
Abstract
Introduction:
Coronary artery disease (CAD) is the leading cause of mortality in Malaysia. Psychological risk factors are associated with detrimental outcomes in CAD. Our study aimed to evaluate procedural anxiety and depression levels among subjects who underwent coronary angioplasty.
Methods:
A single-centre prospective cohort study was conducted on patients electively admitted to a tertiary hospital in Malaysia for percutaneous coronary intervention (PCI) over a half-year period. The Hospital Anxiety and Depression Scale (HADS) and the EuroQol-5 Dimension (EQ5D) Health Questionnaire were used to evaluate subjects’ psychological statuses. The EQ Visual Analogue Scale was used for the global assessment of their health.
Results:
The analysis included 65 patients with a mean age of 63 years from a predominately educated population (n=54; 83.1%). Before the PCI procedure, female sex was found to be protective against depression, with an odds ratio (ORs) of 0.29 (95% confidence interval (CI) 0.08–1.03). A high level of education was protective against anxiety (OR=0.21; 95% CI 0.06–0.83). After the PCI, females were more likely to be depressed (OR=3.89; 95% CI 1.13–13.37), and those of Malay ethnicity were more likely to be anxious (OR=4.2; 95% CI 1.03–17.07). Using the HADS, subjects were significantly less anxious and depressed (pre-PCI: median (IQR) score=4 (7.0)); post-PCI: median (IQR) score=3 (5.0), p=0.02), measured by the HADS. Using the EQ5D, subjects had an improved mean VAS score (post-PCI: 75±14.9; pre-PCI: 68±12.6; p<0.05).
Conclusions:
PCI may predispose patients with CAD to psychological stressors. Female patients and those of Malay ethnicity are more likely to experience psychological stress. Being highly educated is protective against such stress.
Keywords
Introduction
Cardiovascular diseases, which include coronary artery disease (CAD), have been the leading cause of morbidity and mortality in Malaysia and globally.1,2 Conventional risk factors for CAD include hypertension, diabetes mellitus, dyslipidaemia, cigarette smoking and a family history of CAD. Although the majority (85.6%) of patients with CAD present with at least one conventional risk factor, a sizeable population (14.4%) do not present with any of the five risk factors. 3 Other risk factors include obesity, sedentary lifestyle, psychological illness and elevated serum high-sensitivity C-reactive protein and coronary artery calcium score. Establishing these risk factors would provide highly comprehensive clinical risk strata and therefore enable better management of these patients. 4
The emergence of depression, anxiety and chronic psychosocial stress is associated with a determinantal outcome towards CAD, which is often overlooked by clinicians.5,6 The disease progression is believed to be mediated by heart rate variability, endothelial inflammation and impaired myocardial perfusion linked to mental stress, such as depression and anxiety.7,8 A paucity of knowledge exists regarding the level of anxiety and depression of patients undergoing coronary angiogram (CAG) and percutaneous coronary intervention (PCI). Little is known about which baseline characteristics in Malaysian patients are associated with mental stresses before and after a procedure.
The objective of this study is to evaluate the procedural anxiety level among subjects who underwent CAG or PCI. We aimed to elucidate the clinical characteristics that could be attributed to high anxiety levels, which may in turn be associated with poor clinical outcomes in patients with CAD.
Methods
Subjects
The study was a prospective single-centre cohort study conducted at the Cardiology Unit, University of Malaya Medical Centre, between June 2020 and December 2020. All the patients aged ⩾18 years who underwent CAG or PCI were recruited into the study. We defined ‘elective’ PCI as all PCI procedures that were not to be delivered urgently within 24 hours of myocardial infarction, excluding patients with ST-elevation myocardial infraction (STEMI), where PCI treatment should be delivered in a timely fashion. Elective PCI cases were further classified into two main groups: (a) elective outpatient (clinic) admissions, where the decision to admit made in clinic visits precedes the time of actual admission to hospital; and (b) elective inpatients/ad hoc PCI cases, where the decision for PCI was made after the actual admission and schedule for PCI as inpatients after 24 hours. A total of 100 elective cases for CAG or PCI who consented to participate in the study by written consent were subsequently enrolled. Exclusion criteria included a history of at least one of the following: any psychological disorder, valvular heart diseases, heart failure, stroke or cognitive impairment. The patients were interviewed the day before the elective angiogram and the day after the angiogram for psychological tests. Demographics, clinical data on cardiac evaluation and laboratory investigation were documented at the initial interview. The details of the CAG findings and intervention done were recorded on the day of PCI.
