
Abstract
Objective
Development of personalized sleep–wake management tools is critical to improving sleep and functional outcomes for shift workers. The objective of the current study was to test the performance, engagement and usability of a mobile app (SleepSync) for personalized sleep–wake management in shift workers that aid behavioural change and provide practical advice by providing personalized sleep scheduling recommendations and education.
Methods
Shift workers (n = 27; 20 healthcare and 7 from other industries) trialled the mobile app for two weeks to determine performance, engagement and usability. Primary outcomes were self-reported total sleep time, ability to fall asleep, sleep quality and perception of overall recovery on days off. Secondary performance outcomes included sleep disturbances (insomnia and sleep hygiene symptoms, and sleep-related impairments) and mood (anxiety, stress and depression) pre- and post-app use. Satisfaction with schedule management, integration into daily routine and influence on behaviour were used to determine engagement, while the usability was assessed for functionality and ease of use of features.
Results
Total sleep time (P = .04), ability to fall asleep (P < .001), quality of sleep (P = .001), insomnia (P = .02), sleep hygiene (P = .01), sleep-related impairments (P = .001), anxiety (P = .001), and stress (P = .006) were all improved, with non-significant improvements in recovery on days off (P = .19) and depression (P = .07). All measures of engagement and usability were scored positively by the majority of users.
Conclusions
This pilot trial provides preliminary evidence of the positive impact of the SleepSync app in improving sleep and mood outcomes in shift workers, and warrants confirmation in a larger controlled trial.
Introduction
With the advent of a 24-h society, an increasing proportion of individuals are required to work irregular hours, with approximately 20% of western workforces working either night or rotating shift patterns. 1 In addition to these typical shift types, an increasing number of individuals are engaged in work outside their standard 9 AM–5 PM working hours, due to the increasing demand for workplace flexibility, expanding remote work and diversified communication options. The COVID-19 pandemic accelerated the growing trend towards flexible work arrangements. 2 There are recognized benefits to the flexibility afforded by shift work or non-standard work hours. At a societal level, there is increased productivity and improved provision of necessary services. For individuals working shift work or non-standard hours, increased flexibility assists in accommodating the demands of work, social and family life and allows individuals to shift activities to more convenient times.
The most immediate adverse consequence of shift work and non-standard hours is inadequate sleep (acute and chronic). In addition, the schedules imposed by shift work often oppose the timing of the internal circadian clock, 3 such that it is misaligned with sleep and wake. Consequently, shift workers report an increased functional impact of sleep disturbance and misalignment, including impaired alertness/increased sleepiness during wakefulness,4–7 compared to the general population. Shift workers are also at greater risk of a range of long-term adverse health consequences such as gastrointestinal problems, cardiovascular disease, mood and affective disorders and cancer,8,9 as well as an increase in sleepiness and the risk of errors, accidents and injuries.10,11 Shift work, and the resultant sleep and circadian clock disruption, is also associated with negative consequences to family life, overall lifestyle and motivation. 12
Given the widespread adverse impacts of shift work on sleep and health outcomes, as well as the high personal and societal cost of these, there is a compelling need for effective shift work management strategies. To date, the emphasis of research and development of interventions to improve outcomes for shift workers has been on broad, systemic approaches, 13 such as changes to shift scheduling, 14 workplace lighting interventions, 15 scheduled workplace napping, 16 wellness programs and workplace fatigue management programs. 17 In addition to organizational-level interventions, the individual should also be equipped with resources, interventions and tools to personally manage their sleep disturbances. For example, the efficacy of physical activity 18 and sleep hygiene education19,20 in counteracting the negative consequences of shift work has been examined. Although these interventions have been shown to have some success in ameliorating the detrimental effects of shift work, there remains a need for individual workers to have evidence-based strategies to optimize their sleep around their work schedule. Regardless of organizational-level improvements in managing alertness and fatigue on shift, these approaches do not meet the needs of the underlying biology of all individuals and as such, improved strategies are required to assist in optimizing sleep around individuals’ specific work patterns. There are, however, few approaches that are both individualized and specifically focused on optimizing sleep through its timing.
