
Abstract
Objective
The effect of alcohol consumption on the risk of coronary heart disease is controversial. Several studies have assessed the effects of alcohol on the formation of atherosclerotic plaques, but few studies have evaluated the chronic effects of alcohol consumption on the coronary artery diameter. We investigated whether alcohol consumption affects the coronary artery diameter.
Methods
This prospective study enrolled men who were undergoing coronary angiography at the First Affiliated Hospital of Chongqing Medical University from November 2016 to December 2017. The participants were categorized into three groups based on their drinking behavior: heavy drinking (>175 g/week in the last 2 years, n = 70), moderate drinking (>42 to ≤175 g/week in the last 2 years, n = 53), and nondrinking (lifetime alcohol consumption of <98 g, n = 79). The diameters of the left and right coronary arteries were compared among the three groups.
Results
No significant differences in the diameters of the left and right coronary arteries were observed among the three groups.
Conclusions
Alcohol consumption may not affect the diameter of the coronary arteries.
Keywords
Introduction
Alcohol consumption (AC) is associated with negative health consequences and an increased incidence of diseases such as cancer and liver cirrhosis. However, the relationship between AC and coronary heart disease (CHD) is unclear. Some studies have suggested that moderate AC may reduce the incidence of CHD, while excessive AC is associated with an increased incidence of CHD. This effect, known as the “U/J curve,” is controversial.1,2
The mechanism of action underlying the cardioprotective effect of AC is not clear. Studies have shown that alcohol exerts protective effects against risk factors for atherosclerosis, such as hypertension, a high body mass index (BMI), and an increased level of high-density lipoprotein cholesterol (HDL-c); improves endothelial function; increases insulin sensitivity; and reduces fasting insulin resistance.3,4
Many studies have focused on the formation of atherosclerotic plaques, but few studies have focused on changes in artery diameter. An increased coronary artery diameter may be associated with a reduced severity of CHD. 5 Furthermore, a larger initial coronary artery diameter is associated with a reduced risk of ischemia. The coronary artery diameter varies under different conditions. For example, the diameter of the vascular lumen has been shown to increase significantly 1 year after revascularization of chronic totally occluded coronary lesions, suggesting that the diameter of the vascular lumen can be increased. 6 Studies have also shown that coronary atherosclerosis can enlarge the lumen as a compensatory protective mechanism. 7 Alcohol has been shown to induce acute vasodilation of the splanchnic arteries, resulting in acute widening of blood vessels. 8 Fried et al. 9 performed a study involving 31 Caucasian men and found that the diameters of the left main coronary artery and left anterior descending artery were larger in men with moderate AC than in nondrinkers. Furthermore, long-term AC can increase the diameters of the aorta and the common carotid artery.10,11 Some Chinese physicians have observed and postulated that people with chronic, heavy AC have larger coronary arteries, but conclusive evidence is lacking. 12 We tested the hypothesis that chronic AC is associated with an increased coronary artery diameter.
Methods
This prospective study protocol was approved by the ethics committee of the First Affiliated Hospital of Chongqing Medical University (2016-166; Chongqing, China). All participants provided written informed consent.
Typically, men have larger coronary arteries than women, 13 and women seldom drink alcohol in China; 14 therefore, we enrolled only men in this study. At least 50 samples were required to achieve >80% power for the comparison between two groups for the right coronary artery ostium calibrated by body surface area (2.4 vs. 2.2 mm, standard deviation = 0.4, α = 0.05). We enrolled 123 consecutive men with known AC. They underwent coronary angiography at our hospital from November 2016 to December 2017. Additionally, 79 age-matched participants with no AC were simultaneously enrolled.
All participants underwent coronary artery angiography for investigation of typical or atypical chest pain. Coronary angiography was performed using the standard Judkins method through the radial artery or femoral artery.
The following questions were asked to determine each patient’s level of AC: (1) How much alcohol do you consume each week? (2) How often do you drink alcohol each week? (3) How long have you been drinking alcohol? (4) Have you quit drinking, and if so, when?
The most commonly consumed alcoholic beverages in China are beer, wine, and strong liquor. The participants were categorized into three groups according to the amount and frequency of AC: heavy drinking (AC of >175 g/week during the last 2 years), moderate drinking (AC of >42 to ≤175 g/week during the last 2 years), or nondrinking (lifetime AC of <98 g among nondrinking patients age-matched to patients in the AC groups). This study did not include a light drinking group because no participants had not stopped drinking <1 month prior to the study starting date and had drunk >0 to <42 g/week during the last 2 years.15,16
Patients with Kawasaki disease, systemic arteritis, lesions of the coronary artery ostium, or an anomalous origin of the coronary arteries were excluded. We also excluded individuals who had quit drinking alcohol >1 month prior to initiation of the study because changes in the coronary artery diameter may appear relatively early. Allahwala et al. 6 found that the size of the coronary artery increased shortly after revascularization of chronic total occlusion.
