
Abstract
Modifiable, behavioral risk factors like occupational sitting may contribute to inflammation, an important cardiovascular risk factor. This study evaluated the association of self-reported occupational sitting with changes in c-reactive protein (CRP) and the role of sex. We examined occupational sitting and baseline CRP levels for 2889 African American participants in the Jackson Heart Study. Four multivariable linear regression models were estimated to determine the association of occupational sitting and CRP. Analyses were conducted in 2020. The mean age was 50.8 years and 61% were female. Participants who reported occupational sitting as “often/always” had CRP levels of 4.9±6.8 mg/L, “sometimes” had levels of 4.8±8.1 mg/L, and “never/seldom” had levels of 4.3±6.8 mg/L. In the unadjusted model, “often/always” engaging in occupational sitting was significantly associated with higher levels of CRP when compared to “never/seldom” (P < .05). This differed by sex with female participants who reported “often/always” occupational sitting had CRP levels of 6.0±7.6 mg/L compared to only 5.1±6.9 mg/L for “never/seldom.” Neither the overall association nor the female-specific association remained statistically significant in the adjusted models. We found an association between occupational sitting and inflammation, measured by CRP. This association varied by sex but did not remain significant after fully adjusting for covariates.
“…the association between occupational sitting and CRP varied by sex but did not remain independently significant…”
Background/Introduction
African Americans have higher rates of cardiovascular disease (CVD) and shorter life expectancy compared with White individuals.1,2 These racial disparities continue to persist despite advances in identifying CVD risk factors and the use of evidence-based practices to manage and prevent cardiovascular diseases, particularly atherosclerosis.1,2 With the understanding that atherosclerosis is an inflammatory process, c-reactive protein (CRP), a biomarker used to measure inflammation, has been identified as a CVD risk factor. 3 CRP is one of the most studied inflammatory markers, and previous epidemiologic studies have shown that increased levels of CRP are associated with adverse cardiovascular events in adults.4-6 It has been shown previously that engaging in increased levels of physical activity is associated with decreased levels of CRP. 7 However, little is known about sedentary behavior and its implication for CRP.
Sedentary behavior is defined as any waking behavior carried out in the lying, reclining, or sitting position and characterized by an energy expenditure of ≤ 1.5 metabolic equivalents (METs). 8 Technological advancements have altered work and recreation in the United States to be more conducive to sedentary behaviors, especially prolonged sitting.9,10 Prolonged sitting has been found to have adverse implications for health,11,12 and the workplace has become an important environment for the promotion of physical activity and reduction of sedentary behavior. In a typical, contemporary occupational environment, workers spend more than half of their entire workday seated. 13 Due to the reduction in discretionary time after the workday, overall workplace demands tend to influence lifestyle choices outside of work (ie, less time engaged in both light- and moderate-to-vigorous physical activity).10,14 Therefore, the occupational environment represents an important realm of an individual’s activity profile.
A recent systematic review found that occupational behaviors, such as sitting, can have negative health implications due to duration and repetition of the behavior, and both environmental and psychological factors. 15 Recent evidence has shown that occupational physical activity is directly associated with CRP levels, suggesting an increased risk of inflammation. 16 A small body of literature has also examined the association between occupational sitting and CVD risk factors, and the results are varied. Some studies have indicated that occupational sitting has no association with any CVD risk factors and/or CVD outcomes for African Americans17-19; however, one investigation has indicated an inverse relation between occupational sitting and subclinical atherosclerosis among African Americans. 20 There is limited evidence implicating occupational sitting as a risk factor for inflammation among African Americans, who make up 13% and 37% of the work force in the United States and Mississippi, respectively. 21
Additionally, females tend to have higher CRP levels and engage in more occupational sitting than males.22,23 The current study evaluated the association between occupational sitting with CRP in a large sample of African Americans in the Jackson Heart Study, conducted in the greater Jackson, Mississippi metropolitan area. Because sex appears to play a potential role in both occupational sitting and CRP levels, these associations were also examined separately for males and females.
Methods
Population
The Jackson Heart Study (JHS) is a single-site, population-based, prospective, cohort study investigating the determinants of CVD among African Americans living in the greater Jackson, Mississippi metropolitan area. Details on study design, recruitment, and collection have been previously published.24,25 Briefly, 5301 non-institutionalized African Americans ≥ 21 years of age living in the 3 counties including and surrounding Jackson (Hinds, Madison, Rankin counties) provided their written, informed consent and were enrolled in the study between September 2000 and March 2004. Data for this study was drawn from the baseline Exam 1, which had 3 components: a home interview, a self-administered questionnaire, and a clinic visit collecting blood samples, anthropometrics, and clinical measures associated with CVD risk. The research was approved by the Institutional Review Boards (IRBs) at the University of Mississippi Medical Center, Jackson State University, and Tougaloo College. Participants were excluded from all analyses if they had incomplete data for the independent variable of occupational sitting (n = 1846), dependent variable of CRP (n = 59), and the covariates (income: n = 468; education: n = 4; smoking: n = 19). Further exclusions were made if the participant reported having an occupation of military (n = 3), unemployed (n = 2), retired (n = 1), or student (n = 1). Participants who reported “never” or “always” for each sitting, standing, and walking at work simultaneously were excluded (n = 9). 20 Thus, the current analyses were restricted to 2889 participants.
