
Abstract
Background:
Breaking up sedentary behavior with standing or walking can decrease discomfort, fatigue, and sleepiness. However, less is known about acceptability and impact of resistance exercise breaks on these outcomes. Therefore, we evaluated the acceptability of resistance exercise breaks and their influence on discomfort, physical and mental fatigue, and sleepiness during occupational sitting.
Methods:
Workers completed two 4-hour conditions in random order: prolonged sitting (SIT) and sitting with hourly resistance exercise breaks (REX). All outcomes were measured at baseline and every hour thereafter with five total breaks. Linear mixed models evaluated overall condition effects and differences at each hour. Cohen’s d estimated magnitudes of effect. Acceptability was assessed via questionnaire after the REX condition and reported as percentages.
Findings:
Fourteen adults (age: 53.4 ± 9.5 years, body mass index [BMI]: 30.9 ± 4.8 kg/m2) were enrolled. Although ratings of discomfort, fatigue, and sleepiness were typically lower during REX as compared with SIT, overall outcomes were not significantly different between conditions (p > .05). However, a significant reduction in mental fatigue at hour 4 in favor of the REX condition (β = −0.48 log-points, p < .05, d = 0.37) was observed. Program acceptability questions revealed the majority (>50%) of participants reported a “4” or “5” on a 5-point Likert-type scale for all questions, indicating high acceptability for implementation.
Conclusions/Application to Practice:
Resistance exercise breaks had high acceptability and provided preliminary evidence of improving ratings of mental fatigue. More research is needed to better understand the role of resistance training to reduce sedentary behavior.
Introduction
Evidence supports reducing prolonged sedentary bouts to improve activity level as well as cardio-metabolic outcomes associated with increased health-related risk (de Rezende et al., 2014; Owen et al., 2010, 2011; Restaino et al., 2015). Although sedentary time can be accumulated in various forms (e.g., leisure time pursuits and transportation), occupational time contributes a large proportion (Yang et al., 2019). Time at work provides opportunities for implementation of strategies to reduce sedentary time (Owen et al., 2011) including active workstations (sit-stand desk), walking breaks, or resistance exercises (bodyweight or light resistance). Notably, the use of resistance exercise breaks is least studied, though recently appears to improve cardio-metabolic responses to prolonged sitting for glucose and blood pressure (Dempsey et al., 2016; Kowalsky et al., 2019).
Prolonged sitting is directly associated with increased levels of musculoskeletal discomfort, fatigue, and sleepiness at work (Baker et al., 2018; Daneshmandi et al., 2017; Hosteng et al., 2019) and perceived as detrimental to health (Gilson et al., 2011). Developing interventions to target these outcomes is important to combat issues such as the high prevalence of musculoskeletal pain in the United States, with 25% reporting musculoskeletal discomfort significant enough to impact daily living (Deyo et al., 2006) and 90% of workers reporting these symptoms regardless of severity (Widanarko et al., 2011). Previous research demonstrated interrupting sedentary behavior with brief bouts of walking or standing can lead to improvements in discomfort and fatigue (Gibbs et al., 2018; Kowalsky et al., 2018). Yet, it is not clear if resistance exercise breaks assist with discomfort and fatigue.
It is equally important to determine acceptability of programs in office environments from both an employee and employer perspective (De Cocker et al., 2015; Pellegrini et al., 2015). Although the use of resistance exercise breaks certainly has its limitations such as stopping work for a brief period of time, all activity interventions, regardless of method have limitations for implementation, such as space, cost, and equipment needs. Understanding benefits and limitations of all strategies is important for designing and implementing effective workplace interventions based on employee and employer needs and restrictions.
To address these gaps, we examined the acute (4-hour simulated work day) effect of interrupting occupational sitting time with hourly, brief resistance exercise bouts on discomfort, mental fatigue, physical fatigue, and sleepiness in working-aged adults. In addition, we assessed the acceptability of resistance exercise breaks and identified any barriers that could limit implementation.
