
Abstract
Background
Most meatpacking workers have pain affecting their back, arms, and/or wrists from work-related repetitive motions, forceful exertion, and awkward positioning. Chronic musculoskeletal pain is associated with obesity, hypertension, type II diabetes, heart attack, and stroke. Hispanic/Latino workers in the meatpacking industry are a vulnerable population; limited English, lack of health insurance, and fear of deportation often deter them from seeking care where preventable cardiovascular risks might be detected. The purpose of this study was to examine perceived health and actual cardiovascular risk among Hispanic/Latino meatpacking workers with musculoskeletal pain in Nebraska.
Methods
Structured interviews were used to examine perceived health, awareness of cardiometabolic risk, and capacity for health self-management. Body mass index (BMI), lipids, blood pressure, Hemoglobin A1c (HbA1c), and cardiorespiratory fitness (step test) were used to examine cardiovascular risk.
Findings
Of those interviewed (n = 39), musculoskeletal pain affected usual life activities in 64% (n = 25) of participants. Of those tested (n = 30), 93% (n = 28) had a BMI > 30 kg/m2, 86% (n = 26) had at least one lipid abnormality, 50% (n = 15) had blood pressure > 120/80 mm Hg, and 43% (n = 13) had an HbA1c > 5.7%. Males had greater fitness than females (p = .03), but also greater lifetime risk of heart attack or stroke compared with females (p = .02).
Conclusion/Application to Practice
In this sample, cardiovascular risk exceeded that found in the general Hispanic population in the United States. Occupational health nurses can assist workers to be aware of their risk by measuring and providing culturally and linguistically appropriate education on blood pressure, BMI, cholesterol, and HbA1c.
Background
Meat production in the United States (U.S.) depends on the health of the workers who perform manual labor in meat processing (meatpacking) facilities. Injury and illness rates in meatpacking have consistently surpassed that of any other industry since reporting began in the early 1990s (Government Accountability Office, 2016). Most meatpackers work with pain; over 90% have reported pain affecting their upper back, arms, and/or wrists (Quandt et al., 2006; Tirloni et al., 2012). In the general population, musculoskeletal pain and/or conditions are associated with depression (Faoro et al., 2018), obesity (Walsh et al., 2018), elevated low-density lipoprotein (LDL; Kumagai et al., 2018), hypertension and diabetes (Williams et al., 2018), and cardiovascular disease (Oliveira et al., 2020). People with chronic musculoskeletal pain are nearly twice as likely to have cardiovascular disease (Oliveira et al., 2020). Reasons for this are thought to be related to pain-induced physical limitations and psychological distress that leads to physical inactivity, a known risk factor for cardiovascular disease. In addition, chronic pain is associated with inflammation and use of nonsteroidal anti-inflammatory medications, both of which are risk factors for heart attack and stroke (Oliveira et al., 2020).
Poor health among meatpacking workers has long been attributed to the combination of hazardous working conditions, socioeconomic position of workers, and structural barriers limiting access to health-related resources. Hispanic/Latino adults (HLA) comprise an estimated 45% of the meatpacking workforce (Fremstad et al., 2020). Approximately half of all meatpacking workers are undocumented immigrants (Passel & Cohn, 2016) and most are not covered by employer-based health insurance (Barnett & Vornovitsky, 2015). Language barriers and immigration-related fears often deter workers from addressing job-related safety and general health issues (Ramos et al., 2020, 2021).
