
Abstract
Background:
Ischemic heart disease (IHD) is the major cause of duty-related fatalities in the fire service. Age and career length are not only important risk factors associated with IHD, but are also highly correlated. The aim of this secondary analyses was to assess the relationship between age, career length, and IHD, based on ischemic severity, to identify whether age or career length had a stronger relationship to IHD.
Methods:
This was a secondary, correlational analysis of on-duty firefighters without known cardiovascular or respiratory disease who underwent exercise treadmill testing with 12-lead electrocardiography. Ischemia was defined based on current guidelines. Maximum ST-segment depression was measured to determine IHD ischemic severity. Age, years of employment, demographics, weight, blood pressure were recorded. Multiple correlations were computed between age, career length, and IHD.
Findings:
Twenty-two firefighters were included (96% male, 82% White, 82% overweight or obese, 77% hypertensive). The partial correlation between maximum ST-segment depression and age controlled for career length was not significant (r = –.392, p = .079). The partial correlation between maximum ST-segment depression and career length controlled for age was statistically significant (r = .466, p = .033).
Conclusion/Application to Practice:
Career length, not age, moderately correlates with IHD ischemic severity among firefighters. Career length is a proxy measure of occupational exposures which contributes to IHD. When assessing IHD risk in firefighters, health practitioners should consider incorporating the occupational exposure history (i.e., career length) in addition to age when providing risk reduction services.
Keywords
Background
Ischemic heart disease (IHD) is the leading underlying cause of morbidity and mortality among on-service professional firefighters yet screening for IHD remains a challenge because of the inter-relatedness of risk factors (Dzikowicz & Carey, 2020; Smith et al., 2019; Wimberley, 2016). Recognized IHD risk factors include older age, male sex, hypertension, and obesity (Al-Zaiti & Carey, 2015; Dzikowicz & Carey, 2019a; Holdsworth et al., 2019). Occupationally related IHD risk factors specific to the fire service have been identified and include exposure to hazardous chemicals, sleep deprivation, chronic stress, and career length (Carey, Al-Zaiti, Dean, et al., 2011; Cohen et al., 2019; Holdsworth et al., 2019; Holtermann et al., 2012). Age and career length are important but highly correlated IHD risk factors among professional firefighters because firefighter careers start at a young age and last for several decades. Given that age and career length have significant overlap, it is unclear if one is a better correlate of IHD and thus a potentially superior risk factor than the other (Baur et al., 2012; Holdsworth et al., 2019).
The purpose of this study was to assess the relationships between age, career length, and IHD, based on ischemic severity, to identify whether age or career length had a stronger relationship to IHD. To perform this analysis, we used partial and part correlations and discuss the methodology in greater detail to inform readers.
Methods
Data for this analysis were collected from the Surveying & Assessing Firefighters Fitness & Electrocardiogram (SAFFE) study. The SAFFE study was conducted between 2008 and 2010, and the design has been previously described (Al-Zaiti & Carey, 2015; Carey, Al-Zaiti, Dean, et al., 2011; Dzikowicz & Carey, 2019a, 2019b). This analysis of the SAFFE study was a planned sub-study that included 22 firefighters who were randomly selected to participate. Exclusion criteria included firefighters who received treatment for either a cardiovascular or respiratory disease, were unable to exercise due to musculoskeletal conditions, or reported symptoms during exercise (i.e., chest pain). A power analysis using G*Power (Version 3.1.9.4) was performed with a sample size of 22 and computed a total power of 75%, therefore we were limited to correlational analyses.
For this study, demographic and anthropometric data were collected. Demographic data were self-reported and included age, medical comorbidities and treatments, career length, and position at fire department (i.e., firefighter, driver, or officer). Anthropometric data were assessed by a Registered Nurse (RN) and included height (m), weight (kg), body mass index (BMI, kg/m2), and resting blood pressure (mmHg). Body mass index categories included the following: Underweight was less than 18.5 kg/m2; Normal was 18.5 kg/m2 up to but less than 25 kg/m2; Overweight was 25.0 kg/m2 up to but less than 30 kg/m2; and obese was 30.0 kg/m2 or greater (Calle et al., 1999). Blood pressure categories included normal systolic <120 mmHg and diastolic <80 mmHg, elevated as systolic 120 to 129 mmHg and diastolic <80 mmHg, hypertension stage I as systolic 130 to 139 mmHg or diastolic 80 to 89 mmHg, and hypertension stage II as systolic ≥140 or diastolic ≥90 mmHg (Whelton et al., 2018).
