
Abstract
Musculoskeletal injuries, especially back injuries, are among the most frequent injuries sustained by direct caregivers who lift, transfer, and reposition patients. These injuries can be debilitating and, for some caregivers, career ending. In the first year following implementation of the safe patient handling program in a multihospital health care system, an 82% reduction in Occupational Health and Safety Administration (OSHA) recordable patient handling injuries was realized, a 94% decrease in days away from work, an 85% reduction in restricted duty days, and an 82% reduction in incurred workers’ compensation costs. These reductions have been sustained for an 8-year period since the program’s implementation in 2008. The primary focus of the program’s first year was training and education. Compliance and retraining efforts began in the second year, followed by a gradual transition to the present emphasis on sustainability. This article describes the development and implementation of a safe patient handling program in a multihospital health system and the impact on caregiver injuries over 8 years. Also presented are key strategies that were used to achieve sustainability.
Keywords
In 2006, more than half of all workplace injuries and illnesses among health care workers were attributed to overexertion. Most of the overexertion injuries were directly related to lifting and moving patients. In 2013, the U.S. Bureau of Labor Statistics (BLS) reported 66,910 cases of work-related musculoskeletal disorders (WMSD) in the health care and social assistance private sector. In almost half of those cases (32,950), a patient or resident of a health care facility was involved. Health care personnel accounted for 11% of all WMSD cases that resulted in at least one lost workday in 2013. Nursing assistants as a group experience the most WMSD cases involving a patient; registered nurses accounted for 20% of the cases (U.S. Department of Labor, BLS, 2014). Nursing is one of the top five occupations for sustaining work-related injuries (U.S. Department of Labor, BLS, 2014). For the past 7 years, nurses and nursing assistants have remained in the group of occupations that has sustained the highest number of WMSD injuries (U.S. Department of Labor, BLS, 2014).
Overexertion injuries are the most costly workers’ compensation (WC) claims in health care settings (Gallagher, 2013; Nelson, Fragala, & Menzel, 2003). Associated direct costs, which include dollars spent for health care, indemnity (lost wages), and, in some cases, legal expenses, can be significant for this category of injury. In addition to the direct costs of injuries, indirect or hidden costs may include overtime (i.e., staff working extra hours to cover the shifts of injured coworkers), lost productivity due to replacement staff performing injured worker’s duties, added costs of accommodating injured workers (e.g., allowing injured workers to work but scheduling extra staff to perform duties that are outside injured workers’ restrictions), training costs (i.e., training staff to cover the assignments of injured workers), costs of replacement staff, and the potential negative impact coworkers’ injuries can have on employee morale and absenteeism, affecting retention and turnover (de Castro, 2004). Indirect costs can be anywhere from 1.1 to 4.5 times actual direct costs (Association of Occupational Health Professionals [AOHP], 2014; www.osha.gov/Regio7/fallprotection/safetypays.html, 2016).
Strong evidence suggests that traditional approaches to patient handling (e.g., manual lifting and training in body mechanics) are not effective in eliminating caregiver injuries as a result of patient handling (Marras, Davis, Kirking, & Bertsche, 1999; Nelson & Baptiste, 2004; Waters, 2007). Research has shown (Table 1) that by introducing a safe patient handling (SPH) program, a health care organization can reduce the number and severity of injuries to caregivers, decrease lost time and restricted duty days, and realize significant savings in WC costs (Aslam, Davis, Feldman, & Martin, 2015; Cadmus, Brigley, & Pearson, 2011; Fujishiro et al., 2005; Garg & Kapellusch, 2012; Hinton, 2010; Knoblauch & Bethel, 2010; Missar, Metcalfe, & Gilmore, 2012; Schoenfisch, Lipscomb, Pompeii, Myers, & Dememt, 2013) Several studies have also shown a significant difference in caregiver perceived exertion and patient comfort when using SPH equipment to move and transfer patients (Fragala & Fragala, 2014; Garg & Kapellusch, 2012; Knoblauch & Bethel, 2010; Silverwood & Haddock, 2006).
