
Abstract
Background:
Meatpacking is dirty, dangerous, and demanding work. In the United States, the industry predominately employs people from racial/ethnic minority backgrounds and immigrants, with 45% of the workforce identifying as Hispanic/Latino. Little is known about how the work environment affects worker engagement in health-promoting activities; however, occupational health professionals are uniquely positioned to advance worker health, safety, and general well-being.
Methods:
Hispanic/Latino meatpacking workers with work-related musculoskeletal pain and active health concerns were recruited to participate in a study to explore health, health behaviors, and the work environment. Five focus groups (N = 28) were conducted in Nebraska between March 2019 and February 2020. Thematic analysis using the Health Belief Model constructs was used to explain workers’ health behaviors including utilization of occupational health services at their workplace.
Findings:
Workers believed that there was little they could do to prevent and treat health problems. They understood the perceived threat of health problems and the benefits of self-care, but the perceived barriers often outweighed the benefits. The workplace had few prompts to motivate or incentivize self-care both in and outside of work. In addition, workers did not trust the occupational health office and saw few benefits to accessing services. Together, these conditions resulted in low self-efficacy and limited engagement in health-promoting behaviors.
Conclusion/Application to practice:
Occupational health professionals should promote Total Worker Health and foster trust by providing culturally, linguistically, and literacy appropriate services and by identifying opportunities and reducing barriers for workers to engage in activities to promote their health, safety, and well-being.
Keywords
Background
The coronavirus disease (COVID-19) pandemic has illuminated health disparities among various vulnerable worker populations, particularly those within the meat processing (meatpacking) industry (Ramos, Lowe et al., 2021; Yearby & Mohapatra, 2020). Meatpacking plants disproportionally employ low-income populations, including people from racial and ethnic minority backgrounds and immigrants. In fact, Hispanic/Latino workers comprise about 45% of the meatpacking workforce in the United States (Fremstad et al., 2020). Close worker proximity, long work hours, and limited personal protective equipment are commonly cited factors facilitating the rapid spread of COVID-19 through meatpacking plants which have led to temporary closures at facilities across the country (Ramos et al., in press).
COVID-19 is not the only occupational health concern in these plants. There are other long-standing factors affecting the health of more than half a million people in the United States who work in the industry (Fremstad et al., 2020). Meatpacking plants are dangerous workplaces. Although under-reporting of occupational injuries and illnesses is common in the industry, rates are still twice that of general industry (Fagan & Hodgson, 2017; U.S. Bureau of Labor Statistics, 2020). Safety culture in these facilities is poor (Ramos et al., 2021), and multiple reports across decades have highlighted the inherent health and safety hazards associated with working in meatpacking (McConnell, 2019; Nebraska Appleseed, 2009). Work within these plants is difficult, and although there have been advances in mechanization, the work largely remains manual with the use of pace-set production lines. Previous research has indicated that meatpacking workers have high levels of unhealthy physical activity at work, including repetitive motions, forceful exertions, and awkward and stagnant positioning (Leibler & Perry, 2017; Nebraska Appleseed, 2009). Pain in the shoulders, wrists, and hands affects both work and usual life activities of meatpacking workers (Rowland et al., in press; Smith, 2017). Chronic musculoskeletal pain is associated with physical inactivity, psychological distress, increased inflammation, and use of non-steroidal anti-inflammatory drugs, all of which contribute to an increased risk of diabetes, hypertension, obesity, heart disease, and stroke (Malmberg-Ceder et al., 2017; Oliveira et al., 2020; Walsh et al., 2018).
Occupational health professionals in food processing are uniquely positioned to identify and intervene in managing and preventing work-related health and safety concerns as well as advancing the overall health and well-being of workers (American Association of Occupational Health Nurses, 2015). The Total Worker Health concept was developed to integrate efforts to improve the overall health of workers with occupational health and safety (Hudson et al., 2019). Total Worker Health promotes occupational policies, programs, and practices that favorably affect the health and well-being of workers, their families, and their communities (National Institute for Occupational Safety and Health, 2020). To the authors’ knowledge, no studies have been conducted on the general health and well-being of Hispanic/Latino meatpacking workers in the United States with respect to the Total Worker Health model. Most occupational health research within the meatpacking industry has been conducted outside the United States and has focused on work-related injuries, chronic pain, or work-related exposures affecting the skin or respiratory tract (van Holland et al., 2015).