Measurement of Occupational Sitting
The Jackson Heart Study Physical Activity Cohort (JPAC) survey was administered by trained interviewers prior to the clinical examination.24,26 The JPAC was derived and adapted from the Baecke physical activity survey to improve the quality of physical assessments among African American adults. 26 The JPAC provides 4 subscores for the different areas of physical activity: 1) active living; 2) occupational activities; 3) home, family, yard, and garden; and 4) sports and exercise. 26 The occupational activity area of the JPAC includes 8 items assessing occupational-related physical activity (ie, sitting, walking, standing, lifting heavy loads, etc.).
Occupational sitting was measured using the single-item question of the JPAC: “When you are at work how often do you sit?”. Response options included “Never,” “Seldom,” “Sometimes,” “Often,” and “Always.” For analyses of occupational sitting, the participants were grouped as follows: “never or seldom,” “sometimes,” and “often or always,” with “never or seldom” serving as the referent group. 20 Overall assessment of occupational sitting using a single-item question from the Last 7-Day Sedentary Time Questionnaire (SIT-Q-7d) has been validated against accelerometry and activity logs (rho = .63) and has an intraclass correlation coefficient of .74, indicating good reproducibility. 27
Measurement of C-Reactive Protein
Blood samples of CRP (mg/L) were measured by the immunoturbidimetric-latex assay method (Kamiya Biomedical Company, Seattle, WA) using a Hitachi 911 analyzer (Roche Diagnostics, Indianapolis, IN). Measurements of CRP were conducted in duplicate with any duplicates not within 3 standard deviations (SD) from one other being rerun. The interassay coefficient of variation on the control samples and the reliability coefficient for the masked quality control replicates were 4.4% and 95%, respectively. 28