To address this unmet need, an automated, personalized sleep–wake management iOS Swift mobile phone app (SleepSync) was created for shift workers. SleepSync was co-designed with formative research and key stakeholders in several stages: (i) proof of concept (POC) testing; (ii) voice of customer (VOC) analysis; and (iii) prototype development. The POC study utilized theoretically driven principles of sleep–wake management to provide paper-based, personalized sleep–wake schedules to nurses who screened a high risk for shift work disorder (SWD). 21 The POC study demonstrated an improvement in sleep and functional outcomes with a sleep–wake management tool specifically tailored to individuals 22 and provided the rationale for further development of an automated app. VOC analysis was then conducted with intensive care unit and emergency department shift working nurses. Through qualitative semi-structured interviews, this analysis aimed to understand shift worker attitudes and behaviours surrounding sleep and lifestyle management to identify problem areas and opportunities for improvement, and co-design a solution. Through an iterative process informed by users, clickable wireframes were presented to the users and their feedback was used to inform the final product concept and acceptability. Based on the key findings, app features and the user interface were developed through a series of development cycles. The algorithm for calculating sleep–wake recommendations is based on the circadian and sleep homeostatic interaction, 23 the principles of which are built into a decision-tree model. The algorithm was developed, coded and packaged in an industry-standard app programming interface conforming to the constraints of representational state transfer (REST) architectural style.
Mobile technology provides a novel and innovative way in which to deliver personalized interventions, particularly to address sleep disturbances such as those experienced by shift workers. Although there has been limited evidence for the clinical utility, 24 safety 25 and accuracy 26 of mobile health (mHealth) apps and fitness tracking devices, increased interest in this intervention modality has encouraged more substantive investigation. A recent review of mHealth apps for sleep showed that the implementation of behaviour change techniques in mHealth apps is effective for improving sleep outcomes, particularly subjective sleep quality. 25 Although most mHealth apps reviewed included multiple behaviour change techniques, the most frequently implemented were (i) feedback and monitoring, (ii) knowledge shaping, and (iii) goals and planning. These components also had the highest rate of positive outcomes for sleep. 25 User engagement is also a critical element of mHealth apps for sleep interventions and is largely driven by app functionality and usability. 27 Relevancy and personalization of information and educational material are also important for maintaining engagement. 27
SleepSync is intended to aid behaviour change and provide practical guidance via sleep scheduling recommendations and education. The key features of the app include: (i) a schedule management calendar for work and personal commitments; (ii) biologically viable recommendations for sleep timing that account for work and social obligations based on the information users input into the calendar, such as work shifts and important personal activities; (iii) daily logging of actual sleep/wake times and mood; and (iv) feedback to users in the form of a ‘recovery score’ based on the level of adherence with the recommended sleep times.
The study reports outcomes for user testing and positive impact of SleepSync. The primary objective was to assess users’ perception of the SleepSync app in aiding recovery from shift work, in addition to the level of user engagement with the app. Examination of participants’ mood and sleep-related impairment changes during trial participation was included as a secondary assessment of app impact. Finally, the study examined user perception of usability of the SleepSync app.
Methods
This project was facilitated by the Cooperative Research Centre for Alertness, Safety and Productivity (Alertness CRC), based in Australia, and includes Monash University, The Institute for Breathing and Sleep at Austin Health, The University of Sydney, Woolcock Institute of Medical Research, and Koninklijke Philips N.V. (Philips). The study was approved by the Monash University Human Research Ethics Committee. All participants provided written informed consent and were reimbursed for the time committed to the trial.
Recruitment
Participants were recruited and enrolled in the study from October 2019 to December 2019 via social media (e.g., Facebook), including occupation-specific pages, interest groups and unions. Potential participants completed an Expression of Interest survey that included contact information, basic demographic information and current shift details. Participants were included if they were aged 25–55 years old, employed a minimum of 30 h per week in shift work and expressed difficulty managing their professional and/or personal schedules due to shift work. They were also required to have an iPhone 8 or newer model and be willing to use SleepSync on a daily basis for the duration of the trial. Participants were excluded if they had previously participated in user testing of SleepSync, had less than three day-to-night shift rotations during the testing period, or did not have a live-in partner, children or other dependents.