The Health Belief Model (HBM) has been used widely to explain and predict a variety of individual health behaviors associated with health outcomes. It is one of the core models used in health promotion and disease prevention research and interventions, contributing considerably to understanding the determinants of health-related behaviors, such as the acceptance of preventive health services and adherence to treatment (Carpenter, 2010; Champion & Skinner, 2008). The HBM suggests that health behaviors are influenced by individuals’ beliefs and perceptions about their susceptibility to a particular health condition as well as cues that the health condition is important, both of which affect an individual’s desire to engage in health-promoting behaviors. According to this model, for successful behavior change, people must be motivated to act, feel threatened by their current behavioral patterns, and believe that change will be beneficial. In addition, people must feel confident and have the necessary skills to make the change (Rosenstock, 2005; Rosenstock et al., 1988). The model predicts that when people have strong perceptions about their susceptibility and the severity of a health outcome, they are more likely to take action to prevent an unfavorable outcome. Table 1 highlights the major constructs of the HBM (Champion & Skinner, 2008).
The Health Belief Model: Key Constructs and Definitions Used for Focus Group Domains
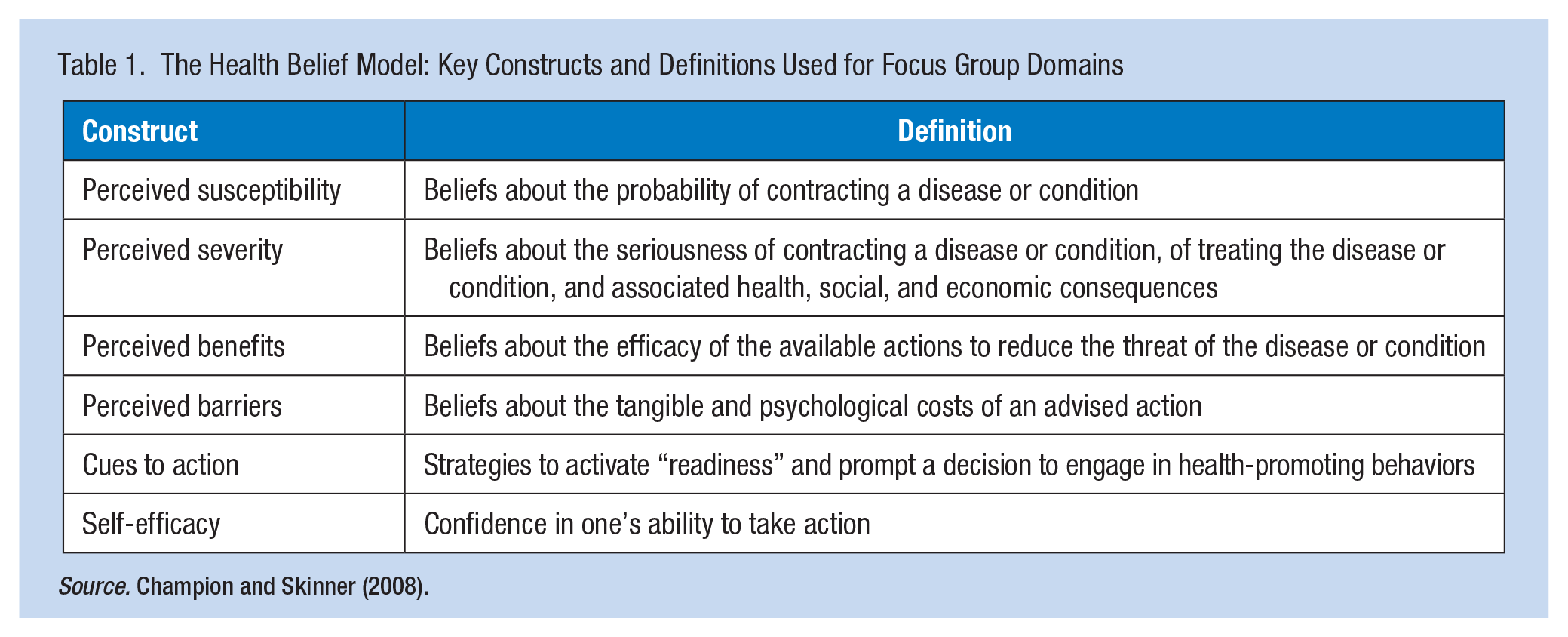
Source. Champion and Skinner (2008).