After collection of baseline demographic and anthropometric data, firefighters underwent an exercise stress test using the Bruce protocol on the X-Scribe™ exercise stress testing system (Mortara Instruments; Milwaukee, WI; Bruce et al., 1973). The firefighters were instructed to continue exercising as long as possible so long as they did not experience symptoms (e.g., chest pain, shortness of breath). Diagnostic quality 12-lead electrocardiograms (ECGs) were obtained wirelessly from the X-Scribe™ exercise stress testing system, and displayed on a high-definition screen. The system automatically computed an average ST-segment amplitude for each ECG lead and compared this value with a resting baseline to increase the sensitivity of detecting even minor ST-segment changes. All ECGs were reviewed and annotated by a PhD-prepared nurse practitioner (PhD, Acute Care Nurse Practitioner, RN) blinded to the study, and verified by a second PhD-prepared nurse (PhD, RN). According to clinical guidelines, ischemia was considered pathological if the presence of exercise-induced, horizontal ST-segment depression ≥ 2 mm at 0.08 seconds from the J point in ≥ 2 contagious leads for ≥ 30 seconds at peak or recovery of exercise (Gibbons et al., 2002). The maximum sustained ST-segment depression was measured and used to assess severity of IHD (Desmet et al., 2004). Metabolic equivalents of task (METs), defined as a ratio of the metabolic rate during exercise to the metabolic rate at rest, were also measured as a measure of activity intensity (1 MET = 3.5 mL O2·kg−1·min−1; Ainsworth et al., 1993). Maximum speed (miles per hour, mph) and maximum incline (% from baseline) were measured.
All analyses were conducted using R (R Core Team, 2017, Version 4.02, Vienna Austria; Kim, 2015). Statistical significance was considered when p < .05. Continuous variables were assessed for normality with the Shapiro–Wilk Test, and the distribution of variables was assessed by visual inspection. No transformations were necessary. Categorical variables are provided as % (n) and continuous variables as mean ± standard deviation (SD). Bivariate Pearson’s r correlations, that is, zero-order correlations and partial and part Spearman’s r correlations were computed using the variables maximum ST-segment change, age, and career length. Of note, partial and part correlations were used to express the specific portion of variance explained between two variables by removing the variance of another variable (Kim, 2015). The partial correlation specifically removed the variance of a third variable on both the independent and dependent variable, while the part correlation only removed the variance with the independent variable (Kim, 2015). The findings are reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) recommendations (von Elm et al., 2007).
Results
Twenty-two of the 122 SAFFE study firefighters were included in this sub-analysis (Table 1). This sample was largely male (96%, 21), middle-aged (46 ± 5.4 years), overweight or obese (82%, n = 18), hypertensive (77%, n = 18) and mid-to-senior career (17 ± 5.9 years of career service). Firefighters in this fire department worked 15-hour shifts with on-site housing for overnight shifts. Among the duties within the fire department, 41% (n = 9) were firefighters, 23% (n = 5) were firetruck drivers, and 36% (n = 8) were officers.