Covariates
Potential covariates from the current exam were chosen based on existing literature regarding factors that may influence occupational behaviors and systemic inflammation. Covariates included sociodemographic characteristics (age,
29
sex,
30
education,
31
income
31
), select CVD risk factors
20
(body mass index,
32
diabetes,
33
hypertension,
34
cholesterol
34
[total, HDL]), lifestyle behaviors (cigarette smoking,
32
leisure-time moderate-to-vigorous physical activity
29
[defined by the American Heart Association’s Life’s Simple 7
35
], occupational standing and walking
36
(single-item questions from JPAC), and self-reported history of myocardial infarction and stroke.
36
In Figure 1, we present a directed acyclic graph (DAG) used to determine the covariates that were introduced into the analytic model per the DAG rules.
37
Directed acyclic graph (DAG) for the causal relationship between occupational sitting and CRP. Factors in boxes are covariates to adjust for per the DAG rules. Sociodemographics included age, sex, education, and income. Cardiovascular disease risk factors included diabetes, hypertension, cholesterol (total, HDL), and self-report myocardial infarction and stroke. Lifestyle behaviors referred cigarette smoking, leisure-time moderate-to-vigorous physical activity, occupational standing, and occupational walking. Note: CRP: c-reactive protein, DAG: directed acyclic graph.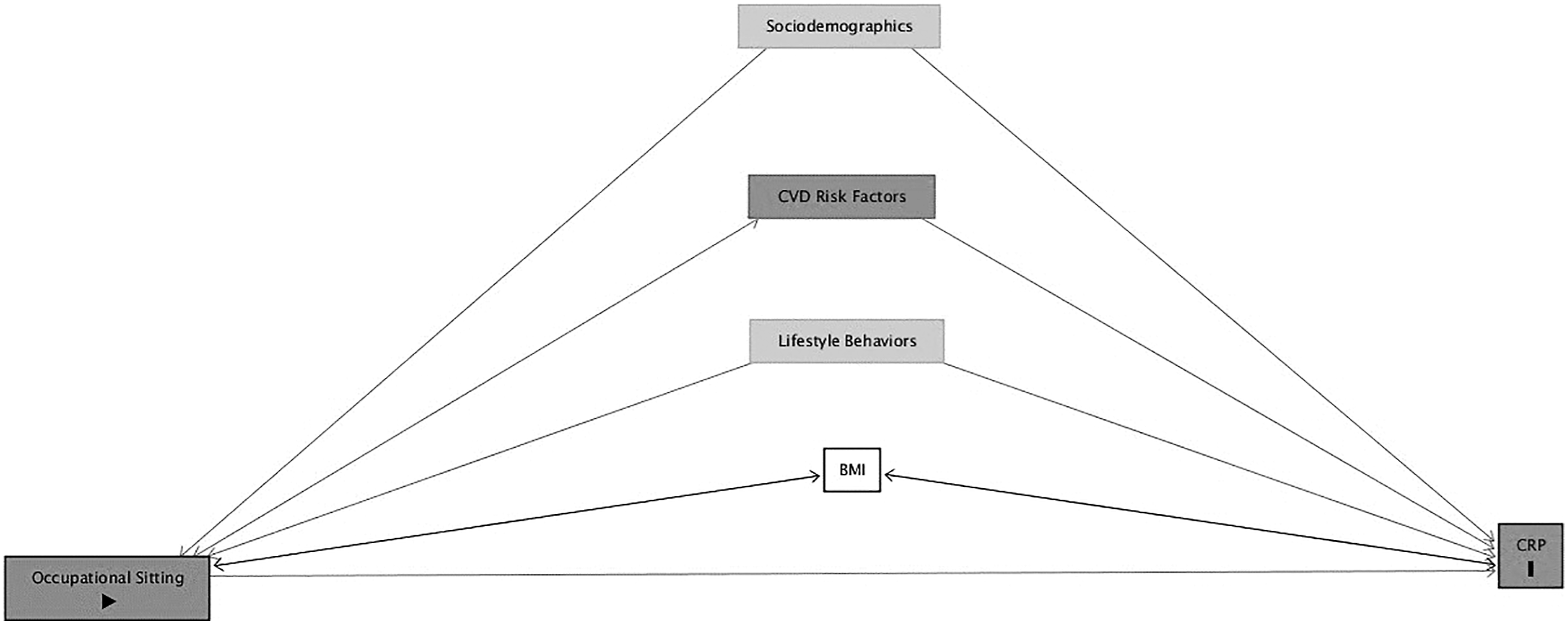
Statistical Analysis