Methods
We examined secondary outcomes from a previous study investigating the effects of resistance exercise breaks on cardio-metabolic health (Kowalsky et al., 2019). This study was approved by the University of Pittsburgh Institution Review Board. Subjects were recruited from the University of Pittsburgh Clinical and Transitional Science Institute research registry online and via posted flyers on campus and the surrounding community’s public bulletin boards. Interested individuals were instructed to call study staff to provide verbal interest and schedule screening visit. Participants did not have to be employed by the University of Pittsburgh to participate.
Individuals who were inactive, at increased risk for cardio-metabolic disease, and able to complete office-like tasks were recruited. Workers were included if they were 30 to 65 years old, had at least two of three predetermined cardio-metabolic risk factors (elevated blood pressure, increased abdominal obesity, or family history of metabolic disease and/or confirmed prediabetes), and were able to perform the resistance exercise breaks protocol (confirmed during screening visit). Workers were excluded if they engaged in >90 minutes per week of moderate-to-vigorous physical activity, participated in ≥2 days per week of resistance training, or had a contraindication to exercise based upon the physical activity readiness questionnaire (PAR-Q). Individuals who reported musculoskeletal conditions were included as long as they were able to perform the resistance exercises without any difficulty.
This study utilized a randomized crossover design with three separate laboratory visits separated by 2 to 14 days. Following the first in-person screening visit to confirm eligibility and obtain informed consent, individuals reported to the laboratory at 7:30 a.m. on two different occasions to complete each study condition. Each condition consisted of baseline testing, followed by a standardized meal (30% of daily caloric need, based on Harris–Benedict Equation) (Harris & Benedict, 1918), then 4 hours of performing seated, work-related tasks of the participants’ choice under direct observation of study staff. Participants were equipped with a computer with internet to simulate a typical office environment and could adjust the chair, screen, and keyboard for comfort.
For the prolonged sitting condition (SIT), participants were asked to sit the entire 4-hour session, except for restroom breaks. Number of restroom breaks were tracked and compared across conditions. During the condition, measurements of discomfort, fatigue, and sleepiness were assessed once per hour over the 4-hour condition to total five measurement times (including baseline) with paper-based questionnaires.
For the resistance exercise break condition (REX), participants completed the same protocol as the SIT condition with the addition of the hourly resistance exercise breaks (4 total). These breaks began 30 minutes into the 4-hour session, so that the breaks were offset from the measurement times by 30 minutes. Resistance exercises during the breaks were performed in the following order: (a) chair stands with calf raises, (b) desk push-ups, (c) lunges with high knees, and (d) banded bicep curls with upright row. Exercises were designed to target all major muscles groups and were performed as two sets of 15 repetitions each, with a minute rest between sets. Each exercise break utilized a standardized video that provided verbal and visual instructions for completing each exercise. Length of each break and time spent exercising (initiation of movement to completion of movement) was tracked. Ratings of perceived exertion (RPE) were measured following each exercise break to characterize intensity (6–20 scale) (Borg, 1998).
Physical discomfort was assessed using the self-administered Physical Discomfort and Fatigue Questionnaire developed by Stalker et al. (1997) and modified by Kar and Hedge (2016). This questionnaire first asks whether any discomfort is present. If present, the participant is asked to rate their levels of discomfort at 15 sites across the body using 100-point visual analog scales (ranging from 0 = no discomfort to 100 = extreme discomfort). This questionnaire also assessed physical fatigue and mental fatigue via single item, 100-point visual analog scales (ranging from no fatigue to extreme fatigue). Sleepiness was assessed using the Karolinska Sleepiness scale, a 9-point scale ranging from 1 (very alert) to 9 (very sleepy, great effort to keep awake, fighting sleep).
A final questionnaire was administered at completion of the REX condition to examine the acceptability of such programming in a real office setting. This included five questions regarding the acceptability of the resistance exercise breaks using 5-point Likert-type scales and an open-ended question about barriers. Questions asked about (a) their willingness to use a resistance exercise program at work, (b) how well it would be received by their coworkers and (c) employers, (d) if they would be comfortable doing the program unsupervised, and (e) whether the amount and frequency of the resistance exercise breaks was appropriate. Finally, to help characterize our sample, the questionnaire asked participants to self-report their office setting and job type.
