
Abstract
Nursing students make an abrupt transition from traditional classes to clinical rotations and shift work. Little is known about students’ sleep, sleep disturbances, and safe practice behaviors during this critical phase of professional development. The purpose of this study was to identify nursing students’ perceptions of problems and potential solutions related to shift work and long work hours. This qualitative, descriptive study used two nursing student focus groups which engaged in a two-round participatory process aimed at framing future interventions. Participants identified problems and solutions related to personal and workplace well-being. Findings will inform undergraduate curricular revisions, and hospital hiring and managerial practices.
Keywords
Each year, over 150,000 new graduates join the U.S. nursing workforce of approximately 2.9 million workers (U.S. Department of Health and Human Services & Health Resources and Services Administration, December, 2014). Practicing nurses frequently report problems with excessive sleepiness or insomnia; prevalence rates for self-reported sleep disturbances range from 24% to 45% (Asaoka et al., 2013; Waage et al., 2014; West, Ahern, Byrnes, & Kwanten, 2007). Nurses’ sleep disturbances have been associated with patient and staff adverse health events (e.g., medication errors and occupational injuries, respectively; Shao, Chou, Yeh, & Tzeng, 2010; Suzuki, Ohida, Kaneita, Yokoyama, & Uchiyama, 2005). However, in contrast to practicing nurses, little is known about nursing students’ sleep, fatigue, and occupational health as they transition to shift work. The extent to which nursing students’ transition to shift work poses immediate or long-term risks to nurses’ health or patient safety is unknown. It is known that nursing students have a deep fear of causing adverse events (Noland & Carmack, 2015). When engaged in facilitated dialogues regarding mistakes, students’ narratives focused on negligence, administering incorrect medications, or mislabeling something such as laboratory results (Noland & Carmack, 2015).
The purpose of this study was to identify prelicensure, baccalaureate nursing students’ perceptions of problems and potential solutions related to adapting to shift work in clinical settings. Following prerequisite coursework, nursing students make an abrupt transition to clinical rotations with schedules that require an additional 6 to 40 hours per week of shift work. Some programs assign students to a role transition or clinically-intensive practicum just prior to graduation; such experiences are intended to promote students’ integration of clinical knowledge as well as prepare them to transition from nursing education to employment.
Compelling evidence demonstrates that risks to both workers and patients increase when nurses’ sleep deviates from traditional patterns. Approximately 57% of practicing nurses are employed in hospitals with shift times and durations varying by unit, organizational need, and collective bargaining agreements (U.S. Department of Health and Human Services & Health Resources and Services Administration, September, 2010). An extensive body of research addresses relationships among practicing nurses’ sleep deficits, shift work, and health outcomes. Recent findings from the Nurses’ Health Study (n = 54,000) demonstrated connections between nighttime work and multiple risks for chronic disease (Ramin et al., 2015). In addition, nurses engaged in shift work or reporting sleep debt exhibited disproportionally high rates of cardiovascular mortality, all-cause mortality, and hypertension (Gangwisch, Feskanich, Malaspina, Shen, & Forman, 2013; Gu et al., 2015). Niu and colleagues (2013) measured selective attention between day and night shift nurses; error rates were 0.44 times greater for night versus day shift nurses.
In response to the known risks of sleep deprivation and fatigue for nurses, fatigue mitigation training has been recently developed for practicing nurses (NIOSH, 2015). However, training that addresses students’ adjustment to night shifts, rotating schedules, and long work hours has yet to be developed. Understanding nursing student perceptions as they transition to shift work can inform the development of interventions from a Total Worker Health™ (TWH) perspective. A TWH framework integrates “ . . . protection from work-related safety and health hazards with promotion of injury and illness prevention efforts to advance worker wellbeing” (Centers for Disease Control and Prevention, 2015). Sleep and sleep hygiene have been cited as opportunities in TWH research (Hammer & Sauter, 2013) and are the focus of this study.
