
Abstract
Objective
Smoking is a risk factor for coronary artery disease (CAD) and a known factor influencing the severity and pattern of CAD. We summarized evidence regarding the effect of smoking on the number of occluded coronary arteries and the severity and pattern of CAD.
Methods
We extracted data from observational studies reporting the pattern and severity of CAD in smokers. The quality of studies was assessed using the Strengthening the Reporting of Observational Studies in Epidemiology checklist, and results are reported in the Garrard table. The review process followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement.
Results
We screened 11 studies including 6037 samples. Six studies reported no relationship between smoking and the number of damaged arteries. One study reported that smoking was related to occlusion in the left anterior descending artery, but there was no relationship between smoking and the location of occlusion in the arteries. Smoking was related to CAD severity in five studies.
Conclusions
Smoking was found to be related to CAD severity and location of the damaged artery in the heart. However, there was no significant association of smoking with the number of damaged arteries and location of arterial occlusion.
Introduction
Owing to the increasing number of deaths from non-communicable diseases, especially in developing countries, the World Health Organization has declared non-communicable diseases among the health priorities for the next two decades. 1 Among these, cardiovascular disease is now recognized as the most important and leading cause of death in many countries, seen in 48% of the population in the United States (US). 2 The total annual cost of cardiovascular disease in the US is estimated at USD 180 billion, of which USD 170 billion is for direct costs and USD 10 billion is for indirect costs owing to the loss of production and labor capacity. 3 The overall percentage of deaths from cardiovascular disease during the 20th century rose from 10% to 30%. 4 The main cause of cardiovascular disease is reported to be coronary artery disease (CAD), 5 with 2 out of 10 deaths being associated with CAD, 2 and CAD-related deaths are expected to rise from 17.3 million in 2012 to 23.6 million in 2030.2,6 The prevalence of cardiovascular disease is rapidly increasing in developing countries. 7 The coronary arteries, which originate in the aorta and immediately above the aortic valve, are responsible for supplying blood to the heart muscle. 8 Several tests are used to diagnose cardiovascular disease. One of these is angiography, which is the gold standard method for diagnosing CAD. 9 CAD is mostly caused by smoking and physical inactivity, but high blood pressure, dyslipidemia, and some factors related to ethnicity also lead to CAD.10,11 Numerous studies have been performed on the prevalence of cardiovascular risk factors in different populations, but inconsistent results have been reported because CAD is a multifactorial disease with risk factors that include age, sex, family history, genetic factors, hypertension, diabetes mellitus, smoking, and high blood cholesterol.5,12–16 As a primary risk factor, smoking plays a major role in premature coronary atherosclerosis and in accelerating atherosclerosis by increasing the oxidation of low-density lipoprotein (LDL) and damaging coronary endothelial vasodilation. 17 In addition to causing CAD, premature and accelerated coronary atherosclerosis are determinants of the severity and extent of vascular occlusion. 18 Understanding the patient’s pattern and severity of vascular occlusion is important because these factors determine the choice of appropriate treatment and the success of treatment.19,20 Various studies have examined the effect of multiple risk factors, such as diabetes, hypertension, hyperlipidemia, sex, and smoking, on the pattern and severity of CAD.20–23 Of these risk factors, smoking is one of the most important, but related studies have yielded conflicting results.
Given the rapid increase in CAD and the widespread use of tobacco products, including cigarettes, understanding the importance of smoking and its effects on the pattern and severity of CAD is critical. Therefore, in this study, we aimed to aggregate the findings on this topic. Because no studies have reviewed the pattern of coronary artery occlusion and severity among cigarette smokers, understanding these factors will help physicians in choosing the appropriate treatment for their patients.
Methods
Protocol and search strategy
This study is registered in Kermanshah University of Medical Sciences. The aim of the study was to report the pattern and severity of CAD in patients who smoked cigarettes. We following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol in this study. 24 This protocol is considered a valid method to comprehensively review past studies, following the conceptual and structural framework of review studies. We performed a comprehensive search using international databases up to 20 March 2021. The searched databases included Web of Sciences, PubMed, Scopus, Cochrane Library, Elsevier, and Google Scholar. The search strategy included MeSH terms and keywords mentioned in published articles, as follows: “cardiovascular,” “coronary artery,” “coronary vessels,” “cigarettes,” and “smoking.” The reference lists of eligible titles were also screened to identify additional articles.
