
Abstract
Background: Sleep disorders can result in sleepiness, fatigue, and apathy, and may contribute to serious occupational consequences such as errors at work. The aim of the study was to examine the level of insomnia, sleepiness, and fatigue in a sample of Polish nurses. Methods: The research was conducted among nurses employed in the Lublin region of Poland. A sample of nurses were invited to participate in a survey in which we measured insomnia, sleepiness, and fatigue using the Athens Insomnia Scale (AIS), the Epworth Sleepiness Scale (ESS), and the Fatigue Severity Scale (FSS). Findings: Among the 200 nurses that were surveyed, 141 (70.5%) responded. The findings indicated that a total of 47.8% of the surveyed nurses reported insomnia. Half (50.0%) exceeded the threshold for fatigue relative to the general population. Although no differences in fatigue and sleepiness were observed by level of insomnia between those who did and did not work night shift, we observed an overall correlation between insomnia (AIS) and sleepiness (ESS), as well as between insomnia (AIS) and fatigue (FSS). Conclusions/Application to practice: This sample of Polish nurses displayed problems with sleep quality. The consequences of insomnia and fatigue challenge occupational health workers to go beyond traditional care and standard diagnostic tests. Undertaking preventive measures aimed at reducing health hazards, and the risk of making a mistake at work due to increased sleepiness and fatigue, in nurses are warranted.
Background
Human sleep is defined as an altered state in which there is an impaired conscious awareness of the external world with different controls, rhythms, emotions, and dreams (Chokroverty, 2017). Sleep is a transient, natural, periodic, spontaneous, physiologic phenomenon that is reversible. It consists of two main phases including rapid eye movement (REM) and nonrapid eye movement (NREM), which, together with wakefulness, form a circadian rhythm (Chokroverty, 2017; Kowalska, 2013).
During NREM sleep, metabolism slows down, blood pressure drops, and heart and respiratory rates decrease (Traczyk, 2010). This phase accounts for 70% to 80% of the total sleep time. REM sleep is characterized by rapid eye movements and dreaming. The REM sleep state accounts for 20% to 30% of the total sleep time (Chokroverty, 2017; Traczyk, 2010). During REM sleep, our awareness of external events decreases dramatically, and consciousness is dominated mainly by internal images and a lack of explicit thinking. It is assumed that the REM phase is responsible for memory consolidation, selective forgetfulness, and brainpower (Chokroverty, 2017; Hobson, 2004; Traczyk, 2010).
Because sleep determines the effectiveness of human performance in the real-life environment, proper sleep hygiene is essential. Sleep disorders may result in sleepiness, fatigue, and apathy, or lead to more serious consequences such as errors and accidents at work (Kasperczyk & Jośko, 2012; Millman, 2005). Unfortunately, estimates show that approximately 15% to 20% of professionally active inhabitants of Europe and North America perform shift work at night. According to the 2010 Central Statistical Office’s data in Poland, the percentage was smaller with 7.9% of all employees who worked at night, and 16.6% of those were comprised of social welfare and health care employees, including a substantial number of nurses (Burdelak & Pepłońska, 2013). Therefore, we aimed to examine the level of insomnia, sleepiness, and fatigue among Polish nurses who performed shift work with and without night duties.
Methods
This study was conducted in May and June 2017, and involved the implementation of an anonymous, voluntary survey among professionally active nurses from the Lublin region of Poland who performed rotation work with and without night work duties. According to the information provided by the Bioethics Committee of the Poznań University of Medical Sciences, consent to conduct research was not mandatory due to the anonymous nature of the study.
There are two main work systems among Polish nurses working as full-time employees. The first is based on 12-hour shifts, and most of the nurses hired by hospitals adhere to this system. This includes working three to four shifts per week, from 7:00 a.m. to 7:00 p.m. (or 7:00 p.m. to 7:00 a.m.). The second includes a work schedule including five workdays, Monday through Friday, from 7:00 a.m. until 2:35 p.m., for a total of 37.5 hours per week. It is important to mention that there are no nursing assistants at many Polish hospitals, and situations in which two nurses must care for 24 patients or more at a time are not unusual.