The patients’ baseline data included age, height, body weight, body surface area, low-density lipoprotein cholesterol (LDL-c) level, HDL-c level, smoking status, and history of hypertension, diabetes mellitus (DM), or hyperlipidemia. A smoker was defined as a former and current smoker. Hypertension was defined as a systolic blood pressure of ≥140 mmHg and/or diastolic pressure of ≥90 mmHg. DM was defined as a non-fasting plasma glucose level of ≥200 mg/dL or a fasting plasma glucose level of ≥140 mg/dL. Hyperlipidemia was defined as a total serum cholesterol concentration of ≥220 mg/dL. Reported or recorded medical treatments for hypertension, DM, or hyperlipidemia were also used to define these disease conditions.
After implantation of an artery sheath, all participants received routine injections of nitroglycerin (300 μg). The coronary artery diameters of the 202 participants were measured by two interventional cardiologists blinded to the clinical data and patient groups. Angiograms were analyzed using a digital acquisition system (GE Medical, Chicago, IL, USA). Measurements were taken during diastole, and the widest diameter was recorded. A catheter tip with a known diameter (1.67 mm for a 5.0-French catheter) was used for calibration to determine the diameters of the coronary arteries, with the settings of the image intensifier kept constant. The coronary artery ostium was trumpet-shaped; therefore, the minimum diameter of the trumpet-shaped region was measured as the diameter of the coronary artery. The diameters of the left and right coronary arteries were used to determine the representative diameters of the whole vessel because they are the widest part of the coronary artery. The diameter of the left main coronary artery was evaluated in the caudal 30°, right anterior oblique 30° projection. The diameter of the right coronary artery was evaluated in the 45° left anterior oblique projection. The branches of the coronary arteries were highly variable in size and anatomical distribution; therefore, their diameters were not measured.
Statistical analyses
Statistical analyses were carried out using SPSS, version 18.0 (IBM Corp., Armonk, NY, USA). Age, height, weight, BMI, body surface area, and HDL-c level were treated as continuous variables. Hypertension, DM, hyperlipidemia, and smoking status were treated as categorical variables. All continuous variables are expressed as mean ±standard deviation. The coronary artery diameters are presented as boxplots for the three groups. Differences among the groups were compared using one-way analysis of variance. We defined nondrinking as the reference category and compared the other two groups with the nondrinking group using Student’s t-test. Differences between categorical variables were compared using Pearson’s chi-squared test. Fewer participants smoked cigarettes in the nondrinking group, and research has shown that smoking may have an impact on coronary artery atherosclerosis. 17 Therefore, we used a covariate analysis to adjust for any interaction between smoking and AC. However, the conditions for the covariate analysis were not met during the data analysis. We also compared the different drinking groups within groups of participants who smoked and compared the different drinking groups within groups of participants who did not smoke using one-way analysis of variance. A P value of <0.05 was considered statistically significant.
Results
The boxplots presented in Figure 1 show that the artery diameters were similar among the three groups. The mean age of the patients in each group was 60 years. There were no significant differences in the potentially confounding variables of age, height, weight, BMI, hypertension, DM, hypercholesterolemia, or HDL-c level. The heavy drinking group had significantly higher LDL-c levels than the nondrinking and moderate drinking groups (2.31 ± 0.79, 2.60 ± 0.90, and 2.67 ± 0.97 mmol/L, respectively; P = 0.047). Significantly fewer participants smoked in the nondrinking group (68.35%) than in the moderate drinking group (88.68%) and heavy drinking group (92.86%) (P < 0.05). The smoking status may have confounded the results, but the conditions for the covariate analysis were not met (Table 1). Therefore, we evaluated smoking and nonsmoking participants separately. The proximal portion is typically the largest part of a coronary artery, and the diameters of the branch arteries are variable. Therefore, we chose the diameter of the proximal portion to represent the whole artery. No significant differences in the diameter of the left and right coronary arteries were observed among the groups. The mean diameter of the left coronary artery was approximately 4.6 mm (2.7 mm after normalization to body surface area), and that of the right coronary artery was approximately 4.0 mm (2.3 mm after normalization to body surface area). There was no significant difference in the mean diameter between the nonsmoking and smoking groups (Tables 2 and 3).
