
Abstract
Background
Nurses who work at night have used naps to alleviate their sleepiness and fatigue. Research has shown night shifts, sleepiness, and fatigue predict nurses’ missed workdays. Thus, nighttime napping may have a beneficial consequence of reducing nurses’ sickness absences. The purpose of this brief report was to describe the difference in rates of short-term sickness absence before and after implementation of a 30-min nap opportunity in one U.S. hospital for 12-hr shift nurses.
Methods
The study was a retrospective pre–post evaluation design. Eight units provided nap opportunities for the nurses. Full-time nurses were classified into night and rotating shifts based on their 2 years of scheduling patterns. Absence data were extracted from the hospital’s timekeeping system and annual absence rates were computed. A single linear mixed model with rank transformed data was conducted for each group. Median estimates, minimum and maximum, and p-values were reported.
Findings
The median absence rates for night shift nurses were 4.3% and 4.0% for the pre-napping and post-napping implementation periods, respectively; however, this difference was not statistically significant (p = .241). The median absence rates for rotating shift nurses were 2.0% and 3.9% for the pre-napping and post-napping implementation periods, respectively; and the difference increase was statistically significant (p < .001).
Conclusion/Application to practice
A nap policy which provides nurses with the opportunity to take nighttime naps did not benefit their sickness absence rates. Future research needs to examine the actual napping process on sickness absences, as well as explore other sickness management avenues.
Background
Shift workers have used brief naps during night shift work as a countermeasure to alleviate sleepiness, fatigue, and drowsy driving (Han et al., 2021; Martin-Gill et al., 2018; Ruggiero & Redeker, 2014; Watson et al., 2015) and improve cognitive performance (Dutheil et al., 2020). In hospital nursing, napping for night shift nurses is not widely implemented due to limited space, stigma around sleeping at work, fear of sleep inertia, and institutional policies that prohibit sleep while on duty (Li et al., 2019). While studies have shown that workers who nap show benefits, at the institutional level the benefits to acute care hospitals are less clear.
Sickness absence—missing scheduled workdays—among hospital nurses is an institutional valued outcome where the data can be monitored closely and extracted from the time and attendance system without subjectivity. Sickness absence is problematic because it interferes with the workflow on in-patient units, creates temporary staffing shortage, negatively influences the continuity of patient care, and is costly to the institution. Longitudinal research has shown night shift work, sleepiness and work-related fatigue increase nurses’ future sickness absences from the workplace (Dall’Ora et al., 2020; Gohar et al., 2020; Sagherian et al., 2017). The purpose of this brief report was to describe, for one U.S. hospital, the difference in rates of short-term sickness absence before and after implementation of a 30-min nap opportunity for 12-hr shift nurses on eight nursing units.
To test the association between napping and sickness absence, we used administrative data from a single metropolitan hospital that successfully implemented a nighttime nap opportunity on eight nursing units. For the night shift nurses, we hypothesized that there would be an association of nap opportunities during the night shift with short-term sickness absence rates. Second, we hypothesized that the rotating shift nurses would show smaller reductions in short-term sickness absence rates due to less frequent night shifts worked.
Methods
The study was a pre–post evaluation design. It was a retrospective analysis of time and attendance/payroll records that were extracted by a system analyst from the hospital’s timekeeping system. Eight nursing units where a nap opportunity was implemented provided data for a year beginning on the date of napping implementation (Year 2) and the year prior to implementation (Year 1). Most nursing units had started with providing the nap opportunities in 2016 or 2017. The napping policy allowed nurses working during the night shift to take a 30-min nap in a designated room when staffing and patient acuity afforded them the opportunity to do so. The details of the napping implementation process were published elsewhere (Geiger-Brown et al., 2016, 2021). Nurses designated as a registered nurse (RN), assigned to one of the eight nursing units, and coded as full-time in the timekeeping system formed the sample.
The initial data file had 650 nurses with 154,776 shifts over the 2 years of observation. Each shift that was worked was coded as either day or night shift based on the U.S. Department of Labor, Bureau of Labor Statistics definition (McMenamin, 2007). Night shift was defined as having a majority of the hours worked during the shift occurring between 9 p.m. and 8 a.m. Day shift was defined as having a majority of hours worked falling between 8 a.m. and 4 p.m. Each nurse was assigned a classification as to their predominant shift pattern. Classifications were either night shift (≥90% of all shifts worked over the 2 years meeting the night shift case definition), day shift (≥90% of all shifts worked over the 2 years meeting the day shift case definition), or rotating shift (fell between day and night shift classification, with both nights and days over the 2 years). The sample included night and rotating shift nurses because both groups were eligible to nap during the night if staffing and patient acuity permitted them on that shift. The analytic file had 68 night shift nurses and 220 rotating shift nurses who were present over the 2 years on their assigned units (i.e., matched pre- to post-implementation) and maintained a full-time work status.