Firefighter Characteristics, n = 22
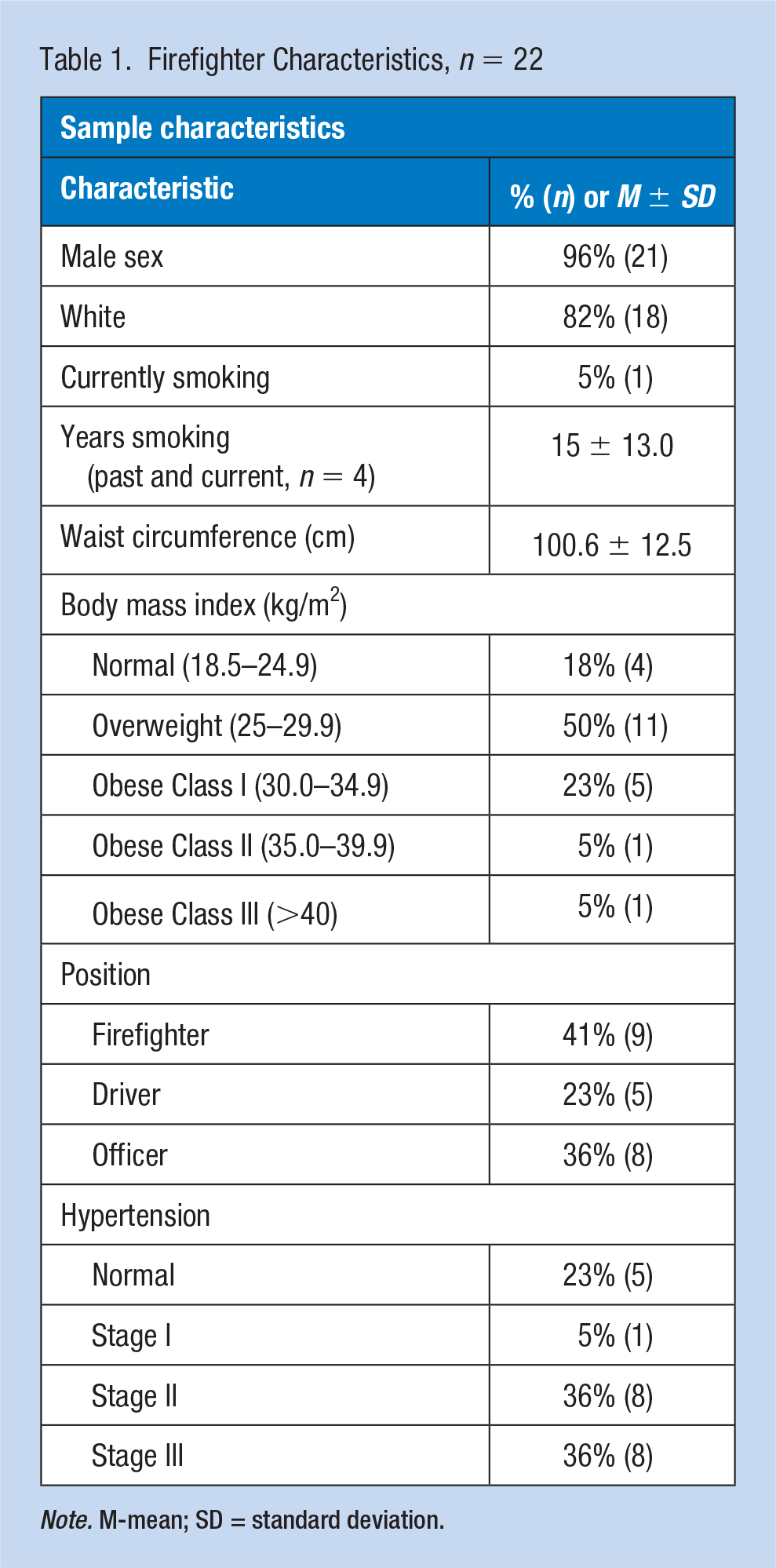
Note. M-mean; SD = standard deviation.
During exercise, 10 firefighters (46%) had pathological myocardial ischemia, with the mean maximum ST-segment depression being 2.5 ± 1.3 mm. Myocardial ischemia was distributed equally across coronary regions: 27% (n = 6) in the lateral wall, 36% (n = 8) in the inferior wall, and 36% (n = 8) in all cardiac walls. The mean treadmill time in which the maximum ST-segment depression occurred was 12.0 ± 2.2 minutes, which neared the end of treadmill testing given that the average total exercise time was 12.8 ± 2.0 minutes. The mean MET achieved during exercise was 13.0 ± 1.7, the mean maximum speed achieved during exercise was 4.8 ± 0.5 mph, and the mean maximum incline achieved during exercise was 18.4% ± 6.7%. Figure 1 is an example of a 12-lead ECG with pathological myocardial ischemia.