Inclusion criteria
Included papers were observational studies, such as retrospective or prospective cohort studies and descriptive or analytical studies. We excluded review articles, letters to the editor, and similar articles. The included studies must have reported the number of occluded coronary arteries and the pattern and/or severity of CAD in patients who smoked cigarettes.
In this study, the pattern of CAD was considered to be the site of the occluded artery in the heart and the site of occlusion in the affected artery. Additionally, the type of occlusion was stenosis or plaque in the artery.
Search validation and study selection
All related articles found using our search terms, as well as those in the reference lists of eligible studies, were reviewed. First, all results were entered into Endnote software. The titles of studies were independently reviewed by three authors (MJ, NS, and PJ) to select potential studies for inclusion. The abstract and full text of the selected articles were then screened independently by these authors. Finally, articles that met the inclusion criteria were carefully screened and the data were extracted for the number of affected arteries and the pattern and severity of CAD. Any conflicts among the authors during screening were resolved through discussion. This process was guided by the PRISMA statement. 24 Data were extracted using a standard form and the Garrard table.
Quality assessment
The quality of studies is one of the most important criteria for assessing the results of published reports. To assess study quality, we used the 22-item Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist. 25 Each item is scored from 0 to 2, with minimum and maximum scores between 0 and 44. A score of 0 to 15.9 indicates poor quality, a score of 16 to 29.9 medium quality, and a score of 30 to 44 indicates high quality of the study.26,27
Data extraction and reporting
Data from all eligible studies were screened and extracted by the research team. The data are reported in a Garrard table. The Garrard table was designed by Judith Garrard as a way to report the results of review studies and meta-analyses. 28 Reported data included characteristics such as study design, patients, year and location of the study, and study quality. The associations of smoking with the number of coronary arteries and the pattern and severity of CAD were also reported. Additionally, we discuss the gold standard for diagnosing coronary artery occlusion.
Results
Selected studies
In the initial search, 139 studies were identified. After removing duplicate articles, 128 studies remained. In the evaluation of titles, 98 studies were considered for further screening; after reviewing the abstracts and full text of these articles, 38 studies were retained for data screening.
Finally, we included 11 studies with sufficient data on the number of arteries and pattern and severity of coronary artery occlusion among smokers (Figure 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram of study selection.
Characteristics of studies