Participants
A total of 30 participants were recruited. As this study was a feasibility user testing trial for which the standard deviation will be used in a sample size calculation for a full-scale trial, this is in line with previously recommended sample sizes. 28 The primary participant cohort in this study was nurses (n = 21). Nurses were identified as a core demographic for testing the app for several reasons: (i) they comprise the largest body of shift workers in Australia 29 ; and (ii) shift schedules in healthcare settings are often more variable than other industries, thus providing the opportunity to test the app in a complex shift working environment. The primary population of interest was hospital nurses; however, we recognize that several other industries are engaged in shift work. We, therefore, included a limited number of participants (N = 9) to represent other industries, using a purposive sampling approach. This included the following industries: law enforcement (n = 2), manufacturing (n = 3), retail (n = 1), construction (n = 1), laboratory technician (n = 1) and emergency services (paramedic; n = 1). Due to technical problems with the app, three participants were not included in the analysis. Thus, the final sample size was 27 participants.
Data collection procedures
The study had a pre-post design. Following the completion of an online consent form, data were collected prior to app users via an online survey including validated questionnaires (65 items) assessing sleep and recovery, mood and daytime functioning. The same survey, with the exception of demographic questions and the composite Morningness-Eveningness Questionnaire (cMEQ),30,31 was administered within 3 days of the end of the trial period, in addition to a semi-structured interview conducted either face-to-face or via Zoom, with each participant covering sleep and recovery as well as the functionality of the various features of the app.
Participants installed SleepSync on their mobile device following the completion of the online questionnaires. Other than for downloading and installing the app, participants were given minimal instruction on how to use the app to simulate a ‘real-world’ consumer experience. They were instructed to set up and use the app for 14 days. A researcher contacted each participant at least twice throughout the 14-day trial period to troubleshoot any problems with the app.
Participants were asked to explore and engage with all of the features of the app, including entering work shifts into the calendar, entering daily sleep and wake times, daily mood ratings and their adherence to the advised limitation on caffeine intake prior to bedtime and device screen time. Participants were asked to follow the sleep recommendations as closely as possible.
Demographic information and participant characteristics
Demographic information was collected in the online survey and included sex, age, years of shift work experience and number of children. Participants also completed the cMEQ.30,31 The cMEQ is a self-report assessment of an individual's predisposed preference for the timing of mental and physical activity, referred to as chronotype, and is considered to be an indication of the timing of the internal circadian clock. Early chronotypes have very early sleep and wake times, whereas late chronotypes follow very late sleep and wake patterns. Early and late chronotypes describe the two extreme ends of the spectrum, although most individuals sit somewhere in the middle (Intermediate chronotypes).30,31
Primary outcome measures
Primary outcome measures for engagement and usability were measured on either an 11-point or 5-point Likert scale. An 11-point scale was used to avoid skewness and increase sensitivity. 32 A 5-point Likert scale was implemented for usability questions to ensure comparability with other usability measures, such as the Systems Usability Scale. 33
User perception of the impact of the SleepSync app
App impact was determined via one Likert-type question per measure in the online survey. Participants were asked to rate the following on a scale of 0–10, where 0 was ‘not at all’ and 10 was ‘fully recovered/satisfied’: (i) recovery following shift work on days off; (ii) sleep quality; and (iii) satisfaction in their ability to fall asleep. Self-reported total sleep time was also collected via the online survey, in which participants were asked to record their average sleep duration, in hours, over the past two weeks. The difference between pre- and post-app scores for each of the self-report outcomes was calculated.
User engagement with the SleepSync app
Questions assessing engagement were measured on an 11-point Likert-type scale and assessed by the degree to which the participants’ scores differed from a score of neutral/no change and were only measured post-app use. Scores above 5 (neutral) indicated an improvement, while worse outcomes were indicated by a score below neutral. The following outcomes were used to determine engagement: (i) satisfaction in their ability to manage their schedule; (ii) ease of integration of the app into their daily routine; and (iii) influence of the app on behaviour and habits.
