
Abstract
Background:
Musculoskeletal injuries from patient handling are significant problems among health care workers. In California, legislation requiring hospitals to implement safe patient handling (SPH) programs was enacted in 2011. This qualitative study explored workers’ experiences and perceptions about the law, their hospital’s SPH policies and programs, patient handling practices, and work environment.
Methods:
Three focus groups were conducted with 21 participants (19 nurses and 2 patient handling specialists) recruited from 12 hospitals located in the San Francisco Bay Area and San Joaquin Valley. Qualitative content analysis was used for data analysis.
Results:
Multiple themes emerged from diverse experiences and perceptions. Positive perceptions included empowerment to advocate for safety, increased awareness of SPH policies and programs, increased provision of patient handling equipment and training, increased lift use, and improvement in safety culture. Perceived concerns included continuing barriers to safe practices and lift use such as difficulty securing assistance, limited availability of lift teams, understaffing, limited nursing employee input in the safety committee, blaming of individuals for injury, increased workload, and continuing injury concerns. Participants indicated the need for effective training, sufficient staffing, and management support for injured workers.
Conclusions/Application to Practice:
This study identified improvements in hospitals’ SPH programs and practices since the passage of California’s SPH law, as well as continuing challenges and barriers to safe practices and injury prevention. The findings provide useful information to understanding the positive impacts of the SPH law but also notes the potential limitations of this legislation in the view of health care workers.
Introduction
Musculoskeletal injuries and disorders have been a major occupational health problem among nursing personnel (Davis & Kotowski, 2015). Patient handling, such as lifting, transferring, repositioning, and mobilizing patients, puts patient care workers at high risk for musculoskeletal injury (Gomaa et al., 2015; Lee et al., 2015; Menzel et al., 2004). According to the U.S. Bureau of Labor Statistics 2015 data, 10,290 registered nurses and 19,360 nursing assistants had work-related musculoskeletal disorders requiring days away from work, and the median lost worktime was 9 days for nurses and 6 days for nursing assistant (Bureau of Labor Statistics, 2016). In a 2011 American Nurses Association survey, 56% of nurses reported musculoskeletal pain in the past year caused or made worse by their job (LCWA Research Group, 2011).
In the United States, 11 states—California, Illinois, Maryland, Minnesota, Missouri, New Jersey, New York, Ohio, Rhode Island, Texas, and Washington—have enacted legislation on safe patient handling (SPH) to prevent patient handling injuries among health care workers (Weinmeyer, 2016). California passed SPH legislation in 2011 that requires general acute care hospitals to establish SPH policies and programs to provide employee training, lift teams or trained staff to assist, and patient handling equipment to replace manual handling (California Department of Industrial Relations, 2017); the law took effect in January 2012. Subsequently, the California Division of Occupational Safety and Health (Cal/OSHA) developed its enforceable regulation §5120—Health Care Worker Back and Musculoskeletal Injury Prevention—which became effective in 2014. The regulation specifies that hospital plans should include procedures for identification, evaluation, and correction of patient handling hazards, investigation of patient handling injuries, communication with employees, and evaluation of the effectiveness of the plan (California Department of Industrial Relations, 2017).
A recent study assessed the impact of the California SPH legislation by comparing data from two surveys conducted in 2013 and 2016 involving California registered nurses (Lee et al., 2018). The study reported significant improvements in nurses’ awareness of their hospital’s policy on SPH, receipt of annual SPH training, and availability of lift equipment, along with significant reductions in the prevalence of work-related musculoskeletal symptoms. The study provided useful measures on the effect of the SPH law and related changes that have been made in California hospitals. However, the information was limited in fully capturing the impact and changes on work practices and perceptions, at the worker level, and identifying successes and challenges experienced by hospital workers. Therefore, we conducted a qualitative study to fill this gap. This study explored nurses’ and patient handling staff’s experiences and perceptions about the SPH law, changes in their hospital’s policies and programs, patient handling practices and work environment, since the passage of California’s SPH law.
Methods
Design and Sample
This was a qualitative study using focus groups with a purposive sample of nurses and patient handling staff employed in acute care hospitals. Nurses have the primary responsibility for patient care and handling activities of assigned patients. In hospitals with lift teams, the staff dedicated to patient handling tasks are mobilized to perform patient handling tasks when needed. We aimed to recruit participants from a diverse sample of hospitals to understand experiences and perceptions of workers employed in different hospital settings. Eligibility criteria included staff nurses or other hospital workers who (a) frequently performed patient handling duties and (b) were employed for at least 5 years in an acute care hospital. We used email advertisements, on-site flyers, and word-of-mouth via networks of unions (i.e., California Nurses Association and Service Employees International Union), a nursing professional association (i.e., a local chapter of occupational health nurses association), nursing schools (San Francisco, East Bay), a training event, and a personal network. An online study registration site was created using Qualtrics software (Qualtrics, Provo, UT). Initially, 46 hospital workers from more than 22 hospitals signed up for the study and provided their demographic information and hospital names. In the screening and scheduling processes, 25 people did not respond to our calls or were not able to participate due to schedule conflicts or other reasons. The study was approved by the Institutional Review Board at the University of California, San Francisco.