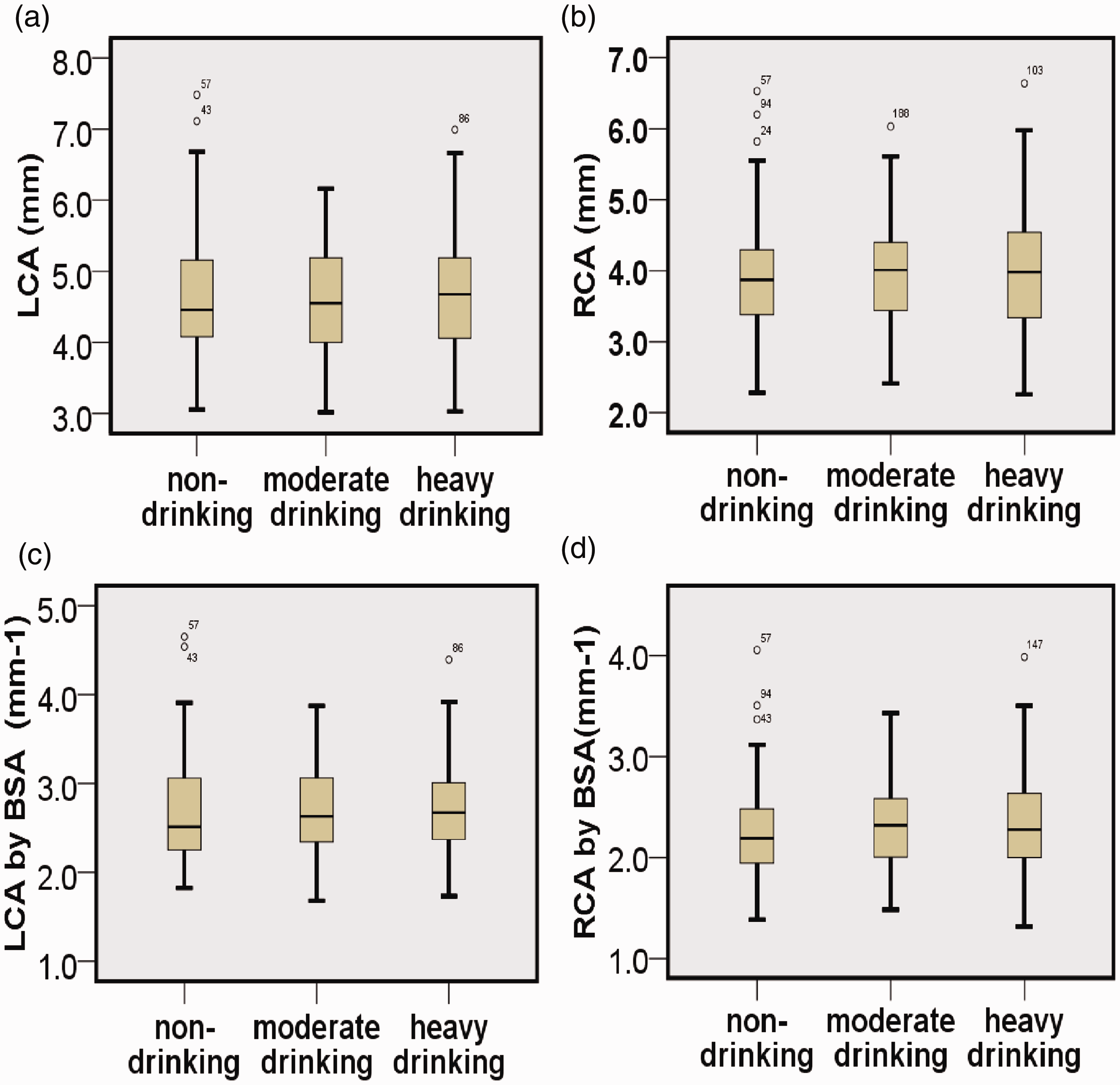
The boxplots show that the coronary artery distributions were similar among the three groups. (a) LCA. (b) RCA. (c) LCA normalized to BSA. (d) RCA normalized to BSA. LCA, left coronary artery; RCA, right coronary artery; BSA, body surface area.
Patients’ baseline data.

Data are presented as mean ± standard deviation or n (%).
BMI, body mass index; LDL-c, low-density lipoprotein cholesterol; HDL-c, high-density lipoprotein cholesterol; LCA, left coronary artery; RCA, right coronary artery; BSA, body surface area.
