
Abstract
Background
Type II (customer-on-worker) workplace violence (WPV) against nurses and its underreporting are ongoing safety and health challenges in health care. The COVID-19 pandemic has strained patients and nurses and, in turn, may have increased WPV. The purpose of this cross-sectional study was to describe and compare a sample of nurses’ reported prevalence of Type II WPV and their reporting of these events during the pandemic.
Methods
Data from an online survey of registered nurses (N = 373) working in hospitals were included. Prevalence was calculated for physical violence and verbal abuse, and their reporting of these events, including the experience of violence between nurses who did and did not care for patients with COVID-19.
Findings
Overall, 44.4% and 67.8% of the nurses reported experiencing physical violence and verbal abuse, respectively, between February and May/June 2020. Nurses who provided care for patients with COVID-19 experienced more physical violence (adjusted odds ratio [aOR] = 2.18, 95% confidence interval [CI] = [1.30, 3.67]) and verbal abuse (aOR = 2.10, 95% CI = [1.22, 3.61]) than nurses who did not care for these patients. One in 10 nurses felt reporting the incident was more difficult during the pandemic.
Conclusion/Application to Practice
A significant proportion of nurses who cared for patients with COVID-19 experienced more physical violence and verbal abuse, and more difficulty in reporting to management. As the pandemic continues, health care organizations need to recognize that workers may be at an elevated risk for experiencing WPV and may be less likely to report, resulting in an urgent need for prevention efforts on their part.
Background
Workplace violence (WPV) against health care workers has been a persistent problem in the United States (Phillips, 2016) and worldwide for decades (Liu et al., 2019). The most prevalent type of WPV in health care is customer-on-worker (Type II) violence, which is perpetrated by patients, family members, and visitors (Howard, 1996). In 2019, the rate of non-fatal occupational injuries and illnesses from violence by a person in the private health care and social assistance industry, requiring days away from work, was more than 4 times that in all private industries combined (13.6 vs. 2.9 per 10,000 full-time workers; U.S. Bureau of Labor Statistics, 2020a). Nurses experience one of the highest Type II WPV in the U.S. health care settings (U.S. Bureau of Labor Statistics, 2020b) as involved in direct patient care (Pompeii et al., 2015). Workplace violence in the health care setting is compounded by the problem of underreporting incidents to hospital administration, thereby underestimating the magnitude of the problem and reducing efforts to control the hazard (Arnetz et al., 2015; Byon et al., 2020; Pompeii et al., 2016).
The COVID-19 pandemic has physically and psychologically strained hospitalized patients, their families, health care personnel, as well as the overall health care system (Blumenthal et al., 2020; Luttik et al., 2020; Shreffler et al., 2020). Patients hospitalized during the COVID-19 pandemic exhibited fear for the disease prognosis, stress from quarantine measures, and emotional/behavioral changes (e.g., anger, anxiety, aggressive languages; Sun et al., 2021). Nurses suffered from anxiety, work pressure, staff shortage, and lack of peer and organizational support during the pandemic (Arnetz et al., 2020; Karimi et al., 2020; Maben & Bridges 2020). These vulnerable conditions may compound the already high rate of WPV and its underreporting. For example, unmet patient health care needs/requests have been shown to be a risk factor for Type II violence (Najafi et al., 2018), and it is likely that these may have been aggravated because of staffing shortages and decreased hospital capacity during the COVID-19 pandemic. Globally, there have also been reports of frontline health care workers including nurses being attacked by perpetrators because of fear, panic, misplaced anger, and misinformation (McKay et al., 2020). Moreover, insufficient time and support during patient care in the pandemic may heighten the threshold for nurses to overcome when reporting Type II WPV.
There have been no studies that examined how the COVID-19 pandemic affected the prevalence of Type II WPV and its reporting practice. To understand this, first, we described Type II WPV among registered nurses (RNs) during the COVID-19 pandemic. Second, we compared the prevalence of Type II WPV between RNs who provided care for patients with COVID-19 and those who did not. Finally, we described whether the nurses experienced more Type II violence and more challenges in reporting the violence during the COVID-19 pandemic than before the pandemic.