Data Collection and Procedure
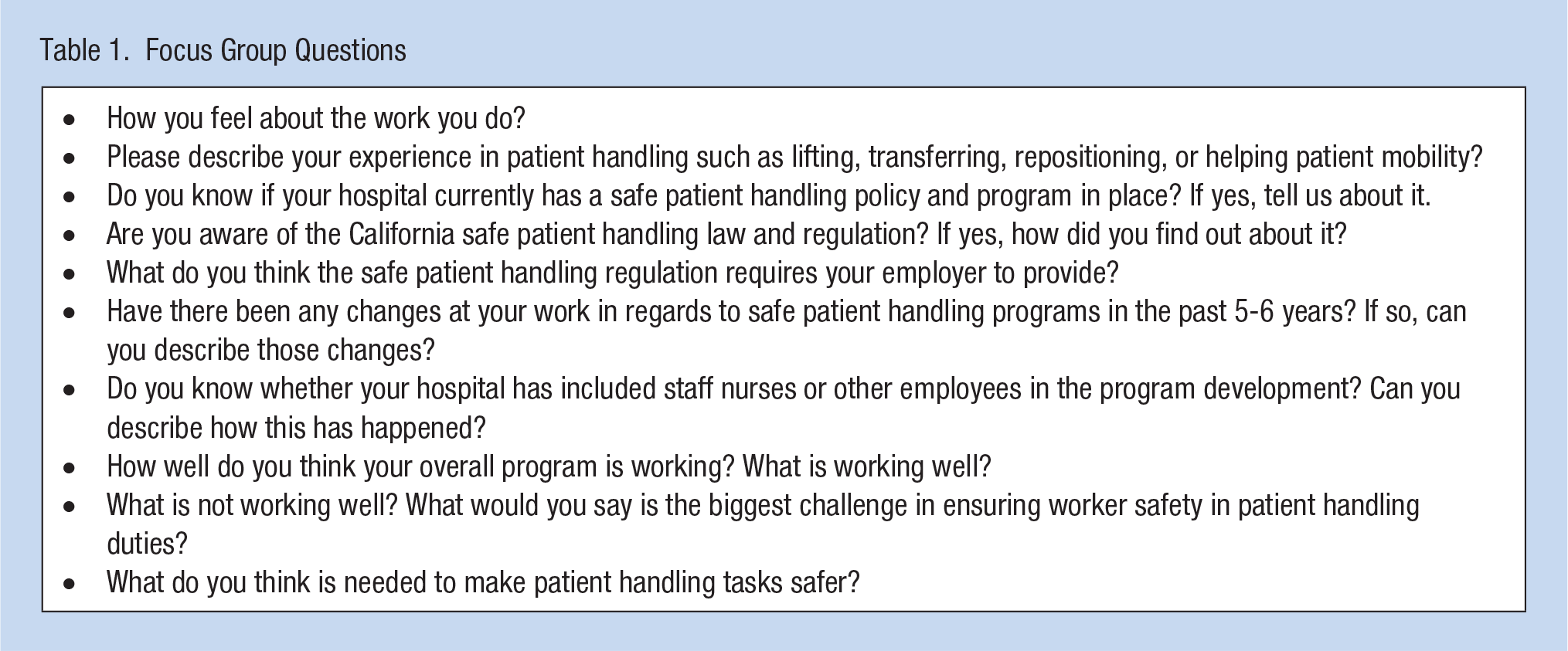
The focus group script with questions and probes was developed with inputs from two nurse union representatives and one occupational health professional. The focus group questions are provided in Table 1. Three focus groups consisting of six to eight participants were conducted between November and December 2017. Written informed consent was obtained at the beginning of the focus group session. Focus group sessions led by an expert facilitator were digitally recorded and lasted approximately 2 hours. Focus groups began with introductions, ground rules, and an icebreaker activity of selecting a picture that best represented their work and talking about the feelings the picture evoked. At the end of the session, study participants received a $75 gift card as a reward for their participation. For participants’ hospital ownership and size information, we referred to the health care facility listing information from the Office of Statewide Health Planning and Development (OSHPD) (https://data.chhs.ca.gov/dataset/licensed-healthcare-facility-listing).
Focus Group Questions
Data Analysis
Focus group recordings were transcribed verbatim. Qualitative content analysis was used for data analysis using the Dedoose software program for data coding. Qualitative content analysis is “a research method for the subjective interpretation of the content of test data through the systematic classification process of coding and identifying themes or patterns” (Hsieh & Shannon, 2005). Three research team members independently reviewed the transcript of the first group and derived initial categories and codes from the text data. The categories and codes served as the coding scheme for the remaining data analysis. New codes were added as needed within categories in the coding process. The codes were grouped into the following nine categories: (a) knowledge and impact of the SPH law; (b) hospital policies, procedures, and employee involvement; (c) training; (d) patient handling equipment; (e) lift team; (f) staffing; (g) organizational climate and safety culture; (h) workload; and (i) injury concerns. For validity, at least two research team members coded data for each transcript, and each member presented their analysis results with identified themes to the team. We organized themes by subcategories of positive experiences and perceived challenges or concerns within each category. In presenting the quotes, we only edited if necessary to increase readability and reduce length (e.g., correct grammatical errors or omit less relevant parts). Replaced or added words were indicated by brackets.
