-K, is a doctoral student at the Duke University School of Nursing.
Brett Bagshaw, MSN, RN, CPN, is a crisis nurse at Children’s National Hospital.
Knar Sagherian, PhD, RN, is an assistant professor at the University of Tennessee Knoxville School of Nursing.
Pamela S. Hinds, PhD, RN, FAAN, is the executive director for the Department of Nursing Science and Professional Practice and Quality, the William and Joanne Conway Chair in Pediatrics, and the research integrity officer at Children’s National Hospital. She is also a professor of pediatrics at the George Washington University School of Medicine and Health Sciences.