Study Design and Methodology
This qualitative, descriptive study engaged nursing students in a process designed to guide the development of future interventions addressing sleep and safe practice. The study methods were adapted from a structured participatory process developed by the Center for Promotion of Health in the New England Workplace (Robertson et al., 2013). The goal of this process, referred to as the Intervention Design and Analysis Scorecard (IDEAS) Process, was to use iterative rounds of worker input to inform a more comprehensive understanding of occupational health issues, problems, and solutions (Robertson et al., 2013). For this study, steps in the IDEAS process were modified to fit the characteristics of study participants (i.e., students rather than workers) and setting (i.e., a clinical program rather than a specific worksite).
A convenience sample of undergraduate nursing students in their final semester was recruited through social media, course presentations, flyers, and emails. Two focus groups (meeting twice each; two rounds) were facilitated by a member of the research team. The IDEAS tool was used to structure data collection. During the first focus group round, participants were asked to “identify problems and contributing factors” associated with shift work, including shifts over 8 hours, multiple shifts in a row, and working nights and evenings. In the second focus group round, returning participants used the same structure to “brainstorm solutions” to previously identified problems. Demographics and information about clinical site placements were also collected.
The first round of focus groups was held in December 2015, and the second round was held in May 2016, both soon after students’ completion of clinical practica, which involved 120 hours of work. Each session lasted 90 to 120 minutes, with the research team meeting afterward to debrief. Focus groups were audio-recorded and two research team members took field notes. Participants each received US$50 remuneration. The university institutional review board approved all procedures prior to the study commencing.