To the authors’ knowledge, the HBM has not been applied to the meatpacking industry through a Total Worker Health approach. Therefore, this preliminary study used the HBM to understand the factors that may influence meatpacking workers’ decisions to engage in self-care and health-promoting activities as well as access occupational health services at their workplace.
Methods
Data were collected through five focus groups (N = 28) conducted in Nebraska between March 2019 and February 2020 as part of a mixed methods study. Hispanic/Latino men and women, aged 19 to 65, currently employed in a meatpacking facility, and reporting work-related musculoskeletal pain were eligible to participate. Individuals were excluded from participating if they were unable to provide verbal consent or answered “rarely” or “never” when questioned about having pain that negatively affected their life. Participants with both work-related musculoskeletal pain and risk factors for cardiovascular disease were desired for the study to understand the co-occurrence of these health problems and to gain insight into how a future physical activity intervention might be developed to target both. Recruitment strategies included partnerships with community-based organizations, Facebook promotion, Spanish-language radio ads, and word-of-mouth. Written informed consent was obtained from participants. Data collection was conducted between March 2019 and February 2020 in community settings (e.g., public library, church, and non-profit organization) near meatpacking plants located in Nebraska. Participants were not recruited directly through the occupational health office because workers may have perceived undue company influence and may have been fearful that information could be reported back to the company, resulting in negative consequences for the workers. Focus groups were conducted and led by a bilingual facilitator in Spanish using a semi-structured guide that centered on perceptions of health and safety within the work environment, tasks completed by workers, and workers’ ideas for improving health, safety, and well-being. Sample questions included the following: “How does your job affect your health?” and “What do you believe should be done to prevent work-related accidents, injuries, and illnesses in the plant?” Demographic information from each participant was also collected. Participants received a US$40 gift card for participating in the focus group, and because the focus groups were scheduled after work, a meal was provided to all participants. This study was approved by the Institutional Review Board at the University of Nebraska Medical Center.
Focus groups were audio-recorded and lasted approximately 90 minutes. Each focus group was transcribed in Spanish and translated into English for analysis. Four members of the research team analyzed the transcripts using thematic analysis techniques. Each transcript was independently reviewed and coded by at least two researchers using an a priori codebook. Then the team met to review coding, reconcile differences, and agree on any emergent codes within the transcripts. Each coder developed summary statements across groups of codes, and themes were identified through consensus.
Results
A total of 28 workers participated across the five focus groups. Most participants were from Mexico or Guatemala and had been working in meatpacking for more than 11 years. Table 2 highlights the demographic characteristics of the participants.
Demographic Characteristics of Meatpacking Worker Participants (N = 28)
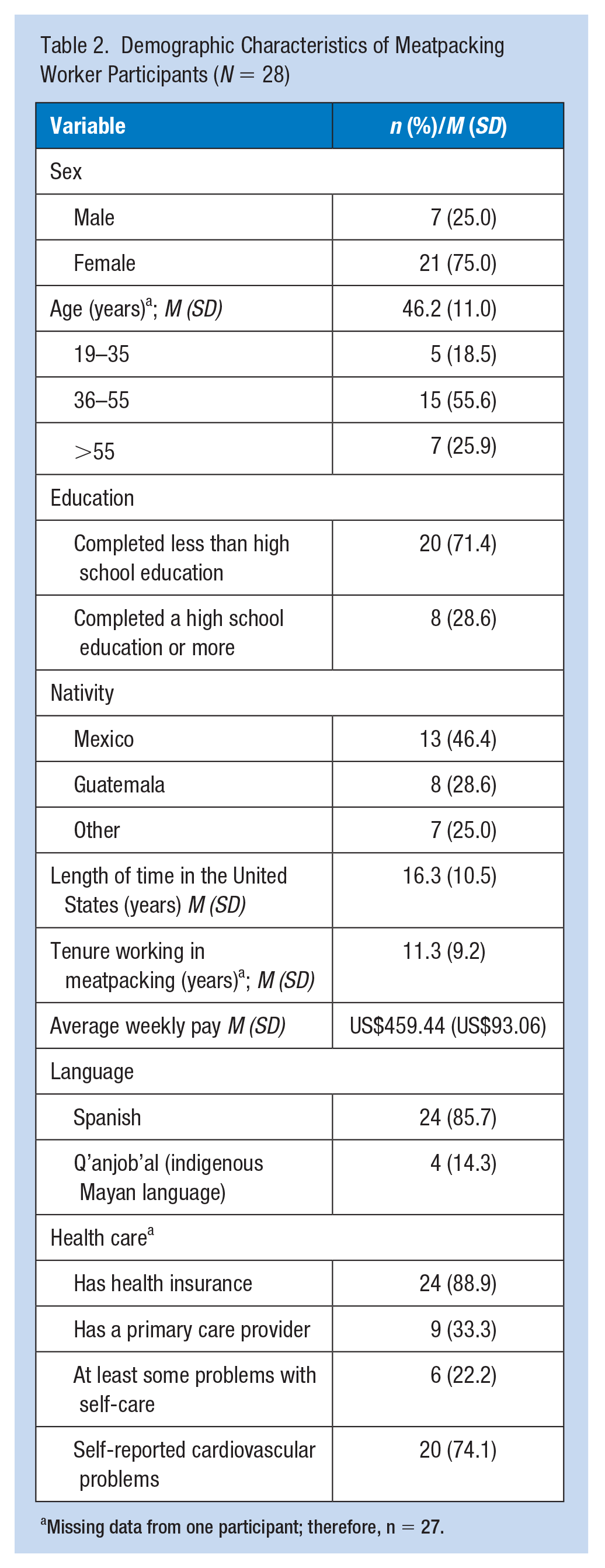
Missing data from one participant; therefore, n = 27.
Three themes emerged regarding worker engagement with self-care, health promotion, and the use of services at the occupational health office: (1) workers believed that there was little they could do to prevent and treat health problems, (2) the workplace had few cues to action to motivate or incentivize self-care at work, and (3) workers had little confidence and trust in the occupational health office—they saw few benefits in accessing services. Careful review of the themes in relation to the HBM allowed the investigators to grade the workers’ experiences with the model constructs. Specifically, worker descriptions within and across the themes indicated that despite a high perceived threat to health, workers had limited engagement with health promotion and self-care. Furthermore, perceived barriers to health were high, perceived benefits for taking action were moderate, and cues to action within the meatpacking environment were few. These forces left workers with low self-efficacy that they could positively affect their health.
Theme 1: Workers Believed That There Was Little They Could Do to Prevent and Treat Health Problems