Methods
Study Design and Recruitment
This cross-sectional study of Type II WPV was part of the online SAFE-CARE survey conducted between May 27, 2020, and June 25, 2020 (Sagherian et al., 2020). The anonymous survey was developed to understand insomnia, work-related fatigue, psychological well-being, and Type II WPV among hospital nursing staff in the United States during the COVID-19 pandemic. The analyses for this article focused on Type II WPV among RNs. With a convenience sampling approach, participants were recruited from online social media outlets that included Twitter, Facebook, and LinkedIn. The link to the survey was embedded on each outlet, and a short invitation message included hashtags such as #nurse, #sleep, #fatigue, #wellbeing, and #Covid19. In addition, the researchers sent emails to their colleagues in the nursing profession to share the recruitment flyer with other nurses (i.e., snowball sampling). Social media are shown to provide accessible, low-cost, high-yield approaches to the recruitment of nurses for survey study (Bethel et al., 2021). Nursing staff who were on a vacation or maternity leave or had a nursing administration or leadership role were excluded. The study was approved by the reviews of Institutional Review Board at the University of Virginia, University of Tennessee, Knoxville, and the University of Wisconsin–Madison.
Measures
Demographics and occupational characteristics
These items included age (≤30, 31–40, 41–50, and ≥51 years), sex (male and female), race (White, Black, Asian, and Other), years of work experience (≤2, 3–8, 9–14, and ≥15), work unit (emergency department, intensive care, medical-surgical, and other), and residence regions based on the United States Census Bureau designation (Northeast, Midwest, South, and West).
WPV
Type II WPV was measured by two items. The first asked about physical violence as follows: “In the few months since the COVID-19 pandemic started, how often have you been physically attacked (for example, hitting, pinching, biting, scratching, choking, hair-pulling) by your patients or their visitors/family members?” The second asked about verbal abuse as follows: “In the few months since the COVID-19 pandemic, how often have you been verbally abused (for example, cursing, yelling, name-calling, insulting) by your patients or their visitors/family members?” Response options to both questions were as follows: none, once, 2 to 3 times, 4 to 5 times, and more than 5 times. The respondents were also asked, “Since COVID-19, have you experienced more violence from your patients or their visitors/family members than before COVID-19?” (yes, no, never experienced violence). The final question asked, “Since COVID-19, has it been more difficult for you to report such a violent incident to management than before COVID-19?” (yes, no, never experienced violence). Because the pandemic was recognized at different times in different parts of the United States in early 2020, we intentionally did not specify the start date of the pandemic period in the survey. Thus, these questions refer to nurses’ experiences in the past 5 months (February to May or mid-June 2020) of the pandemic.
Care of COVID-19 patients
One survey item asked whether nurses provided care for any known patients with COVID-19 (yes, no).
Statistical Analyses
Descriptive statistics (counts and percentages for categorical variables) were computed for all survey items. Chi-square tests or Fisher’s exact tests were performed for bivariate comparisons of the proportions of Type II WPV between the RNs who provided care for patients with COVID-19 and those who did not. Results of logistic regressions (adjusted odds ratios [aORs] and 95% confidence intervals [CIs]) were reported to describe the difference in the odds of experiencing Type II WPV between the two groups of RNs while adjusting for covariates. Finally, we computed proportions of the RNs who experienced more Type II violence and more challenges in reporting the violence during the COVID-19 pandemic than before the pandemic. In all analyses, we used a pairwise deletion approach (available-case analysis) rather than listwise deletion (complete-case analysis). Therefore, some subsample sizes varied by analysis. STATA Version 13 was used for all statistical analyses.
Results
Of the 384 RNs who participated in the survey, 373 completed the violence and the care for COVID-19 questions (N = 373). Table 1 shows the demographic and occupational characteristics of the RNs and their experience of WPV. More than half (62.7%) of the nurses were 40 years old or less (M = 38.3, SD = 10.8). The sample was predominantly female (94.4%) and White (90.3%), and had at least 3 years of nursing experience (85.5%) (M = 5.0, SD = 2.5). More than half (66.2%) worked in either the emergency department, a medical-surgical unit, or an intensive care unit. More than three quarters (81.7%) resided in the Midwest or South region. There were significant differences in the proportions of work units and regions between the groups of RNs who took care of COVID-19 patients and those who did not. The largest portion of the RNs who cared for the COVID-19 patients worked in intensive care units (32.4%), while the other group of RNs worked in other units (44.7%) than the emergency department, intensive care, or medical-surgical. The biggest portion of the former group of RNs resided in the South region (44.6%), while the other group of RNs resided in the Midwest (53.7%). The majority (n = 250, 67%) of RNs reported taking care of patients with COVID-19 at least once.