Beyond muscle and joint pain, little is known about other chronic health problems faced by the HLA men and women who work in meatpacking facilities. Although depression and psychological distress have been described in Midwestern meatpacking workers (Lander et al., 2016; Leibler et al., 2017; Ramos et al., 2020), the prevalence of preventable chronic conditions such as hypertension and type II diabetes is not clear. In the general U.S. HLA population, an estimated 40% have diagnosed hypertension and 14% have diagnosed type II diabetes (Virani Salim et al., 2020). Ongoing surveillance data in U.S. women shows HLA women consistently have lower awareness of cardiovascular disease risk, symptoms, and prevention measures compared with non-Hispanic Whites (Mosca et al., 2013). During the coronavirus pandemic, meatpacking workers were deemed “essential.” Although the literature examining both occupational and personal health characteristics of meatpacking workers is sparse, it suggests they are a vulnerable population with limited awareness, support, and/or resources to self-manage both acute (i.e., pain) and chronic (i.e., cardiovascular risk) health concerns. Undiagnosed and poorly managed chronic health conditions may place HLA at higher risk of COVID-19 infection, hospitalization, and death rates compared with non-Hispanic Whites (Hsu et al., 2020; Macias Gil et al., 2020). While musculoskeletal pain is a common health problem for meatpacking workers, little is known about the co-occurrence of cardiovascular risk in those workers who are HLA. This study will address this knowledge gap. The purpose of this descriptive study in HLA meatpacking workers with work-related musculoskeletal pain was to examine (a) their perceived general health status and (b) their actual cardiovascular risk. This article reports only on the quantitative results related to perceived health and cardiovascular risk. The qualitative findings on the occupational, physical, social, and service conditions factors affecting health are reported separately (Ramos et al., 2021).
Methods
A cross-sectional design with structured interviews to describe perceived general health and physical/biometrics assessments were used to examine cardiovascular risk among a sample of meatpacking HLAs who self-reported active work-related musculoskeletal pain.
Hispanic/Latino men and women, ages 19 to 65, currently employed in meatpacking with self-reported work-related musculoskeletal pain were eligible to participate in this study. The exclusion criteria were as follows: (a) unable to provide verbal consent, (b) answering “rarely” or “never” when questioned about having pain that negatively affected their life, and (c) not having at least one self-reported risk factor for cardiovascular disease: hypertension, type II diabetes, obesity, smoking or engaging in less than 30 minutes of leisure-time physical activity per week. To complete a 3-minute fitness test assessment, participants may not have been pregnant, physically unable to walk upstairs, or “high risk” for the occurrence of a cardiac event during fitness testing (Arena et al., 2014).
Participants were recruited through community-based organizations, Facebook promotions, Spanish-language radio ads, and word-of-mouth. Interested participants were to call the study coordinator to review eligibility and receive participation instructions. Informed consent was obtained in-person prior to enrolling participants. Data collection was conducted in both rural and urban community settings (e.g., public library, church, and nonprofit organization) near meatpacking plants located in Nebraska. Between March 2019 and May 2020, participants completed a structured interview (in-person or zoom video) and an in-person biometric assessment conducted in a private area within the community location by a bilingual nurse practitioner or by an English-speaking nurse practitioner with a Spanish-language interpreter. Participants were instructed to fast at least 8 hours prior to their biometric assessment. After the fasting lab work was collected, participants were offered healthy snacks and water while they waited to complete the remaining physical assessments. Participants received a US$20 gift card for completing a structured interview and an additional US$20 gift card for completing a biometric assessment (body mass index [BMI], fasting lab, and step test). This study was approved by the University of Nebraska Medical Center’s Institutional Review Board.
Measures
Questionnaires were collected via structured interview in-person or via zoom video. Lipids, HbA1c, and the step test were collected in-person.
The EuroQOL (EQ-5D-3L) was used to evaluate self-rated health across five areas: mobility, self-care, usual activities, pain, and anxiety/depression. Response options were 1 (no problems), 2 (some problems) and 3 (extreme problems). The measure also includes a visual analog scale that inquires about a current state of health rating from 0 or “worst imaginable health” to 100 or “best imaginable health” (Brooks & Group, 1996). The EuroQOL has test–re-test reliability (interclass coefficients .78 and .73; Brooks & Group, 1996).
The Patient Activation Measure (PAM®) was used to evaluate knowledge, skills, and confidence in health self-management (Hibbard et al., 2005). The original 13-item questionnaire had good internal consistency (Cronbach’s α = .87; Hibbard et al., 2005). In this study, internal consistency was acceptable (Cronbach’s α = .70).