The study nurses were selected among randomly selected work units from two hospitals including one university hospital and one small community hospital. Fourteen hospital wards were selected randomly, as well as 14 to 16 nurses on each unit were randomly selected to participate (n = 200). This resulted in a 3:1 ratio of hospital unit types. For example, three general medicine units and three surgical units were chosen from the university hospital, while one general medicine unit and one surgical unit were chosen from the community hospital. The same number of questionnaires was distributed among nurses working in the intensive care units (ICUs), operating rooms, and outpatient clinic at both hospitals. Questionnaires were distributed and returned within a 2-week cycle, in which nurses were provided a sealed envelope to ensure privacy so they could express themselves freely.
Data Collection Tool
The data collection tool comprised of three scales including the Athens Insomnia Scale (AIS), the Epworth Sleepiness Scale (ESS), and the Fatigue Severity Scale (FSS). The surveys also ascertained demographic details about the respondents’ gender, age, work experience, place of living, education level, and type of work unit.
Insomnia
The AIS is based on the International Statistical Classification of Diseases and Related Health Problems (10th revision; ICD-10; Folrnal-Pawłowska et al., 2011) diagnostic criteria for insomnia. It consists of eight questions regarding frequency and severity of insomnia symptoms. The first five items pertain to sleep induction, awakening during the night, final awakening, total sleep duration, and sleep quality; the last three items refer to daytime symptoms including well-being, functioning capacity, and sleepiness during the day. Answer scores range from 0 to 3 with a total possible score ranging from 0 to 24. A total score of >6 indicates early symptoms of insomnia; the higher the score, the more intensive the symptoms of insomnia. The internal consistency of the Polish version measured with Cronbach’s alpha was .90 and the test–retest reliability was .92 (Folrnal-Pawłowska et al., 2011; Soldatos et al., 2003).
Sleepiness
The ESS measures the likelihood of falling asleep in eight typical situations. Each statement is accompanied by numerical values from which the participant selects the best answer that conveys with their likelihood of falling asleep in a given situation (0—probability of falling asleep, 1—mild, 2—moderate, 3—high; Johns, 1991). The final score is the sum all the points (possible range = 0–24), with a score >9 indicating excessive daytime sleepiness. The original version of the questionnaire was found to have a high level of internal consistency (Cronbach’s α = .88), while the Polish version had a lower, but still respectable level (.69; Tryniszewska, 2012).
Fatigue
The FSS measures the degree of fatigue that one is experiencing, and is comprised of nine statements in which the participant is asked to rank on a 7-point scale the degree to which they identified with the statement. Lower values indicate poor identification; whereas, a high value indicates greater identification or agreement. The scale score is the sum of points for all statements; with a score >36 indicating greater-than-normal fatigue. The final outcome of the scale is usually divided by 9 (for the total number of items), providing the mean score for the nine items as the FSS score. Internal consistency measured with Cronbach’s alpha was .93 (Krupp et al., 1989; Valko et al., 2008).
Data Analysis
Descriptive statistics were employed to examine the demographic characteristics of the study population by calculating frequencies by demographic strata. To examine the differences between the tests results and sex or work scheme, the Mann–Whitney U test was used. Due to the lack of a normal distribution, the Spearman rank correlation coefficient was computed to detect the relationship between other variables. R Spearman correlation was also utilized to determine whether the ESS and FSS results increased along with an increase in the AIS results. Statistical significance was assumed at p < .05. All data analyses were performed using Statistica 13.2 software.
Results
Among the 200 nurses that were surveyed, 141 (70.5%) responded. After the completeness and correctness of the questionnaires were verified, the results of 134 forms were analyzed. The participants comprised of 84 nurses (62.7%) who performed rotation work with night duties, and 50 nurses (37.3%) who worked day shift only (Table 1). Most of the nurses were female (85.8%). More than half of the nurses (56.4%) had over 20 years of experience in the profession. Most of the participants who decided to be surveyed worked on general medicine (28.4%) and surgical (35.1%) units. Only 10 nurses (7.5%) employed in the outpatient clinic decided to complete the questionnaires. Over half of the participants (58.2%) resided in urban areas, while the remaining resided in villages (21.6%) or towns (21.6%). One-fourth (25.4%) were registered nurses (RNs) without further education, while 24.6% had obtained a bachelor’s in nursing (BSN), and almost half (47.8%) had obtained a master’s degree.