Participants felt that there was little they could do, particularly in the work environment, to prevent injuries or pain—They were inevitable and inherent in the work. Injuries from repetitive motions, slips, falls, cuts, stabs, or crushing forces were expected as part of the job. Participants in all five focus groups described common musculoskeletal pain sites, including the shoulders, elbows, wrists, and hands, and the effect of prolonged standing on the back, knees, and feet. Many workers reported being diagnosed with arthritis, bursitis, tendonitis, and/or neuropathy. One worker indicated, “There is no way to prevent an injury. There is no way. When you are working at that pace, you do not have a way to prevent an injury” (Worker 4). Another mentioned, “I don’t think there is any way for us to take care of ourselves” (Worker 13). A worker from the fabrication department indicated, The bad thing about working in a meatpacking is that with time the cold starts affecting our body. Also, the repetitive movements have already started affecting me. One of my arms already hurts. That is the bad thing . . . that at the end we are all going to end up getting hurt. (Worker 12)
Workers predominately used reactive strategies both at home and at work to manage their work-related pain, including massages, ice and/or heat application, joint bracing, acetaminophen, ibuprofen, and topical ointments. One worker mentioned, “What is affected the most is the back, the arms, and the hands that fall asleep or become numb. No, no, I cannot live without painkillers” (Worker 11). Another commented, [I] take ibuprofen, take it every five hours, six hours . . . you go to the infirmary due to the pain . . . the pain cannot be masked. A towel with hot water or a towel with cold water; that is not healing. It is because of that, the work there, that people get hurt. It is because of such continuous repetitions, the quickness that the job has. (Worker 28)
A variety of barriers made it difficult for self-care such as the disciplinary point system where “points” were awarded for worker behavior concerns which eventually could lead to termination. During the focus groups, workers described getting points for missing work due to illness and the inability to leave the line for self-care activities (e.g., using the restroom, visiting the health office, or stretching) due to production goals. One worker noted, We have to go to work daily. In the plant where I work, they say, “Do not miss work.” They give some classes and they say, “When you are sick due to the flu, you may miss work—just give us a call” but anyway, when we return, they give us our point. (Worker 9)
Several workers indicated that prescribed medications for hypertension and diabetes affected their productivity, and some avoided taking their medication because of the need to use the bathroom. They described how the line did not stop for a bathroom break and that there was no one to cover. Others felt that if coworkers forgot to take their medication, the team was slowed down. One worker mentioned, What we have to deal with there is the stress and I see it with my coworkers—the majority of them, we are seven. A coworker and I are the only ones that don’t have high blood pressure. All others have high blood pressure. With just a small thing, if they don’t take their pill, they slow us all down. But everyone understands already that it is because of the high blood pressure and that sometimes they don’t take their pill. (Worker 4)
Many workers perceived that production pressures undermined their ability to recover from work-related injuries. They felt workers temporarily assigned to “light duty” by the health office were not allowed to truly “rest” their injury because the work still required heavy lifting and/or repetitive motions. One worker noted, In the case where someone gets hurt . . . they send you to a “rest area” . . . They put you to pack boxes all day long. It is the same thing. All day you lift containers of meat that weigh around 30 pounds. (Worker 2)
Another commented, They have to be more considerate . . . Because I went with some pain to the office . . . They told me, “Take this. Go to the machine, take a painkiller, relax for about 10 minutes, and when it has been more than 15 minutes, come back, and come back to your post.” That is what happened. It has happened to me over a hundred times. (Worker 11)
Others were frustrated with this practice because of the risk of working with an injured team member. One worker noted, “They send you one that is injured or one from therapy [a worker that has duty restrictions] . . . They are people that instead of helping you are in your way” (Worker 27).
