
Abstract
Background
Nurses and nursing students are increasingly vulnerable to workplace violence, both verbal and physical, as health care settings and clients cope with unprecedented challenges including the COVID-19 pandemic. Concurrently, clinical learning opportunities for nursing students have been curtailed by public health restrictions and limited capacity. While virtual simulations have been promoted as an alternative to clinical hours, their effectiveness as an educational intervention on workplace violence has yet to be assessed.
Purpose
The authors sought to evaluate a virtual, simulated code white—a set of organized responses to a client, visitor, or staff member exhibiting the potential for violence—involving 4th year undergraduate nursing students, randomly sorted into an intervention group and a control group.
Methods
Pre and post test measures of knowledge and attitudes about mental health, workplace violence and virtual simulation were collected, as well as qualitative data from focus groups.
Findings
While the sample size (n = 24) was insufficient to detect meaningful differences between the intervention and control groups, descriptive statistics and focus group data revealed significant gaps in participants’ knowledge around managing workplace violence. Participants rated the virtual simulation highly for its realism and the opportunity to experience working in a virtual environment, while they felt the preamble and debrief were too short.
Conclusions
The findings illustrate a virtual code white simulation has clear educational benefits, and that multiple iterations, both virtual and in person, would most likely increase the benefits of the intervention.
Keywords
Introduction
Workplace violence is a significant and growing concern for healthcare administrators, policymakers and researchers. Healthcare workers face greater odds of experiencing violence at work than police officers or prison guards (ICN, 2021). It is estimated one half of all healthcare workers may be assaulted at some point in their careers, with nurses being three times more likely to experience violence than any other health care group (Brophy et al., 2018; Havaei et al., 2020; Somani et al., 2021). Nursing students are more vulnerable still, by virtue of their liminal status and level of experience (Martinez & De Oliveira, 2021).
Code white refers to a set of organized responses to a client, visitor, or staff member exhibiting extreme agitation and/or indicating the potential for aggression, violence, or immediate risk of bodily harm to themselves or to others (CAMH, 2013). This article reports on the development, implementation, and evaluation of a virtual, simulated, code white learning experience, designed to prepare undergraduate nursing students to address aggression and violence related to a mental health crisis.
Background
In Canada, occupational safety for nurses has attracted national media attention in recent years (Roussy, 2018). Workplace violence in clinical settings can take the form of psychological and physical abuse, intimidation and aggression (Mento et al., 2020), and it is most commonly encountered when caring for patients experiencing mental health concerns (Iozzino et al., 2015; Mento et al., 2020). One in five acute psychiatric inpatients may act out violently (Iozzino et al., 2015). In emergency departments, perceived waiting times and lack of communication may result in aggression (Angland et al., 2014). Multiple stressors arising from the COVID-19 pandemic have compounded these instances of violence (Devi, 2020; Taylor, 2020). This is demonstrated by the reporting of of over 600 violent incidents directed at healthcare workers during the first five months of the outbreak (ICRC, 2020). As instances of violence have increased (Devi, 2020; Havaei et al., 2020), so too have instances of anxiety, depression, anger, and guilt amongst healthcare professionals (Mento et al., 2020).
Under these increasingly volatile circumstances, nurses and nursing students require active learning strategies to build their awareness of this issue and the capacities to respond (Havaei et al., 2019). Educational interventions need to be developed in relation to specific organizational contexts, contributing factors, prevention and de-escalation interventions, and ethically-informed policies (Irwin, 2006). Nursing students in particular must learn resiliency skills to cope with workplace aggression and violence (Hopkins et al., 2018); however, the intervention studies necessary to guide evidence-based practice in this area are lacking (Taylor & Rew, 2011). Nursing organizations in Canada may express zero tolerance for violence against nursing students (RNAO, 2008), but only evidence-based, active learning initiatives can empower this vulnerable cohort to better protect itself.
Enhancing safety through simulation
Simulation is a pedagogical tool wherein actual or potential clinical events are replicated in a controlled environment to develop participants’ performance, knowledge and attitudes through realistic experience (INACSL, 2016; Lioce, 2020). In global healthcare education, patient simulation is widely employed to improve critical thinking skills and professional competencies. Simulations are also utilized to enhance the safety of patients and learners in clinical settings (CPSI, 2021).