User perception of usability
Usability was assessed on the ease with which participants were able to use key features, as well as the app's functionality, as a sleep and schedule management system. During the semi-structured interview, participants rated how easy or difficult manually entering and editing/changing shifts was in the app, ease of following sleep recommendations, ease of navigating the app and satisfaction with the ability to manage their schedule. Confidence to manage their schedule and satisfaction with the ability to manage their schedule was reported on an 11-point scale (0–10), where 5 was neutral/no change and scores higher than 5 indicated a positive improvement/change. The remaining measures of usability were measured on 5-point scale, where 3 was neutral and scores higher than 3 indicated a positive response.
Secondary outcome measures
Mood and sleep-related impairments
Each of the questionnaires to assess mood and sleep-related impairments was previously validated and included as part of the 65-item online survey.34–37 Mood and sleep-related impairments were included as secondary outcome measures for a positive impact of the app and were assessed by determining the magnitude of change in pre- and post-app use scores on the following self-report outcome measures: (i) sleep hygiene: the degree to which participants practiced healthy sleep behaviours and habits, measured using the Sleep Hygiene Index; 34 (ii) mood: symptoms of depression, anxiety and stress, measured using the Depression Anxiety Stress Scale-21; 35 (iii) insomnia symptoms: the degree of severity of symptoms of insomnia by participants, measured using the Insomnia Severity Index; 36 and (iv) functional impairments, measured using the Patient-Reported Outcomes Measurement Information System: Sleep-related Impairments questionnaire. 37
Statistical analyses
All data are reported as mean ± standard deviation (M ± SD), median or proportion (%); 95% confidence intervals (95% CIs) are also reported (Clopper–Pearson CI for proportions). Where appropriate, paired sample t-tests were conducted to compare mean scores for pre- and post-app use, except where the difference score between paired samples was not normally distributed, in which case a Wilcoxon ranks signed test was conducted. As the usability variables were not normally distributed, a one-sample Wilcoxon signed rank test was conducted to analyze these variables. CTQ variables are reported as absolute values, percentages, means and standard deviations. SPSS Statistics Version 20.0 (IBM, Armonk, New York) was used for all data analysis. The significance level was set at 0.05.
Results
Participant demographics
Demographic information is shown in Table 1. There were a greater proportion of females compared to males. Participants were, on average, aged 36 years, and had 1.5 children. The largest proportion of participants had more than 10 years of shift work experience (55.6%), while there was an equal proportion (22.2%) of those who had between 6 and 10 years or 1–5 years’ experience. All participants were classified as intermediate chronotypes according to the cMEQ, with no morning or evening chronotypes.
Participant characteristics.

Shift work industries: healthcare, law enforcement, manufacturing, retail, construction, laboratory technician and emergency services.
User perception of the SleepSync app
Overall, self-reported total sleep time was significantly higher post-app use compared to baseline, with users reporting 29 min longer total sleep time, on average (P = .04; 95% CI [−1.09, −0.02]). After using SleepSync, participants reported a significant improvement in their ability to fall asleep (average 1.85-point increase; P = .001; 95% CI [−2.95, −0.97]), and quality of sleep (average 2.1-point increase; P < .001; 95% CI [−3.11, −1.11]), compared to prior to app use. The difference between pre- and post-app use for recovery following shift work on days off, however, was not significant (average 1-point increase; P = .19; 95% CI [−2.16, 0.46]). The majority of individuals, however, reported positive changes in recovery (52%), the ability to fall asleep (70%) and quality of sleep (81%). Figure 1 illustrates the differences between pre- and post-app use.

Pre- and post-app use scores for total sleep time, ability to fall asleep, quality of sleep and recovery. Grey bars represent mean scores taken at onboarding, prior to app use; Black bars represent mean scores at end of trial, after two weeks of app use; and error bars represent the standard error of the mean.