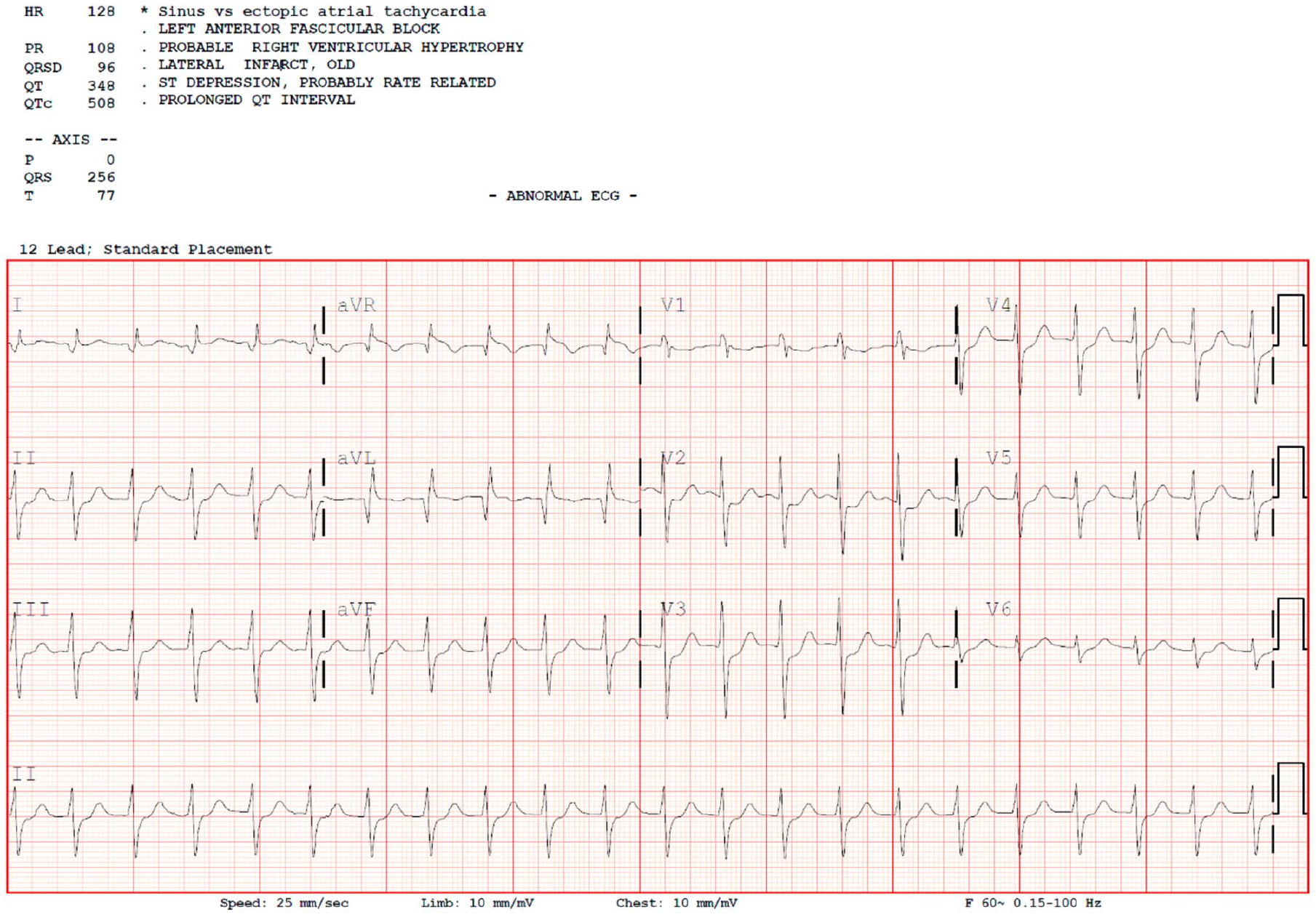
A 12-lead ECG recorded during Exercise Treadmill Testing of a 44-year-old male firefighter with a 22-year career length.
Next, we assessed the relationships between maximum ST-segment depression, age, and career length. The correlation matrix is provided in Table 2. The zero-order correlation between age and maximum ST-segment depression was .036 (p = .875), between career length and maximum ST-segment depression was .276 (p = .218), and between age and career length was .849 (p < .01). The partial correlation between career length and maximum of ST-segment depression controlled for age was .466 (p = .033), and the part correlation was the same. In comparison, the partial correlation between age and maximum ST-segment depression controlled for career length was –.392 (p = .079), and the part correlation was –.377 (p = .091). In summary, removing age from the relationship between maximum ST-segment depression and career length caused the strength to increase in the positive direction; whereas, removing career length from the relationship between maximum ST-segment depression and age also increased the strength of the relationship but in the negative direction.