The rate of production affected workers’ ability to engage in health-promoting behaviors. Many workers noted that the line speed continued with or without a full crew. When there were absences due to injury or illness, those at work were subjected to increased risk of injury as they hurried to keep up. Others felt that time away from the line for self-care or to seek treatment in the health office was not justified. They felt that visiting the health office would take too long and they perceived they could not do anything for them anyway. Some workers noted that they avoided complaining about any pain or visiting the health office because they believed that this would earn them the reputation of being “lazy” or give their employer a reason to fire them. One worker said, We are afraid to say that something is hurting . . . we are afraid that we will be fired . . . The pressure that we have there has a lot of influence because we are afraid of a lot of things. (Worker 7)
Workers described what happens when injuries occur, and one worker commented, When many people complain about something that hurts them, the safety people come and tell the supervisors, “They need to stretch . . . put the employees to stretch, to exercise.” But when they see that a lot of people are arriving at the nurse’s office when it is not convenient for them to have a lot of people go to the nurse’s office because they have to find someone else to cover that position while they are gone for 30 minutes to get therapy then that is when . . . We do not see that they care about us, no. (Worker 24)
Workers understood the health threats but commonly reported that there was “nothing that could be done” to improve their health if they continued working in meatpacking because of barriers such as production goals and disciplinary policies. Despite some workers reporting chronic health concerns (e.g., diabetes, high blood pressure, pain, depression, and anxiety), no workers identified the health office as a source of support for self-care or management of these conditions.
Theme 2: The Workplace Had Few Cues to Action to Motivate or Incentivize Self-Care at Work
Participants described having safety meetings but also that there was little meaningful action by employers to motivate or incentivize self-care activities. A worker commented, “They already told you that it is dangerous. That is the only thing, but they are only chats. They are not going to give you additional PPE to protect yourself” (Worker 13). Another indicated, They don’t give you a chance to express oneself and sometimes when one tells them, they ignore what you tell them and only during the meetings . . . they tell us what to do but they never give us a chance to or the time to do it. There is no time for the warm-ups and things like that because that is what prevents things. (Worker 24)
Participants provided limited examples of cues to action. Some workers were aware of measures like stretching to avoid musculoskeletal soreness or injury, but few workers reported organized, allotted on-the-clock time for stretching or rotation of tasks to break up the repetitive movements while at work. One plant had instituted dedicated time for workers to stretch, but the practice has since been abandoned. A worker commented, . . . we would stretch our hands and everything . . . I don’t know if the safety people require it, but they don’t want to do it anymore because they never want to waste time. We do it sometimes when we are changing the plastic or something because they [the lines] stop. We do it because we want to. It is not because they say, “We are going to stop for about two minutes so everyone can do it.” No, they do not do it anymore. (Worker 24)
Workers across all focus groups discussed ergonomic issues. Participants described the “proper” way to lift, transfer, and move as instructed by health office staff. However, they indicated the line speed and/or covering for missing team members did not allow them to implement these strategies. Workers described having to adapt to the line speed and the machinery, not the other way around. One worked noted, There are boxes that weigh more than 5 pounds, and you grab it with one hand because you have to do it fast. You do not have the chance to grab it with both hands and take your time to accommodate it. You have to put it in quickly because you have to produce 100 coolers per hour . . . You have to grab them [boxes] to the rhythm of the production because if you do not complete the production, then you are useless. (Worker 8)
Another worker noted that the production line was not designed for people of their physical stature stating, There are jobs where you are required to stretch [to reach something]. Among us, three are people who are short. We have to stretch to be able to pull the product. Therefore, with the height and all that, there are parts of the body that are deteriorating more. (Worker 20)
Several workers noted the potential role of the health office being more involved in health promotion. One worker commented, I also can do something [to be healthy] like take my blood pressure two or three times per week. Have a team, a nurse, that during lunchtime she or he can take your blood pressure. Because sometimes one does not take his or her pills because of the pressure to continue working and then you forget. They can take your blood pressure and that is how they would know if a worker has high blood pressure or not. That is something that is very important that they can do. (Worker 3)