Data saturation was reached after the second round. Audio-recordings were transcribed, as were IDEAS worksheets completed by participants. Problems (and subissues) and solutions (and related activities) were summarized in separate tables. Directed content analysis was used to identify how students cope with shift work and summarize their suggestions to promote healthy behaviors and safe clinical practice (Hsieh & Shannon, 2005). The goal of directed content analysis is to validate, or conceptually extend, a theoretical framework, in this case the TWH model. Two members of the research team used the TWH model to deductively identify codes to categorize the data, including problems and solutions that impacted (a) personal well-being and (b) workplace well-being. Exemplar quotes from narratives were combined with worksheet data to offer a richer description of the student voice. Similarities noted in both rounds of focus groups were independently coded by the researchers, compared and combined (Hsieh & Shannon, 2005). Data (e.g., transcripts, field notes, and facilitator’s summaries) were maintained on a secure server and accessed via Microsoft Sharepoint. Rigor was assessed throughout the analysis process using documented methods addressing confirmability and credibility (Lincoln & Guba, 1985). Confirmability was judged by keeping records of all data collection and analysis steps (audit trail) and reporting results in narrative form that could be judged by readers for credibility.
Results
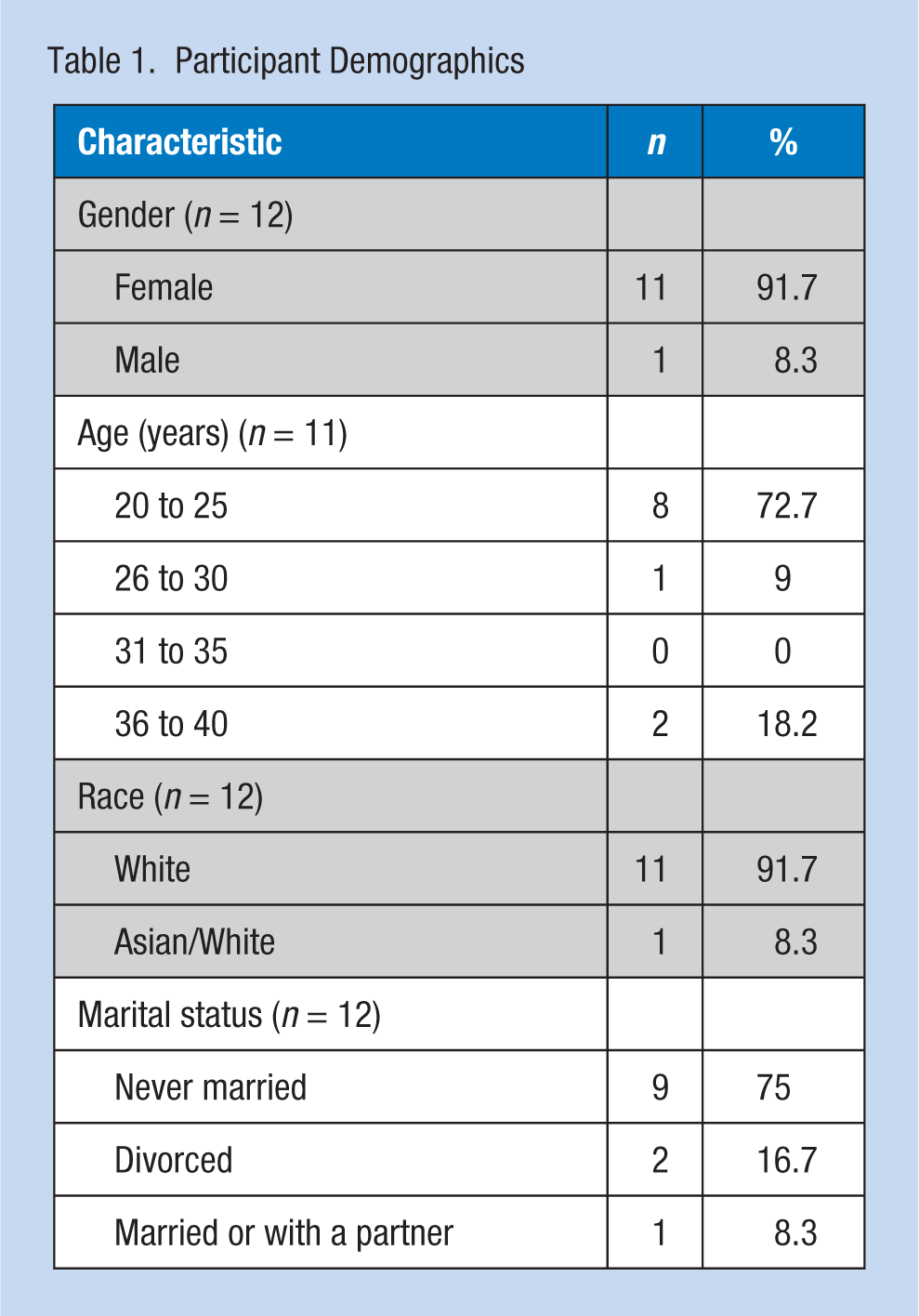
Participants (n = 12) were predominately female, White, unmarried, and between the ages of 20 and 25 years (Table 1). Clinical placements and shifts varied, with the majority working shifts longer than 8 hours and approximately half working night shift (Table 2).