Correlational Matrix Between Maximum ST-Segment Depression, Age, and Career Length Among Firefighters (n = 22)
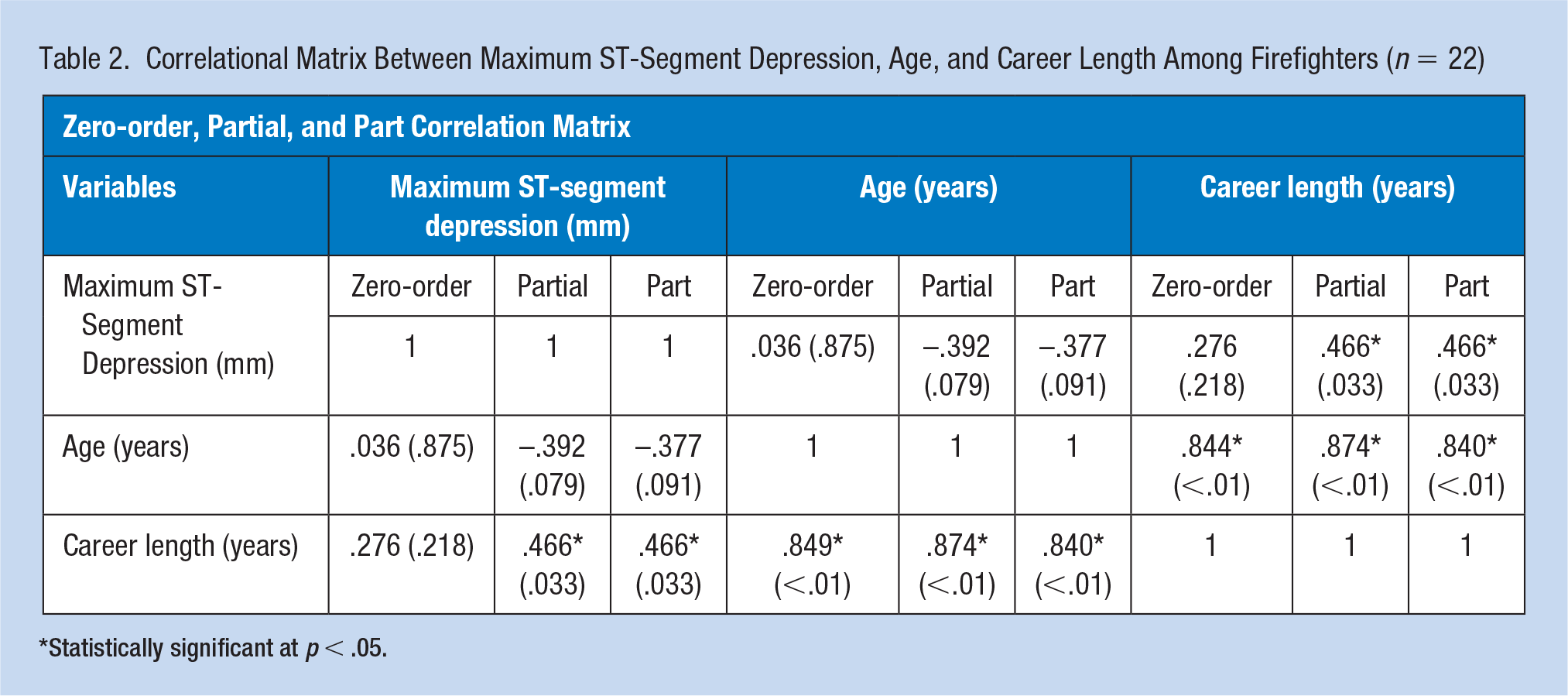
Statistically significant at p < .05.
Discussion
We investigated the relationships between maximum ST-segment depression during exercise as a measure of ischemic severity in IHD, age, and career length. We report essentially no relationship between age and maximum ST-segment depression; whereas, the relationship between career length and maximum ST-segment depression was modest. The partial correlation between age and maximum ST-segment depression controlled for career length produced a modest effect size but negative direction whereas the partial correlation between career length and maximum ST-segment depression controlled for age was larger and remained a positive. This suggests career length has a stronger association with IHD when compared with age.