Results
Table 2 presents characteristics of 21 participants recruited from 12 different hospitals located in eight counties in the San Francisco Bay Area and San Joaquin Valley. The participants consisted of 19 staff nurses and two patient handling specialists on a lift team (one of the two was a former certified nursing assistant). The majority of participants were female (85.7%) and worked in medical-surgical units or intensive care units (61.9%) and nonprofit hospitals (90.5%). Eleven participants (52.4%) worked in large hospitals with more than 400 beds, and one participant worked in a small hospital less than 100 beds. Most participants (81.0%) worked more than 5 years in their current hospitals. In discussing the impact of the SPH law, the focus group participants described both improvements and continuing issues over the past several years since the passage of the law. Participants expressed contradictory experiences in some areas. The participants’ perceptions and experiences are described by content category with positive experiences and perceived concerns.
Demographics of Focus Group Participants
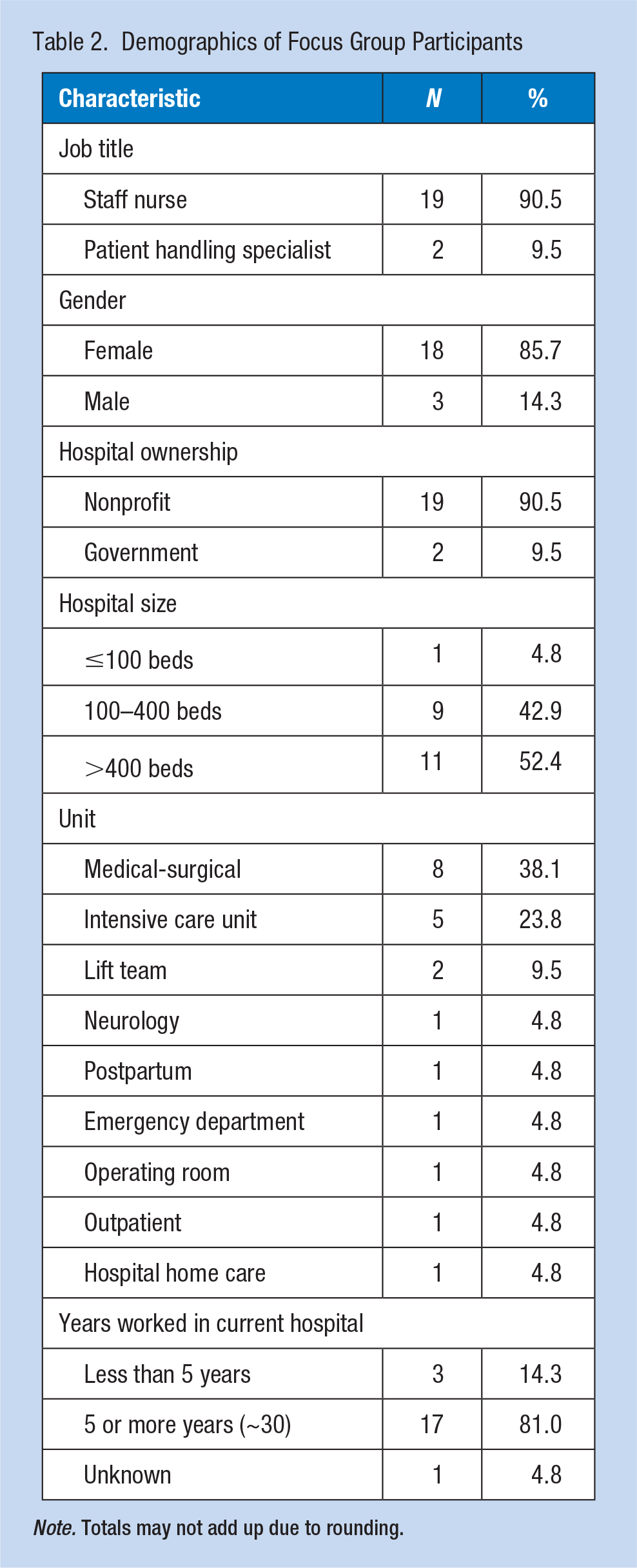
Note. Totals may not add up due to rounding.
Knowledge and Impact of the SPH Law
Two thirds of participants indicated some level of awareness of the SPH law, such as “I don’t know the particulars of the law, but I know they require annual competency training.” Unions were identified as a key source of knowledge and education on the SPH law and regulation, with one nurse indicating “I didn’t know about that it became a law . . . but I know that the union passed [out] a lot of information about it.” Sixteen participants reported benefits of the SPH law such as increased equipment availability or increased training because of the law. One nurse stated “[Legislation] has been the only reason they have improved. Had legislation and regulation never been put into place we wouldn’t have what we have now.” Some participants indicated that the law empowered them to advocate for what they needed: Nurses pay more attention to safety . . . They may not understand the whole law, but the knowledge that there are rules . . . has really helped. Nurses now feel like they can say, “I know there’s a law about this somewhere,” or “I heard that there are regulations that we’re not supposed to have to do that.” So that has empowered a lot of nurses.