Assessment of anxiety and depression
Hospital Anxiety and Depression Scale
The Hospital Anxiety and Depression Scale (HADS) is a 14-item self-reported questionnaire developed as a screening tool in the assessment of anxiety and a depressive state in non-psychiatric departments. The HADS comprises four-point Likert-scale items evaluating the presence of anxiety (HADS-A) and depression (HADS-D) over the past two weeks. 9 Items in the HADS-A and HADS-D are summed up to a total score of 21 each. HADS-A has an optimal cut-off of ⩾8 (sensitivity 0.89; specificity 0.75), and HADS-D has an optimal cut-off of ⩾8 (sensitivity 0.80; specificity 0.88). Both scales correlate to generalised anxiety disorder and major depressive episodes. The HADS Malay version has been validated and utilised for good understanding by the Malaysian population. 10
EuroQol-5 Dimension Health Questionnaire
The EuroQol-5 Dimension Health Questionnaire (EQ5D) is a widely used generic quality-of-life scale to measure health outcomes and has two parts. The EQ-5D-5L self-classifier comprises five questions involving mobility, self-care, pain, usual activities and psychological status. Patients are required to describe their health in the level of problems classified as ‘no’, ‘some’ or ‘extreme’ for each of the five categories. The EQ Visual Analogue Scale (EQ VAS) is a vertical analogue scale with values between 0 (the worst imaginable health) to 100 (the best imaginable health); it is focused on providing a global assessment of patient health. 11
Following the psychological test, the patients underwent elective CAG or PCI, as planned. The HADS and EQ5D questionnaires are provided in the Supplemental Material.
Analytical methods
Statistical analysis was performed using IBM SPSS Statistics for Windows v24 (IBM Corp., Armonk, NY). Normality was tested using a Shapiro–Wilk test. Qualitative and quantitative demographic data are presented in tabulated and graphical format. From the results, sensitivity and specificity study were calculated. Discrete variables were analysed using a chi-square test, and normally distributed continuous variables were analysed with an independent t-test. Data that were not normally distributed were analysed using a Mann–Whitney U-test. For the correlation test, either Spearman or Pearson correlation tests were performed, depending on the data collected.
Results
General characteristics
All patients who consented (n=100) and who were electively admitted for CAG or PCI were initially recruited. Sixty-five subjects were subsequently enrolled and analysed, whereas 35 patients were excluded due to the presence of at least one of the exclusion criteria upon further history taking and reassessment in the ward. The participants had a mean age of 63±10.7 years and were predominately male (male-to-female ratio 1:0.3). The majority of the sampled population were of Malay ethnicity (n=36; 55.4%), married (n=54; 83.4%) and had secondary or tertiary education (n=54; 83.1%). Just under half (n=10; 45.5%) had a middle-class income, which is defined as monthly income of more than 4000 Malaysian Ringgit. The study population had at least one of the following conventional cardiovascular risk factors: dyslipidaemia (n=59; 90.8%), followed by hypertension (n=50; 76.9%), active or ex-smoker (n=44; 67.3%) and diabetes mellitus (n=30; 46.2%). Details on the demographic breakdown are shown in Supplemental Table S1.
Determination of factors associated with symptoms of anxiety and depression before and after PCI
A univariate analysis of risk factors was conducted to evaluate the correlation of anxiety and depression with the following baseline characteristics as independent variables: age, sex, race, education, smoking, diabetes mellitus, dyslipidaemia and hypertension. The analysis indicated that females were less likely to be depressed before the procedure (p=0.047, odds ratio (OR)=0.29, 95% confidence interval (CI) 0.08–1.03) compared to males. As shown in Table 1, subjects with hypertension were less likely to be depressed than those without hypertension (p=0.047, OR=0.29, 95% CI 0.08–1.03). The type of PCI was significantly associated with depressive symptoms before the procedure. Elective PCI cases were significantly associated with more depressive symptoms (n=9; 40.9%; p=0.046) compared to ad hoc PCI cases (n=2; 9.5%). Furthermore, a higher level of education, which was defined as secondary school and above, was identified as a protective factor against preoperative anxiety (p=0.03, OR=0.21, 95% CI 0.06–0.83). However, the level of education did not confer any significance for preoperative depressive symptoms (Table 2).
Association between patient background and abnormal depressive symptoms before PCI.