Previous studies have used age and not career length when examining exercise and cardiovascular health among firefighters. Li et al. (2018) reported age greater than 55 years was a significant predictor of 10-year atherosclerotic cardiovascular disease risk, but when included with other significant predictors such as body fat percentage was no longer statistically significant. Gao et al. (2020) reported that cardiorespiratory fitness declined with age among firefighters, an expected finding although occupational risk factors most likely exacerbated the decline (Cohen et al., 2019). This strengthened the evidence found by Baur et al. (2012) that there was a prominent age-related decline in cardiorespiratory fitness among older firefighters, potentially exacerbated by occupational exposures although attenuated by physical activity. However, these papers do not directly assess career length similarly to age. Given the evidence from this small study, future analyses should compare career length and age in a larger population-based sample. Based on our results, we hypothesize career length may provide a more precise measurement of repeated exposures to occupational-related risks such as chronic stress, emissions, and poor sleep that are highly prevalent in the fire service and linked to cardiovascular health (Carey, Al-Zaiti, Dean, et al., 2011; Carey, Al-Zaiti, Liao, et al., 2011; Cohen et al., 2019; Holdsworth et al., 2019; Holtermann et al., 2012).
Interestingly, when career length was controlled for in the relationship between maximum ST-segment depression and age, the strength of the relationship increased but the direction became negative. This can be interpreted that younger age was associated with greater severity of ischemia after controlling for career length. The inverse relationship is counterintuitive given that the relationship between older age and myocardial ischemia is well established among firefighters (Al-Zaiti & Carey, 2015). We formulated two potential conclusions: (a) Other physiological mechanisms may be contributing to myocardial ischemia measured during exercise among younger firefighters or (b) the relationship is spurious. Hunter et al. (2017) reported multiple physiological mechanisms can produce myocardial ischemia during exercise among firefighters such as coronary vasospasm, thrombosis, and arterial stiffening. This would explain the inverse relationship between age and magnitude in this study; although, the firefighters in the present study harbored multiple IHD risk factors such as obesity and hypertension. It is most likely that a combination of pro-ischemic factors including IHD was responsible for myocardial ischemia among this sample but to confirm this, other approaches to measuring the extent and severity of ischemia such as imaging should be used (Desmet et al., 2004). The other conclusion for this finding may be the result is spurious and given our small and homogeneous sample which limits generalizability this is also plausible. Future research should use larger and more heterogeneous samples to confirm these exploratory findings.
Nearly half of this small sample had significant ischemia demonstrating the lack of appropriate IHD screening and use of primary and secondary prevention techniques among professional firefighters. Occupational Health Nurses play a vital role in screening firefighters for IHD, improving access to medical care, and educating firefighters on heart health. Nurses can use the information presented in this article to better inform primary and secondary prevention efforts based on career length (Banes, 2014; Wimberley, 2016). Given the very high rates of pathological ischemia, obesity, and hypertension among this small sample, there is a need for nurses to use effective non-pharmacological interventions to improve the IHD risk profiles of firefighters (Banes, 2014; Carey, Al-Zaiti, Dean, et al., 2011; Carey, Al-Zaiti, Liao, et al., 2011; Wimberley, 2016).
Applying Research to Occupational Health Practice:
Ischemic heart disease (IHD) is the leading underlying cause of death among professional firefighters. Non-occupational (i.e., age) and occupational (i.e., career length) risk factors of IHD have been identified, but can overlap. In this article, we assessed the relationships between age, career length, and IHD, based on ischemic severity, and provide evidence that career length has a stronger association with IHD than age.
For nurses caring for professional firefighters, consider age and career length as important cardiovascular risk factors when conducting an IHD screening. More informed screening focused on the unique risk factors of firefighters will be benefical. Furthermore, implementation of primary and secondary prevention techniques are urgently needed to combat IHD among professional firefighters and reduce firefighter mortality.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This was funded by a grant from the National Institute of Health/ National Institute of Nursing Research (R21 NR-011077, MGC).
Author Biographies
Dillon J. Dzikowicz, BS, RN, is a doctoral (PhD) student at the University of Rochester School of Nursing and practicing registered nurse at the University of Rochester Medical Center. His research interests include cardiovascular risk stratification based on 12-lead electrocardiography.
Mary G. Carey, PhD, RN, FAHA, FAAN, is associate professor at the University of Rochester School of Nursing. Her research focuses on improving the heart health of on-duty firefighters.