SPH Program Literature Review
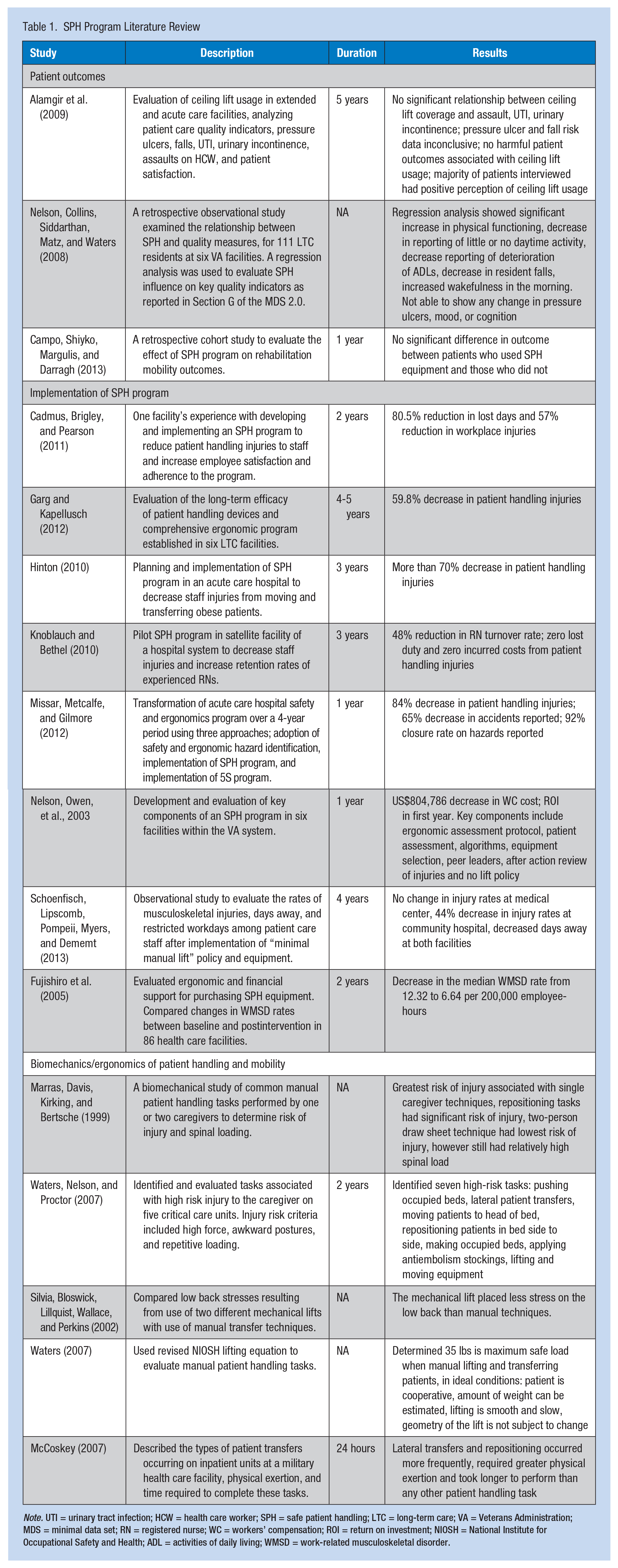
Note. UTI = urinary tract infection; HCW = health care worker; SPH = safe patient handling; LTC = long-term care; VA = Veterans Administration; MDS = minimal data set; RN = registered nurse; WC = workers’ compensation; ROI = return on investment; NIOSH = National Institute for Occupational Safety and Health; ADL = activities of daily living; WMSD = work-related musculoskeletal disorder.
In addition, investing in protecting the health and safety of nurses in turn contributes to protecting patients (American Nurses Association, 2004; Charney & Schrimer, 2007). Patients should feel safe and secure when lifted, moved, or repositioned and their dignity must be preserved in the process. Research has shown that the use of SPH equipment contributes to positive patient outcomes, encourages safe early ambulation, and decreases falls and skin breakdown (Alamgir et al., 2009; Flanders, Harrington, & Fowler, 2009; Knoblauch & Bethel, 2010; Nelson, Collins, Siddarthan, Matz, & Waters, 2008).
However, purchasing equipment alone does not guarantee a successful program (Nelson, Fragala, & Menzel, 2003). A culture of safety includes the collective attitude of stakeholders at all levels, taking responsibility for safety in the work environment (Nelson & Baptiste, 2004). However, once the culture change is underway, how can various stakeholders ensure the change will continue and caregivers will not revert to their previous habits of manually moving patients? Success requires a fundamental change in mind-set, with regard to how nurses move patients (de Castro, 2004; Gallagher, 2013; Nelson, Fragala, & Menzel, 2003). Therefore, the challenge is to gain support from all stakeholders, who must believe using equipment is not only safer for nurses but also safer for patients. A sustainable culture requires the continual presence of all or most program activities throughout the organization (Virani, Lemieux-Charles, Davis, & Berta, 2009). Program components must become routine within the organization for the program to endure (Pluye, Potvin, Denis, & Pelletier, 2004).
Garg and Kapellusch (2012) examined the results of SPH programs in long-term care (LTC) facilities up to 60 months postintervention, and found a 58% reduction in injuries, 86% reduction in lost time, and 90% reduction in WC costs associated with these injuries. Schoenfisch et al. (2013) found varied outcomes in injury rates at 4 years postimplementation. As of 2016, few studies had been published that examined the results of SPH programs in acute care environments beyond the initial postimplementation period (Table 1). Therefore, without a culture change and continual monitoring of SPH programs, initial results may not be sustained.