Participant Demographics
Practicum Placement Sites, Shift, and Hours Worked
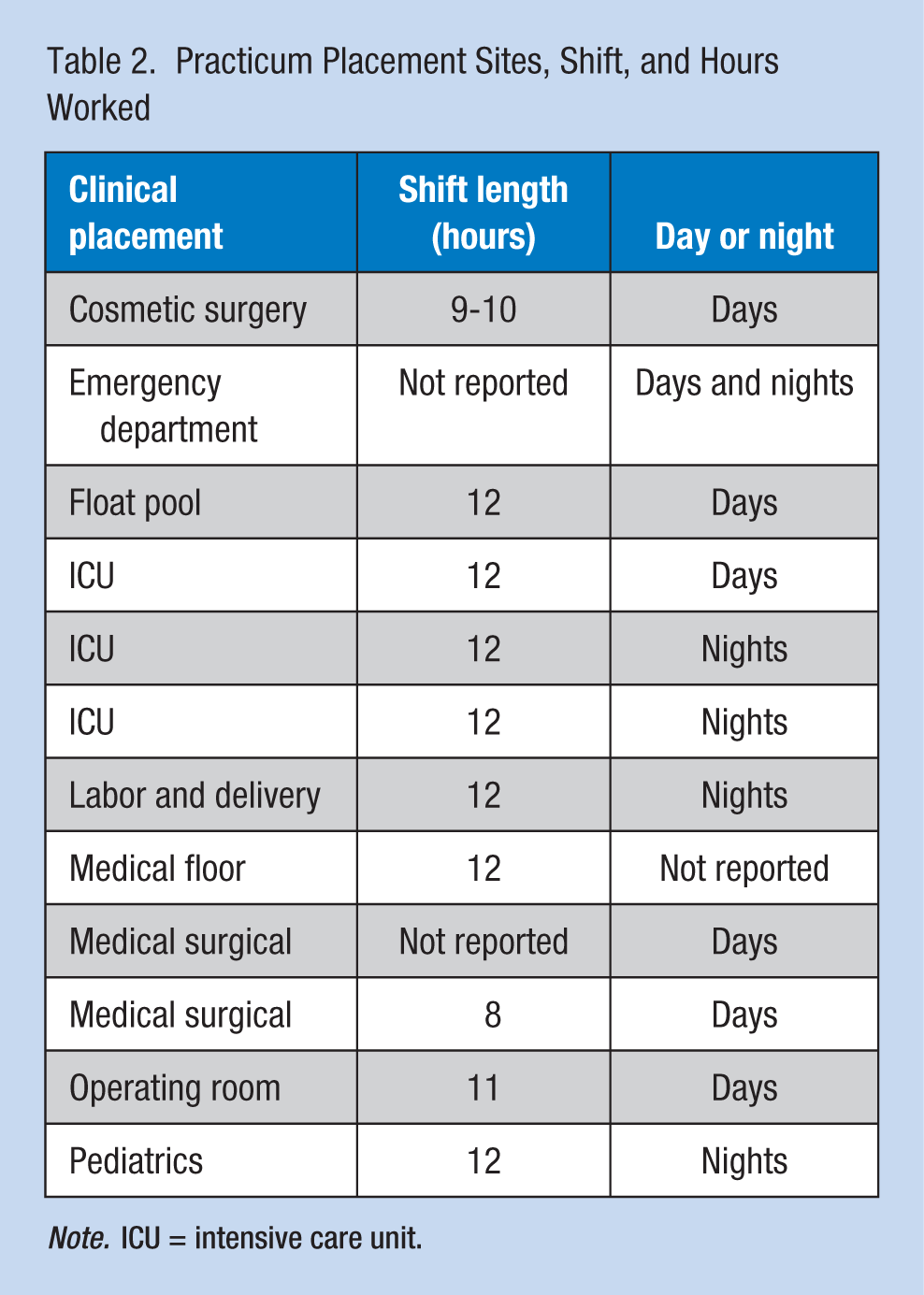
Note. ICU = intensive care unit.
Round 1: Identifying Problems
The first half of each round of focus groups focused on “problems” in the IDEAS process. “Sub-issues,” which were more descriptive than “problems,” were used to code and categorize problems into those that impacted (a) personal well-being and (b) workplace well-being.
Problems associated with personal well-being
Participants reported feeling anxious and isolated as they transitioned from the classroom to time-intensive clinical practice. They noted that their anxiety impacted falling asleep and staying asleep. Participants described simultaneous pressures of completing practica, preparing for the licensure examination, and interviewing for future employment as additional sources of anxiety. One participant shared, “Your mind is racing . . . we’re constantly learning, and so when we come home, we are thinking about that. It’s running through our heads.” Students also reported feeling socially isolated from peers and family due to working night and lengthy shifts. A student summarized by stating, “ . . . I think for a lot of us it felt like drinking out of a fire hose . . . Then that adds to the isolation, and the anxiety, and—the stress . . . and then you don’t sleep.”