Characteristics of the Study Nurses (n = 134)
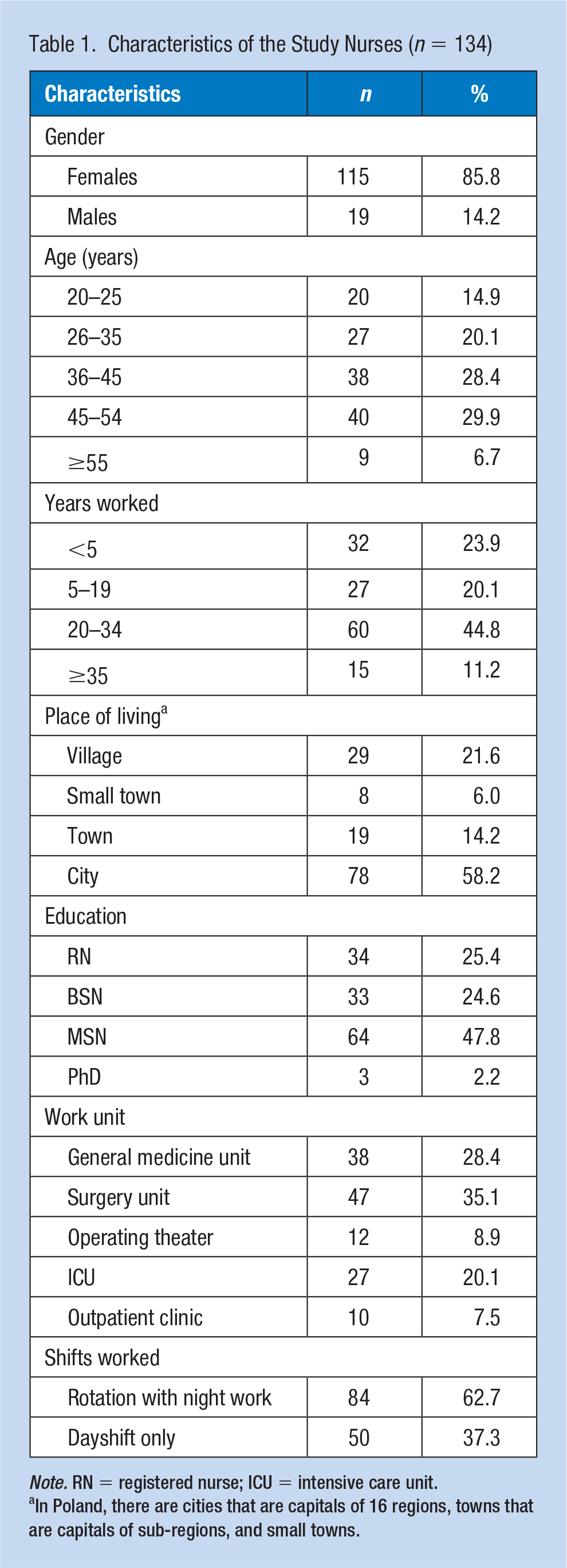
Note. RN = registered nurse; ICU = intensive care unit.
In Poland, there are cities that are capitals of 16 regions, towns that are capitals of sub-regions, and small towns.
The overall mean (standard deviation [SD]) results of the AIS for insomnia was 7.76 ± 4.33 which indicates early symptoms of insomnia (Table 2). The mean results of the AIS for both sexes were similar including 7.11 ± 4.42 for males and 7.87 ± 4.33 for females (p = .450). The female participants assessed their fatigue (FSS) at a mean level of 3.26 ± 1.33, while the males had lower FSS score, with a mean of 2.70 ± 1.43 (p = .079). In addition, no significant correlations between age and AIS, ESS, and FSS were found. It is worth highlighting that nurses aged 46 to 54 years obtained the highest results in all the scales. With regard to education (excluding PhD nurses due to low numbers), AIS for the nurses with a bachelor’s degree had a mean of 7.52 ± 4.61 compared with 7.89 ± 4.15 for those with a master’s degree. The range of the results for the FSS was very small with 3.01 ± 1.39 (RN) to 3.32 ± 1.43 (BSN). Only in the ESS, the nurses with bachelor’s degree obtained results considerably higher (9.18 ± 4.43) than the rest of the study participants (7.14 ± 4.59 to 7.81 ± 4.21). Nevertheless, the difference was not statistically significant (p = .884).