The American Heart Association (AHA)/American College of Sports Medicine Health (ACSM)/Fitness Facility Preparticipation Screening Questionnaire was used to assess health history, symptoms, and/or risk factors of cardiometabolic conditions, including coronary artery disease, hypertension, diabetes, and dyslipidemia (Arena et al., 2014).
Whole capillary blood was collected via fingerstick and tested according to point-of-care procedures outlined by the Clinical Laboratory Standards Institute (Ernst & Clinical Laboratory Standards Institute, 2008). HbA1c was analyzed using the Alere Afinion AS100. Total cholesterol (TC), high-density lipoprotein (HDL), LDL, and triglyceride (TRIG) cholesterol were processed using the CardioChek Plus analyzer.
Efficiency of the heart and lungs working together to meet the oxygen demands of the body was measured using a submaximal step test (Arena et al., 2014). Participants used a self-selected pace to step up and down two steps (20 cm apart) 20 consecutive times using the Step Test and Exercise Prescription (STEP) protocol (Knight et al., 2014). Within 6 seconds of test completion, a posttest heart rate and the total time to complete the test were recorded. The posttest heart rate was compared with gender and age-specific normative standards for heart rate recovery to determine performance according to five categories: superior, excellent, good, fair, and poor (Knight et al., 2014).