The 11 included studies were conducted between 2006 and 2018. All articles had a retrospective descriptive-analytical design. Seven studies were conducted in Iran and the rest were carried out in Italy, China, Japan, and the Netherlands. In all articles, 6037 samples were included, with a minimum and maximum of 80 autopsy samples and 2390 patients, respectively (Table 1).19,20,22,23,29–35
Characteristics of 11 included studies.
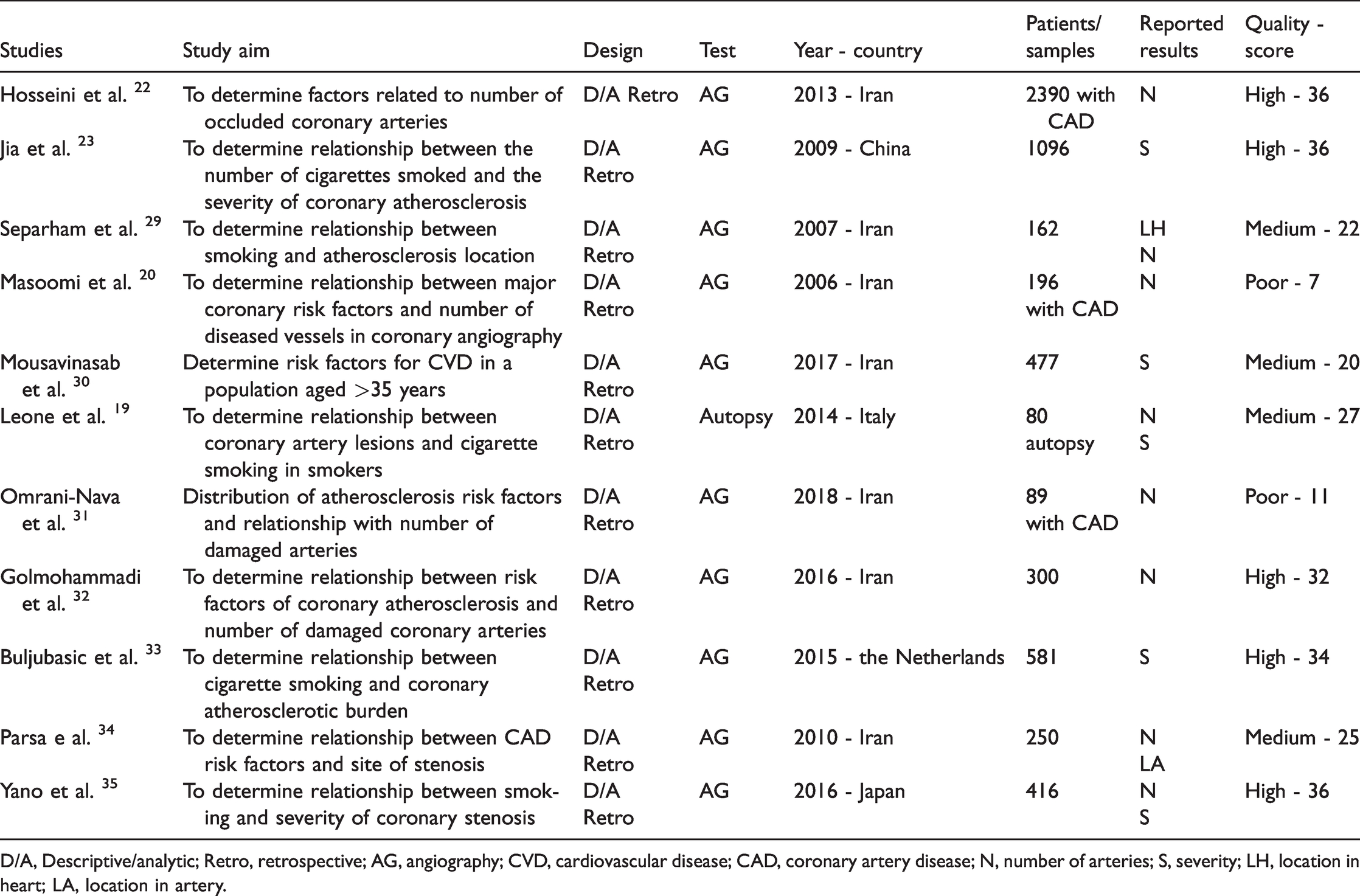
D/A, Descriptive/analytic; Retro, retrospective; AG, angiography; CVD, cardiovascular disease; CAD, coronary artery disease; N, number of arteries; S, severity; LH, location in heart; LA, location in artery.
In the 11 included articles, results were reported related to the number of arteries as well as the pattern and severity of CAD. The distribution of studies in terms of number of diseased coronary arteries, severity of coronary artery occlusion, or location of the occluded coronary artery in the heart or the location of occlusion in the coronary artery are as follows: eight results related to the number of coronary arteries, one result related to the location of the coronary artery in the heart, one result related to the location of occlusion in a coronary artery, and five results related to the severity of coronary artery occlusion (Table 1).
In the assessment of the study quality, five studies were high quality, four studies were medium quality, and two studies were poor quality (Table 1).
Confirmation test
In 10 studies, patients underwent angiography; autopsy was used in only 1 study (Table 1). Therefore, angiography was the predominant method used to detect coronary artery occlusion. The study of CAD and its mortality dates back to the 18th century, but explanation of the pathogenic processes associated with CAD was published in the middle of the 19th century. 36 Angiography is the gold standard method used to examine patients with CAD and its use is expanding with new technologies.37,38 Angiography was first invented in 1929 by Forssman and further developed in 1956 by Cournard and Richard as a diagnostic method. Sones first used selective coronary angiography in 1963. Coronary angiography refers to radiographic observation of the coronary arteries after contrast injection. In addition to coronary angiography, a complete invasive examination of the patient's cardiovascular condition involves examination of the cardiac cavities and hemodynamic evaluation. 39
Number of occluded coronary arteries
In eight included studies, the relationship between smoking and the number of occluded coronary arteries in patients with CAD was investigated. The results in six studies showed no relationship between smoking and the number of damaged coronary arteries. Two studies reported a relationship between smoking and the number of damaged coronary arteries (Table 2); these studies showed that with increased number of cigarettes smoked, the number of occluded coronary arteries was increased.
Effect of smoking on number of disease arteries, pattern, and severity of CAD.