Perceived challenges were also identified. Some participants reported that they were unaware of the SPH law and several participants indicated that the SPH law was not protective enough in practice, and there was a general lack of change or improvement. Participants commented “ With the law, there was absolutely no change in the staffing . . . just acknowledging the law, but doing nothing . . .,” and “ What I’ve actually seen in real life is that the hospital industry . . . spends much of their time, energy, and resources, finding ways to work around it.” One nurse indicated: [It] looks pretty on paper. The policy is all nicely updated. There [are] nice handouts . . . required on-screen computer video we do every year and there’s maybe more equipment. There’s definitely more education . . . but not more support to get the job done.
Hospital Policies, Procedures, and Employee Involvement
The majority of participants expressed some level of awareness of a policy on SPH in their hospital, such as “There is a safe patient handling policy. During my orientation, they showed me where I can find it online . . . If there is any question, I can search [for] a document.” Most participants indicated that the policy focused on the use of lift equipment.
I attended a task group last year . . . comparing what the law is to what our policy is . . . When you peel back all the layers, the policy is you have to use lift equipment.
One participant commented on assessment algorithms and the right to refuse unsafe patient handling: Algorithms. That’s one of the big words in our policy . . . you can read the policy about how [and when] to use equipment and the algorithms will tell you how many people you need. You can say no. If you see you’re in an unsafe situation, you can refuse to do [the lift] without being punished.
Almost half of the participants were aware that there were safety committees discussing patient handling, such as “There is a safety committee, so there is a discussion every Wednesday. They are focused on patient safety as well as employee safety . . . handling of our equipment.” One participant mentioned multidisciplinary participation on the committees: “Safe patient handling committee . . . co-chaired by a member of management and a member of labor . . . There is involvement of a different bunch of disciplines: PT, nursing, lift team.” Communication on employee injuries was also noted. “[A weekly injury] report goes out to Region . . . and it tells how somebody got hurt, and what they could’ve done different to prevent it.”
Many participants described challenges associated with hospital policies and committees. Some participants expressed the perceived lack of usefulness of the policy, such as “The one thing that really stuck out in my mind when I read the policy is . . . if a nurse is injured moving a patient, then [the nurse is] subject to discipline.” Participants also indicated limited employee involvement or nursing representation in the SPH committee. One nurse said “We have a really big committee that’s corporate-wide, but it hasn’t trickled down to our hospital . . . They have definitely not involved employees in their policy at a local level.” Another nurse noted “We have safety committees now . . . primarily administration, management and non-nursing staff . . . [but] no input from the actual user, the nurses.” One participant also addressed the committee’s lack of authority to make changes: “It’s a powerless committee . . . They come up with little posters like it’s been X amount of days since we’ve had an injury. There is nothing that is constructive that comes out of those committees.”
Training
Almost half of the participants indicated that there was increased and more regular training. Participants reported that training focused on equipment use was provided in both in person and online using computer-based modules, and was offered at a variety of times, including orientation, annually, in-services, skills day, and when new equipment was introduced. One nurse said, “I got trained once, then annually, we do a module on the computer . . . and the annual skill check [using] the machines . . . they want to check the competency.”
Several participants indicated that the training received was insufficient or ineffective and also noted that the quality and depth of training varied by facility, department, and shift. Participants described: “That first year when [the law] came out, they had a very comprehensive training for all the inpatient departments. But since then, it just kind of petered out,” “When education rolls out something new, the day shift gets the product rep there . . . they have huddles . . . massive amount of education . . . And nights, you get a flyer . . . You get a picture,” and “[When] equipment was introduced [we] got initial training . . . then several months, a year later when the equipment finally showed up, there’s a long gap of time between receiving the knowledge and using it . . . There’s no re-education, no refreshers.” One nurse reported no receipt of training: [Some] departments haven’t had a training in three years. I had the director look me straight in the face and say, “We give you that training every year.” [But] I’ve not [received training in] 10 years. I think what makes me the most crazy about it is that the lift equipment isn’t the only thing we need . . . We need to be taught how to take care of ourselves. Even when you’re using the lift equipment, you can hurt your back.
Patient Handling Equipment
Many participants expressed both positive experiences and challenges regarding lifting equipment. Most participants reported increased availability of lift equipment but limited increase in the use of lift equipment, with continuing barriers. One nurse indicated “There’s more of a variety of equipment available . . . But I don’t necessarily think there’s been a huge increase [in] the use of equipment.” Another nurse stated “We have in-ceiling lifts now, which are great. But I feel people don’t use them because they’re slower and because they’re intimidated because they don’t feel they have enough competency or training on them.” Several participants mentioned certain types of equipment that are particularly helpful, such as “I think the thing that’s been the most beneficial is that now we all have a HoverMatt® (HoverTech International, Allentown, Pennsylvania, USA).”