Ways in which shift work impacted physical health included disrupted sleeping and unhealthy eating habits, increased use of caffeine, and decreased exercise. Specifically, participants identified problems transitioning between schedules, transitioning from work to sleep, getting to sleep at irregular times, and staying asleep. Falling asleep was impeded by package deliveries, pets, roommates, children, and light. Once asleep, participants spoke of waking up suddenly: “You may fall asleep, but then you’re sleeping, and then all of a sudden, you’re like—You’re having a dream that you’re just messing up something in clinical, which I’ve done.” Nutrition was driven by short-term needs, especially at critical times during the shift (e.g., 5:00 a.m.). Sugar and caffeinated products were used as “pick me ups.” A lack of time for exercise, which had been used to “de-stress,” also impacted participants’ quality of life.
Shift work impacted participants’ personal safety outside of work, primarily when driving home after a long shift. A participant shared, “I was tired, and I did a very, very large yawn, and in the middle of my yawn, I closed my eyes, and I rear ended the person in front of me.” Another participant questioned her decision-making when she stated, “I would keep it cold, just so that I would stay awake, and I would talk to myself. You can’t drive drunk, but you can drive this tired?”
Problems associated with workplace well-being
Organizational culture impacted well-being with participants noting that they conceded to the norms of the clinical unit, which, in turn, had a deleterious effect on their health. Participants discussed the lack of regular breaks, staying past their shift, fluctuating shifts, and the lack of exposure they had to night or 12-hour shifts. One participant, whose preceptor worked in the emergency department, shared that they rarely took breaks and . . . at least three times, when we sat down for lunch, within five minutes, there was a code blue or a trauma code, and so we’d just shovel our food and then go back and never actually took our full half-hour.
Other participants were invited to take a break, but did not “Because there’s so much to do.” Another noted that the preceptor encouraged her to take a break. The participant went on to say, “I was trying to get a job in this department, so I didn’t wanna be like, ‘Time for my break.’”
Participants described the impact that shift work had on patient safety in terms of feeling a lack of focus, moving slowly, making medication errors, and feeling irritable and unmotivated. One participant recognized that a lack of focus affects “assessments, calculations, and then interaction with the patient.”
Round 2: Identifying Solutions
The second half of each round of focus groups focused on “solutions” in the IDEAS process. Participants identified solutions in response to each problem they previously identified. Solutions were categorized into those that impacted personal well-being, impacted workplace well-being, or were related to the curriculum.
Solutions associated with personal well-being
Participants identified diverse strategies to decrease stress, anxiety, and isolation during this transitional period. Participants talked about the need for an adequate support system to decrease isolation, primarily with their nursing student peers. “Debriefing” was emphasized as a way to “ . . . unwind and talk about your day with somebody . . . that knows what you’re going through.” Participants stressed that this could be brief and occur as a clinical conference once a week through video.
Participants provided multiple suggestions for maintaining their physical health while working long and erratic hours, including building in time to decompress, relax, and meditate to get to sleep. Other ideas included purchasing fans to create white noise, a sunrise/sunset light, and blackout curtains. To improve sleep quality, participants suggested establishing a consistent bedtime routine. Others encouraged clear communication with roommates and family members to let them know about revised sleep schedules, but cautioned others to “ . . . set some time aside for friends and family . . . ” They cautioned against using electronics before bed; watching television to “wind down”; taking Nyquil, melatonin, or Benadryl to sleep; or drinking caffeinated drinks at work to stay awake.
Solutions to unhealthy eating included prepping meals in advance, finding easy healthy meals, and bringing a water bottle to clinical. Participants suggested consuming smoothies or vitamin drinks, and eating nuts and protein bars to get through long shifts. Modifying regular exercise routines was emphasized as a way to “keep that stress level down and to keep that norm.” Other ideas included at home workouts (e.g., bike trainer) and stretching.
Participants offered strategies (i.e., blasting cold air, talking to self or someone on the phone, singing, eating snacks, pulling over to catnap, and staying with a friend to avoid driving) to prevent falling asleep while driving home after a long shift.