Theme 3: Workers Had Little Confidence and Trust in the Occupational Health Office—They Saw Few Benefits in Accessing Services
In general, participants were apprehensive about visiting or communicating with their occupational health office. The workers’ lack of trust in the health office was multifactorial and centered on fear of job loss, inadequate support for their health and safety needs, and language barriers.
Workers described their fear of losing their job or their “good” standing with employers if they were injured, needing time off for illness, or going to a doctor’s appointment. Participants frequently mentioned the disciplinary point system and that “points” were awarded even when associated with illness or injury. A worker commented, “I have called and told them, ‘I am sick.’ You have to take a doctor’s note, your medications that you are taking, and apart from that you get a point” (Worker 8). Participants commonly described working while ill, injured, or with pain and/or numbness in their extremities either because they were fearful to report it or because prior visits to the health office had not been helpful. Participants acknowledged the potential benefit of alerting the health office to work-related pain or work safety concerns, but the risk of losing their job prevented them from taking action. One worker noted, And for [the work], being fast, the shoulder, my shoulder is in pain. Only once I complained in the office and they almost fired me, because of course—then, as my colleague said, I do not complain anymore . . . They did not give me a pill, not even for the pain, nor for anything so instead I look for medicine—I buy it, my pain killers. (Worker 5)
Participants felt that the services received were inadequate. Workers mentioned going to the health office due to pain and injury and receiving a minimal level of care. One worker commented, I do come out very tired, with my arms in pain. Sometimes I have complained that it hurts . . . they take me to the nurse. They give us a little bit of ice, a pill, and that is it. (Worker 12)
Some workers avoided the health office altogether because of this poor treatment and perceived lack of care, noting that “they don’t care about you” (Worker 8). Another worker mentioned, They don’t like it when you go to the infirmary, and if the supervisor begins to imagine why you did something to yourself and that you are going to the infirmary too often, they even want to take you out [terminate you], see? And then, if you told me: “No, I hurt myself, and I go there for the nurses that they are supposed to be there to support you, to help you.” No, they are worse than the supervisor. They mistreat you and they tell you that you did not do that [injury] there [at work], that you did it at home. (Worker 28)
Several participants described traumatic work-related injuries where workers were unable to render aid or assist the injured worker because they were “not allowed to touch” the injured person. One worker commented, About six years ago, a pig belly fell on a young man . . . I tried to lift him up, but no, they told me not to, not to touch him. The poor guy. He was just there, trembling, trembling terribly. (Worker 14)
Another worker cited another example: . . . the danger is that some people have stabbed themselves and have died there. Once at the company this person stabbed himself—years ago—in the leg and bled out because they don’t let anyone touch them until the nurses get there. They have to stay there. Nobody was allowed to touch him. (Worker 8)
Participants were disturbed by this policy and could not offer a rationale for it. It was thought that they were at risk of injury if they touched the injured coworker or it might disrupt the scene and consequently the ability to determine the cause of the injury. Policies without clear explanation fostered mistrust.
Workers reported that they had difficulty communicating with the health office staff due to language barriers. Language discordance between workers and the health office staff compromised many important functions of the occupational health office. Participants described difficulty with simple tasks such as completing a hearing test as well as with complex activities like documenting work injuries or reviewing a treatment plan. One worker commented, “The nurse told me that I had to do it [the hearing test] over again. I’m not sure why she was telling me in English. I understand it a bit, but it needs to be repeated” (Worker 27). Interpretation services were not always available, so coworkers were often called upon to interpret but often lacked the skills to do so. Workers reported being frustrated because they were aware that they were not able to communicate their point effectively.