Virtual simulation is defined as any interactive, educational process in which learners engage with screen-based systems that simulate real patients or clinical situations (Cant et al., 2019), and is used to improve knowledge retention, clinical reasoning and learner engagement, in line with other simulation strategies (Cant & Cooper, 2014; Padilha et al., 2019; Shin et al., 2019; Verkuyl & Hughes, 2019). In the wake of the global COVID-19 outbreak and the resulting pressure on health human resources and infrastructure, the Society for Simulation in Healthcare (SSH) and the International Nursing Association for Clinical Simulation and Learning (INACSL) have advocated for the substitution of clinical hours for healthcare learners with virtual simulation alternatives, citing the effectiveness of the latter in supporting clinical learning objectives (INACSL & SSH, 2020).
A 2017 pilot study, “Mental Health Nursing Simulation on Workplace Violence,” determined that simulations have the potential to raise nursing students’ confidence and knowledge about managing agitated psychiatric patients (Martinez, 2017). Beyond this, there is little knowledge available on the efficacy of simulated learning activities—whether in person or virtual—in preparing nursing students to manage violence in clinical settings. The study reported below investigated the views of nursing students on simulation, their experiences in participating in a simulated code white, and the potential effect of the simulation on their knowledge and attitudes towards workplace violence and mental illness.
Methodology
Objectives
The authors planned a controlled, randomized trial of a virtual, simulated code white learning experience for undergraduate nursing students, sorted randomly into experimental and control groups. The study compared a simulated code white scenario (intervention) with standard nursing curriculum (comparator). Pre and post test measures were planned to gather data pertaining to students’ attitudes, knowledge and awareness on workplace violence, mental illness, and taking part in the simulation. Two focus groups were carried out in order to provide contextual, qualitative data. The authors sought to answer the following research questions:
What is the impact of a simulated learning experience on awareness and knowledge about workplace violence among undergraduate nursing students? What are the attitudes of undergraduate nursing students towards the code white simulated learning experience? What is the impact of the simulation on attitudes toward mental illness among the undergraduate nursing students? What are the students’ views on and experiences in participating in the simulation?
While the initial study design was based on in-person simulations, the global COVID-19 outbreak necessitated a redesign, and resubmission for ethics approval, based on virtual simulations in line with recommended learning protocols during the pandemic. Qualitative content analysis (QCA), an atheoretical approach often used in nursing research (Forman & Damschroder, 2007), was deemed most appropriate for the focus group component of the data. The quantitative data were analyzed using descriptive statistics.
Recruitment and participants
The researchers used a convenience sample of 4th year undergraduate baccalaureate nursing students, randomly assigned to an intervention group and a control group. Inclusion criteria were completion of the third year undergraduate Mental Health & Wellness course, comprising knowledge, skills and practice applications such as: assessment of risk, decision-making, verbal de-escalation, personal safety, debriefing after an incident, and code white. No exclusion criteria were necessary. A Graduate Research Assistant (GRA), who had no prior connection to the participant cohort, circulated a short video message via the campus listserv, briefly describing the study and how to sign up.
Twenty-three students self-identifying as female, and one self-identifying as male (n = 24) agreed to take part. Using a random number table, the GRA manually allocated 14 participants to an intervention group that would undergo the simulated learning experience, while the remaining 10 comprised a control group that would not. Throughout the study, all participants followed their normal 4th year nursing curriculum. Members of the control group were given the opportunity to undergo the code white simulation once data collection was complete.
Ethics
Prospective participants were provided access to the study website, where they were able to view the project information letter and provide electronic, informed consent. The site automatically assigned each participant a project ID number; at no time did the research team have access to the participants’ personal information. Pseudonyms are employed in this article and all other project output.