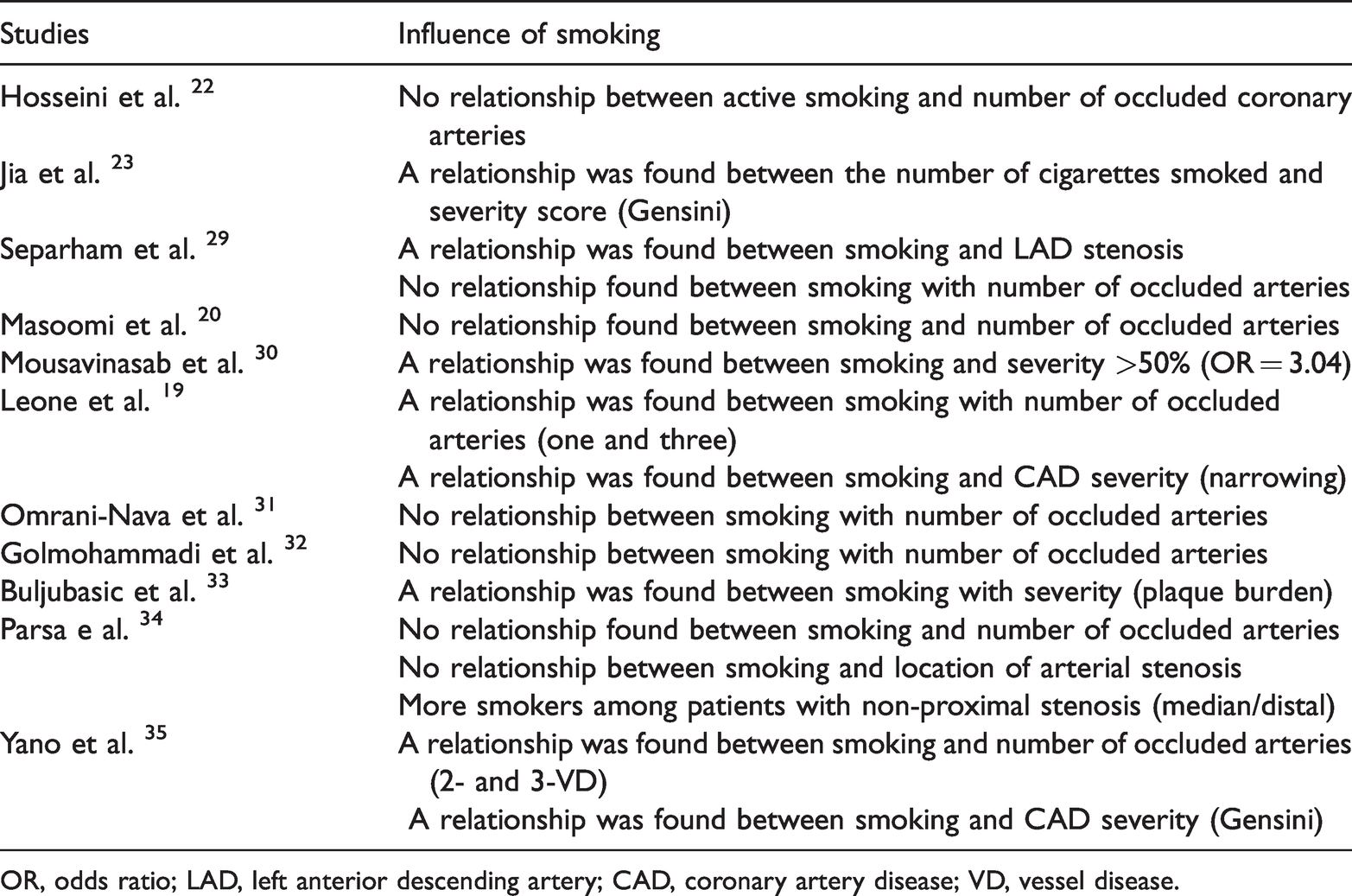
OR, odds ratio; LAD, left anterior descending artery; CAD, coronary artery disease; VD, vessel disease.
Location of occluded arteries in the heart
Only one study reported a relationship between smoking and occlusion of the left anterior descending (LAD) artery among patients with CAD (Table 2).
Location of arterial occlusion
One study assessed the relationship between smoking and the location of occlusion in the coronary arteries. The study found no relationship between smoking and the location of occlusion in coronary arteries, but the number of smokers was higher among patients with non-proximal CAD (Table 2).