Characteristics of Registered Nurses and Their Experience of Type II Violence, Stratified by the Care Status for COVID-19 Patients (N = 373)
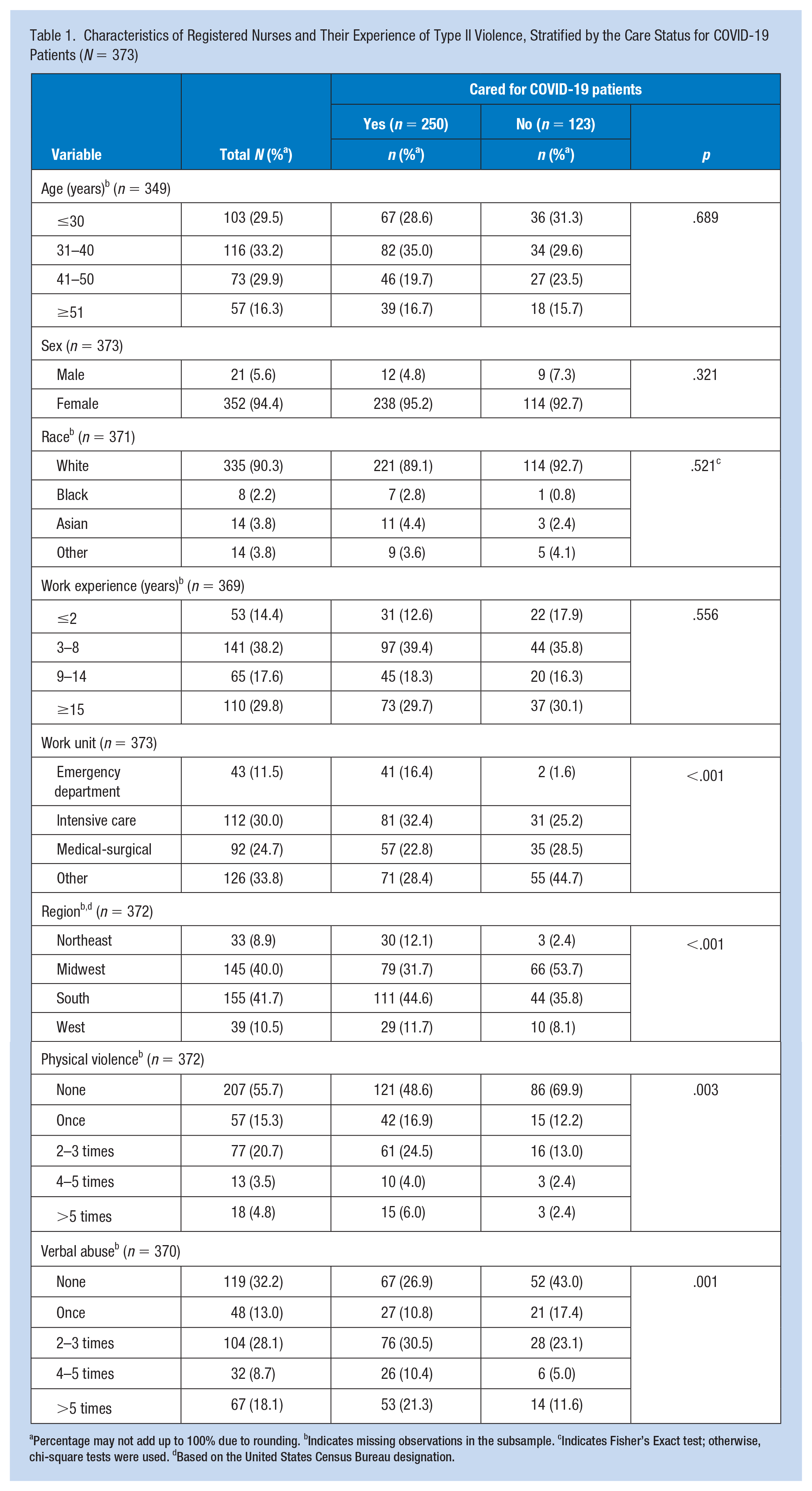
Percentage may not add up to 100% due to rounding. bIndicates missing observations in the subsample. cIndicates Fisher’s Exact test; otherwise, chi-square tests were used. dBased on the United States Census Bureau designation.