Intervention
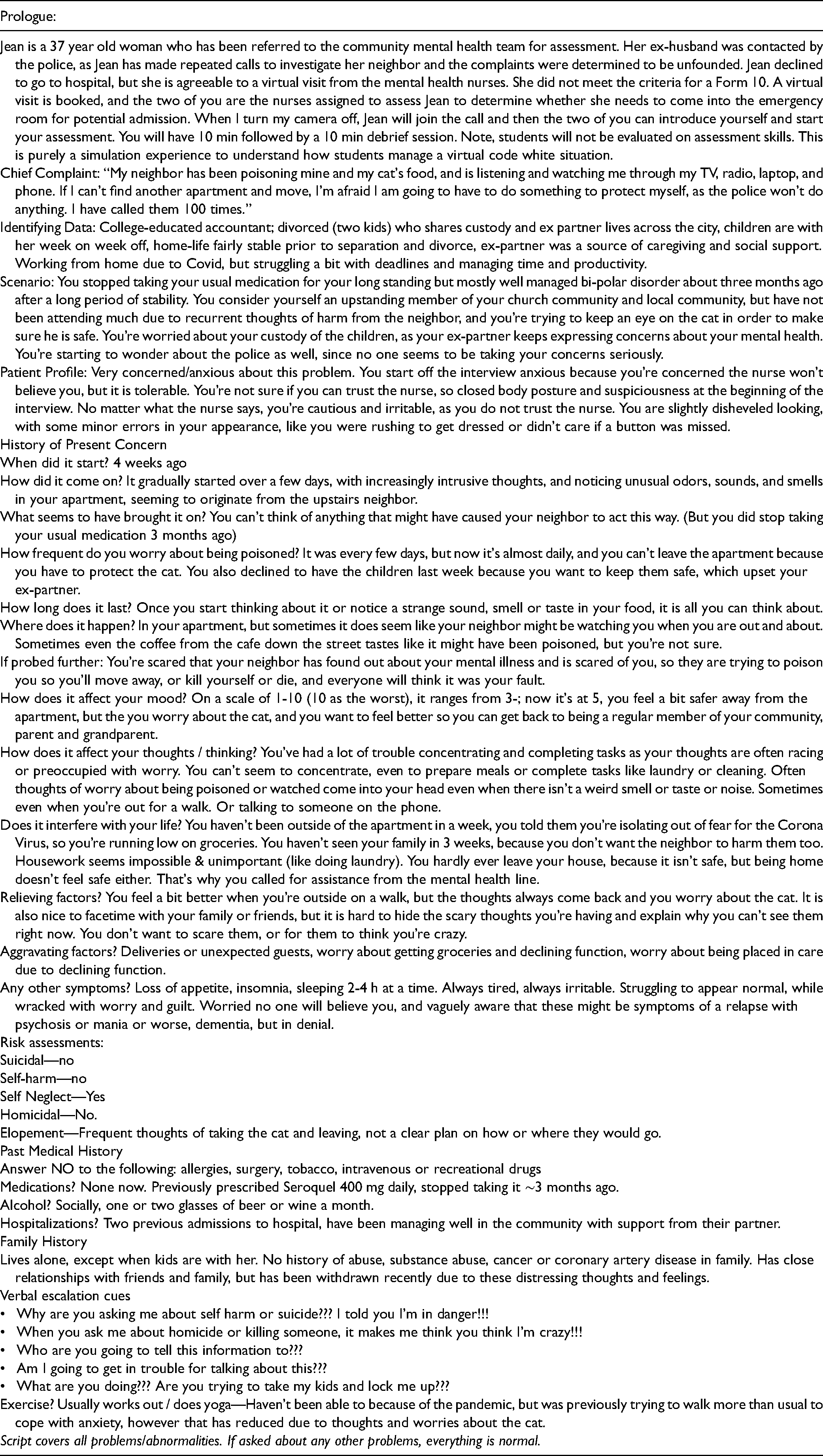
The intervention group progressed through the management of a virtual mental health crisis situation, conducted via Zoom™. This involved a virtual mental health care visit with a community member, played by a trained actor in the role of a standardized patient (SP), who would be the subject of a mental status assessment. The SP escalated verbally through the stages of a crisis, obliging the participants to employ de-escalation skills learned in the course of their undergraduate nursing studies. The scenario, based on actual clinical experiences of the research team, involved only verbal violence (See Table 1).
Standardized patient script.
The simulation adhered to existing practice standards such as confidentiality around the simulated learning experiences, fictional contracts, commitment to respect, and professional communication with others. Participants underwent the simulation in pairs, overseen by a research team member. Prior to undergoing the simulation, participants were given a brief preamble on the process, and advised they could stop the simulation or ask the research team member to intervene at any time.