Relationship Between Nurse Participant Characteristics and Insomnia (AIS), Sleepiness (ESS), and Fatigue (FSS)
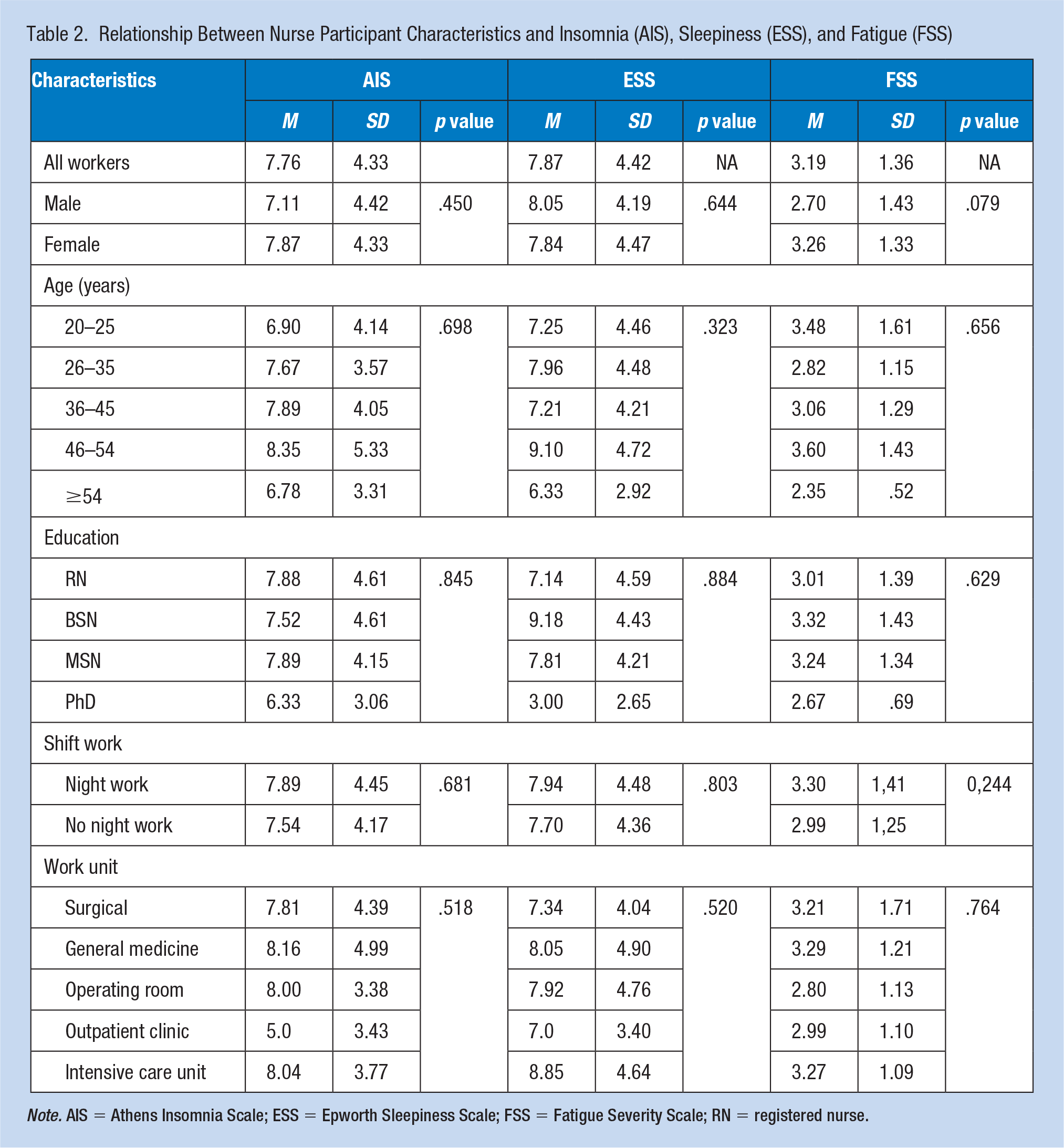
Note. AIS = Athens Insomnia Scale; ESS = Epworth Sleepiness Scale; FSS = Fatigue Severity Scale; RN = registered nurse.