Data Analysis
Analyses were performed using Stata 15 software (Statacorp LP, College Station, Texas). Statistical significance was set at p ≤ .05. Sample size for the parent study (N = 14) was predetermined to identify a difference in blood glucose between conditions (REX vs. SIT) (Kowalsky et al., 2019). Analyses were performed to check for normality of data and non-parametric testing or log transformation were performed when appropriate. Descriptive statistics were calculated to describe the sample. Generalized linear mixed models were used to evaluate the effects of condition on outcomes. A time-by-condition interaction was evaluated. If no interaction was present, mixed models evaluated the overall effect of condition (REX vs. SIT) controlling for baseline value, sex, age, and condition order. Cohen’s d was calculated to display the magnitude of effect for each variable. An exploratory, post hoc analysis evaluated the difference between conditions at individual time points. p values reported from the post hoc analyses are Bonferroni-adjusted to protect against type 1 error.
Results
For the 14 adults (53.4 ± 9.5 years, body mass index [BMI] 30.9 ± 4.8 kg/m2, 14% male, 36% non-White; Table 1), each exercise break ranged from 3.7 to 5.29 minutes, with time spent actually engaged in the exercises lasting 3.75 minutes. Ratings of perceived exertion for the exercise breaks ranged from 10.6 to 12.6. Number of restroom breaks between conditions were tracked and compared with no statistical difference between SIT vs. REX conditions (1.6 ± 1.2 breaks SIT, 1.6 ± 1.1 breaks REX, p = 1.00). Length of each restroom break was not tracked.
Demographic Characteristics of Study Participants (N = 14)
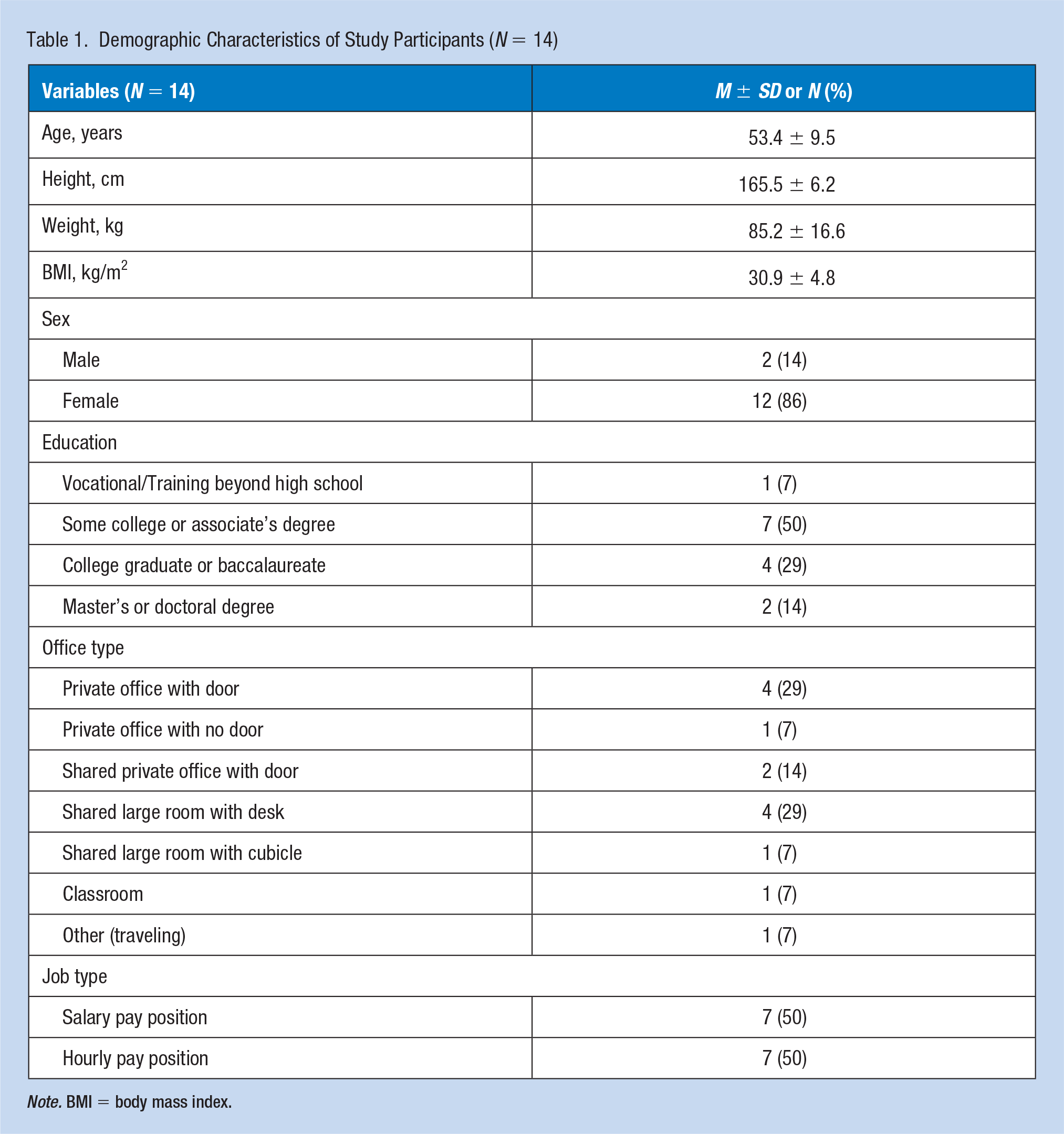
Note. BMI = body mass index.