To derive an annual short-term absence rate, each shift that was scheduled was coded as either present (worked), absent, or time off-excused (e.g., holiday, vacation, jury duty, bereavement, military leave, and maternity leave). Short-term sickness absences were absences that lasted less than three consecutive weeks. Data for time off-excused codes and extended long-term sickness absences (absence periods extending beyond three continuous calendar weeks) were removed from the analytic file. After the data cleaning process, annual short-term sickness absence rates were computed by dividing the total number of hours of absence by the total number of scheduled hours of work (absent hours plus worked hours) for each nurse. The hours worked and absence hours were captured to one decimal place. Multiplied by 100, the absence rate represented the percentage of absenteeism for that specific period.
The Institutional Review Board at Children’s National Hospital study determined the study as exempt from continued board oversight.
For data analysis, the data were analyzed in SPSS version 28. The outcome had a nonnormal distribution. The analysis was conducted on rank transformed data and the assumption for residuals being normally distributed was met. Two separate single linear mixed models (LMMs) with pre–post napping period as fixed effects with an AR1 covariance structure for repeated effects was conducted for night shift nurse rosters and rotating shift nurse rosters. The random effect of the units was not statistically significant (p = .658), and the variable was removed from the models. The single model that reduced the risk for type I error tested if the napping policy had any effect on changes in short-term sickness absence rates in the post-napping implementation (Year 2) period as compared with the pre-napping implementation (Year 1) period. Median, minimum, and maximum estimates and p-values were reported. Significance level was set at .05 level.
Results
Table 1 presented the percentage of short-term sickness absence rates for the pre-napping and post-napping implementation period among night and rotating shift nurses. Night shift nurses had a median annual short-term sickness absence rate of 4.0% in Year 2 which was slightly lower than the 4.3% in Year 1. However, this difference in absence rates between the pre-napping and post-napping implementation periods was not statistically significant: F(1, 67) = 1.40, p = .241. Rotating shift nurses had a median annual short-term sickness absence rate of 3.9% in Year 2 which was higher than the 2.0% in Year 1. This difference in absence rates between the pre-napping and post-napping implementation period was statistically significant: F(1, 219) = 69.40, p < .001. This result indicated nurses on rotating shifts after the nap opportunity had a significant increase in short-term sickness absence rates when compared with the previous year.
Short-Term Sickness Absence Rates of Night and Rotating Shift Nurses by the Pre-Napping and Post-Napping Periods
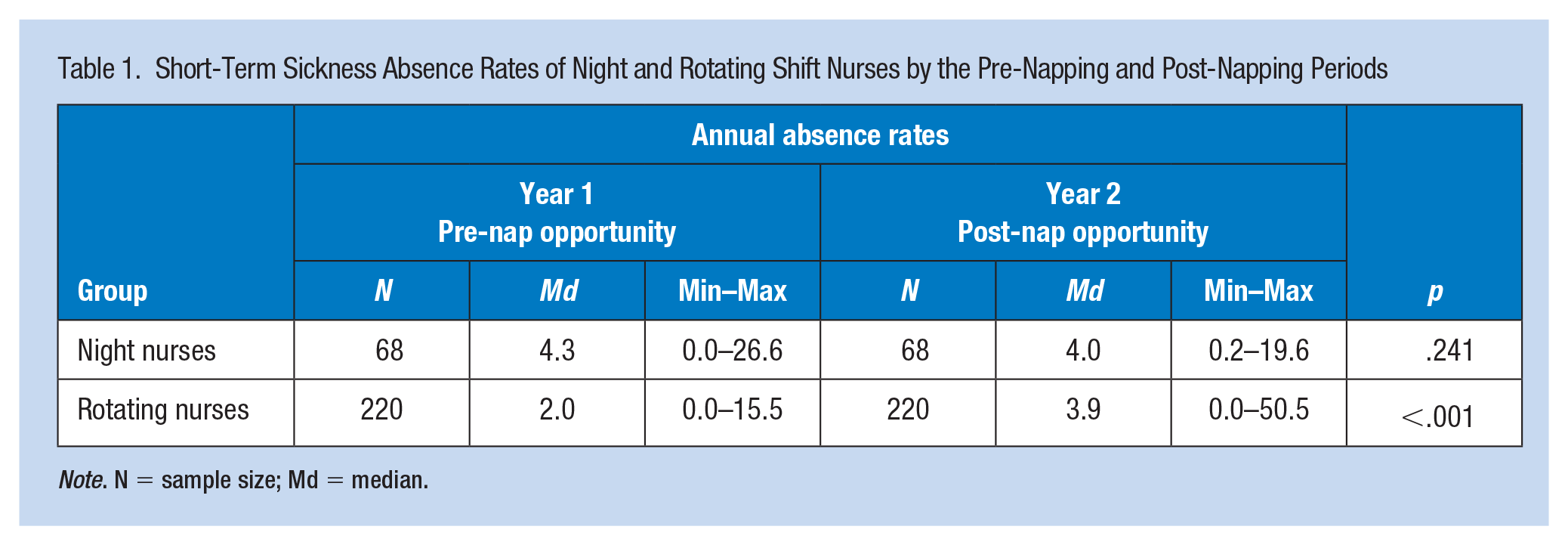
Note. N = sample size; Md = median.