For nurses who worked shifts with night duties, the mean AIS was 7.89 ± 4.45, compared with 7.54 ± 4.17 for those who did not work at night, indicating no correlation between insomnia and work schedule (p = .679). When we examined categories of AIS, we observed very little difference between those who worked at night and those who did not regardless of AIS categories of borderline insomnia (36.9% night shift vs. 38.0% day shift), as well as insomnia (26.2% night shift vs. 28% day shift). The ESS results were similar for both groups, with scores of 7.94 ± 4.46 among the nurses who worked at night and 7.76 ± 4.48 among those who did not work at night, with no statistically significant differences between the groups (p = .803). In addition, the FSS results were not significantly diverse for those who worked at night (FSS = 3.30 ± 1.41) and for those who did not (FSS = 2.99 ± 1.25), suggesting that neither group was fatigued.
The final stage of the statistical analysis involved determining whether higher AIS resulted in higher ESS and FSS using R Spearman rank correlation. Statistical analysis showed that nurses who presented more serious problems with insomnia (AIS) experienced sleepiness more frequently during the day (ESS; p = .006; Figure 1) and were more fatigued (FSS; p = .012; Figure 2).
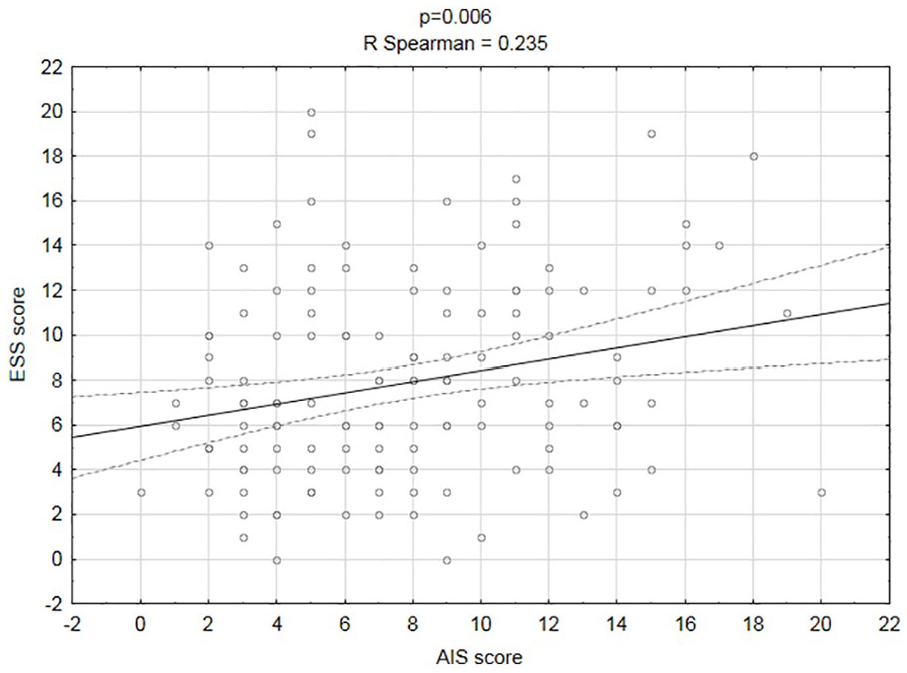
Correlation between insomnia (AIS) and sleepiness during the day (ESS).