User engagement with the SleepSync app
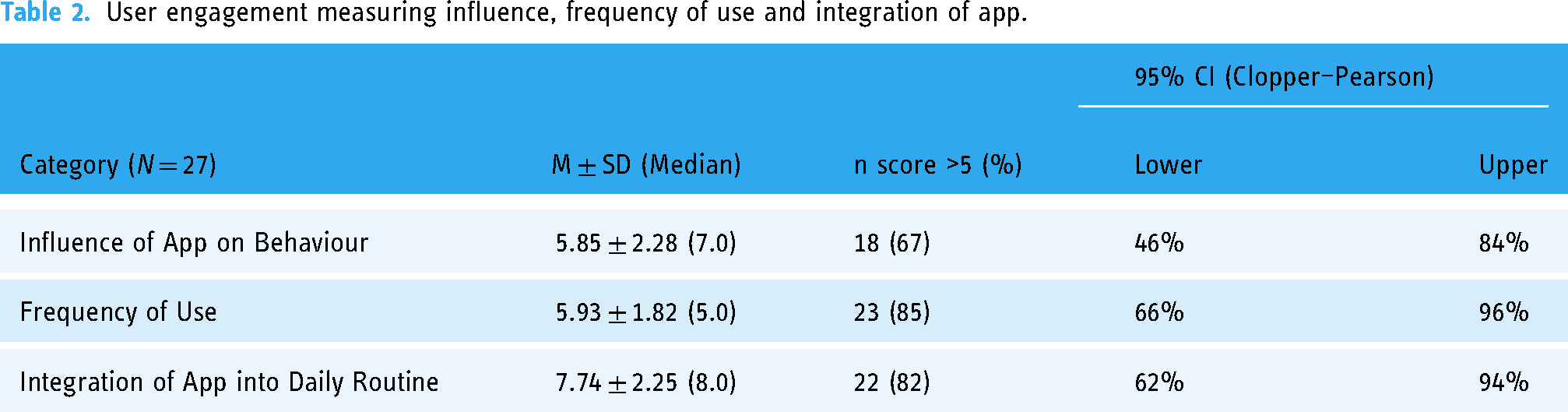
Participants also reported how influential SleepSync was for modifying their behaviour and habits, as well as the ease with which they were able to integrate the app into their lives, and frequency of app use (Table 2). Specifically, 67% of users reported that the app influenced their behaviour (95% CI [46%, 84%]), 85% of users engaged with the app for the right amount of time or more as perceived by the user (95% CI [66%, 96%]), while 82% of users found it easy to integrate the app into their daily routines (95% CI [62%, 94%]).
User engagement measuring influence, frequency of use and integration of app.
User perception of the usability of the SleepSync app
Table 3 shows the number of participants who scored higher than 5 (where 5 is neutral/no change) on an 11-point scale for confidence and satisfaction with schedule management using SleepSync. A score greater than 5 indicates that their confidence and satisfaction with managing their schedule using SleepSync was increased, compared to prior to SleepSync use. The mean confidence score was 6.07 ± 1.38, indicating an overall improvement in confidence with schedule management, although approximately half of the participants (48.2%) had a score greater than 5. Satisfaction with the ability to manage their schedule was greatly improved (mean score 7.51 ± 1.55), with 88.9% of participants scoring higher than 5.
Usability (N = 27).

A one-sample Wilcoxon signed-rank test was used to compare whether median values differed significantly from 5 (11-point scale variables) or 3 (5-point scale variables). Bold values indicate significance <0.05.
Also reported in Table 3 is the number and proportion of participants who scored higher than 3, where 3 is neutral, on the usability of app features. For each of these measures of usability, participants rated maintaining personal events as the most difficult function to complete in the app.
Changes in mood and sleep-related impairments as secondary measures
Secondary outcome measures of the performance of the app were also determined by assessing outcomes for mood (depression, anxiety and stress), insomnia symptom severity, sleep hygiene and sleep-related daytime impairments. There were significant improvements to all measures (P < .05), except depression (P = .07), which showed a trend for improvement. Figure 2 illustrates the pre- and post-app use scores for each outcome.

Mood and sleep-related impairment measures. Grey bars represent mean scores taken at onboarding, prior to app use; black bars represent mean scores at end of trial, after two weeks of app use; and error bars represent the standard error of the mean. *Wilcoxon signed-rank test used to compare whether mean values differed significantly.