Discussion
This study was a first attempt to investigate the effect of a nap opportunity on short-term absenteeism among night and rotating shift nurses. For our first hypothesis, the findings showed the nap opportunity was not related to night shift nurses’ short-term sickness absence rates over 12 months though the change was in the hypothesized direction. A nap opportunity may not be always present at nights due to staffing matters and patient acuity, and therefore, some nurses may not have napped resulting in a weakened effect. Moreover, our overall rate of short-term sickness absence is a crude outcome measure that does not differentiate between missed days of work for health or nonhealth (family or social responsibilities) reason, and where naps may influence one but not the other. Brief naps during the night shift have been shown to some extent help nurses and other health care providers with their fatigue and sleepiness at work (Han et al., 2021; Martin-Gill et al., 2018). The hypothesis for possibly reducing short-term sickness absences via a nap opportunity was based on the longitudinal associations between sleepiness, acute fatigue, night shifts, and increased risk for sickness absence episodes among nurses (Dall’Ora et al., 2020; Lallukka et al., 2014; Sagherian et al., 2017). Our findings may also be affected by the turnover rate at that time ranged from 11% to 14% across the units. This speaks to the benefit of conducting a future longitudinal prospective study where attrition related to leaving the hospital setting to avoid night shifts could be carefully tracked and accounted for in the analysis.
For our second hypothesis, the findings in rotating shift nurses showed the napping implementation period had a higher short-term sickness absence rate when compared with the pre-napping implementation period. However, this increase of almost 2% in Year 2 is unlikely related to the nap opportunity that is limited in this group. One possible explanation may be related to the operational definition of rotating shift nurses where the percentage of working night or days shifts can range anywhere from 11% to 89%. For example, a nurse who worked 30% day shifts and a nurse who worked 30% night shifts may have different absence rates over the study period and yet they are considered rotating shift nurses. There is anecdotal evidence from the hospital that rotating shift nurses have a different approach to working nights than permanent night shift nurses. Night shift nurses organize their life around their work schedules and plan for adequate rest and power naps prior to work which is believed not to be the case for the rotating shift nurses. Despite their different approaches, our findings showed that rotating shift nurses had lower annual short-term sickness absence rates both in the pre-napping and post-napping implementation periods than the night shift nurses (Table 1). Several studies from England and Scandinavia have reported an increased risk for short-term (Bernstrøm & Houkes, 2020; Ropponen et al., 2019) and long-term (Dall’Ora et al., 2020; Larsen et al., 2020) sickness absences when nurses and hospital staff worked mainly night shifts. For future research, it would be helpful to explore over extended periods if rotations that are more evenly distributed between 12-hr day and night shifts will yield similar results or help lower future short-term sickness absence rates.