Sample characteristics are described for the total sample and by occupational sitting categories using means and standard deviations for continuous variables and percentages for categorical variables. One-way analysis of variance (ANOVA) and chi-square tests were used to assess how participants at each occupational sitting category varied across the different indicators. Because the distribution of CRP was skewed within this JHS cohort, CRP was log-transformed for the analyses.28,38-40
Hierarchical regression models were used to determine the association of occupational sitting and CRP after adjusting for covariates. Four models were specified. Model 1 was unadjusted. Model 2 was adjusted for age, sex, and BMI. Model 3 further adjusted for income, education, smoking status, hypertension, diabetes, total cholesterol, HDL cholesterol, history of stroke, and history of myocardial infarction. Model 4, the fully adjusted model, included all variables in model 3 and moderate-to-vigorous physical activity, occupational standing, and occupational walking. Diagnostic tests were run to assess for variance inflation among the predictors and covariates in the models. The average variance inflation factor (VIF) was 1.89 with the highest VIF of 3.23, indicative of no correlation between the variables in the models; thus no additional attention was required.
Analyses were repeated to determine the association of occupational sitting with CRP when stratified by sex. P-values < .05 were considered significant. Reporting includes regression coefficients (B), standard error (SE), significance (p), model fit [r2]). All statistical analyses were conducted in 2020 using StataSE Version 16 (StataCorp LLC, College Station, TX).
Results
Characteristics
Distribution of Characteristics of African Americans in the Jackson Heart Study for the Overall Sample and by Occupational Sitting Category.