There was evidence that participants lacked understanding of workers’ compensation processes and labor rights. Many perceived a need for “permission” from the health office to be able to seek medical care. This in turn increased their distrust of the health office. A worker commented, I want to see the doctor because I can’t handle the pain anymore. You can’t go. You have to wait until they send you. By chance if you get home and can’t bear the pain, and you go see a doctor, they’ll take you out of work. (Worker 28)
Discussion
We used the HBM to explain factors that affect meatpacking workers’ engagement in health-promoting behaviors and their use of occupational health services. We found that workers understood the perceived threat of health problems; however, they experienced high barriers and few cues to action in the work environment. Although many workers understood the benefits of self-care and safety, the perceived barriers often outweighed the benefits, which resulted in low self-efficacy and limited engagement in health-promoting behaviors. Consistent with previous literature, the work environment did not promote the health and well-being of the workforce, and workers perceived that production was the sole priority of the company (Ramos, Carvajal-Suarez et al., 2021). Workers chose to work sick and/or injured and avoided advocating for themselves for fear of losing their only source of income. Meatpacking was often the only employment option with guaranteed hours and benefits for immigrants, particularly females, with limited English proficiency (Ramos et al., in press).
Many workers felt that they received unfair consequences and minimal treatment at the occupational health office, leading to reduced trust and confidence in accessing health services at the workplace. Previous studies have found that language concordance between health care providers and patients results in higher satisfaction and adherence to treatment (Detz et al., 2014; Parker et al., 2017; Traylor et al., 2010). Unfortunately, language discordance between workers and occupational health professionals and/or plant management was identified as a key factor that undermined efforts to mitigate risks of work-related injury and illness. Workers with limited English were less likely to address safety concerns with supervisors. In this study, mistrust of the occupational health office, limited English proficiency, and the prevalence of unmanaged chronic health conditions resulted in limited engagement in health-promoting behaviors and poor outcomes. While current efforts to protect meatpacking workers center on workplace safety and personal protective equipment, taking a Total Worker Health focus is critical.
Unfortunately, the constant focus on production and the physical nature of meatpacking work may generate and exacerbate chronic health conditions, and common occupational injuries may not receive appropriate treatment (Rowland et al., in press). Multiple strategies are needed to promote health, well-being, and behavior change. For example, workers must understand the perceived threat, view clear benefits for changing their behavior, have cues to action in their surrounding environment, and have adequate self-efficacy to make a change. Organizational efforts from management and the health office are critical in improving workers’ recognition of health and safety risks and engagement in health-promoting behaviors both at the worksite and at home, given the reciprocal relationship between the occupational context and a worker’s personal life.
This study is limited in that it only examined health and perceptions of health among Hispanic/Latino workers who had self-reported pain. It may be helpful to explore differences among workers based on acculturation, immigrant generation, and country of origin. Furthermore, the HBM may be limited by the real barriers that workers experience, many of which are controlled by plant management. Future research that explores perceptions of diverse worker populations, plant management, and occupational health office staff would balance the findings of this study. Future studies may also evaluate self-care and self-efficacy among workers and grade health office practices, including cues to action to enhance performance.
Implications for Occupational Health Nursing Practice
Occupational health offices within meatpacking plants are well positioned to advance the Total Worker Health objective to improve the health and well-being of workers, their families, and communities. This study suggests that an initial area of focus for occupational health office staff is developing trust with diverse workers. Workers’ cultures, educational attainment, and English language proficiency make communication with the health office more challenging. To adequately address the health needs of this population, it is critical to have multilingual staff and culturally, linguistically, and literacy appropriate materials and programs that respond to the most salient needs of workers. This may go a long way toward fostering clear communication and trust between workers and the health office. Workers may be hesitant to discuss their health and safety concerns through an interpreter, especially one who may be a coworker or supervisor. Companies are encouraged to evaluate the most common languages spoken by the workforce and ensure the health office has the corresponding language capacity. If there is no capacity, then access to a formalized interpretation service including the use of certified medical interpreters such as through a language line or video interpretation service should be available.