Comparison of coronary artery diameter in smokers among different drinking groups.

Data are presented as mean ± standard deviation.
LCA, left coronary artery; RCA, right coronary artery; BSA, body surface area.
Comparison of coronary artery diameter in nonsmokers among different drinking groups.

Data are presented as mean ± standard deviation.
LCA, left coronary artery; RCA, right coronary artery; BSA, body surface area.
Discussion
In the present study, the diameter of the coronary artery (both before and after normalization to body surface area) did not differ among heavy drinkers, moderate drinkers, and nondrinkers. In addition, no differences were observed among the three groups irrespective of smoking status. These results suggest that AC may not be associated with the diameter of the coronary arteries.
We showed that AC may have no long-term effects on the diameter of the coronary arteries. Other studies have shown that AC causes acute vasodilation. AC can induce the release of calcitonin gene-related peptide, 18 which results in vasodilation of the coronary arteries and increased coronary blood flow. However, these acute reactions may not become long-term effects. Furthermore, AC may cause coronary artery constriction. Rogers and Bove 19 showed that moderate doses of alcohol can induce significant vasoconstriction in epicardial coronary arteries. This may occur because alcohol can make vessels sensitive to local or circulating contractile agents. Alcohol has even been found to induce coronary artery spasm. 20 These opposing effects on vascular tone may cancel each other out, resulting in no change in the coronary artery diameter.
The diameter of the coronary arteries is strongly correlated with the risk of CHD. Zhou et al. 5 evaluated the potential relationship between the coronary artery diameter and the severity of coronary artery disease. Their study involved 167 participants, including 124 patients with CHD. They compared the coronary artery diameters of the participants and found a negative correlation between the coronary artery diameter and the severity of coronary artery disease (as assessed by the Gensini score). 5 Hiteshi et al. 13 found that women usually have smaller luminal diameters and therefore exhibit larger changes in the luminal area than do men with the same degree of atherosclerosis, resulting in worse prognoses for women than for men.
We used quantitative coronary angiography (QCA) to measure the coronary artery diameter. QCA is widely used in clinical practice and has good repeatability. It provides effective guidance for percutaneous coronary intervention. QCA can also be used to reliably measure the size of the coronary arteries. However, most studies have evaluated autopsy specimens, and various factors associated with the acquisition, preservation, fixation, and analysis of the epicardial coronary artery have resulted in unreliable measurements and conclusions. 21 QCA is not subject to these factors and thus provides a good representation of the size of the coronary arteries.
Our results are inconsistent with those of a study by Fried et al., 9 who found that moderate AC increased luminal diameters. This difference might be attributable to two factors. First, the number of participants in their study was small: 31 patients, among whom only 11 were moderate drinkers, were assessed. Second, in our study, 300 μg of nitroglycerin was injected into the artery sheath of each participant before angiography. The coronary artery diameter is highly variable within an individual because blood vessels may spasm, resulting in a reduced diameter. Patients undergoing coronary angiography usually exhibit artery spasm because of pain and anxiety. Interventionists prefer to standardize the coronary tone by induction of maximal dilatation. Nitroglycerin is used to induce coronary artery dilatation, which may eliminate the bias caused by vasoconstriction.22,23 However, neither nitroglycerin nor other vasodilators were used in the study by Fried et al. 9 The differences in diameter may have resulted from the different tone of the coronary arteries.
Our study had several limitations. First, the sample size was small. Second, it was a cross-sectional observational study. Third, estimation of the amount of drinking was dependent upon patients’ self-reports, and we excluded former drinkers; this may have biased the data. Fourth, the male participants were of Chinese Han ethnicity and had angina pectoris, which limits the generalizability of our study. Finally, coronary angiography was used to determine the diameter of the lumen. The cross section of the coronary artery lumen is often irregular, which may have resulted in measurement errors.
Conclusion
We found no significant correlation between AC and the coronary artery diameter.
Footnotes
Acknowledgement
We thank Dr. Liu Jun-Hao for providing help with the statistical analysis.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Ethical approval/patient consent
The study protocol was approved by the ethics committee of the First Affiliated Hospital of Chongqing Medical University (2016-166; Chongqing, China). All participants provided written informed consent.
Funding
This work was supported by the Chongqing Science and Technology Bureau (No. cstc2019jscx-msxmX0307) and the National Natural Science Foundation of China (No. 81270210 and 81541098).
Supplemental material
Supplemental material for this article is available online.