During the pandemic, 44.4% of the RNs reported experiencing physical violence at least once from their patient, visitors, or family members. Among this group, those who experienced it 2 to 3 times were most frequent (20.7%). Two thirds (67.8%) of the RNs experienced verbal abuse at least once during the pandemic. Those who experienced it 2 to 3 times were most frequent (28.1%). Furthermore, RNs who provided care for patients with COVID-19 reported experiencing significantly more physical violence than those who did not (p = .003). Over half (51.2%) of the former experienced physical violence at least once, while 30.1% of the latter experienced it. Also, RNs who took care of patients with COVID-19 experienced significantly more verbal abuse than those who did not (p = .001). Seventy-three percent of the former experienced verbal abuse at least once, while 56.1% of the latter experienced it.
Logistic regressions showed that the odds of experiencing physical violence (aOR = 2.18, 95% CI = [1.30, 3.67]) and verbal abuse (aOR = 2.10, 95% CI = [1.22, 3.61]) were statistically higher among those who cared for patients with COVID-19 than those who did not, while adjusted for age, sex, race, work experience, work unit, and residence region (Table 2). Among 270 RNs who experienced any type of WPV, 27.4% (n = 74) reported having experienced more violence during the pandemic than they did previously. A smaller percentage (9.5%, n = 31) of 326 RNs responded that reporting the violent incident to management was more difficult during the pandemic than before.
Logistic Regression Models of Experiencing Violence At Least Once in Registered Nurses and Their Care Status for COVID-19 Patients (N = 373)
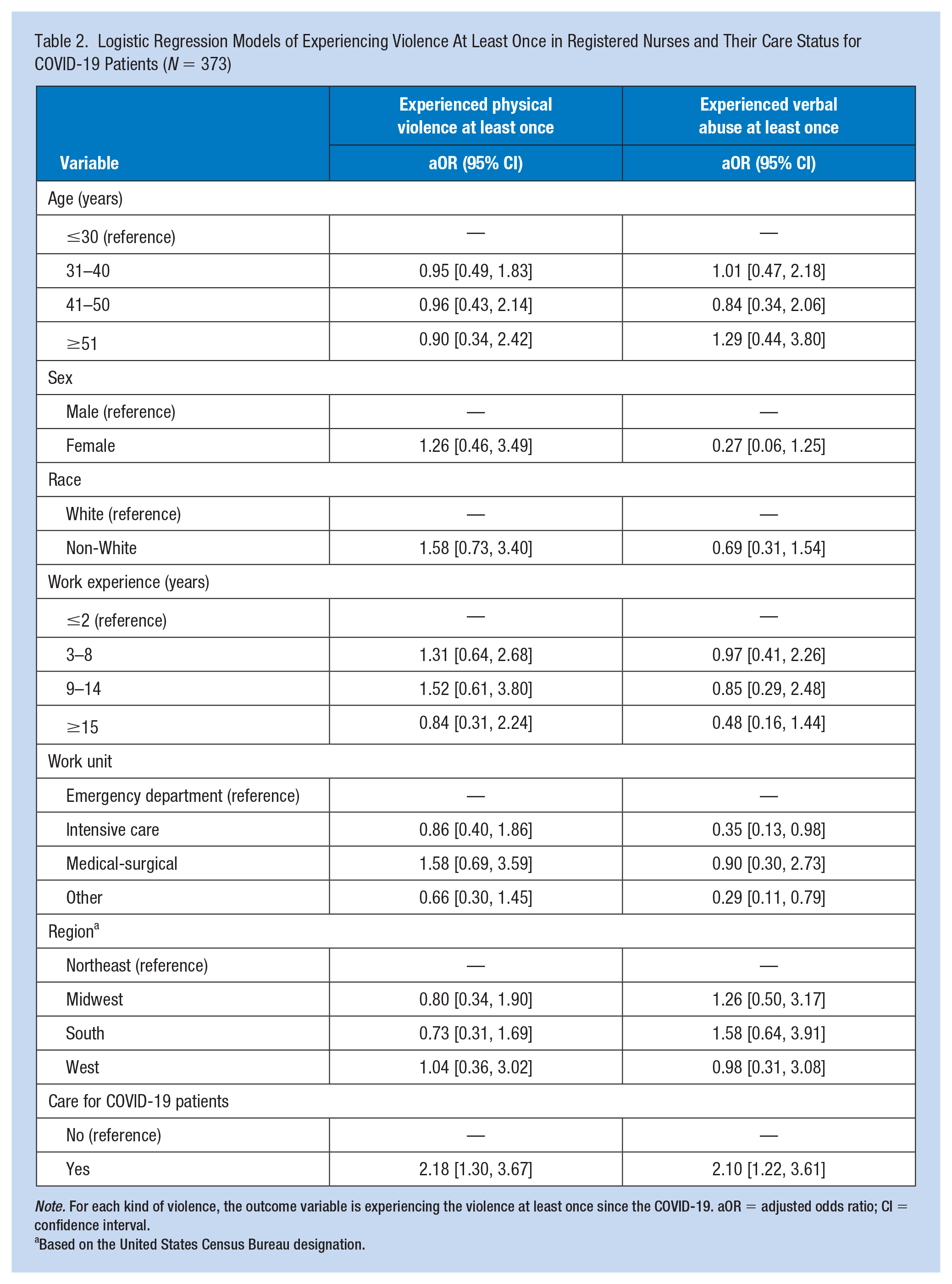
Note. For each kind of violence, the outcome variable is experiencing the violence at least once since the COVID-19. aOR = adjusted odds ratio; CI = confidence interval.
Based on the United States Census Bureau designation.
Discussion
We found that during an approximately 5-month period at the beginning of the COVID-19 pandemic in the United States, 44% and 68% of the RNs in our study reported experiencing Type II physical violence and verbal abuse. Incidents of both types of violence were significantly higher among the RNs who cared for patients with COVID-19 than those who did not. Also, approximately one fifth of participants reported having experienced more violence during the pandemic than they did before.
The high reported prevalence of physical violence (hitting, pinching, biting, scratching, choking, hair-pulling) toward nurses during the pandemic is especially troubling and a great concern for their safety. In their meta-analysis, Liu et al. (2019) found, annually, 26.8% and 44.9% of nurses worldwide experience physical and non-physical violence, including verbal abuse and other non-physical violence perpetrated against them. Pompeii et