Figure 1A displays the response for overall discomfort (log-transformed) by condition. Although there was no significant difference across conditions at baseline (β = −0.15 log-points, p = .076, d = 0.34), it should be noted that discomfort was higher at the beginning of SIT and increased throughout the day. Discomfort in the REX condition increased slightly, but returned near baseline values by the end of the 4-hour condition. Linear mixed modeling revealed no overall statistically significant difference between conditions; however, the difference approaching significance in favor of the REX condition. There were no statistically significant differences at each individual time points (all p ≥ .05).
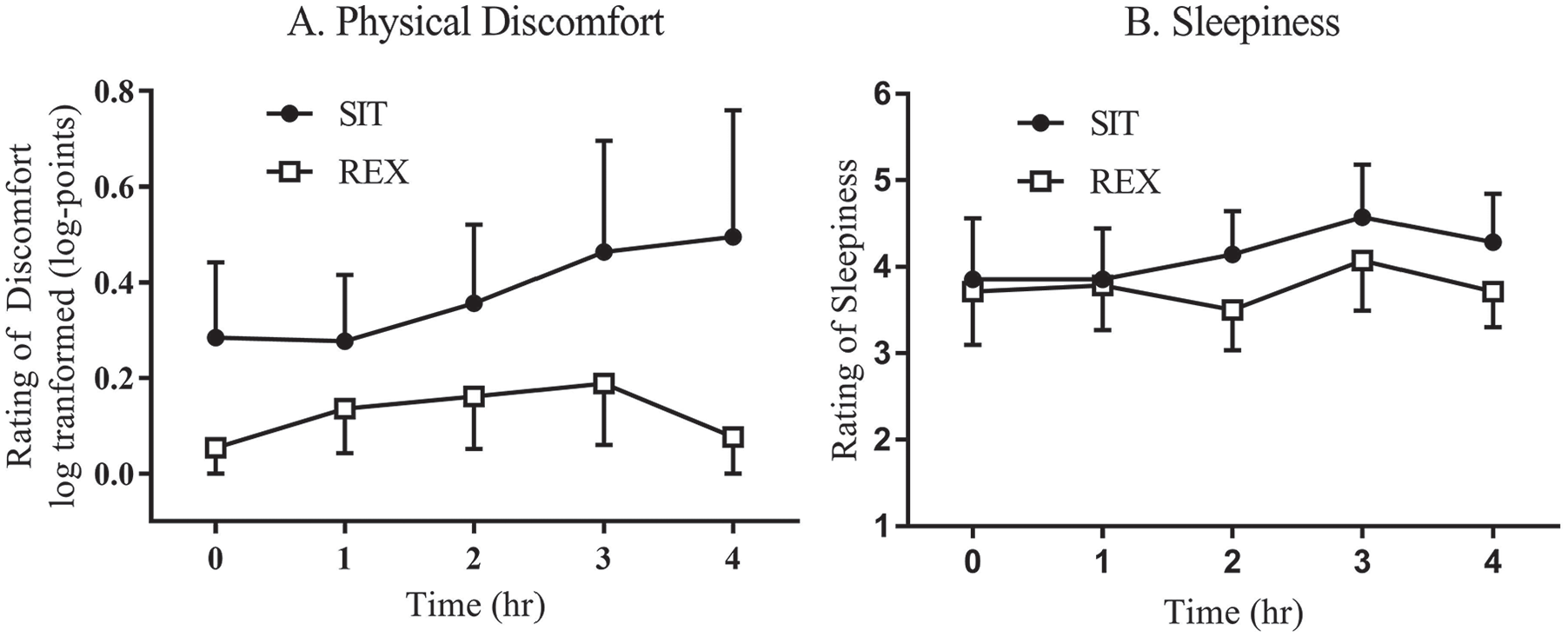
Overall discomfort and sleepiness response REX versus SIT.
Ratings for sleepiness were similar between conditions across the day (Figure 1B). Linear mixed modeling revealed no statistically significant difference between conditions for sleepiness (β = −0.33 points, p = .106, d = 0.14). Post hoc analysis revealed that no time points were statistically significant between conditions (p ≥ .05).
Figure 2 displays the response for both (A) mental and (B) physical fatigue (log-transformed), respectfully, by condition. Although both mental and physical fatigue were typically lower during REX versus SIT, linear mixed modeling revealed no statistically significant differences in overall effect by condition for mental fatigue (β = −0.23 log-points, p = .116, d = 0.18) or physical fatigue (β = −0.30 log-points, p = .056, d = 0.20). When analyzed further by individual time points, mental fatigue was statistically different at hour 4 (β = −0.48 log-points, p = .005, d = 0.37) but there were no statistically significant time points for physical fatigue (p ≥ .05).