A strength of this study was the use of objectively documented absence data from the timekeeping system in full-time nurses over 2 years. The data allowed the researcher to classify full-time nurses into night shift nurses and rotating shift nurses objectively based on their patterns of worked shifts over 2 years and not rely on self-reporting of shift type. Also, the pre–post design was useful in examining the impact of an institutional wide napping implementation among the same group of nurses within a single hospital. The study had limitations that inform future research. The first limitation is related to the difference between having a napping opportunity and the actual event of napping. The presence of a napping opportunity in Year 2 does not guarantee that actual napping occurred during the nights. In addition, the nursing units did not track and collect any administrative data on which nurses or how many nurses were able to nap. Therefore, testing our hypothesized relationships without such detailed data makes the analysis dependent on large differences that may not exist. The findings from a previous cross-sectional study using survey data from the same hospital showed that fewer than half of the nurses napped during the night shift. Naps were not taken when staffing or patient acuity did not permit the nurses to cover each other’s patients (Geiger-Brown et al., 2021), so the opportunity to nap varied night by night on each unit. This may likely be the case in this study where actual napping events could not be confirmed nor napping patterns established which may weaken the effect of napping on short-term sickness absence rates if a true relationship existed. Future similar research initiatives should consider collecting more detailed nap data when evaluating brief naps in relation to short-term sickness absence. Second, as is true with any administrative data that are collected for other purposes, there may be some misclassification bias, but the amount of this bias is likely very small, and in the direction of the null. The data about absence rates were accurate, but provided little explanation that could allow the researchers to interpret the meaning of the rates more fully in the context of other unmeasured or contextual factors. Third, the data used in our analysis accounted for full-time nurses only. However, the nursing units were also staffed with part-time nurses, per diem nurses, and float nurses. All of these nurses were eligible to use the napping opportunity while being on night shifts. Therefore, the short-term sickness absence rates reported here may not be a full representation of absence rates on the nursing units. Regarding external validity, the study findings cannot be generalized to nurses with different employment status, shift durations, and from other hospitals and therefore must be interpreted with caution.
Conclusion
Our study showed the implementation of a 30-min nap opportunity did not influence or overall benefit the short-term sickness absences of night or rotating shift nurses at one hospital. Surprisingly, the annual short-term sickness absence rate of rotating shift nurses during the nap opportunity period was higher than the prior year. Our findings and in the absence of napping usage data are inconclusive on the effectiveness of naps for managing short-term sickness absences among night shift and rotating shift nurses.
There continues to be a need to identify and test practical strategies tailored toward short-term sickness absence management among hospital nurses. One unit-level approach is the use of participatory working time scheduling software that has been shown to lower short-term sickness absences among hospital staff (Turunen et al., 2020). It is also important to collect more focused data on the usage of the napping on nursing units, separate absences for health and nonhealth reasons, and extract additional administrative data related to nurse-level characteristics. As for the next step, the hospital has plans to conduct a longitudinal prospective study and further expand on the napping implementation policy with a renewed emphasis on sleep hygiene, use of mindfulness, and physical activity during the night shifts.
Implications for Occupational Health Nursing Practice
Brief nighttime naps are one of the most common fatigue countermeasure strategies used during work hours. Experimental and field studies have shown the benefits of brief nighttime naps on sleepiness, fatigue and cognitive performance. These naps when taken during nadir periods are effective in reducing nurses’ sleepiness and fatigue during the nights, and are recommended for these purposes only. At the present, our findings are inconclusive in the use of naps specifically for short-term sickness absence management on nursing units, and thus other practical strategies need to be explored in the meantime.
Applying Research to Occupational Health Practice
A 30-min nap opportunity supported by an institutional napping policy provided the nurses on 12-hr night shifts with the time and space to take brief naps when patient acuity and staffing permitted. The hospital’s primary purpose of implementing nighttime napping was to reduce nurses’ sleepiness and fatigue, and therefore napping practices were recommended. It is worth mentioning that a nap opportunity does not always guarantee the actual event of taking a nap on the nursing unit. Our study showed that the adoption and implementation of 30-min nap opportunity for 12 months had no immediate beneficial impact on nurses’ short-term sickness absence rates when compared with the previous year. Given the inconclusive nature of the findings, we recommend nursing administration in partnership with hospital nurses to explore other practical strategies for short-term sickness absence management in the workplace.
Footnotes
Authorship
All authors have made substantial contributions to the manuscript to meet the criteria for authorship and have reviewed and agreed to the final version. K.S. and J.G.B. conceived the study and its design, D.D. performed data extraction from the hospital’s timekeeping system; J.G.B. performed data management and data cleaning; C.S. and K.S. conducted the statistical analysis and interpretation of data; K.S. and J.G.B. drafted the manuscript; P.S.H., D.D., J.G.B., and J.J.M. revised the manuscript for critically important intellectual content, and all members approved the final version for submission.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study received the Suzanne Feetham Research Support Award from the hospital.