al. (2013) reported in their review of the year 2000–2010 literature that 2% to 32% and 22% to 90% of hospital workers, including nurses and other professions, experienced Type II physical violence and verbal abuse, respectively. These findings are not exclusive to the United States or verbal abuse (Liu et al., 2019) or nurses (Pompeii et al., 2013). Therefore, a direct comparison of our results with them warrants some caution. Nevertheless, the higher reported prevalence from our study—44% and 68% for physical violence and verbal abuse, respectively—seems to indicate that Type II violence toward RNs has likely increased during the pandemic. Furthermore, the percentage of RNs having experienced physical violence and verbal abuse would likely be higher in our study if we asked their experience for the past 1 year as most of the prior reported studies have done.
We found an overall increase, as well as disproportionate inflation in the reported prevalence of Type II WPV among the RNs who provided care for COVID-19 patients during the early months of the pandemic. During the COVID-19 pandemic, hospitals in the United States experienced a drastic reduction in patient admissions (Birkmeyer et al., 2020). This likely reduced the number of encounters between nurses and patients, visitors, and family members, the main source of Type II violence. However, our study showed that more than one quarter (27.4%) of the RNs experienced higher numbers of Type II violence during the pandemic than before. Importantly, RNs who provided care for patients with COVID-19 experienced 118% more physical violence and 110% more verbal abuse than those who did not provide such care. Although the reasons are uncertain, there are possible explanations. First, hospital requirements that severely limited or prohibited visitors or tightened visit conditions (Virani et al., 2020) may have led to patients expressing their anxiety and frustration toward nurses in the form of violence. Although these policies reduced the number of visitors, they likely created or increased patient frustration and anger that led to an increase of Type II violence toward nurses. In addition, nurses who worked in a more stressful and tiring environment due to increased patient to nurse ratio (Maben & Bridges 2020) and job requirements (e.g., longer work hours, irregular shift type, the laborious procedure of donning personal protective equipment for protection) may have experienced increased agitation, fatigue, and burnout, which may have made them more vulnerable to Type II violence. Finally, a lack of resources at the hospital organization level and especially on the units where nurses required more resources for the care of COVID-19 patients (e.g., reduced security staff, lack of administrative support for violence prevention due to increased attention to patient care) may have contributed to an increased number of violent incidents.