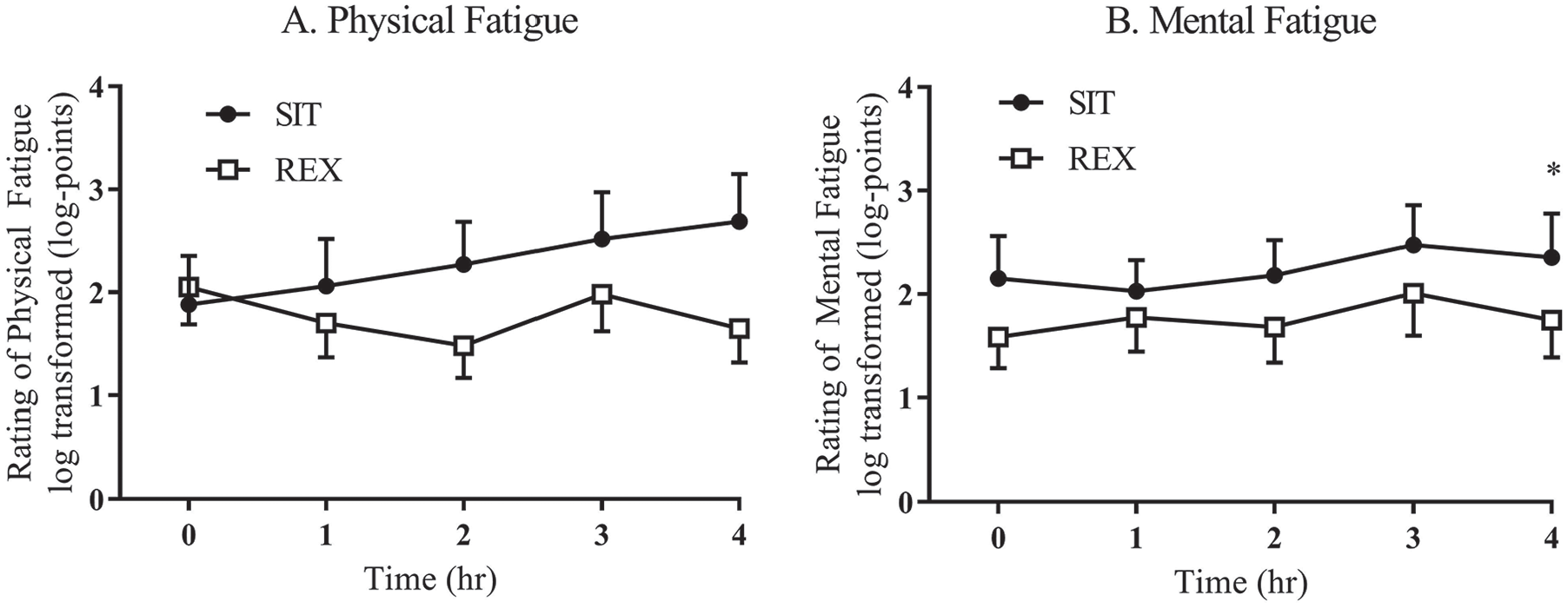
Mental and physical fatigue response REX versus SIT.
Questions addressing acceptability of REX breaks scored with ratings of “high” or “very high” as follows: Question 1: 86% regarding willingness to use exercises at work; Question 2: 100% thought it would be received well by their coworkers; Question 3: 72% thought it would be received well by their employers; Question 4: 57% for completing the exercises unsupervised; and Question 5: 65% if the amount and frequency of breaks was appropriate. Furthermore, an open-ended question asking for potential barriers revealed that seven out of 14 individuals reported concerns about the ability to adhere to the strict once per hour protocol, suggesting a need for more flexibility in the timing of breaks. Four out of 14 participants reported space as a potential barrier for implementing such a strategy.
Discussion
Our results indicate high acceptability for the use of resistance exercise breaks in the office to reduce sedentary behavior that reduced mental fatigue. To date, several studies have demonstrated improvements on ratings of discomfort, fatigue, and sleepiness via interventions designed to reduce occupational sitting (Foley et al., 2016; Gibbs et al., 2018; Kowalsky et al., 2018). However, no study to our knowledge has evaluated how these outcomes might be impacted by resistance exercise breaks. Our results provide preliminary data that support further exploration of resistance exercise breaks in the workplace.