Discussion
SleepSync was developed as a tool to assist shift workers in managing their sleep–wake schedules and sleep habits to enhance sleep and health outcomes. The primary objective of the study was to assess users’ perception of SleepSync for recovery, quality of sleep, satisfaction with ability to fall asleep and satisfaction with ability to manage their schedule. Secondary measures included mood and sleep-related impairment outcomes. Recovery, quality of sleep and ability to fall asleep significantly improved during the trial period, suggesting that SleepSync could be an effective tool for improving recovery and sleep outcomes in shift workers. Similarly, there were significant improvements in mood and sleep-related impairment measures, including a reduction in insomnia symptoms, anxiety and stress and an improvement in daytime function. There was a non-significant reduction in the severity of depressive symptoms. Sleep hygiene also improved, suggesting the app modified behaviour directed at improving sleep.
The ability to integrate the SleepSync app into a daily routine and the level of influence the app had on behaviour and habits were assessed to measure user engagement. For each of the engagement measures, over 50% of users rated SleepSync favourably. Users considered SleepSync to be influential on behaviour and habits, easily integrated into their daily routine and satisfactory for managing their work and personal schedules. The influence of SleepSync and ease of integration suggest that users found SleepSync easy to use and relevant to their needs, 27 proving their use as an effective measure of app engagement. Finally, this study examined user perception of app usability, including ability to manually enter and maintain work shifts and personal events into the calendar, ability to follow the sleep recommendations and ability to navigate the app and find features, given these elements are critical to ongoing user engagement. 27 Overall, users indicated that SleepSync was a satisfactory tool for managing their sleep and provided them with increased confidence to manage their schedules. Overall, users felt confident in entering shift details, understanding button functions and navigating the app. Although some features were rated as less easy to operate, users understood the function of these features. Their utility is likely to be improved with simple adjustments to the user interface to enhance operability.
The SleepSync app successfully demonstrated that by assisting shift workers in managing their sleep schedules to prioritize sleep, their self-reported ability to fall asleep, perceived sleep quality and, as a result, the overall perception of recovery on days off, were improved. Elements critical to successful behaviour change techniques in mHealth sleep apps, such as monitoring (daily sleep log) and feedback (recovery score), knowledge shaping (recovery score/sleep hygiene information) and goal planning (recovery score/shift management calendar), 25 were key features of the SleepSync app and likely enhanced sleep outcomes through individual prioritization of sleep. This aligns with previous work in which prioritization of sleep has been shown to improve sleep quality. 38 Sleep disturbances, such as difficulty initiating sleep and obtaining sufficient sleep, are primary complaints of shift workers.39–41 Although this is driven primarily by misalignment of the circadian pacemaker's propensity for sleep and actual sleep and wake times,23,42 it is likely that sleep is also often under-prioritized in preference for social and family commitments, further perpetuating sleep disturbances and the resulting consequences. Prioritization of other commitments over sleep was observed in a study investigating the impact of sleep prioritization on social and family dynamics in shift-working firefighters. 43 Firefighters with a spouse or dependents, a demographic similar to that of the current study, chose social and family commitments over spending time sleeping. In the current study, SleepSync facilitated sleep prioritization by providing feasible sleep recommendations that ensured adequate sleep time that improved sleep quality for the users. SleepSync further facilitated sleep prioritization by providing warnings when work and personal commitments did not allow adequate sleep time. Additionally, while it is not possible to completely eliminate changes in circadian timing, nor the irregularity of bed and wake times due to shift work schedules, sleep recommendations provided by SleepSync may have improved sleep quality and recovery by better aligning sleep–wake timing with the endogenous circadian rhythm. Sleep at an appropriate circadian time is both easier to initiate and more restorative, 42 both of which were self-reported in the relatively small sample of in the present study.
The recommendations for sleep and wake times enabled users of SleepSync to optimize their sleep opportunity, both in terms of the amount and quality of sleep, which may have resulted in a positive effect on mental health and functional outcomes. Sleep and circadian disruption are strongly associated with a number of negative health and functional outcomes in shift worker populations. 7 Beyond acute impairments to alertness and performance, and chronic health complaints and disease, shift work is strongly associated with negative mood and mental health outcomes,12,44,45 as well as increased stress 46 and burnout. 47 A recent longitudinal meta-analysis investigating mental health outcomes in shift workers revealed that shift workers were 30% more likely to experience poor mental health, particularly symptoms of depression. 48 The combination of chronic insufficient sleep and circadian misalignment is likely contributing factors, playing an overlapping mechanistic role in the development and maintenance of mood disorders such as depression and anxiety.39,49–51 The results of the current study suggest that SleepSync mitigated the degree of sleep deprivation by increasing total sleep time and sleep quality, improving mood and functional outcomes.