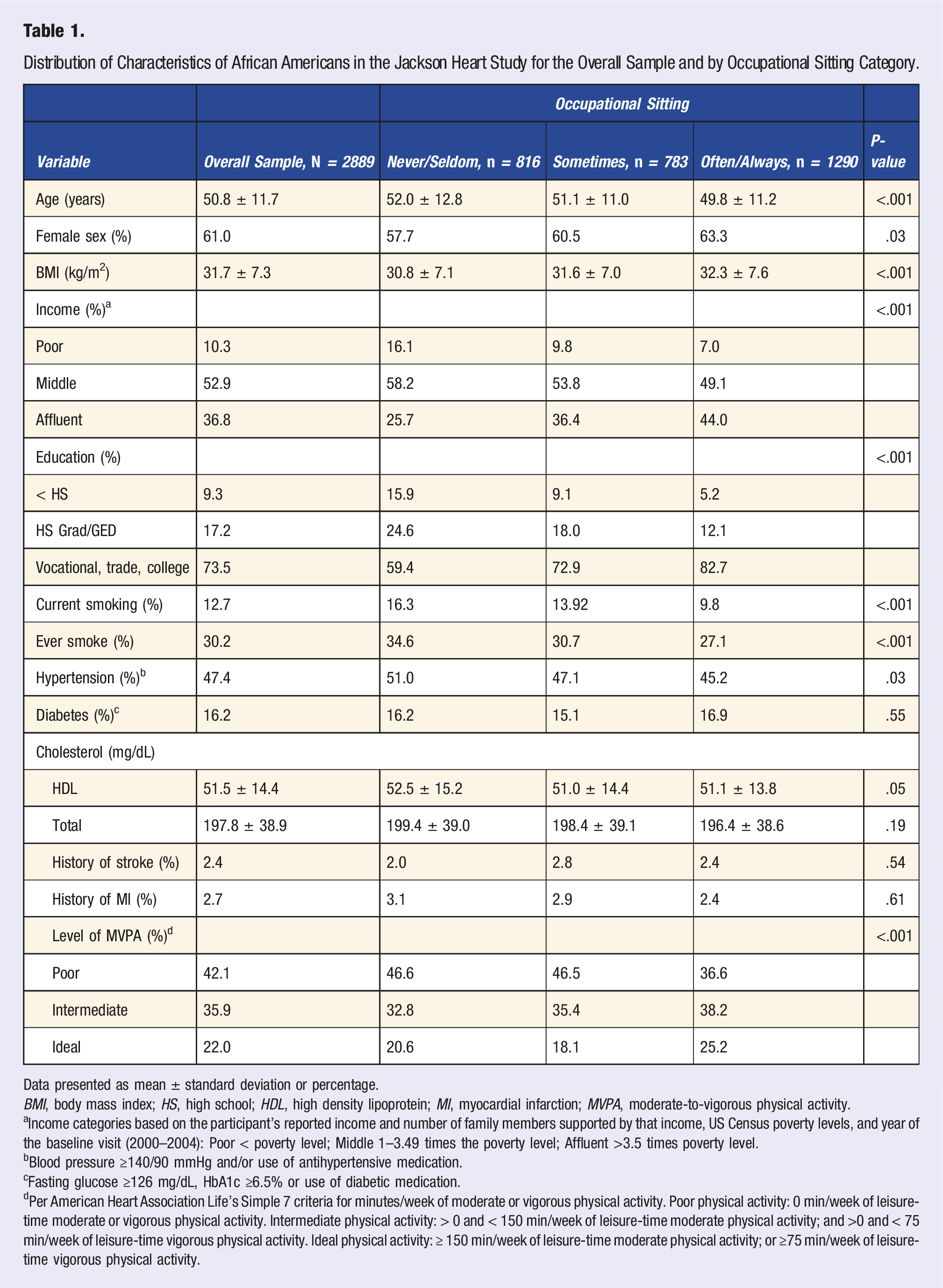
Data presented as mean ± standard deviation or percentage.
BMI, body mass index; HS, high school; HDL, high density lipoprotein; MI, myocardial infarction; MVPA, moderate-to-vigorous physical activity.
aIncome categories based on the participant’s reported income and number of family members supported by that income, US Census poverty levels, and year of the baseline visit (2000–2004): Poor < poverty level; Middle 1–3.49 times the poverty level; Affluent >3.5 times poverty level.
bBlood pressure ≥140/90 mmHg and/or use of antihypertensive medication.
cFasting glucose ≥126 mg/dL, HbA1c ≥6.5% or use of diabetic medication.
dPer American Heart Association Life’s Simple 7 criteria for minutes/week of moderate or vigorous physical activity. Poor physical activity: 0 min/week of leisure-time moderate or vigorous physical activity. Intermediate physical activity: > 0 and < 150 min/week of leisure-time moderate physical activity; and >0 and < 75 min/week of leisure-time vigorous physical activity. Ideal physical activity: ≥ 150 min/week of leisure-time moderate physical activity; or ≥75 min/week of leisure-time vigorous physical activity.
Occupational Activity Characteristics of African Americans in the Jackson Heart Study for the Overall Sample and By Occupational Sitting Categories.
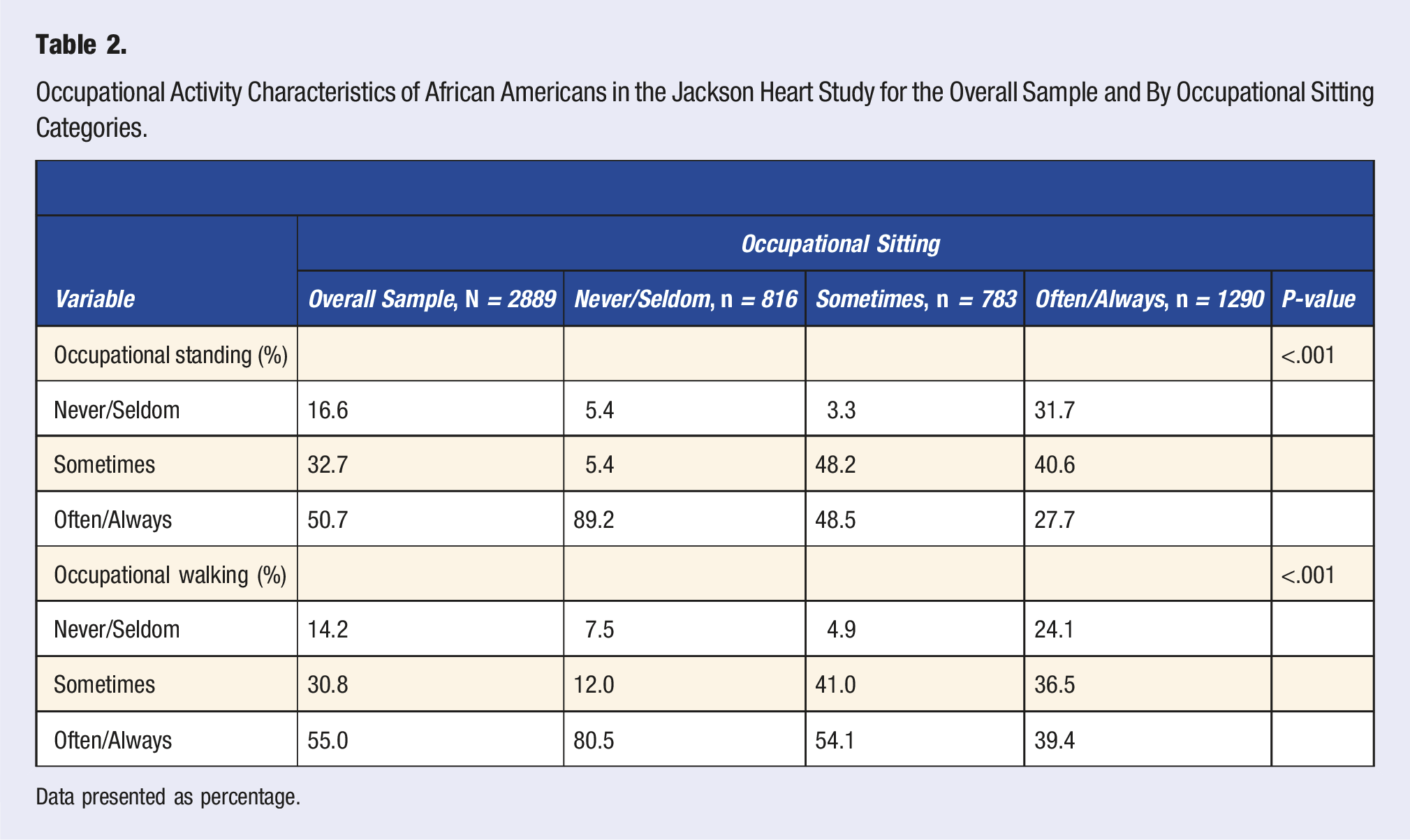
Data presented as percentage.
Occupational Sitting and CRP
Relation Between Occupational Sitting and CRP Among African Americans in the Jackson Heart Study.
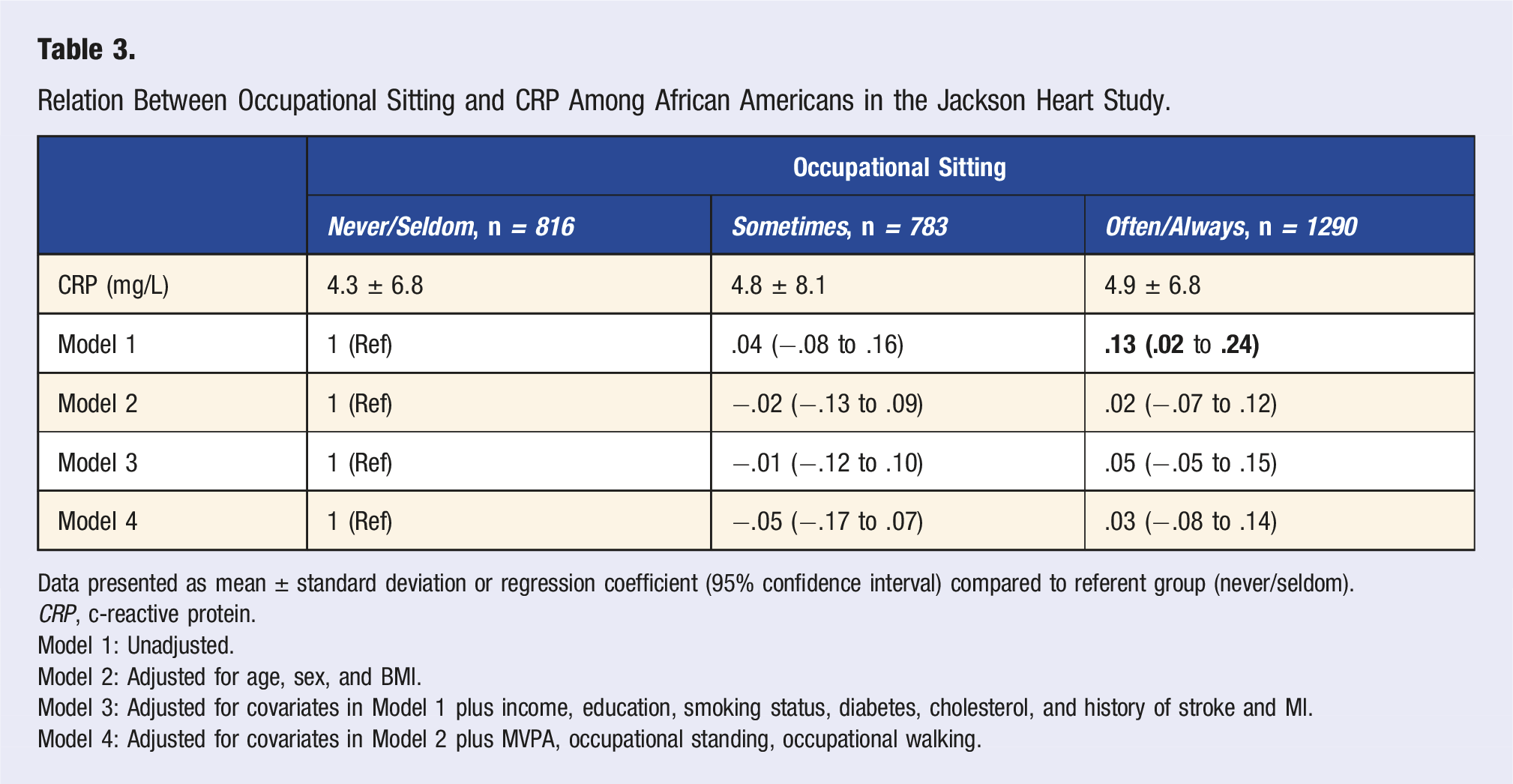
Data presented as mean ± standard deviation or regression coefficient (95% confidence interval) compared to referent group (never/seldom).