A strength of this study includes the simulated work environment that allowed participants to complete ecological valid, personal work tasks, which in turn improves our external validity. In addition, having repeated assessment across each study visit allowed for comprehensive, time course analysis of outcomes. Yet, our study is not without limitations. Our 4-hour protocol, instead of a full 8-hour simulated workday, limits our conclusions. We also limit the generalizability of our results due to our recruitment criteria of increased cardio-metabolic risk, which was relevant for our primary study outcomes but does not reflect the entire working population. In addition, our study was previously powered to detect differences in our primary cardio-metabolic outcomes; this could have limited our ability to detect differences in this secondary analysis.
Studies have used various activity breaks to interrupt prolonged occupational sitting. For discomfort, activity breaks of walking, sit-stand desks, and stretching have all demonstrated a positive impact (Agarwal et al., 2018; Foley et al., 2016; Gibbs et al., 2018; Kowalsky et al., 2018; Waongenngarm et al., 2018). However, our study is one of the first studies to utilize resistance exercise breaks. Our study found no overall difference for discomfort. The lack of significance with our study could be due to the exercise stimulus (intensity or duration) not being sufficient to elicit change. Other studies have utilized low-level (load) resistance exercises with beneficial outcomes in chronic low back pain individuals (Carpenter & Nelson, 1999), but these exercises were performed to volitional fatigue. The difference in their intensity and study population could help explain why we did not observe a similar benefit. Therefore, our protocol should be explored with higher intensities and perhaps a longer duration of use (1 week or 1 month) with a diverse population, including those with significant musculoskeletal discomfort.