Solutions associated with workplace well-being
Participants identified solutions to improve workplace well-being through a variety of mechanisms. They recommended that the college offer earlier opportunities to experience night and 12-hour shifts and that faculty assist participants to anticipate clinical settings in which night shift will be required. They suggested lengthier clinical practica so students had more time to align their schedules with their clinical preceptors’ schedules.
Solutions were offered to ensure breaks and meal times. One suggestion was to mandate break times in contracts between hospitals and the college. A participant suggested that nurse managers tell students that they have a right to take a break and faculty reinforce students’ rights to take breaks with preceptors. Participants recognized the need to assert their right to take a break and articulated the importance of time away from the unit. Likewise, participants spoke about the importance of clear communication with clinical preceptors around expectations to come in early or stay late after a shift. Participants discussed ways to assess the organizational culture when looking for employment, including asking whether the unit has a resource nurse or a float nurse to relieve staff, whether the charge nurse schedules breaks for staff, whether the nurses are unionized, and if the hospital has earned awards for nursing or organizational excellence.
Creating a culture of safety by building team work into the workplace infrastructure was discussed as essential for patient safety. Participants discussed the importance of appropriate patient assignments for participant nurses, and working in an environment where questions are welcome.
Solutions related to curriculum
When prompted, participants identified curricular changes and pedagogical approaches to teaching students about shift work. Participants suggested learning sleep pathology in medical-surgical nursing, applying published findings about the “impact of lack of sleep on patient safety,” and writing “implications on self-care” for an evidence-based practice course. A participant suggested having students complete medication calculations after staying up all night to “wake them up” to how their brain is functioning. When queried specifically about sleep health education, students responded that they would have been receptive to a sleep education module. Finally, skills such as advocating that they take breaks could be taught in the “transition to practice” or leadership class.
Discussion
Participants were forthcoming in voicing concerns about health and safety during their transition to longer hours and shift work. Problems identified addressed a range of issues, from not knowing when to eat during night shift to feeling overstimulated and isolated when they returned home after their shifts. Of note were participants’ concerns about drowsy driving; numerous comments addressed feeling impaired (at a level analogous to driving drunk) and using a variety of strategies to stay focused. Participants worked to mitigate fatigue by increasing caffeine intake. Parallel to concerns about their own health, participants also expressed doubt about their ability to make medication calculations and respond to patients’ needs in an effective and timely way.
Without exception, participants stated that they needed regular breaks to reestablish their physical and mental health equilibrium. They felt reluctant to take breaks if their preceptor did not. Some participants noted unit-level cultures where staff did not take breaks; others reported being on units where nurses circulated among themselves, offering social and instrumental support as well as encouraging each other to take breaks. Participants felt strongly that the college should ensure that students received regular breaks; they requested that faculty reinforce this expectation in all conversations with preceptors.
Study findings aligned well with related research addressing stressors during transitions in nursing. In their study examining senior nursing students’ expectations of work and the workforce, Saber, Anglade, and Schirle (2016) described role transition as the greatest stressor students encountered. A second stressor was the impact that nursing schedules had on their personal lives. Student nurses reported coping strategies for each stressor, including working in environments that support transitions (e.g., nursing residency programs) and identifying mentors. Adequate rest was identified as a strategy for self-care amid erratic work schedules, as was creating a network of coworkers willing to change schedules if needed.
Findings reinforced the TWH model in that participants framed almost every issue from a cross-cutting personal health and worksite safety perspective. Although it remains unclear whether this was an artifact of student nurse (versus employed worker) status, participants in this sample did not delineate between their own health goals (e.g., adequate nutrition, regular exercise) and safe practices on the job. Rather participants saw their personal and worksite well-being as logical extensions of each other; in addition, a number of statements provided evidence that participants saw their own ability to be mentally and emotionally “present” as a central antecedent to safe patient care.
Limitations of this study include the small sample from a single university. Study participants were predominantly White and relatively young, thus providing an incomplete representation of diversity in the national student nurse population. Likewise, the sample was drawn from a program that mandated a clinically intense and time-consuming clinical capstone immediately before graduation, one of many curricular approaches to assure their students are employment ready.