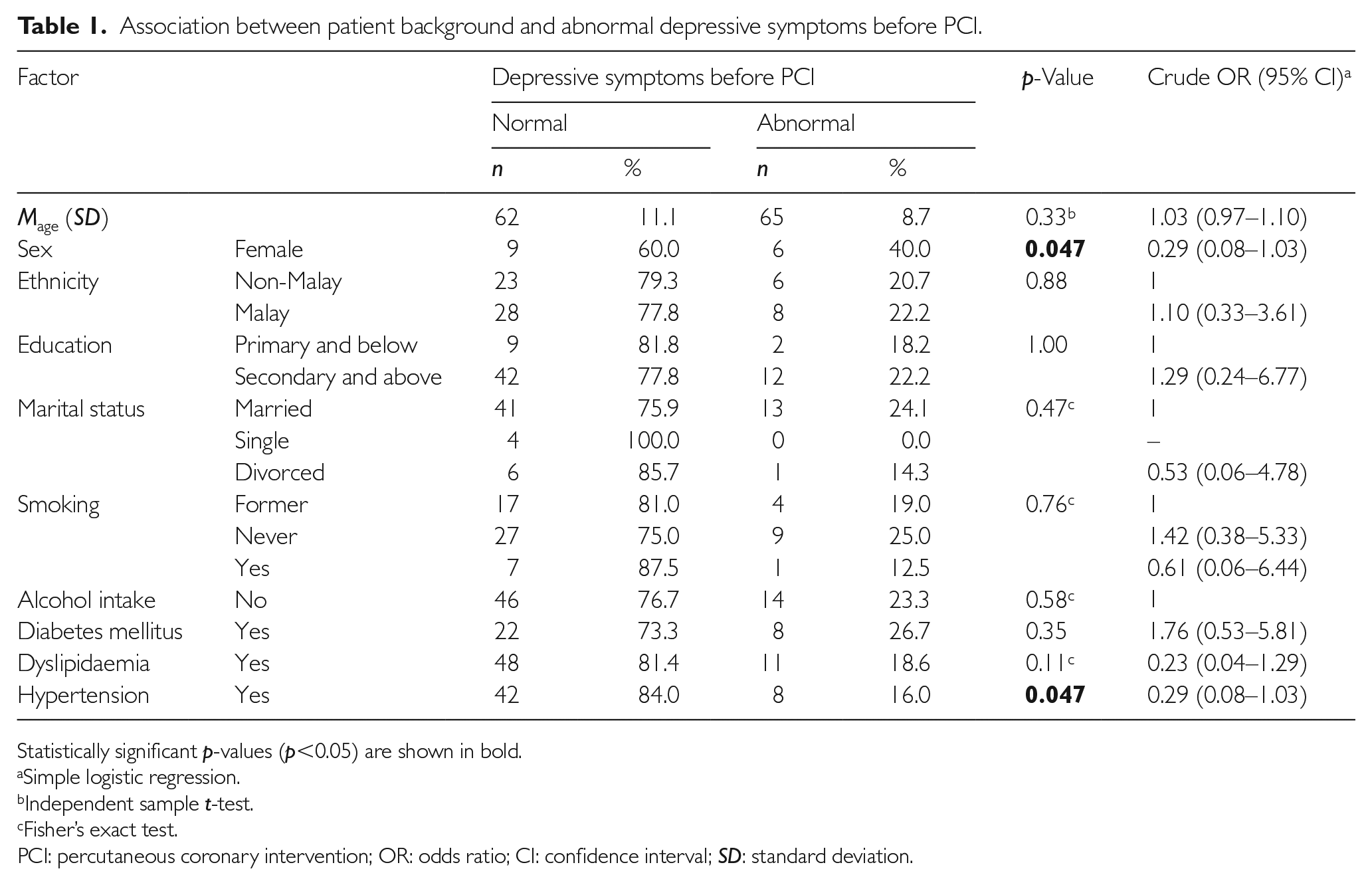
Statistically significant p-values (p<0.05) are shown in bold.
Simple logistic regression.
Independent sample t-test.
Fisher’s exact test.
PCI: percutaneous coronary intervention; OR: odds ratio; CI: confidence interval; SD: standard deviation.
Association between patient background and abnormal anxiety symptoms before PCI.

Statistically significant p-values (p<0.05) are shown in bold.
Simple logistic regression.
Independent samples t-test.
Fisher’s exact test.
As shown in Table 3, females were three times more likely to develop depression following the PCI than males were (p=0.03, OR=3.89, 95% CI 1.13–13.37). Patients of Malay ethnicity were four times more likely to be anxious after the procedure compared to other races in Malaysia (p=0.04, OR=4.2, 95% CI 1.03–17.07). The other factors were found not to be significantly associated with depressive or anxiety symptoms after PCI (Table 4).