Each simulation lasted 10–15 minutes, and each was followed by a 10–20 minute debrief with a team member specializing in mental health nursing practice. The Plus Delta simulation debriefing model (Cheng et al., 2021) was chosen as it prompts learners to reflect on the entire simulation scenario and assess their learning experience and performance. This model is a simple and effective way to facilitate reflection and application of learning to future clinical practice. Critical Incident Stress Debriefing (Mitchell & Everly, 2001) was moreover offered to all learners, in the event they felt overwhelmed by the simulation. Field notes were taken during the debriefs in order to ensure the fidelity and consistency of the intervention.
Data collection
Prior to the intervention, the intervention and control groups completed: (1) a brief survey collecting demographic information, previous experience with violence and aggression management training, and exposure to violence in any nursing setting; (2) workplace violence awareness and knowledge measures (Brann & Hartley, 2017); (3) five Likert items, developed with reference to Allen (1986), measuring attitudes towards simulation (ATS); and (4) the Community Attitudes to Mental Illness scale (Taylor & Dear, 1981). All data were submitted using the campus online content management system (CMS). Immediately after the simulation, intervention group members (n = 14) repeated the latter three measures, also using the CMS.
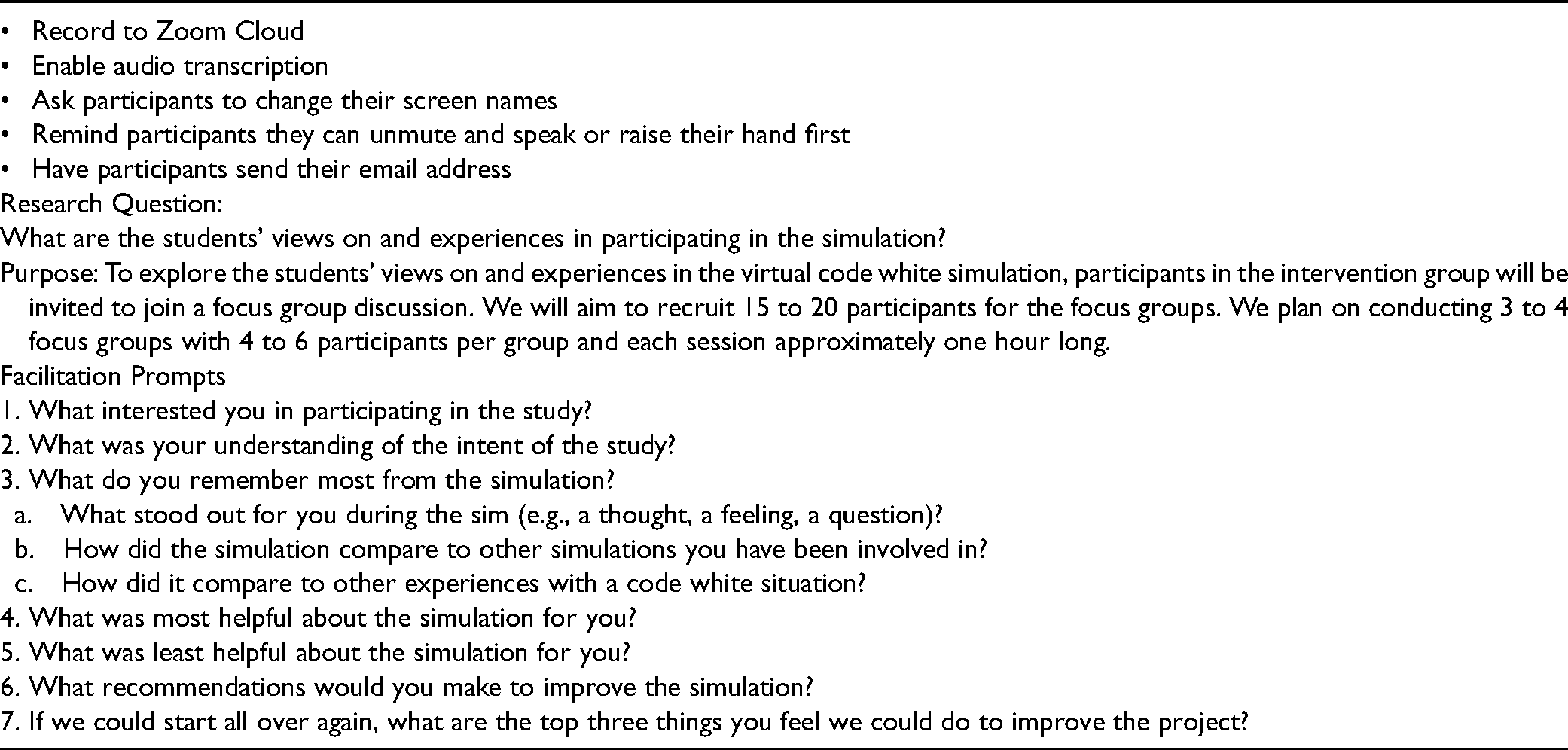
Two 60-min, online focus groups were held in early July, 2021, moderated by the Principal Investigator and two research assistants, to explore the intervention group participants’ views and experiences of participating in the virtual code white simulation. Four participants took part in the first focus group (n = 4), and two in the second (n = 2), based on interest and availability to participate; no other inclusion criteria were set for the focus groups. Discussions were directed according to a focus group guide (See Table 2), developed iteratively throughout data collection. The discussions were video-recorded using Zoom, and transcribed for analysis.