For mental and physical fatigue, we determined that there was no overall difference between conditions, but was in favor to lower values in the REX condition with a significant difference at hour 4 for mental fatigue. Similar findings for sleepiness were observed with non-significant lower values in the REX condition. Several strategies exist to reduce fatigue such as breaks ranging from 15 to 30 minutes that incorporate doing nothing, consuming food or drink, and taking a brief nap (Tucker, 2003), transitioning from sitting to standing (Kowalsky et al., 2018), and physical activity participation such as walking (Wennberg et al., 2016). Success with each of these interventions is related to type of activity the person is doing, length of the break, and at which point in the work period the break is taken (Tucker, 2003). Reducing fatigue is important because they contribute to reduced worker productivity, with up to 65.7% of individuals with fatigue reporting loss of productivity, costing employers $136.4 billion annually (Ricci et al., 2007). As for daytime sleepiness, it is associated with low exercise frequency (Chasens et al., 2007) and improved with higher amounts of physical activity (McClain et al., 2014). Therefore, programming like ours (if used daily) may be one strategy to counteract daytime sleepiness though our acute (1-day) exposure may not be sufficient.
Implications for Occupational Health Practice
Occupational health interventionists should consider the use of resistance exercise breaks to offset prolonged work sitting. Our preliminary findings suggest potential benefits which are clinically meaningful, yet mostly statistically insignificant. In addition, the high acceptability of the program suggests easy implementation, though interventionists should consider space available and ensure management supports the workers in these pursuits. Interventionists should consider using a flexible program as well, since completing resistance exercises hourly may not be feasible (yet could result in less benefit). Furthermore, with many U.S. adults not meeting the recommendations for participation in resistance exercise participation, this strategy may provide a simple solution to build resistance exercise into daily routines.
Applying Research to Occupational Health Practice
Our findings suggest that offsetting prolonged sitting with resistance exercise breaks once per hour resulted in a statistically significant reduction in mental fatigue after 4 hours. In addition, our findings suggest non-significant but clinically meaningful reductions in discomfort, sleepiness, and physical fatigue while using resistance exercise breaks. These findings, along with participants reporting high acceptability of resistance breaks into the office setting, suggest that using resistance breaks can provide health benefits in an easily implemented, cost-friendly approach. Employers and occupational health practitioners should consider using resistance exercise breaks to promote better health in the workplace. Implementation of this type of program should rely on flexibility with implementation and the support of management as well as providing reasonable space for completion of exercises to avoid the commonly perceived barriers for implementation. In addition, this programming would aid individuals attempting to meet the U.S. guidelines for weekly resistance exercise participation of 8 to 10 exercises 2 to 3 days per week.
Footnotes
Acknowledgements
The authors are thankful for the assistance provided by Sophy Perdomo, Tayler Magda, Nanami Mano, Alec Freeman, and Madison Hueber with data collection and management. Additional thanks must be given to the “Moving Health with Media Core” of the Healthy Lifestyle Institute at the University of Pittsburgh for filming, editing, and producing videos used in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the University of Pittsburgh School of Education Dean’s office student/faculty research grant, the University of Pittsburgh’s Council of Graduate Students in Education research grant, National Institutes of Health (Grant Number UL1 TR001857), and the Tomayko Foundation.
Author Biographies
Robert J. Kowalsky, PhD, earned his master’s and doctoral degrees in exercise physiology from the University of Pittsburgh. He is currently working as an assistant professor at Texas A&M University-Kingsville in the department of health & kinesiology.
Andrea L. Hergenroeder, PT, PhD, earned her master’s in physical therapy and her doctoral degree in exercise physiology. She is working as an associate professor in the department of physical therapy program at the University of Pittsburgh.
Bethany Barone Gibbs, PhD, earned her master’s and doctoral degree from John Hopkins University in epidemiology. She is currently working as an associate professor at the University of Pittsburgh in the department of health & human development.