Association between patient background and abnormal depressive symptoms following PCI.

Statistically significant p-values (p<0.05) are shown in bold.
Simple logistic regression.
Independent samples t-test.
Fisher’s exact test.
Association between patient background and abnormal anxiety symptoms after PCI.

Statistically significant p-values (p<0.05) are shown in bold.
Simple logistic regression.
Independent samples t-test.
Fisher’s exact test.
HADS score over time
Subjects were found to be clinically less anxious and depressive following PCI compared to before PCI, as evidenced by a statistically significant reduction of scores on median depressive and anxiety symptoms (Wilcoxon signed rank test). Seventeen (26.1%) patients were clinically anxious before PCI, and only 14 (21.5%) patients were clinically anxious following PCI. HADS scores showed a statistically significant decline in anxiety level (pre-PCI: median (IQR) score=4 (7.0); post-PCI: median (IQR) score=3 (5.0); p=0.02).
Furthermore, more subjects (n=18; 27%) had depression after PCI compared to before PCI (n=14; 21.5%). However, HADS median scores showed a significant decline in depression level (pre-PCI: median (IQR) score=5 (4.5); post-PCI: median (IQR) score=4 (6.3); p=0.006). The results of the psychological test using HADS are shown in Table 5.
Difference in HADS symptoms score and EQ5D VAS score before and after PCI.

Statistically significant p-values (p<0.05) are shown in bold.
Wilcoxon signed rank test.
Paired t-test.
HADS: Hospital Anxiety and Depression Scale; EQ5D: EuroQol-5 Dimension; VAS: visual analogue scale; IQR: interquartile range.
EQ-5D-5L and EQ VAS scores over time
The quality-of-life outcome was measured before and after PCI based on the EQ-5D-5L. Results showed an improvement in patients’ mobility following PCI (79.6%) relative to before PCI (76.9%). The subjects experienced less anxiety and depression after PCI, with 85.2% reporting no symptoms, compared to before PCI (67.7%). The mean current health VAS score improved significantly following PCI, with a score of 75±14.9, compared to before PCI, with a score of 68±12.6 (p<0.005; Tables 5 and 6).
Quality of life before and after PCI based on the EQ-5D-5L.

Discussion
CAD is the leading cause of mortality in Malaysia and worldwide. Contemporary cardiology excels at managing conventional cardiac risk factors as primary or secondary prevention strategies. Non-conventional cardiac risk factors, such as anxiety and depression, which may contribute to detrimental outcomes, are often overlooked. Addressing these non-conventional cardiac risk factors may provide added benefits to the clinical outcome of CAD patients.
The disease burden of depression is significantly higher in females than in males in the general population, consistent with the prevalence of depression observed in the CAD population. 12 Several examples in the literature have postulated that psychosocial factors, sex role factors and biological factors (i.e. hormonal) are the main contributors to the higher prevalence of depression among women than among men with CADs. Differences in behavioural and coping mechanisms, lack of social support, social integration and marital stress may be the main contributory factors to depression in women.13–15 The present study showed that sex was associated with anxiety and depressive symptoms both before and after PCI. Delewi et al. reported that their female study population had a significantly higher anxiety score before PCI, and this remained after PCI and upon hospital discharge compared to males. 16 Conversely, we found that females had 71% lower odds of developing depressive symptoms before the procedure than their male counterparts, but they were three times more likely to be depressive following the procedure.