The 30-year risk of a cardiovascular event was calculated using the LifetimeRisk Calculator (lifetimerisk.org). Self-report variables used in the risk calculator were gender, age, history of diabetes, and smoking status (Berry et al., 2012). Measured variables were systolic blood pressure (mmHg), BMI (kg/m2), total cholesterol, and fitness level in metabolic equivalents (METs). A 30-year risk of ≤4.7% was considered optimal (Berry et al., 2012).
An investigator developed demographic questionnaire was used to collect data on ethnicity, education, income, marital status, English proficiency, tenure in the U.S., and employment history.
Data Analysis
Analysis was conducted using the Statistical Package for Social Sciences (SPSS), version 25 software. The data were examined for missingness and normality. Means, standard deviations, and ranges were calculated for continuous variables. Frequencies and percentages were calculated for categorical variables. Mann–Whitney U and an independent t test were used to evaluate group differences by gender.
Results
A total of 39 participants completed a structured interview and 30 completed a biometric assessment (Figure 1). Participants in this study were predominately female (n = 21). Males and females were similar in terms of age and length of employment with their current meatpacking employer (Table 1). However, tenure living in the U.S. was longer among men compared with women, with a median of 30 and 14 years, respectively (p = .02).
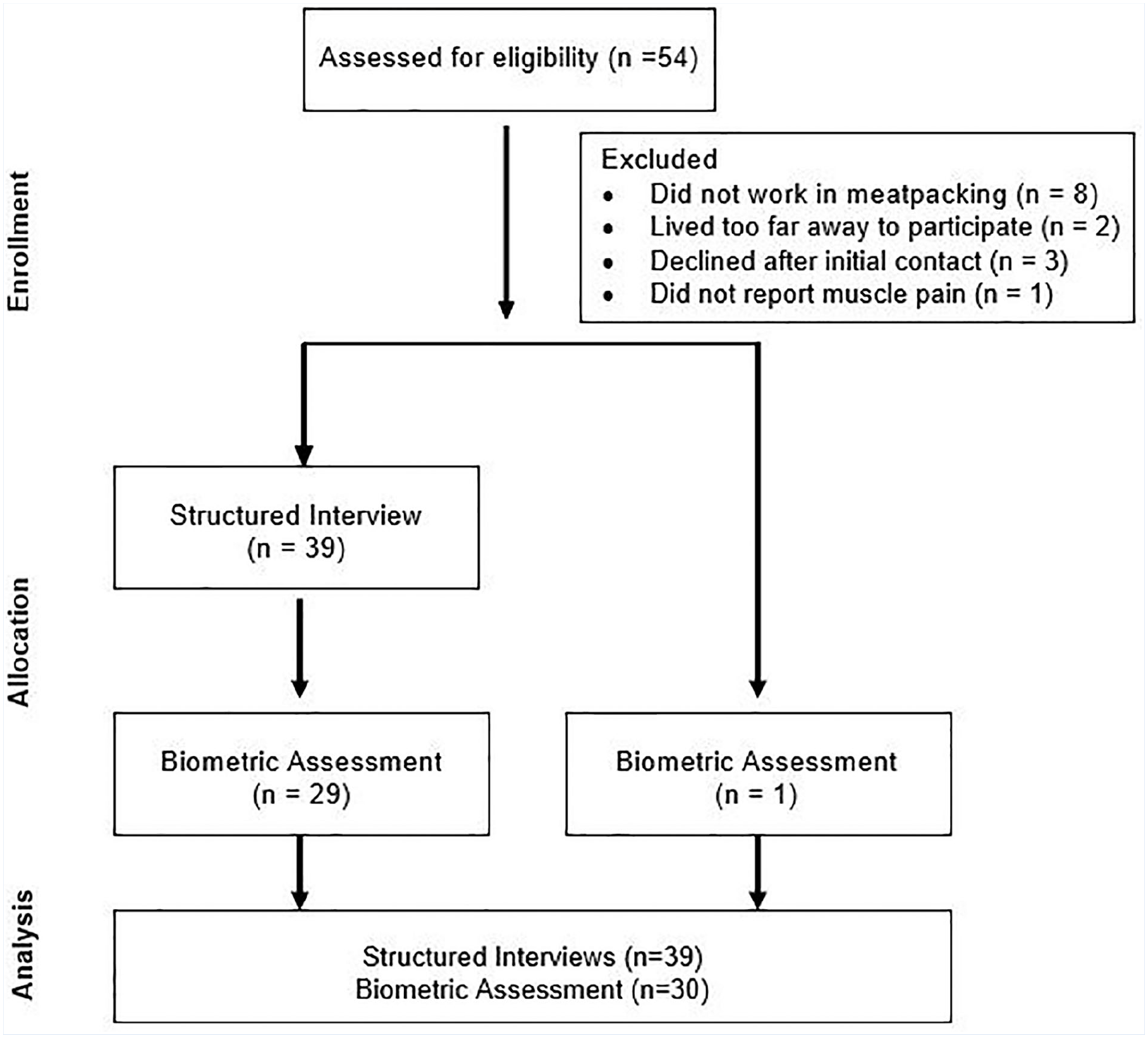
Study flow diagram.
Characteristics of Meatpacking Worker Participants (N = 39).
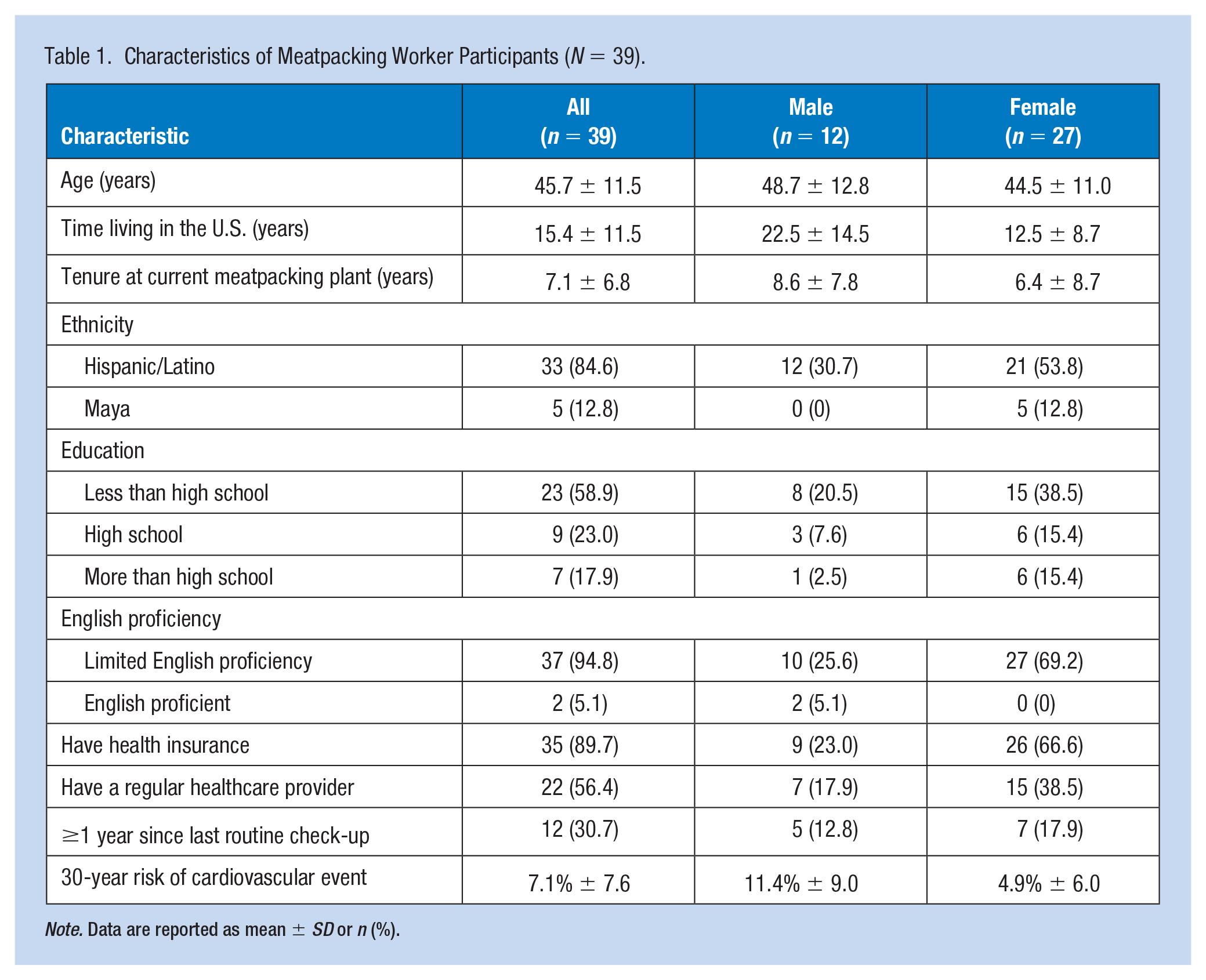
Note. Data are reported as mean ± SD or n (%).
Health status as measured by the biometric assessment indicated most participants had evidence of cardiometabolic risk; 95% had a BMI > 30 kg/m2, 43% had a HbA1c > 5.7%, 50% had a blood pressure > 120/80 mmHg, and 86% had at least one cholesterol abnormality (Table 2). Males had a higher level of cardiorespiratory fitness (estimated VO2max M = 39.7, SD = 6.14) compared with females (estimated VO2max M = 33.9, SD = 6.1; p = .03). Despite having greater fitness, males had a higher level of lifetime risk of heart attack or stroke with a median score of 8.75 compared with 2.20 for women (p = .02).
Participants With Cardiometabolic Risk and Their Awareness of Having Risk (N = 30).