Finally, in the development of SleepSync, it was recognized that improving sleep–wake outcomes is best achieved through a combination of sleep–wake timing management, as well as interventions aimed at modifying sleep-related behaviour. Good sleep behaviours and habits, referred to as sleep hygiene, have been shown to be a critical factor in determining the risk of SWD in shift workers. 52 Previous research has shown that sleep hygiene education can significantly improve sleep–wake timing, with consequent improvements to sleep quality, 25 in shift working nurses, 19 and female day workers. 20 A recent meta-analysis, however, shows that while sleep hygiene education can improve sleep outcomes, greater improvements are observed with cognitive behavioural therapy for insomnia (CBT-I), which includes sleep–wake timing management. 52 As such, key sleep hygiene behaviour modifications were incorporated into SleepSync, namely the timing of light exposure from mobile devices and caffeine intake, in addition to sleep–wake timing management. These behaviours were reinforced when appropriately enacted by contributing to the overall recovery score. Additionally, SleepSync provided users with hints and tips for healthy sleep behaviours. The improvement in sleep hygiene, as evidenced by a significant reduction in sleep hygiene scores, likely contributes to the improvements observed in sleep and functional outcomes. Furthermore, it reiterates the users’ report that SleepSync significantly positively influenced user behaviour.
This pilot study demonstrates the feasibility and positive impact of a mobile app to improve a number of life outcomes for shift workers; however, there are several limitations. Firstly, at the time of user testing, the app had not been developed for the Android platform, thus excluding a large number of potential participants. User testing was conducted with a small number of participants, reducing the generalizability and reliability of the results, and there was no control group in this pilot study. Furthermore, we acknowledge that although diversifying the sample to include other industries may improve generalizability; this approach could have also increased the variability of the sample. Similarly, there was a gender bias in the sample that may reduce generalizability, although this reflects the proportion of females in the nursing profession in Australia, 29 of which the majority of the current sample was recruited. The results, however, provide sufficient evidence for the utility of the app and the value of conducting a future randomized controlled trial in a larger sample. The short duration of the trial period may also be a limiting factor of the study, particularly for user engagement outcomes. Measuring engagement for a longer duration may provide a better indication of the durability of engagement with the app and its potential for inducing long-term behavioural changes. Furthermore, a number of users had roster changes that occurred during the trial period that for some users reduced the number of night shifts they experienced during the trial. Nonetheless, all participants in the current study reported using the app at least once a day for the two-week duration of the trial. Finally, while outcomes were assessed pre- and post-app use with validated measures, the questions included in the semi-structured interview were developed by the study team and have not been validated. The semi-structured interview, however, was designed primarily to gain key insights for the future development of the app.
The user testing conducted with SleepSync suggests the app is effective in improving sleep and mental health outcomes in shift workers. SleepSync positively influenced user behaviour and was easily integrated into users’ daily routine. Users understood the purpose of the app, its functions and its features. Overall, this trial informs further development of the SleepSync app as a digital intervention to provide individualized management of sleep health among shift workers and supports conducting controlled field trials.
Footnotes
Acknowledgements
The authors would like to thank Brent Bellinger for his contribution to the app development. Michelle Magee is presently affiliated with Centre for Neuroscience of Speech, Department of Audiology and Speech Pathology, University of Melbourne, Australia, in addition to the listed affiliations. Lauren Booker is presently affiliated with La Trobe Rural Health School, La Trobe University, Bendigo, Australia, in addition to the Institute for Breathing and Sleep, Austin Health, Victoria, Australia. Beth Galaska is presently affiliated with KPS Life on assignment at Endo Pharmaceuticals.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Cooperative Research Centre for Alertness, Safety and Productivity and Philips RS North America LLC f/k/a Respironics Inc.