Focus group guide.
Data analysis
Pre- and post-test survey data were analyzed using the SPSS statistical package. Descriptive statistics were used to summarize and describe the data. The intervention and comparator group outcomes were compared using independent groups t-tests for measures on interval scales, and paired t-tests to compare mean pre and post intervention scores. An alpha level of p < .05 was considered statistically significant.
For the focus group data, the authors employed QCA—that is, describing and summarizing the characteristics of the textual content while staying close to the data to prevent the analysis from becoming overly abstracted (Mayan, 2016; Vaismoradi et al., 2013). Transcripts were coded by a research assistant using Nvivo 1.5 software. Twenty-nine codes were initially identified. Through iterative feedback and revision, the team produced a final list of 15 codes.
The final codes were further analyzed and organized into categories, based on intrinsic patterns and similarities (Vaismoradi et al., 2013). These categories, the largest units of analysis within the study, constituted its preliminary findings. The categories were: Views on simulation design; Experiences of virtual modality of the sim; Views on Nursing education (code whites, tele-health); Learning experiences and perceptions of the simulation; and Pre-simulation context (students’ understanding, experience, and motivation). Given that the purpose of the focus groups was to understand participants’ experiences of the code white simulation, QCA provided a rich, inductive description and summary that closely reflected what participants shared in the focus groups (Vaismoradi et al., 2013).
Validation
The researchers maintained a detailed audit trail throughout the coding and categorization of the data, with the assistance of coding software and a collaborative online workspace. As codes and categories emerged, they were tested against the entire dataset for reliability and confirmability.
Findings
Survey results
The sample size (n = 24) fell short of the minimum (n = 59) necessary to detect a moderate effect size of 0.4 (calculated using G*power 3.1.9.7), making it impossible to detect statistical differences between the groups for all measures. Therefore, descriptive data are provided below, supplemented with contextual data from the focus groups.
Pre-simulation context
Of the 24 participants, sixteen (66.7%) reported experiencing workplace violence prior to the study, eleven of whom (69%) experienced this in the course of their nursing studies. Eight participants reported violent incidents in acute care settings (n = 8); six in long-term care/residential care (n = 6): one in acute psychiatric/mental health care (n = 1); and three in other specialty areas such as labor & delivery and pediatrics (n = 3). Regarding who was involved in such incidents, ten participants indicated a patient or client (n = 10); six indicated a staff member at worksite (n = 6); two indicated a patient or client family member (n = 2); two indicated a fellow student (n = 2); two indicated a nursing preceptor or supervisor (n = 2); and two indicated a nursing professor or faculty member (n = 2). Twenty-two participants (92%) agreed that workplace violence was a problem for nurses, while the remaining two (8%) responded they did not know.
On the workplace violence knowledge tool, the average score was 68%. Sixteen participants (66.7%) correctly answered the most common workplace violence experienced is from customers/clients. Twenty-one (87.5%) correctly identified workplace violence as “any physical assault, threatening behavior, or verbal abuse occurring in a work setting.” Seven (29.2%) correctly identified “oppressed group behavior” as worker-on-worker violence. Twenty-one (87.5%) correctly identified behaviors that did not typically precede violence. With regard to knowledge about intervention and post-event response, fourteen participants (58.3%) correctly identified loss of cognitive, emotional, and behavioral control as characteristics of a crisis situation. Fourteen (58.3%) correctly identified an example of nonverbal intervention. Twenty-one (87.5%) correctly answered it would be inappropriate to file an incident report when a patient is agitated but does not act out physically or verbally.