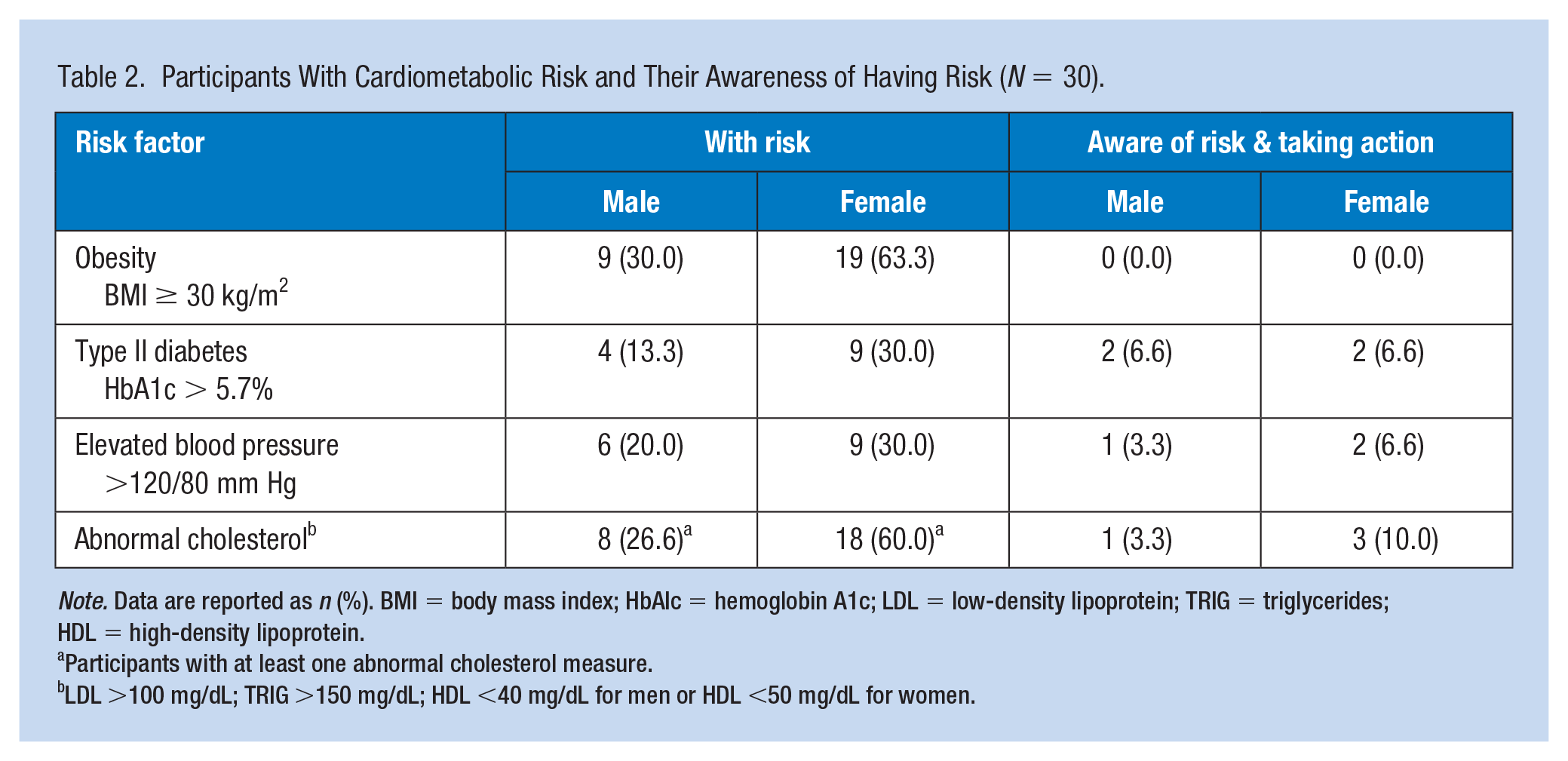
Note. Data are reported as n (%). BMI = body mass index; HbAIc = hemoglobin A1c; LDL = low-density lipoprotein; TRIG = triglycerides; HDL = high-density lipoprotein.
Participants with at least one abnormal cholesterol measure.
LDL >100 mg/dL; TRIG >150 mg/dL; HDL <40 mg/dL for men or HDL <50 mg/dL for women.