The reported increased experience of Type II WPV during the COVID-19 pandemic (e.g., nearly 45% of RNs in our study reported experiencing physical violence) and intensity (e.g., 18% reported they experienced verbal abuse more than 5 times over 5 months) is a great threat to the safety and health of the nurses. Nurses are already under a great burden for providing health care to patients during the pandemic. The constant fear of getting infected, high levels of stress, and feelings of helplessness and distress watching infected patients deteriorate and die alone are risk factors for suicide among health care professionals (Thakur & Jain, 2020). Additional strain from WPV may further exacerbate risks to nurse health and well-being during this extremely stressful and tiring period. Victims of WPV experience serious negative consequences, including threats to physical and personal safety (e.g., injury), psychological (e.g., posttraumatic stress, depression), emotional (e.g., anger, fear), work functioning (e.g., sick leave, job satisfaction), relationship with patients, quality of care, social/general (e.g., disturbed social and family life), and financial (e.g., treatment cost, loss of work time) aspects of health and well-being (Lanctôt & Guay, 2014). Proper attention needs to be paid to the heightened prevalence and prevention of WPV toward nurses who are critical in providing health care to the sick during a health care crisis.
One out of 10 (9.5%) RNs in this study expressed more difficulty in reporting the violent incident to management during the pandemic than before. Studies in various health care settings have shown that barriers of Type II WPV reporting include lack of time to report; belief that violence is part of the job; unstandardized reporting process; ambiguity on the reportability of violence, including an unclear definition of violence; and lack of management support (Byon et al., 2020; Pompeii et al., 2016; Sato et al., 2013). It is likely that some of these factors for underreporting may have been elevated during the pandemic and become more challenging. For example, nurses may have worked in a busier, tighter schedule during the pandemic and did not have the capacity to report violent incidents to the management. The harmful but pervasive belief that violence is part of nursing may have solidified during the pandemic, and the nurses might have felt that they had to provide compassionate health care to the sick, even to those whose behaviors were violent. And the nurses might have found it difficult to report violent behaviors, rationalizing such behaviors were possibly related to the frustration the pandemic had put on their patients, and they were obliged to tolerate and not report them (Byon et al., 2020). The pandemic also restrained the support and resources that management could utilize, thus adding challenges for nurses to report violent incidents. Workplace violence can be prevented more effectively if violence is reported and analyzed at an earlier stage (Occupational Safety and Health Administration [OSHA], 2016a). The identification of risk factors for WPV can lead to various types of hazard control measures that will keep patients and staff safer and ultimately improve patient care. The time to prevent WPV is especially crucial during these difficult times.
We recognize that our study describing Type II WPV toward nurses during the pandemic has several limitations. First, non-random sampling limits the generalizability of the findings to the national level. The high proportion of White nurses in our sample (90%) limits our ability to examine if and how race may have modified our results, and our study underestimates the experience of minority nurses. Also, selection bias may have occurred in recruiting nurses that used social media, as this group may have characteristics that differ from non-users. However, our intention was not to produce national descriptive statistics but provide a description of Type II WPV that is not limited to a specific region. Second, the data were based on self-reporting, which may lack objectivity of the survey responses. Finally, given the social-media-based sampling design, we are unable to estimate a response rate to our survey.