The participants brought a variety of previous experiences to the virtual simulation. Some had trained extensively in virtual environments while others had no experience. A few participants had considerable experience with mental health support, such as Sarah: “I work in long term care,” she explained, “and we don't necessarily call a code white for every situation, because there's situations sometimes on the daily with distress, and verbal and physical abuse.” A number of participants had completed the mental health portion of their nursing education online, due to the COVID-19 restrictions on in-person learning, and therefore wished to practice their skills in a virtual environment as well. Matt, for instance, sought to learn “what it would be like, without being in person with the patient, and trying to do your assessment, or trying to comfort the patient, or help them.” Likewise, Lorna remarked “I didn't get any simulation experiences—just with COVID it wasn't really possible—so I thought the virtual format would be interesting.”
Format and timing
During the focus groups, participants expressed a range of opinions about the overall format of the simulation. Working in pairs was felt to be advantageous, in that participants could alternate taking the lead. “Whenever you didn't know what else to say or how to continue,” said Beth, “most of the time your partner chimed in and would help guide that conversation.” The partnerships also helped participants cope with stress, knowing that “you weren't going into [the simulation] alone” as Sarah put it, and they moreover enabled participants to observe and learn from each other's strategies. “[It] helped me reflect back on my own biases or experiences,” remarked Matt; “maybe I am going overboard with this, maybe I need to take a step back, or maybe I need to … do something or say something.” Nonetheless, Matt went on to observe that differing perspectives could also present challenges in coordinating strategies for de-escalation. “It was hard for me because I said … this is not appropriate, and I set that boundary, whereas the partner that I was with thought that was appropriate.” Eva concurred, adding that additional preparation time together might have been helpful: “if we had maybe decided, maybe we’ll talk about this, or take turns.”
It was generally agreed the preamble and debrief were too short to be of real value. “We got that very brief introduction,” Lorna recalled; “I didn't remember most of the details when I went to do the simulation.” Particularly frustrating was the sense that helpful information was incomplete or missing. Allyson commented, “there wasn't really an end plan to the conversation … which made it hard to guide the assessment and [know] what interventions you could provide over Zoom.” The debrief was likewise felt to be rushed and desultory—a missed opportunity to reflect on the experience and learn additional strategies for managing a code white. “It was over and done really fast,” said Sarah. “We don't really get too much lecture theory [on workplace violence] … so it would be helpful to have some more things in our toolbox to pull out in clinicals and in real life.” The educational value of the simulation may have been further limited by its duration. “I wanted to get right back into it and try out what I had learned, and see if it worked differently in maybe a different scenario,” Sarah remarked. She further suggested that additional simulations might afford the opportunity “to practice what we learned from previous ones.”
Realism, safety and the virtual environment
The involvement of a live actor brought a sense of authenticity. “It didn't feel like that actress was like reading from a script or being prompted by what we were saying,” said Sarah. However, the virtual aspect of the simulation resulted in some limitations. Physical cues, such as “body language—even a hand twitch, or moving their foot,” as Matt said, were imperceptible over Zoom. “Having that screen … creates more distance,” Eva added. In the absence of physical interventions, the virtual environment required participants to draw on other skills, particularly verbal techniques: “In-person code whites, you’re able to put your hand on that person and comfort them physically, whereas the [virtual] simulation challenged my verbal abilities to comfort somebody” said Allyson. Zoom could also make it difficult to communicate clearly, as Allyson explained. “It's very easy to talk over one another, and that makes doing your assessment piece very difficult, and it just becomes a total jumble of information that you’re trying to receive all at once.”