Perceived health status as measured by awareness of having cardiometabolic risk (i.e., elevated blood pressure, cholesterol, HbA1c) was measured using the AHA/ACSM Fitness Facility Preparticipation Screening Questionnaire. Most participants were unaware of their cardiometabolic risk (Table 2). On the EQ-5D-3L, participants rated their health as just above average with a mean of 69.2 (SD = 17.4, n = 39). Men rated their state of health slightly higher than the women with a mean of 71.6 (SD = 13.3, n = 12) compared with a mean of 68.7 (SD = 19.0, n = 27) for women. While most participants reported “no problems” with mobility, self-care, and usual activities, over half reported “some problems” when doing usual life activities (64%) and pain/discomfort (85%). Three participants (8%) reported “extreme problems” with pain/discomfort.
We found a mean score of 56.3 (SD = 8.7, n = 37) on the PAM-13, used to measure knowledge, skills, and confidence to self-manage health conditions, which is associated with a “beginner level” of self-management (Moljord et al., 2015). In this small sample, there were no statistically significant associations between self-rated general health status (EuroQOL), self-management (PAM-13), and actual abnormal cardiometabolic risks (i.e., hypertension, diabetes, obesity, hyperlipidemia).
Discussion
The findings of this study indicate there are unmet health and safety needs among HLA meatpacking workers in Nebraska. Work in meatpacking facilities has long been physically demanding with a high risk of acute and/or chronic injuries (Leibler & Perry, 2017; Tirloni et al., 2012, 2015). Participants in our study reported musculoskeletal pain affected their everyday activities. It is concerning that despite having health insurance, most were unaware and/or not addressing their cardiovascular risk by improving unhealthy behaviors (physical inactivity) or taking medications.
Efforts to address worker health safety in meatpacking began in the 1990s with the development of the Occupational Safety and Health Administration’s guidelines that focused on ergonomic conditions and production processes known to affect health and injury rates (Government Accountability Office, 2017). Since then, there has been a steady decline in the incidence of injury and illness in meatpacking; however, rates continue to surpass that of any other industry (Government Accountability Office, 2016) and more can be done to further reduce injury and illness rates. In addition, chronic health problems affecting work performance are going undetected in the HLA population. Among HLA in the U.S., the estimated prevalence of diagnosed type II diabetes is 15.1% for males and 14.1% for females (Virani Salim et al., 2020), but in this sample of HLA meatpacking workers, the prevalence of type II diabetes was twice as high, 44.5% for males and 43.0% for females. Sadly, only four of the 13 participants who had an elevated HbA1c were aware they had this preventable and manageable health condition. Other modifiable health risks found among study participants were elevated BMI and blood pressure and abnormal blood cholesterol. Most workers were either unaware of these risks or aware but not managing the health condition with medication and/or healthy physical activity. Because meatpacking work is physically demanding, it often increases the risk of injury and development of chronic diseases. Given that most meatpackers work with pain and are a vulnerable population with limited access to resources, occupational health and safety guidelines should expand their focus on assessing cardiovascular risk.
Implications for Occupational Health Nursing Practice
Along with work-related injury and illness, Total Worker Health also prioritizes health promotion outside of the work environment (National Institute for Occupational Safety and Health [NIOSH], 2020). Off-duty health behaviors have a direct impact on work attendance, performance, and longevity with the company (Jinnett et al., 2017). Occupational health professionals are called to support workers to self-manage their health by raising awareness of personal risk. Blood pressure and BMI measurement are low-cost nursing interventions that are invaluable as a first step in developing self-management skills in those at risk. Hosting regular health fairs to check cholesterol and HbA1c levels at the workplace can be managed in-house or outsourced. Space within the occupational health office could be designated as “self-serve” where workers can check their own blood pressure with a digital arm cuff and/or get information on common health problems. Screening results and educational materials should be provided to the workers in their preferred language. Policies and practices should be reviewed for how they prevent or promote Total Worker Health. NIOSH has practical tools to support planning, assessment, and evaluation of Total Worker Health efforts. For example, occupational health professionals might consider completing the Centers for Disease Control and Prevention (CDC) Worksite Health Scorecard to determine organizational strengths and opportunities in implementing evidence-based strategies to improve employee health and well-being (CDC, 2019). This scorecard is a free resource to evaluate employer programs, polices, and environmental factors across 18 different areas, including organization supports, blood pressure, cholesterol, physical activity, weight management, and musculoskeletal disorders.