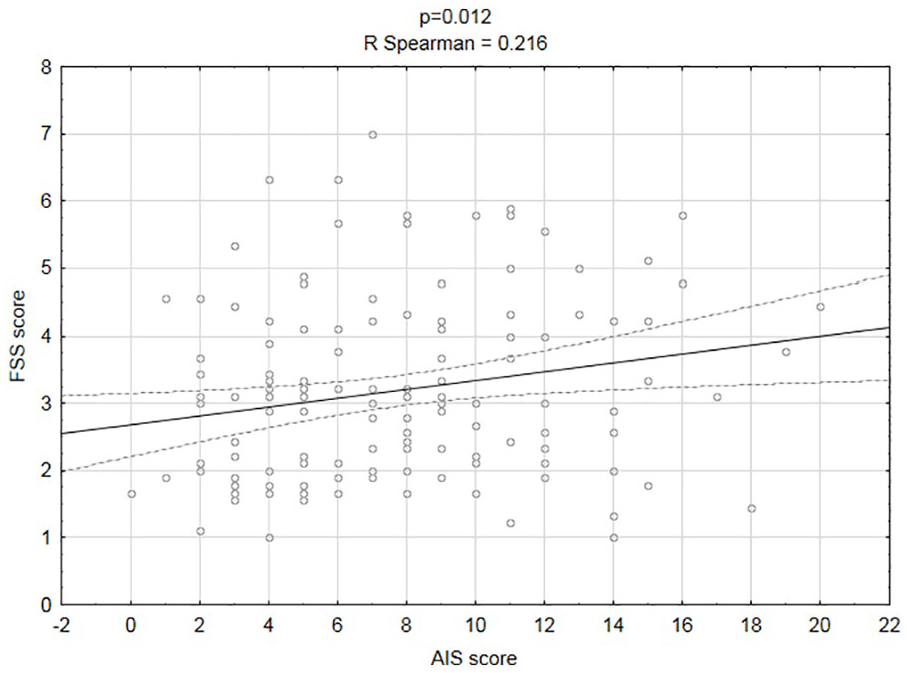
Correlation between insomnia (AIS) and fatigue (FSS).
Discussion
The research performed among the given sample of nurses did not prove that rotation work with night duties had any influence on the prevalence of insomnia. The results obtained for both groups were similar; however, the mean result lead to the conclusion that more serious problems with sleep may occur in nurses. In the research by Folrnal-Pawłowska et al. (2011), aimed at Polish validation of the AIS, two score divisions were obtained. The first division regarded individuals suffering from insomnia and the second one was the control group comprised of healthy individuals. The mean results obtained in nurses ranged between the two divisions indicating that nurses as a group are on the borderline of insomnia. The fact that almost half of the studied population of nurses scored 8 points or more on the AIS was concerning. According to the research by Folrnal-Pawłowska et al. (2011), the result suggests that approximately half of nurses suffered from inorganic insomnia according to ICD-10 criteria.
The results for the ESS were similar between the groups of nurses working at night, which diverges from the results described in other studies. The research by Thun et al. (2016) among Norwegian nurses showed that shift work with night duties was associated with greater sleepiness during the day. Shen showed that shift work among nurses is linked with insomnia, while regular daytime or nighttime shifts were not associated with sleep disorders. Research by Shen et al. (2016) indicated that shift work negatively influenced not only nurses’ sleep patterns but also their health. In addition, Jung and Lee (2016) in a study of 1,431 nurses from South Korea showed a link between rotation work involving night duties and sleep disorders.
The differences between research outcomes may result from various factors, such as the small sample size in this study; we may not have had the power to detect true differences. According to the Head Chamber of Nurses and Midwives Report (2017), in Poland in 2016 there were an average of 5.66 professionally active nurses per 1,000 patients, whereas in Norway, there were as many as 14.84 nurses per 1,000 patients (Wójcik et al., 2007). This remarkable difference may indicate that Polish nurses are overworked. This was supported by Gaweł et al. (2010), who showed that as many as 44% of participating nurses in their study indicated that an excessive number of tasks with a reduced number of staff was a factor that hindered their work. Moreover, factors concerned with work organization, such as poor relationships with supervisors or a lack of independence, may lead to frustration and high levels of stress, which can result in sleep disorders or fatigue (Gaweł et al., 2010).