Participants described challenges that they faced in using lift equipment. Most participants addressed that using equipment was time-consuming, such as It’s [an issue of] time and convenience . . . If we try to use it all day long, we wouldn’t be able to finish our assignments . . . it is a difference between 60 seconds and 15 minutes.
Barriers also included that equipment was often not readily available when needed, and there was insufficient staff available to use the equipment. One nurse stated “If the equipment is not nearby or there’s not someone that I can grab [to help me use it], then [I] maybe try to do it in a way that really I shouldn’t, or it doesn’t get done.” Another nurse noted “You need that second person . . . [Patient handling] is a process that takes time and resources. And you often don’t have either one of them.”
Inconvenience of using or storing equipment was also identified as barriers: “There’s not [enough] room to get a lift into most of our [small] rooms because our hospital is old. They do provide us with the equipment but it’s not practical to use it.” Some participants were concerned about quality of care or patient discomfort related to equipment and certain patient situations where equipment use is not appropriate, such as “I try to use [equipment], but patients don’t like it” and “The equipment is not always appropriate. You can’t use the equipment to get somebody out of the bathroom that’s fallen . . . Equipment’s not always the answer.” One nurse noted the lack of competence in using the equipment, such as “I mean there are so many little complications to using the equipment. It’s intimidating.”
Lift Team
Several participants indicated that they had, or used to have, lift teams in their hospital and described the benefits of having designated staff to assist with patient handling, even though access was difficult at times. “I can always depend on them . . . to know how to use the equipment quickly. They’ve been a good resource for us.” “[Lift team] It wasn’t 24/7, it wasn’t enough, but it was something . . . they were dedicated . . . and very skilled at what they did.” “At one time we had a very robust lift team . . . It was a huge benefit for us on night shift where we had less staff.”
Several participants described challenges associated with the limited availability of lift teams, such as “I never see them on the day shift. So I don’t know where they are, how many there are . . .” One patient handling specialist addressed inadequate staffing for the limited use of lift teams: I’m on the lift team . . . But we’re like this little island, and there’s about eight of us covering the whole hospital 24/7. And none of us get replaced if we’re either on vacation or call in sick. And now, we’re in a bigger building that has more territory to cover in a way. So I think we get less work because people figure it’s going to take us a half hour to get there, so they go ahead and wreck their backs on their own instead of letting us wreck ours for them.
Some participants described that lift teams in their facilities were eliminated and replaced by equipment. One nurse noted “On night shift . . . we [nurses] have no ancillary staff. We used to have lift teams to aid us with patient mobility, but the teams were removed completely about five years ago and replaced with equipment.” Another nurse described a buddy system where patient care staff would depend on each other for help with lifting, thereby taking staff away from their other patient care responsibilities: At the beginning of the shift, you are assigned a “buddy” nurse co-worker [based] on the proximity of your patient assignments. So when she needs help lifting, you go help, and vice versa. Without consideration for what your individual workload was, your availability [to help] . . ., that system failed us.
Staffing
One patient handling specialist indicated the importance of sufficient staffing for SPH: “Bariatrics is a team sport . . . you need a bunch of people. Even if you’ve got the sling . . . you’ve got to have one or two people [to manage] that whole thing.” However, understaffing was addressed as a critical issue and most participants described insufficient staffing and difficulty securing lift assistance from staff. One nurse stated “The most challenging thing was just getting a CNA to assist [me] if a nurse couldn’t help [me]. All of our CNAs were usually tied up . . . So, [securing] one was nearly next to impossible.” Another nurse stated: We are all chronically understaffed . . . The patients are sicker now than they ever have been in my 25 plus years of nursing . . . Without the additional staff to help with mobility, it impacts the total care that’s delivered to the patient. And it also impacts injuries to staff.
One nurse indicated understaffing of lift teams: [The Lift teams] have so much workload. So how can they really cover everybody? So I’m not calling the lift guy at all . . . I’d rather ask [a coworker] or try to [move the patient] by myself. What the hospital really needs is to hire more people, more nurses, more lift guys.
Some participant felt that the focus on increasing funding for equipment led to a reduction in funding allocated to staffing. One nurse described “We’ve gotten a little bit better with access to equipment. But then [hospital management] cut back staff more, and they’ve cut back employee health to the bare bones.” Many participants indicated that lift equipment would not replace the need for staff.
Organizational Climate and Safety Culture
Many participants described positive experiences and changes in safety culture, specifically an increased awareness of the importance of safe lifting on the part of staff and management, increased use of lifts, and increased appreciation of helping each other. One nurse noted “Another change is I think that we have a lot of training. That’s why if somebody fell on the floor and then somebody says, ‘Oh, let’s use the machine’. So a lot of change in our minds.” Another nurse described: [Knowing] that we’re supposed to be using equipment has at least raised our awareness and we’re much better with the teamwork. We’re much more conscientious about what we’re doing, taking care of ourselves and making sure we’re doing the right thing. I’m gonna have to say, “It’s time to get the lift equipment. I’m not going to [move] this patient unless I get it.”