Malaysia and Singapore have diverse multi-ethnic societies, namely, Malay, Chinese, Indian and other ethnicities. Our study reported that Malay ethnicity is one of the strongest predictors of anxiety after PCI, with a four-times likelihood of anxiety after PCI compared to other races. However, various published studies have shown an inconclusive association between race and anxiety following PCI, citing no significant association found between race and anxiety.17,18
The association showing that a higher education level is protective against depression has been well illustrated in several published studies. This study showed that the group with higher education was almost four times (79%) less likely to be anxious before PCI than those who did not receive formal education or primary school education. Gu et al. suggest that a higher level of education is protective against preoperative anxiety, depression and other affective disorders. 19 Highly educated subjects may have a better understanding of their illness and details of PCI procedures, which could alleviate their anxiety. 20
Percutaneous CAG enables centres in Kuala Lumpur to receive abundant referrals daily for CAD interventions from non-PCI-enabled centres around the nation, leading to long waiting lists for PCI interventions in the government sector. 21 The CAD cases in our centre were triaged to the following based on the urgency of PCI intervention (in order): STEMI for primary PCI, NSTEMI for PCI, angina pain (unstable/stable) and diagnostic coronary angiography. The elective cases scheduled for PCI from the outpatient clinic were typical of lower priority for PCI than elective ad hoc cases, comprising cases admitted for acute coronary syndrome (i.e. NSTEMI/unstable angina), which may benefit from early PCI intervention. Our study concluded that elective PCI cases were significantly associated with more depressive symptoms than elective ad hoc cases. We postulate that the longer waiting period required for elective outpatient cases preceded the intervention, which may heighten the stress, anxiety and depressive symptoms of the subjects, as they might be fearful of the procedure and feel uncertain of the outcome of their illness. Bengtson et al. suggested a strong association between anxiety and depression with the severity of angina pain and the uncertainty of the waiting period in a cohort awaiting coronary revascularisation. 22 The literature on patients with CAD waiting for coronary artery bypass surgery reports that angina symptoms, uncertainty about the waiting period for intervention, physical limitation due to CAD and dissatisfaction with the quality of health services are sources of anxiety.23,24
PCI is an invasive procedure. As expected, the procedure itself is the most significant stressor for patients. A comprehensive study evaluated a patient’s anxiety at different time points – on admission, before PCI, after PCI and on discharge – using the VAS anxiety score. The study reported that the subjects suffered the highest level of anxiety before PCI, and the mean VAS declined significantly following PCI across all independent variables. 16 Similarly, our evaluation using the EQ-5D-5L concluded that the mean health VAS score improved significantly after PCI, with our subjects experiencing less self-reported anxiety, less depression and more mobility. The subjects in our study were also evaluated using another assessment tool: the HADS score for anxiety and depression. We found a significant decline in median HADS anxiety and depression score after PCI, suggesting that PCI may be a significant stressor for patients. However, many subjects had definite depression following PCI, despite a significant reduction in the mean HADS depressive score. Factors other than PCI-related stressors, such as a limited understanding of the illness and procedure, fear of risks and complications associated with PCI and being physically unwell following the procedure, possibly explain the increased occurrence of depression after PCI.19,25
One major limitation of the study is volunteer bias. Patients who volunteered to take part in the study may have intrinsically different characteristics from the general population. In future studies, ensuring confidentiality and anonymity to the participants is crucial to increase the likelihood of volunteering and hence reduce volunteer bias.
Conclusions
The study concluded that PCI predisposes patients with CAD to experience psychological stressors, such as anxiety and depression. Female sex and Malay ethnicity were more significantly associated with psychological stress after PCI, whereas a higher education level appeared to be protective. Physicians should adopt multidisciplinary approaches in managing patients with CAD by targeting interventions on the psychological aspect, which is the non-conventional cardiovascular risk factor, and the conventional ones. General screening following PCI enables the identification of patients vulnerable to psychological stress. A simplified and comprehensive explanation of the procedure should be offered, especially to the less educated population. Social support from caregivers and society needs to be emphasised in physicians’ daily practices.
Supplemental Material
sj-docx-1-psh-10.1177_20101058211025996 – Supplemental material for Neglected cardiovascular risk factors: Relationship of anxiety and depression with percutaneous coronary angioplasty
Supplemental material, sj-docx-1-psh-10.1177_20101058211025996 for Neglected cardiovascular risk factors: Relationship of anxiety and depression with percutaneous coronary angioplasty by Mohd Firdaus bin Hadi, Kelvin Shenq Woei Siew, Mohd Al-Baqlish Mohd Firdaus, Edre bin Mohammad Aidid, Sylvia Wei Wei Kong and Imran Bin Zainal Abidin in Proceedings of Singapore Healthcare
Footnotes
Acknowledgements
The authors are indebted to all members of the Division of Cardiology at the Malaya Medical Centre who contributed to the management of the patients in this study.
Authors’ contributions
M.F., B.H., K.S.W.S., M.B.M.F. and I.B.Z.A. conceptualised the design of the study. S.K.W.W. and E.B.M.A. contributed to the acquisition and analysis of the data. M.F.B.H. and K.S.W.S. drafted and interpreted the data for the initial manuscript. M.F.B.H., K.S.W.S., M.B.M.F. and I.B.Z.A. reviewed and revised the intellectual content of the manuscript. All authors read and approved the final manuscript.
Availability of data and materials
The data used in the literature review are available from the corresponding author on reasonable request.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
Ethical approval to report this case/these cases was obtained from Institutional Ethics Committee of University Malaya Medical Centre approved (No: 202035-8360).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Informed consent
Written informed consent was obtained from the subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.