Strengths of the study include an adequate fit between the structured participatory method and participants’ framing of health and safety issues. Convening focus groups immediately following the last clinical rotation was critical because the sense of their experiences was close at hand. The way participants eagerly offered their concerns and snow-balled their ideas among each other indicated that study questions about personal and worksite health and safety resonated deeply and personally with these students at that juncture in time. The number of similarities between the two rounds validated the findings.
Implications for Practice
Participants were aware that they were entering a critical transition time, not only in their work lives but also as young women and men. As reported in related literature, they wanted to enter their professional lives in a thoughtful precautionary manner that would allow them to balance the rewards and demands of work, family, friends, personal health, and restorative time (Butterfield, 2016; Gidman, McIntosh, Melling, & Smith, 2011; Saber, 2013). Their conceptualizations of occupational health and safety and personal wellness aligned well with multifaceted interventions in both nursing education and clinical practice environments.
One outcome of the study is that faculty at the study college are considering incorporating the “The National Institute for Occupational Safety and Health (NIOSH) training for nurses on shift work and long work hours,” into the curriculum. The training consists of 12 modules (4 hours) covering the concepts of sleep and circadian disruption, risks of shift work-related fatigue, and actionable information on risk mitigation. The training has yet to be empirically tested for its effectiveness in improving nurses’ occupational health outcomes; thus implementation could offer researchers in the college an opportunity to evaluate the impact of such training (NIOSH et al., 2015).
Hospital and nursing executives can support nurses’ transitions by (a) developing processes to discuss workplace and scheduling stressors with employees, (b) incorporating newly licensed registered nurses (RNs) in committees with decision-making authority, and (c) increasing collaboration between schools of nursing and hospitals so that newly licensed RNs can speak to students about workplace realities (Saber et al., 2016). Nurse residency programs, although not uniformly available throughout the country, also provide a mechanism for structured support and mentoring of novice nurses; such programs have been demonstrated to increase job satisfaction and decrease turnover (Welding, 2011).
In summary, student nurses may benefit from both institutional (e.g., policies addressing enforcement of break times) and personal (e.g., education and anticipatory guidance addressing shift work) actions in support of worker health and safety and safe patient care (Butterfield, 2016). Faculty should be mindful that the stewardship of tomorrow’s nursing workforce begins in today’s classrooms, providing proactive education that prepares nurses for a lifetime of health and safe practice.
Applying Research to Practice
Nursing education programs can use findings from this study to inform their curriculum and scheduling decisions regarding clinical practicum expectations for undergraduate nursing students. Participants in this study frequently reported fatigue, sleep disturbances, and overstimulation on clinical days; drowsy driving was repeatedly noted as a concern for self and others on the road. Curricular changes suggested by participants focused on the need for detailed education addressing sleep hygiene, work life balance, the judicious use of caffeine, setting sleep schedules, and de-stressing prior sleep. Participants also noted the importance of support from friends, peers, and faculty supervisors during intense clinical shift work. Finally, participants wanted assurance from their program directors that regular work breaks would be enforced for all students; this finding also has broad implications for hospitals hiring new nurses and other professionals where evening, night, and long shifts are an expectation. The study provides preliminary evidence that student nurses viewed their clinical work expectations, home lives, and personal wellness goals in a holistic manner that aligned well with a Total Worker Health perspective.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by NIOSH U19 OH010154, Oregon Healthy Workforce Center.
Author Biographies
Julie Postma is an Associate Professor at the College of Nursing, Washington State University.
Erica Tuell is a Research Coordinator at the College of Nursing, Washington State University.
Lois James is an Assistant Professor at the College of Nursing, Washington State University.
Janessa M. Graves is an Assistant Professor at the College of Nursing, Washington State University.
Patricia Butterfield is the Associate Dean for Research at the Elson S. Floyd College of Medicine, Washington State University.