CRP, c-reactive protein.
Model 1: Unadjusted.
Model 2: Adjusted for age, sex, and BMI.
Model 3: Adjusted for covariates in Model 1 plus income, education, smoking status, diabetes, cholesterol, and history of stroke and MI.
Model 4: Adjusted for covariates in Model 2 plus MVPA, occupational standing, occupational walking.
Occupational Sitting and CRP by Sex
Relation Between Occupational Sitting and CRP In African Americans In the Jackson Heart Study Stratified By Sex.
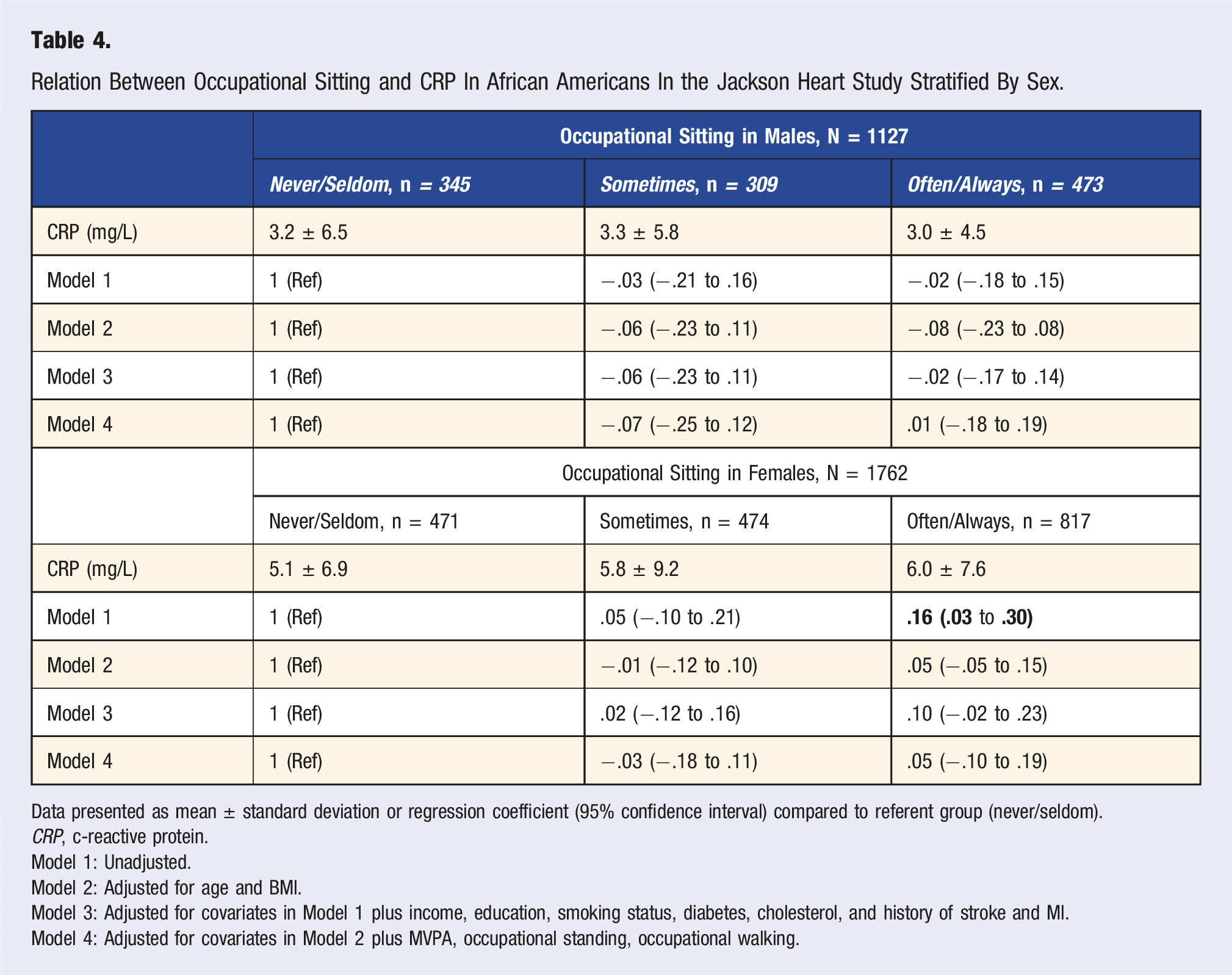
Data presented as mean ± standard deviation or regression coefficient (95% confidence interval) compared to referent group (never/seldom).