In this study, no difference in the prevalence of fatigue was noted between nurses doing rotation work with and without night duties. The combination of occupational stress, physical overload, and duty-bound contact with dying and ill patients has been associated with an increased need for rest and sleep (Santorek-Strumiłło et al., 2012). This problem was also noted by Berger and Hobbs (2016), who highlighted the relationship between shift work, disturbed sleep patterns, and patient safety. One solution suggested by Berger and Hobbs (2006) is a short (maximum of 20 minutes) second-phase nap, such as a “power nap.” Moreover, it is essential to raise awareness among the people who manage nurses’ work to ensure that they plan work schedules in ways that do not overload the staff. Proper sleep hygiene should be taken into consideration in the work schedule not only to protect the personnel’s health but also for the sake and safety of patients. The results obtained in this study call for considering the factors that are responsible for increased fatigue and sleep disorders among nurses. The authors are planning further, more advanced research in this field.
The main weakness of the study was the limited sample size. This research suggests the need for future, larger studies. The study did not include data such as marital status, having children, or being a family caregiver, which may affect sleep quality and fatigue level. Further research into sleeplessness and fatigue in nurses should also consider chronic diseases, the use of psychoactive drugs, and mental disorders as disruptive factors.
Implications for Occupational Health Nursing
Polish nurses are overworked and face problems with sleep quality. Occupational health nurses should be aware of this issue because it may lead to adverse health conditions for nurses, as well as decreased work efficiency. Another consequence of fatigue may be a reduced resistance to stress. An individual who cannot recharge fully in the course of sleep tends to cope with stress in a worse manner, reacts nervously, or may not be able to perform their professional tasks. Moreover, it can lead to professional burnout and lack of job satisfaction. The aforementioned consequences of insomnia and fatigue impose on occupational health nurses challenges that go beyond traditional care and standard diagnostic tests. Deeper interviews during periodical examinations may be needed to diagnose sleep disorders and chronic tiredness. Some ready-made questionnaires for the assessment of sleep disorders and tiredness rate, such as the AIS or the FSS could be utilized. This information could guide occupational health nurses with better assessing and guiding nurses.
Conclusion
Insomnia can be suspected in almost half of the researched Polish nurses. No correlations between work schedule and the incidence of insomnia, sleepiness, and fatigue were found, possibly because of the lack of employment standards for Polish nurses. Nurses with more severe insomnia experienced sleepiness and were more tired during the day.
Application to Practice
Sleep greatly influences the effectiveness of human performance in the real-life environment. Sleep disorders (such as insomnia) may result in sleepiness, fatigue, and apathy, or lead to more serious health and occupational consequences. This study showed that our sample of Polish nurses had poor sleep quality. The findings indicated that a total of 47.8% of the surveyed nurses reported insomnia. Half of them (50.0%) exceeded the threshold for fatigue. It is essential to raise awareness among those who manage nurses’ work to ensure that they plan work schedules in ways that do not overload the staff. Proper sleep hygiene should also be taken into consideration in the work schedule not only to protect the worker’s health but also for the sake and safety of patients. Occupational health nurses can play a key role in raising awareness of the consequences of sleep disorders and the need for sleep hygiene.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Tomasz Zdanowicz, BSN, MSN, is a nurse at Anaesthesiology and Intensive Therapy Department at Teaching Hospital Number 4 in Lublin. He is a doctoral student in health sciences at the Chair and Department of Neurological Nursing, Faculty of Health Sciences, Medical University of Lublin.
Krzysztof Turowski, MD, PhD, is the head of the Chair and Department of Neurological Nursing, Faculty of Health Sciences, Medical University of Lublin. He is a neurosurgeon at Teaching Hospital Number 4 in Lublin.
Jolanta Celej-Szuster, MSN, PhD, is a research assistant at the Chair and Department of Neurological Nursing, Faculty of Health Sciences, Medical University of Lublin.
Regina Lorencowicz, MSN, PhD, is an assistant professor at the Chair and Department of Neurological Nursing, Faculty of Health Sciences, Medical University of Lublin.
Elżbieta Przychodzka, MSN, PhD, is an assistant professor at the Chair and Department of Neurological Nursing, Faculty of Health Sciences, Medical University of Lublin.