Severity of coronary artery occlusion
The relationship between smoking and the severity of CAD was investigated in five studies. The results of these studies showed a relationship between smoking and the severity of congestion. With increased number of cigarettes smoked, the severity of CAD was increased. Importantly, this relationship was measured using different measurement criteria of severity. In two studies, the Gensini tool was used and narrowing of the arteries was considered in one study; in another study, plaque burden was measured (Table 2).
Discussion
In many countries, CAD is a main cause of disability, high health care costs, and death. Investigation of the causes and factors affecting the development of CAD dates back to 1948 in the US. 40 In 1960, results of the Framingham Heart Study proved that smoking increases the risk of heart disease. 41 Since then, smoking has been considered a major risk factor for CAD.
The effect of smoking on the incidence of coronary artery insufficiency has been studied by various researchers. The aim of the present study was to investigate this effect in terms of the number of occluded coronary arteries and the pattern and severity of coronary artery occlusion in patients with CAD. The results of such studies are often contradictory, perhaps owing to the multifactorial nature of CAD.
The findings of the present study showed that smoking was not significantly associated with the number of damaged coronary arteries in patients with CAD; however, this finding was reported in only two studies. Perhaps one reason for this is an insufficiently long study period.42,43 Smoking duration, smoking dose, and duration of illness can lead to an increase in the number of occluded coronary arteries.
The results of our review clarified the evidence that smoking is associated with the severity of CAD. Our study results also showed that smoking was associated with occlusion of the LAD artery and that smokers may be more likely to have non-proximal coronary artery occlusion. The reason for this association may be owing to the effect of cigarettes and nicotine on the vascular epithelium; under the influence of nicotine, the coronary vascular epithelium can become damaged. 44 Smoking also increases sympathetic tone and causes vasospasm. 29 Myocardial necrosis can be caused by the effects of nicotine. 45 In general, two types of necrosis are caused by smoking and nicotine, ischemic necrosis and toxic necrosis, in which the myocardium is affected by the chemicals in cigarettes.19,46 Additionally, calcium deposition as atheroma is another known effect of nicotine. 46 A further mechanism of smoking is its effect on increasing serum LDL and triglycerides in the blood as well as decreasing the amount of high-density lipoprotein. Smoking also causes vascular inflammation and the production of C-reactive protein. 47 Jia et al. stated that smoking causes the onset and progression of atherosclerosis by inhibiting vasodilation and increasing vasoconstriction, stabilizing thrombosis, causing inflammation, and modifying lipid profiles. 23
Other evidence of the influence of smoking on CAD is the effect of smoking cessation on improving patients’ cardiovascular condition. One study found that smoking cessation in patients with CAD reduced the risk of myocardial infarction by up to 20% over the following year. 48 Another study found that smoking cessation reduced the number and extent of changes in the coronary arteries. 49
Smoking should be considered a risk factor associated with the severity of CAD. Additionally, smoking may be associated with the number of occluded coronary arteries and the location of CAD.
Implications and limitations
As mentioned, the results of this study can be used in identifying CAD and in choosing the appropriate treatment and care for patients with CAD. However, further studies are needed to confirm our results.
This study has some limitations. Although we conducted an extensive search of the published literature, a number of articles were excluded owing to a lack of sufficient data or inadequate study methods. Moreover, the quality of the included studies was not high in all cases.
Conclusion
In six of the studies included in this review, smoking was not related to the number of occluded coronary arteries; this relationship was observed in only two studies. A relationship between smoking and the severity of CAD was reported in five studies, as well as between smoking and occlusion of the LAD artery. However, no significant relationship was found between smoking and the location of occlusion in the coronary arteries. Smoking cessation can help to improve the health of patients with CAD.
Further high-quality studies are needed on the relationship of smoking with the number of occluded coronary arteries, the location of occluded coronary arteries in the heart, and the location of occlusion in coronary arteries among patients with CAD. Similar studies for other risk factors of CAD are warranted. Community-based programs to help prevent smoking are needed, to reduce the risk of CAD development in the population.
Footnotes
Acknowledgements
We thank Kermanshah University of Medical Sciences for their assistance in this study.
Author contributions
MJ and NS contributed to the concept of the study. MJ, NS, and PJ performed the comprehensive search and data extraction. The final report and manuscript was written, edited, and approved by all of the authors.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
This study was approved by the ethics committee of Kermanshah University of Medical Sciences (registry number 300116). This study was conducted in compliance with the Declaration of Helsinki. This was a review study; therefore, there was no requirement for patient consent.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.