About half of the participants expressed concerns about management and indicated that management did not prioritize worker safety and was punitive or “blaming of workers” for their injuries. Participants stated: “[If you get injured] the message from hospital management [feels] punitive and condescending. You wouldn’t have gotten hurt if you would have done it the right way. Hospital [management], in general, has gotten more punitive over the years.” “It’s a very hostile, punitive environment, that if you don’t use the equipment, you get hurt. We’re not going to pay for it.” “They [hospital management] don’t want to look at their own systems anymore . . . Now they look at the person and want to blame the person as a general rule.”
Workload
Many participants expressed perceived challenges with their workload and described fast-paced, demanding, or increased workload. One nurse described “I’ve been a nurse for 20 years, and I’m more and more frustrated every day at work because we’re expected to do more with less every day.” Another nurse noted “[My] med-surg unit is very fast-paced. There’s a lot of expectations. There’s not time allowed for things you do need to do like teaching and moving patients, so people have to move quickly.” Participants also indicated increased protocols, such as “They’ve added so [many] more protocols . . . If a patient got a hip or knee surgery, they have to stand up within eight hours of surgery. Those demands are added on the top of everything we have.” Some participants described changes in the patient population and nature of patient care, such as “I feel like patients [are] a lot heavier than before. [There are] more older patients. They have more mobilizing problem [to help].” Insufficient staffing and concerns about overtime was also addressed: I feel like [I have to decide whether] to wait for one hour to [get a lift] team delivered to my room, [or whether to wait] for the second person to come here. [That would] save my back [but can] end up [with] overtime. Then, I [would] get coached by my manager . . . So I would choose . . . just quick do this and get on with it rather than get in trouble.
Injury Concerns
Most participants expressed concerns regarding their safety and injuries, such as “We have a lot of people on modified [duty or] leave, and then I just recently had my own back injury.” Participants indicated that workload, inadequate staffing resulting in the lack of assistance with patient handling, and time pressures put nurses at risk of injuries. One nurse noted: A lot of times, you can’t really wait for help . . . So nurses, including myself . . . just end up doing the lifting [alone]. And that is dangerous [for me and] probably dangerous to the patient. Over time, I know that I’m probably [going to pay] for it.
Two participants speculated that more use or misuse of equipment might be contributing to changes in injury patterns.
There [are] more cervical and shoulder injuries now because [we] have to [use equipment] . . . Bringing the ceiling lift down and [handling] the equipment . . . it’s switching types of injuries, and I think that will become more apparent with time.
Several participants talked about their own or co-workers’ negative experiences with workers’ compensation. One nurse described: There’s a general understanding that [you] don’t get [adequate] medical care if [you’re] on Workers’ Comp . . . We have employees that have been injured . . . and tell us nightmare stories about not being able to get an MRI, and not being able to get a cortisone shot, and not being able to get anything but pain pills.
Discussion
This study conducted three focus groups and explored the impact of California’s SPH legislation by identifying workers’ perceptions and experiences of changes in hospitals’ SPH policies, programs, and patient handling practices. Common themes were identified across the three groups and no new themes emerged in the third group, indicating reaching saturation. Two thirds of participants were aware of the SPH law. Increased provision and use of lift equipment, increased training, improvement in safety culture, and feeling more empowered to advocate for changes were identified as benefits of the law. This study also identified perceived concerns and obstacles including continuing barriers to safe practices and lift use, insufficient staffing, limited availability of lift teams, limited input from nursing staff in the safety committee, increased workload, continuing concerns about injury risk, and punitive management attitude and blaming of individuals for injury. Participants also indicated the need for more effective training, more supportive environment for worker safety and health, and increased management support for injured workers.
Improvements in SPH policies and programs were expected from California hospitals that are required to comply with the legislative and regulatory mandates. As expected, our study participants reported increased provision of lift equipment and more frequent and regular training on SPH since the passage of the SPH law. A recent study of California nurses found statistically significant improvements in hospital SPH programs from 2013 to 2016 with some gaps; in 2016, 87% of hospital nurses with patient handling duties were aware of their hospital’s SPH policy, 66% reported having an SPH committee in their hospital, 80% had lift equipment on their units, and 73% received an SPH training in the previous year (Lee et al., 2018). This focus group study provides further evidence that additional changes may be necessary; for example, participants indicated the need for more nursing staff’s input in the safety committee and more effective training to ensure competency in operating lift equipment among staff across all shifts.
Even though increased provision of lift equipment was identified as a positive consequence of the law in this study and also in the California Nurse Safety Study (Lee et al., 2018), continuing barriers to safe work practices and lift equipment use were also identified as a common theme. Participants described obstacles such as insufficient staffing and difficulty in getting assistance, concern about the increased time needed when using lift equipment, the lack of immediate availability of equipment, lack of competence in using the equipment, concerns about quality of care or patient discomfort related to equipment, and patient situations where equipment use was inappropriate (e.g., dressing change). These barriers have been well identified in previous studies (Koppelaar et al., 2009; Schoenfisch et al., 2011). The California Nurse Safety Study (Lee et al., 2018) showed no significant change in the use of lift equipment between 2013 and 2016, and only 39% reported using lift equipment more frequently in 2016. Our study provides further evidence that providing lift equipment alone may not be the solution. There are continuing challenges in ensuring and increasing the regular use of lift equipment for patient handling in actual practices among nurses.