CRP, c-reactive protein.
Model 1: Unadjusted.
Model 2: Adjusted for age and BMI.
Model 3: Adjusted for covariates in Model 1 plus income, education, smoking status, diabetes, cholesterol, and history of stroke and MI.
Model 4: Adjusted for covariates in Model 2 plus MVPA, occupational standing, occupational walking.
Alternatively, female participants who reported “often/always” engaging in occupational sitting had CRP levels of 6.0 ± 7.6 mg/L, those who reported “sometimes” had levels of 5.8 ± 9.2 mg/L, and “never/seldom” had levels of 5.1 ± 6.9 mg/L. In the unadjusted model, female participants who reported “often/always” engaging in occupational sitting had significantly higher levels of CRP compared to the referent group of “never/seldom” (B = .16, P < .05, r2 = .003). This suggests that when compared to the referent group, “often/always” engaging in occupational sitting may result in a .16 mg/L increase in CRP, on average. The association did not remain statistically significant in the subsequent adjusted models (B = .05, P > .05, r2 = .24), with the fully adjusted Model 4 being the model of best fit. Significant predictors of CRP in females were: age (B = .001, SE = .003, P < .001), BMI (B = .07, SE = .004, P < .001), income (B = .20, SE = .09, P = .03), college education (B = −.22, SE = .11, P = .04), and occupational walking (B = −.18, SE = .09, P = .03).
Discussion
This study examined the association between occupational sitting and CRP in a community-based sample of African Americans in the Jackson Heart Study. Among study participants, individuals’ reporting “often/always” engaging in occupational sitting was not independently associated with CRP levels. Similarly, when stratified by sex, both males’ and females’ reporting “often/always” engaging in occupational sitting was not independently associated with CRP levels. The present study contributes to the growing body of literature on sedentary behavior and CRP18,29,32 and is from one of the largest cohort studies with data to examine potential links between occupational sitting and CRP. It highlights a critical need to further investigate the association of occupational sedentary behavior and the inflammatory process by exploring any potential variables that may be mediating this process.
The observation that CRP levels are positively associated with occupational sitting time prior to any adjustment suggests a potential influence between occupational sitting time and CRP without consideration of any potential covariate. In the unadjusted model, although not necessarily a clinically meaningful change, the data suggests that a .13 mg/L increase is expected for individuals going from engaging in “never/seldom” occupational sitting to “often/always.” However, with the addition of age, sex, and BMI in Model 1, the association between occupational sitting and CRP was no longer significant. This is in contrast to previous findings suggesting that sedentary behavior is independently associated with CRP.18,29,32 Gennuso et al 29 reported a positive independent association between sedentary time and CRP (P < .01). In the 1958 British Birth Cohort, researchers found that an increase in television viewing time, a proxy for sedentary behavior, was associated with higher levels of CRP. In the adjusted models of the study, CRP was higher by 22%, 16%, and 8% per category increase in television viewing. 18 Further analyses were run to determine the covariate(s) that may be contributing to the observed response in the present study. It was determined that the addition of BMI in the model attenuated the association between occupational sitting and CRP in the present study, which is consistent with previous literature. 33 Future research should consider longitudinally investigating BMI as it relates to occupational sitting and CRP to determine causality.
This study provides evidence that among African Americans the impact of occupational sitting may be more relevant for females who engage in more occupational sedentary activity, but was still not independent after controlling for BMI. Consistent with the present findings, results from the British Birth Cohort showed no association between occupational sitting and CRP in males and females. 18 In contrast to the present study, the ADDITION-Leicester study reported a positive association of overall sitting time with CRP levels in women (β = .17, P = .03). 41 Also, in contrast to the present JHS study, a negative association of overall sitting time with CRP levels was reported in men in the ADDITION-Leicester study (β = −.13, P = .04). 41 More research is needed to examining sex differences as they relate to sedentary behavior and inflammation.