Occupational health professionals can take the lead in promoting Total Worker Health by incorporating health-promoting activities into typical duties of managing work-related injuries. For example, observing workers in their environment performing their work duties may assist in advising them how to implement the appropriate safety strategies. This direct observation prepares the occupational health nurse to advocate for improved safety conditions to prevent injuries due to ergonomic or environmental conditions beyond the control of the worker. Other health issues occupational health professionals might support workers on include pain management, risk of gastric bleeding with excessive non-steroidal anti-inflammatory drug use, and the risk of addiction with chronic use of prescription pain medications. If it is true that workers have “no way to take care of themselves,” they are in need of strong, informed advocates on their behalf. As the most trusted profession (Reinhart, 2020), nurses are well positioned to serve in this capacity.
Total Worker Health also directs health promotion efforts toward non-work-related health issues. Occupational health offices might consider education and screenings (e.g., blood pressure, cholesterol, and A1c) for early detection and management of common chronic health conditions such as hypertension and type 2 diabetes. Using culturally appropriate education materials and/or language congruent interactions, occupational health professionals may improve the worker’s ability to self-manage their health conditions. Addressing common chronic health concerns may also change the perception that “production is the priority” and that workers are disposable. The COVID-19 pandemic has elevated the need for these essential workers and made visible many of the health disparities among this vulnerable population. Krieger (2010) noted that “workers are people too” and not just pieces of the production machine (Ramos, Carvajal-Suarez et al., 2021); they should be cared for with dignity and respect (Krieger, 2010). The meatpacking industry can foster the well-being of workers by addressing inequities, changing their policies and practices, and instituting programming to foster trust and the well-being of their workforce through a Total Worker Health approach.
Applying Research to Occupational Health Practice
This study examined factors reported by Hispanic/Latino meatpacking workers that affected their health. Workers found preventing and treating health problems was difficult. The workplace had few cues to action to motivate or incentivize self-care at work. Workers had little confidence and limited trust in the occupational health office, which was due, in part, to the constant focus on production over workers’ well-being and language discordance. Occupational health professionals are encouraged to observe work tasks directly to determine whether production conditions (i.e., line speed and height) conflict with ergonomic safety standards taught and expected of workers. To build trust among workers, all communication should be delivered in the languages predominately used by the workforce. Employers are encouraged to develop health-promoting programs, policies, and practices recognizing that a Total Worker Health approach addresses concerns both on and off the job. Using this approach would incorporate multilingual staff, preventive health screenings, and referrals to culturally and linguistically competent primary care services when needed.
Footnotes
Author Contributions
Athena K. Ramos contributed to conceptualization, methodology, investigation, curation, analysis, and writing; Marcela Carvajal-Suarez and Natalia Trinidad helped in investigation, curation, analysis, and writing; Sophia A. Quintero, Diana Molina, and Rebecca Johnson-Beller helped in curation and writing; and Sheri A. Rowland contributed to conceptualization, funding acquisition, investigation, curation, analysis, and writing.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Athena K. Ramos, PhD, MBA, MS, CPM, is an assistant professor at the University of Nebraska Medical Center in the Department of Health Promotion at the College of Public Health. She conducts research on occupational health and safety of workers within the agri-food system and well-being initiatives within Latino and immigrant communities.
Marcela Carvajal-Suarez, MPH, is an outreach project specialist at the University of Nebraska Medical Center, College of Public Health, Center for Reducing Health Disparities. Her work focuses on community-based health research and education initiatives in tobacco control, health, and safety among immigrant workers in agricultural and food industries, and community well-being.
Natalia Trinidad, MPH, is an outreach project associate at the University of Nebraska Medical Center, College of Public Health, Center for Reducing Health Disparities. She assists in research projects related to health disparities among the Latino population.
Sophia A. Quintero, MPH, is a research assistant with the Center for Reducing Health Disparities at the University of Nebraska Medical Center, College of Public Health.
Diana Molina, BS, is a graduate research assistant with the Center for Reducing Health Disparities at the University of Nebraska Medical Center, College of Public Health.
Rebecca Johnson-Beller, BSN, RN, is a graduate research assistant at the University of Nebraska Medical Center, College of Nursing. She is interested in decreasing the prevalence of cardiovascular disease by focusing on modifiable risk factors.
Sheri A. Rowland, PhD, APRN-BC, FNP, is an assistant professor at the University of Nebraska Medical Center, College of Nursing. She conducts research on health behaviors to manage cardiovascular risk through workplace and community-based interventions.