In this study, staffing and workload were most commonly mentioned as significant barriers to safe work practices, and insufficient staffing was reported by both nurses and patient handling specialists. The Cal/OSHA’s SPH regulation requires that hospital plans include “The procedures by which lift teams and/or other designated health care workers will be available to perform lifts and other patient handling tasks in each patient care unit at all times in accordance with the Safe Patient Handling Policy” (California Department of Industrial Relations, 2016). The SPH regulation also states An employee is not considered to be available if the employee’s other assignments prevent the person from participating in the patient handling tasks within the timeframe determined to be necessary by the person designated to observe and direct the patient lifts and mobilizations.
The gap between the mandates and the actual practice environment experienced by workers was identified in each of the three focus groups. Several participants described the need to be taken away from essential patient care duties to assist other staff with lifting, which is a practice prohibited by the SPH regulation. In addition to the impact on workers’ safety and quality of work life matters, staffing is a well-identified important factor affecting patient care outcomes (Aiken et al., 2002; Stone et al., 2007). It should be noted that California is the only state that mandates minimum nurse-to-patient ratios for hospitals at all times by unit (e.g., 1:1 ratio for trauma units, 1:2 for critical care or intensive care units, or 1:5 for medical/surgical units) (American Nurses Association, 2019).
This study also identified a decrease in the use of lift teams. Several participants noted a removal of lift teams in some hospitals. Participants described a number of practices used to replace lift teams including: (a) buddy systems in which co-workers are expected to provide assistance, (b) the introduction of lift coaches who provide staff training regarding safe lifting, and (c) the increased provision of lift equipment. However, none of the participants felt these systems would be as helpful or protective as having a lift team. California’s SPH law does not require a provision of a dedicated lift team in a hospital’s SPH plan. Thus, the provision is up to the hospital’s decision. Lift teams were viewed as “a huge benefit” but participants indicated that lift teams were often unavailable or required a long waiting time. In addition, in the literature, concerns of the shifting of injury risk from patient care workers to lift team members have been raised (Schoenfisch et al., 2011). Further research on the risk benefit analysis would help to determine the best practices with lift teams.
Our focus group study identified that the passage of the SPH law resulted in workers’ feeling more empowered to advocate for the safety changes they needed. Worker participation and empowerment is an important component of successful and effective workplace safety and health programs. Workplace safety and health programs should encourage workers to report safety and health concerns and “empower all workers to initiate or request a temporary suspension or shut down of any work activity or operation they believe to be unsafe” (Occupational Safety and Health Administration, 2016). Legislation can validate the importance of the safety measures needed and provide a secure foundation for such workers’ participation by ensuring that they can speak up without fear of retaliation. California’s SPH law clearly states that A health care worker who refuses to lift, reposition, or transfer a patient due to concerns about patient or worker safety or the lack of trained lift team personnel or equipment shall not, based upon the refusal, be the subject of disciplinary action by the hospital or any of its managers or employees. (California Department of Industrial Relations, 2017)
On the other hand, our study identified some participants’ perceptions of an increased incidence of managers’ blaming and disciplining workers for injuries suffered from patient handling, given the presence of lift equipment, without considering the systemic issues such as limited access, insufficient staffing, or insufficient training. The important role of organizational climate and management support for worker safety and health has been widely documented in the literature (Eskandari et al., 2017; Gershon et al., 2007; Lee & Lee, 2017; Zohar, 2010). Blame culture has been identified to have a negative impact on workers’ morale as well as on reporting of an injury (Brown et al., 2005; Eskandari et al., 2017). Our findings suggest a need for improvement in safety culture and a recognition of the broader systems impacting worker health and safety.
The provision of lift equipment as a requirement is a crucial measure to prevent a patient handling injury. However, in our study, two participants speculated that injury patterns might be changing due to more frequent use of lift equipment; for example, shoulder injuries from frequent maneuvering of ceiling lifts located above shoulders or injuries from contacting lift equipment. In the California nurse study (Lee et al., 2018), the prevalence of work-related symptoms showed significant reductions between 2013 and 2016 in the lower back, neck, and hands/wrists, but not in the shoulders; however, nurses with ceiling lifts had significantly lower prevalence of shoulder pain than nurses with floor lifts only (Lee & Rempel, 2020). Beneficial effects of lift equipment on reducing shoulder pain prevalence have been reported by previous studies (Lee et al., 2013; Li et al., 2004; Trinkoff et al., 2003; Yassi et al., 2001). Future research can further investigate injury patterns and provide more conclusive evidence on the questions raised from the field.
This study has limitations. The sample included no current nursing assistants who also perform patient handling tasks as main responsibilities; thus, their perspectives were not reflected in our findings. Our sample included participants from 12 different hospitals, but we had no participants from for-profit hospitals and had only one participant from a small hospital (<100 beds). Therefore, our findings may not well represent perspectives of workers in those types of hospitals and cannot be generalized to other hospitals. Moreover, we considered that participants’ comments reached saturation from the three groups of our study sample, but more groups may capture more diverse and detailed experiences among workers.