Some participants saw unique value in employing Zoom for the simulation. “Having it over Zoom is more relevant, especially as, through COVID and also post-COVID, it seems that we’re moving more towards tele-health,” Allyson remarked; “I never learned any tele-health skills during my nursing education.” This sentiment was echoed by several other participants, who felt this aspect of their education was insufficient. “[We need] to figure out how we can train future nurses so that they are successful in giving care in both virtual and in-person settings,” said Matt. For better or worse, Zoom also reduced participants’ sense of physical peril. “Being behind the screen, versus being in person … You don't really have that threat of violence,” said Eva. Lorna commented, “I’d be surprised if a nursing student in their third year hadn't encountered … some sort of verbal aggression, so [it's] helpful to practice in a safe environment.” The simulation made it possible to “have a safe place to go through a very realistic situation,” said Sarah.
Nevertheless, attempting to provide care during the simulation was stressful. “I didn't know what to say to defuse the situation—it just kept getting worse, said Sarah. “It's hard to see someone who's upset and who's … struggling,” Eva put in, but I wouldn't necessarily count that as a bad thing.” Fear of responding inappropriately, and the sense of being lost, were prevalent. “[The standardized patient] was like, Are you laughing at me?,” recalled Beth, “and I had no idea how to respond.” Lorna agreed, adding, “I think my group kind of lost sight of what we were trying to do.” The experience highlighted the necessity of learning, in Eva's words, “how to ask questions in a way that's supportive, and not offend [the patient] … [to] do your assessment, build that trust, [and] also get the information that you need.”
Overall value
At pre-intervention, the mean score on the ATS measure for all participants was 29.4 (95% CI = 27.7–31.2, n = 24), and at post-intervention, it had improved slightly to 31.5 for the intervention group (95% CI = 29.7–33.29, n = 14); the overlap of confidence intervals makes it unlikely this is a significant difference. As the small sample made it impossible to detect differences at the individual question level, non-parametric tests were not carried out.
In the post-simulation questionaire, which used a five-point Likert scale, one intervention group member responded the simulation provided no new information (n = 1); three responded it provided very little new information (n = 3); four responded it provided an average amount (n = 4); five responded it provided somewhat more new information (n = 5); and one responded most of the information was new (n = 1). The average of responses was around an average amount of new information, (M = 3.14, 95% CI = 2.27–4.02). Four participants rated the simulation as neutral in terms of usefulness (n = 4); two rated it somewhat useful (n = 2); and eight rated it very useful (n = 8). The average of the responses was around somewhat useful (M = 4.14, 95% CI = 3.64–4.14). Regardling likelihood of remembering information presented, one participant responded they were not very likely to remember (n = 1); one responded as neutral (n = 1); eight responded as somewhat likely (n = 8); and four responded as very likely (n = 4). The average of the responses was around somewhat likely (M = 4.07, 95% CI = 3.59–4.55).
In response to the post-intervention question “Would you recommend the code white simulation to other nurses, and why?”, 13 out of 14 (93%) intervention group participants stated they would recommend the experience insofar as: (1) It provided the opportunity to put concepts such as de-escalation into practice, as well as new insights into the issue of workplace violence; (2) It provided a safe, non-threatening, non-judgmental environment where mistakes could be made without drastic consequences; and (3) It provided an opportunity to reflect on learning needs and deficits, learn from mistakes, and gain self awareness. Only one respondent (7%) declined to recommend the simulation, on the grounds it provided no benefit.
Participants largely agreed the simulation exposed a gap in their education. “Code white is something we don't really have the opportunity to discuss or practice,” Sarah commented; “we don't really get too much of that before being in real life situations.” Lorna noted, “You learn the de-escalation techniques but you don't practice them.” While no-one suggested the simulation in itself was sufficient to remedy this educational deficit, the experience underscored the need for improved code white education for all nurses. “[It is] really important to have … that continuing education piece for new grads or nurses,” said Allyson. In reflecting on the experience as a whole, participants chose terms such as “eye-opening,” “relevant,” and “beneficial.”
The primary value of the simulation, according to participants, lay in the preparation it offered for managing a real-life code white. “It only gets better as you work on it,” said Eva. “If you actually interact with patients in situations, it gets easier.” Sarah looked back on the simulation as a timely lesson on accepting one's limitations. “Sometimes it's out of your control, and it's okay; accept that and remove yourself from the situation,” she remarked. “That's something I use, even at work today.”