In 2018, approximately 45% of African Americans were part of the blue-collar workforce in the United States. 42 Blue-collar workers tend to engage in less occupational sitting, and they tend to engage in other types of unhealthy behaviors (ie, poor sleep, poor diet, low job status, etc.). 20 In Mississippi, African Americans make up 37% of the workforce and are the most sedentary population in the state. 21 As such, the workplace is an important environment for examination of the daily activity profile. In this context, recent evidence has emerged to explain how the pathophysiology of occupational sedentary behaviors may impact public and population health.43,44 This evidence could, potentially, lead to recommendations for workplace health promotion techniques to reduce sitting time by implementing frequent breaks and active workstations to increase muscle activation and provide cardiovascular-related benefits. 45 Research on the influence of occupational sedentary behaviors on the inflammatory process is in its infancy, especially when examining African Americans. Thus, epidemiologic evidence is necessary to establish potential associations that could be further confirmed in laboratory-based studies. Such work would define potential links between sedentary behaviors and inflammatory biomarkers in African Americans.
Inflammation plays an important role in the progression of atherosclerosis, and CRP is the most widely studied inflammatory blood marker. 46 Increases in CRP levels to 3–10 mg/L have been associated with increased risk of stroke, coronary heart disease, and mortality. 47 However, previous reports suggest a beneficial effect of engaging in regular physical activity on the incidence of cardiovascular disease, and inflammation may be driven by pathways not typical of other cardiovascular disease risk factors. 48 The mechanisms through which sedentary behaviors are associated with inflammation remain unclear. However, sedentary behaviors, such as occupational sitting, are characterized by a lack of muscle contraction. A review by Pedersen and Febbraio 49 concluded that the lack of muscle contraction alters the myokine response in the skeletal muscle and contributes to the proinflammatory state of the muscle. Additionally, prolonged sitting has been associated with a greater expression of genes that may be related to an increase in the inflammatory response. 50
There are several strengths to our study. First, the JHS is a large community-based study conducted, solely, among African Americans. The sizable cohort of African Americans provided more power for detecting any robust associations of interest, which allows for an opportunity to better understand how occupational sitting among African Americans may warrant intervention. Second, CRP, the marker for inflammation, was measured in the study by trained individuals using a strict protocol for quality assurance (ie, measured in duplicate with intraindividual variations assessed).
Limitations of this study should also be noted. Occupational sitting was measured using a self-report, single-item question. However, the self-report nature of this question allows for information to be gathered in the specific occupational domain and the question on occupational sitting has been validated against accelerometry and activity logs. Second, additional measurements of other proinflammatory cytokines (interleukin-6 and tumor necrosis factor-α), which aid in regulating CRP, were unavailable during Exam 1 of the JHS. These measures could have provided a more comprehensive overview of the impact of occupational sedentary behaviors on the inflammatory response in African Americans. Third, the JHS is a single-site study in the southeast region of the United States; thus, the generalizability to other African American populations may be limited. Last, due to the cross-sectional nature of this study, inferences of causality cannot be made. Studies that use more sophisticated technologies (ie, accelerometry) to quantify sitting time, and robust methodologies (ie, full inflammatory profile), along with an exploration of job attributes, are needed to fully understand the impact of occupational sitting on the inflammatory response, as well as any differences across settings.
Conclusions
Among this sample of African Americans in the JHS, we found no independent association between occupational sitting and inflammation, measured by CRP. The findings of the current study add to the growing body of literature that previously reported variable associations between occupational sitting and CVD risk. After finding that sex was a significant predictor of CRP, we noted the association between occupational sitting and CRP varied by sex but did not remain independently significant after controlling for other variables. Use of self-report measures allowed for an exploration of the inflammatory response to occupational sitting. Few studies have sought to examine these associations in a strictly African American cohort while focusing on the effect that sex has on the inflammatory response to occupational sitting. Especially as computer-based work expands, future research is warranted to understand the impact of occupational sitting on CRP, as well as potential interactions with BMI, to aid in determining potential workplace interventions to reduce CVD risk among African Americans.
Footnotes
Acknowledgments
The authors also wish to thank the staffs and participants of the JHS. The views expressed in this manuscript are those of the authors and do not necessarily represent the views of the National Heart, Lung, and Blood Institute; the National Institutes of Health or the U.S. Department of Health and Human Services.
Author Contributions
Each author contributed substantially to study conception and design; analyzing and interpreting; drafting and revising the manuscript for content; and approving the final version for publication.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Jackson Heart Study (JHS) is supported and conducted in collaboration with Jackson State University (HHSN268201800013I), Tougaloo College (HHSN268201800014I), the Mississippi State Department of Health (HHSN268201800015I) and the University of Mississippi Medical Center (HHSN268201800010I, HHSN268201800011I, and HHSN268201800012I), contracts from the National Heart, Lung, and Blood Institute (NHLBI) and the National Institute on Minority Health and Health Disparities (NIMHD). Dr Raymond Jones is currently supported by National Center for Medical Rehabilitation Research (T32HD071886) and Dr Roland Thorpe, Jr is supported by the National Institute on Minority Health and Health Disparities (U54MD000214).