Implications for Occupational Health Practice
We found that a significant portion of hospital nurses reported experienced more physical violence and verbal abuse from patients, visitors, and family members during the pandemic than before. More RNs who provided care for patients with COVID-19 experienced such violence than those who did not. Nurses need to be aware that patients, visitors, and family members can get frustrated and angered from the uncertainty of their care and hospital policies that tighten visit conditions and express their feelings in the form of violence toward frontline workers such as nurses. Hospital managers and administrators need to identify, develop, and implement a Type II violence prevention plan for a public health event such as a pandemic when organizational, human, and financial resources can become significantly short. Reducing Type II WPV is crucial to protect nurses, an indispensable health care workforce, especially during a health system strain, such as the COVID-19 pandemic. Improving reporting is an essential step to accurately assessing the severity of WPV and developing WPV prevention interventions and policies. Also, studies can be conducted to investigate and establish the reasons for increased violence incidents and underreporting. The negative effects of these increased reported rates of WPV on nurses’ health, well-being, and satisfaction will likely continue, and organizations need to closely monitor the safety and stress, and psychological well-being of their nursing workforce. Essentially, the impacts of this increase in WPV are likely to extend beyond the pandemic in terms of the toll they take on nurses.
Fundamentally, the COVID-19 pandemic has revealed critical gaps in State and Federal laws and policies designed for protecting health care workers from WPV, as well as other job hazards, most notably infectious diseases. Voluntary OSHA Guidelines for preventing WPV for health care and social service workers were first issued in 1996, updated in 2004, with the most recent revised Guidelines issued in 2016 (OSHA, 2016a), along with a directive for compliance officer inspections of health care organizations that expose workers to WPV (OSHA, 2017). As the “voluntary” guidelines are only “advisory in nature and informational in content” (OSHA, 2016a), there is a concern that necessary protection is failing our healthcare workers, especially during a national pandemic when hospitals’ capacity to comply with the guidelines is already strained. Legal obligations are desired to protect health care workers from exposure to WPV.
Our findings support the recent federal policy initiatives directed at WPV that specifically offer protections for all workers related to the COVID-19 pandemic. In 2016, OSHA issued a Request for Information (RFI) soliciting information on the issue (OSHA, 2016b) and announced they would develop a federal standard to prevent WPV in the health care and social service settings (OSHA, 2021, April 28). U.S. House of Representative Joe Courtney introduced H.R.1309 (Workplace Violence Prevention for Health Care and Social Service Workers Act, 2019), which would direct the Secretary of Labor to issue an occupational safety and health standard requiring covered employers within the health care and social service industries to develop and implement a comprehensive WPV prevention plan. In addition, OSHA’s long-awaited emergency temporary standard on COVID-19 to secure additional precautions for health care workers was submitted to the White House Office of Management and Budget for review on April 26, 2021. Both of these regulations are critically important to protecting health care workers from the hazard of WPV.
Applying Research to Occupational Health Nursing Practice
This study found that, during the COVID-19 pandemic, 44% and 68% of the sample nurses experienced physical violence and verbal abuse from their patients, visitors, and/or family members, which may be higher than those during the pre-pandemic period. Nurses who cared for patients with COVID-19 experienced more violence than nurses who did not. Hospitals cannot abandon workplace violence (WPV) prevention efforts during high stress times such as the COVID-19 pandemic. Health care organizations need to work with their workers including nurses to adapt and strengthen prevention strategies in the workplace and improve incidence reporting. The need for protecting health care workers has been heightened during the pandemic challenges, and these proposed solutions can help us provide a safe and healthful workplace to better protect our caregivers.
Footnotes
Author Contributions
H.D.B., K.S., and L.S. designed this study; H.D.B. and Y.K. conducted the literature review; H.D.B. and K.S. conducted statistical analyses; H.D.B., K.S., Y.K., J.L., M.C., and L.S. interpreted findings; H.D.B., K.S., and Y.K. drafted the manuscript; and J.L., M.C., and L.S. revised it critically for important intellectual content. All authors approved the final manuscript for publication.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Ha Do Byon, PhD, MPH, MS, RN, is an assistant professor at the University of Virginia School of Nursing.
Knar Sagherian, PhD, RN, is an assistant professor at the University of Tennessee, Knoxville College of Nursing.
Yeonsu Kim, BSN, RN, is a PhD student at the University of Virginia School of Nursing.
Jane Lipscomb, PhD, RN, FAAN, is a retired professor of nursing and medicine at the University of Maryland, Baltimore.
Mary Crandall, PhD, RN, is the director of Continuum Home Health Care and Home Infusion Therapy Services at the University of Virginia Health System.
Linsey Steege, PhD, is an associate professor at the University of Wisconsin–Madison School of Nursing.