Discussion
The virtual code white simulation was predicated on aggressive and intimidating behavior by a patient in a mental health care context, thereby recreating circumstances common to many instances of clinical violence (Angland et al., 2014; Iozzino et al., 2015; Martinez, 2017; Mento et al., 2020; Roussy, 2018). It was apparent from the focus groups and survey responses that the participants did not feel emotionally or professionally equipped to cope with violence in this setting (Martinez & De Oliveira, 2021; Mento et al., 2020). Even students who had already undergone clinical rotations in contexts dealing with complex mental health issues, such as long-term care and psychiatric inpatient settings, found themselves struggling to respond to the code white situation (Iozzino et al., 2015). This finding is consistent with the widespread concern that nursing students, and even experienced nursing staff, are underserved by existing nursing curricula in the domains of mental health and workplace violence (Havaei et al., 2019; Hopkins et al., 2018; Irwin, 2006; Taylor & Rew, 2011).
Participants rated the simulation highly insofar as it created an authentic-feeling verbal confrontation with an aggressive client; it tested the knowledge, skills and emotional resilience of the participants and it afforded the opportunity to reflect on their responses and learn experientially (INACSL, 2016; Lioce, 2020; Martinez, 2017). Criticism of the simulation also lined up along these points. The virtual environment was a barrier to naturalistic interaction with the SP and fellow participants. The preamble, simulation and debrief were too short to fully capitalize on the experience. And absent the threat of physical violence (CPSI, 2021), it remains dubious how well the simulation prepared participants to manage an in-person encounter with an aggressive client. Given the recent spike in mental health crises and incidents of physical violence accompanying COVID-19 (Devi, 2020; Havaei et al., 2020; ICRC, 2020; Taylor, 2020), this is a significant caveat underlying virtual simulations.
It is unsurprising that the code white experience felt overwhelming for many participants. A single, virtual simulation at best provides a baseline assessment of competencies on which to build (Cant & Cooper, 2014; Padilha et al., 2019; Shin et al., 2019; Verkuyl & Hughes, 2019). Participants were astute in observing that any real educational gains would only come with further iterations of the experience. It is also plausible that a more substantive introduction and debrief would enable participants to better capitalize on the experience acquired during the simulation, which can be taken into consideration for future iterations.
One of the more intriguing outcomes—a meta-educational finding, in effect—was the value participants placed on the virtual environment as clinical experience in its own right. The adoption of telehealth and other remote clinical tools is increasingly widespread in practice, not least owing to COVID-19 (Andrews et al., 2020). Long before the pandemic, health regions around the globe were already struggling with a human resource supply crisis (INACSL & SSH, 2020). Even as clinical settings gradually return to their pre-COVID-19 routines, it seems inevitable that tomorrow's healthcare professionals will require virtual healthcare competencies to complement their traditional knowledge base and skillset.
Notwithstanding the endorsement of the Society for Simulation in Healthcare and the International Nursing Association for Clinical Simulation and Learning (INACSL & SSH, 2020), the data cannot be said to show if virtual simulations are a viable alternative to clinical hours, or merely a valuable learning experience. It remains to be seen whether and to what degree the current cohort of nursing students, virtually learning under the shadow of a global pandemic, will find themselves at a professional disadvantage or advantage relative to their colleagues who learned prior to the pandemic.
Limitations
The sample (n = 24) fell short of the minimum deemed necessary to detect statistical differences between the groups for all quantitative measures. This drawback, surmisably, is owing to pandemic related restrictions and time constraints experienced by the study team and potential study participants during the recruitment process. Accordingly, descriptive statistics and qualitative findings are reported here, which may inform a larger quantitative study in future.
Conclusion
This study illustrates what is achievable under the sub-optimal circumstances of a public health emergency and campus-wide lockdown. While skepticism regarding the sufficiency of virtual code white simulations as a standalone educational intervention remains warranted, the findings leave no doubt that they serve a valuable function in the context of a larger curriculum on managing workplace violence, and they are a worthwhile endeavor when circumstances preclude any other alternative. Left unanswered is how much further benefit participants would derive from in-person simulations in addition to virtual simulations. Given the above findings with respect to developing a virtual caregiving skillset, the authors speculate an iterative program comprising both virtual and in-person experiences would deliver the greatest benefit to nursing students.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a University of Alberta Faculty of Nursing Teaching, Learning, and Simulation Research Grant, awarded to the principal investigator, Dr. Carla Hilario.
Ethical approval
Ethical approval for the study was obtained from the University of Alberta Research Ethics Board 2 (approval Pro00088275).