Applying Research to Occupational Health Practice
This study examined perceived and health in Nebraska Hispanic/Latino meatpacking workers who have work-related musculoskeletal pain. Although these workers reported their health as “just above average,” most workers reported at least “some problems” with usual life activities due to work-related pain. Due to the increased risk of cardiovascular disease with chronic pain, the workers’ cardiovascular risk was measured. The prevalence of obesity, lipid abnormalities, and elevated HbA1c was higher in these workers than in the general Hispanic/Latino population. On the measure of engagement with health care, this sample of workers scored at a “beginner” level. Occupational health professionals are encouraged to use a Total Worker Health approach and include cardiovascular risk screening, culturally and linguistically appropriate education, and referral to help reduce health disparities among these essential workers.
Footnotes
Acknowledgements
We thank our participants for their willingness to engage in research and the community agencies who promoted the study and shared their space for data collection: Latino Center of the Midlands, Comunidad Maya Pixan Ixim, and Crete Public Schools Special Programs.
Author Contributions
S.R. contributed to conceptualization, funding acquisition, investigation, curation, analysis, and writing. A.R. contributed to conceptualization, methodology, investigation, curation, analysis, and writing. M.C.-S. contributed to investigation, curation, analysis, and writing. N.T. contributed to investigation, curation, analysis, and writing. R.J.-B. contributed to curation and writing. L.S. contributed to analysis and writing. S.Q. contributed to curation and writing. B.P. contributed to conceptualization, analysis, and writing.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Nebraska Tobacco Settlement Biomedical Research Development Fund (NTSBRDF) 2018–2020.
Author Biographies
Sheri A. Rowland, PhD, APRN-BC FNP, is an assistant professor at the University of Nebraska Medical Center in the College of Nursing. Sheri conducts research on health behaviors to manage cardiovascular risk through workplace and community-based interventions.
Athena K. Ramos, PhD, MBA, MS, CPM, is an assistant professor at the University of Nebraska Medical Center in the Department of Health Promotion in the College of Public Health. She conducts research on occupational health and safety of workers within the agri-food system and well-being initiatives within Latino and immigrant communities.
Marcela Carvajal-Suarez, MPH, is an Outreach Project Specialist at the University of Nebraska Medical Center, College of Public Health, Center for Reducing Health Disparities, in Omaha, Nebraska. Her work focuses on community-based health research and education initiatives in tobacco control, health, and safety among immigrant workers of the agricultural and food industries, and community well-being.
Natalia Trinidad, MPH, is an Outreach Project Associate at the University of Nebraska Medical Center, College of Public Health, Center for Reducing Health Disparities. Natalia assists in research projects related to health disparities among the Latino population.
Rebecca Johnson-Beller, BSN, RN, is a graduate research assistant at the University of Nebraska Medical Center College of Nursing. Rebecca is interested in decreasing the prevalence of cardiovascular disease by focusing on modifiable risk factors.
Leeza Struwe, PhD, MSN, RN, is an assistant professor in the College of Nursing at the University of Nebraska Medical Center. As a biostatistician, Leeza provides consultation to researchers on study design, power analysis, measurement tools, and data analysis.
Sophia A. Quintero, MPH, is a research assistant with the Center for Reducing Health Disparities at the University of Nebraska Medical Center’s College of Public Health.
Bunny Pozehl, PhD, APRN-NP, FHFSA, FAHA, FAAN, is a professor at the University of Nebraska Medical Center in the College of Nursing. As an NIH (National Institutes of Health)–funded researcher, Bunny focuses on physical activity behavior and health-related outcomes in heart failure patients.