Implications for Occupational Health Practice
Occupational health laws and regulations endeavor to provide a fundamental and strong foundation for workplace health and safety programs to protect workers and for occupational health practices. Promulgation of new laws or regulations requires subsequent research effort to evaluate the impact. This study explored the impact of California’s SPH law and regulations from workers’ perspectives to understand how the workplace policies and programs for SPH and injury prevention have been implemented in California hospitals and how the hospital policies and programs affected workers’ practices. Although this study has limitations, our findings provide valuable information about nursing and patient handling staff’s perceptions of their hospital’s SPH programs and work environment and experiences in patient handling practices and highlight both positive changes as well as continuing challenges.
California’s SPH regulation requires hospitals to identify and evaluate patient handling hazards and to evaluate at least annually, use, availability, accessibility, and effectiveness of patient handling equipment and procedures (California Department of Industrial Relations, 2017). Hospitals are also required to investigate musculoskeletal injuries related to patient handling; review whether their SPH plan was effectively implemented, whether sufficient staff was available and used, and whether the employees involved had been trained as required; and solicit opinions from the injured employee and other staff involved in the incident regarding the cause of the incident and possible prevention measures. In these processes, occupational health nurses can play a pivotal role. The hospital plan should also include procedures for communications with employees regarding SPH matters and “the means by which employees may communicate without fear of reprisal their concerns regarding performing a patient handling activity” (California Department of Industrial Relations, 2017). In our study, some participants reported feeling empowered by the SPH law to speak up for their safety, but some other workers expressed concerns about management’s punitive attitude toward injured workers.
Our study findings provide useful information to understanding the positive impacts of the SPH law but also notes the potential limitations of this legislation in the view of health care workers. These findings can help hospital management, SPH program managers, and occupational health professionals understand nursing and patient handling staff’s experiences and perceptions, particularly about challenges and barriers to SPH practices, and identify areas where improvements are needed. Occupational health professionals can apply the information to address staff’s concerns and promote successful SPH programs for injury prevention.
Applying Research to Occupational Health Practice
This focus group study explored nurses’ and patient handling staff’s experiences and perceptions to understand the impact of California’s Safe Patient Handling (SPH) legislation from workers’ perspectives. Positive experiences and perceptions included feeling empowered to advocate for safety, increased awareness of SPH policies and committee activities, increased provision and variety of lift equipment, more provision of training, increased lift use, and improvement in safety culture. Perceived concerns and obstacles included continuing barriers to safe practices and lift use, limited availability of lift teams, insufficient staffing, limited nursing employee input in the safety committee, increased workload and continuing injury concerns, and more punitive management about worker injury. Participants also indicated the need for more effective training, a more supportive environment for worker safety and health, and increased management support for injured workers. These findings speak to the influence of a State law on SPH practices as perceived by direct care nurses from multiple unit and hospital types. The findings can help occupational health professionals identify factors that direct care nurses find most useful to encourage the full implementation of SPH programs.
Footnotes
Acknowledgements
The authors acknowledge the California Nurses Association and SEIU Nurses Alliance for assistance in the focus group script development and participant recruitment. We also acknowledge study participants for providing valuable information.
Author Contributions
S.J.L. conceptualized and designed the study, recruited participants, participated in the data analysis, and wrote the manuscript. L.S. developed the focus group script, solicited input from researchers and impacted unions, facilitated focus groups, conducted data analysis, and contributed to critical revision of the manuscript. V.M., K.A., and K.M. contributed to the data analysis and critical revision of the manuscript. All authors approved the final version to be published and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the U.S. Department of Labor, Labor Research and Evaluation Grant (grant no. EO-30270-17-60-5-6).
Institution and Ethics approval and informed consent
The study was approved by the Institutional Review Board at the University of California, San Francisco (UCSF), and was performed at UCSF. The informed consent was obtained from all participants.
Author Biographies
Soo-Jeong Lee, RN, PhD, FAAOHN is an associate professor at University of California, San Francisco, School of Nursing. Her research focuses on the health effects of occupational exposure and the prevention of occupational injuries and illnesses.
Laura Stock, MPH, is the Director of the Labor Occupational Health Program at the University of California at Berkeley. She has an MPH from UC Berkeley. She has extensive experience in conducting qualitative research on worker safety and health and developing training programs and policies to promote worker involvement in the development of effective intervention programs.
Victoria Michalchuk, MSN, RN is a doctoral candidate at the University of California San Francisco, School of Nursing.
Kelsie Adesoye, MPH, was a coordinator of Public Programs at the Labor Occupational Health Program at University of California at Berkeley, and she is now the manager of Preventive Health at the Stanford University Occupational Health Center. Her work focuses on occupational safety and the prevention of occupational injuries and illnesses.
Kathleen Mullen, RN, PhD, received her PhD from University of California San Francisco, School of Nursing and has held nursing faculty positions. Using qualitative research methods, her research has focused on understanding of work environments and injury experiences of hospital nurses. Currently, she works at Kaiser Permanente in San Rafael in California.