Method
An SPH program, TLC: Transfer and Lift With Care, was implemented in a multihospital health care system in northeast Florida in 2006. The health system is comprised of five hospitals, including a pediatric hospital, with a total of 1,052 beds. In addition, the health system also has an extensive primary care network and several specialty group practices. Presently, the system employs more than 10,000 team members. Since 2007, the health system has held Magnet designation.
In 2006, a multidisciplinary core group in the health system began to explore possible solutions to an alarming 82% increase in the total number of Occupational Health and Safety Administration (OSHA) recordable patient handling injuries over a 4-year period (Figure 1). In addition to the sharp increase in the number of injuries, the impact of patient handling injuries on caregivers was significant. Some caregivers were reluctant to return to the bedside for “fear of re-injury.” Several caregivers sustained injuries which resulted in permanent restrictions, thus affecting their ability to remain at the bedside.
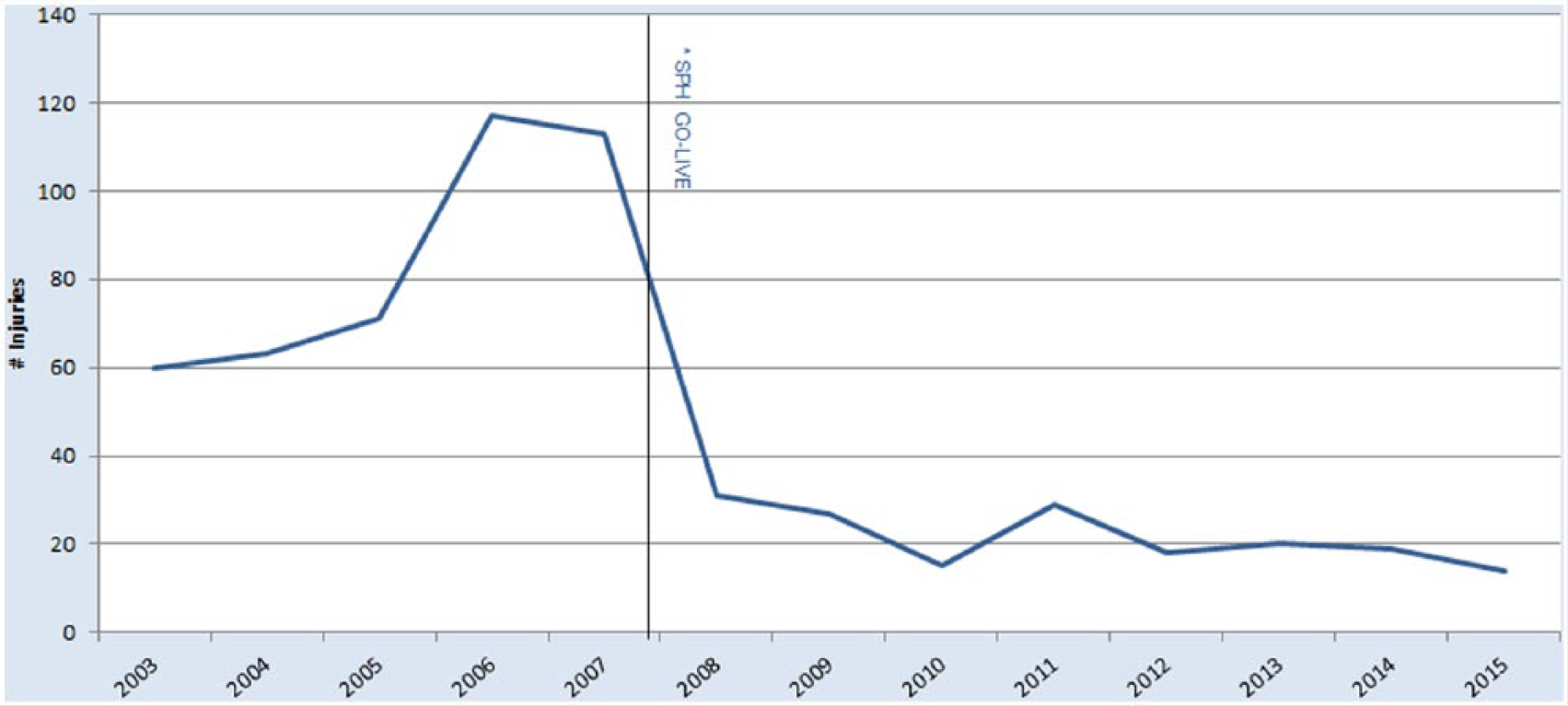
Number of OSHA-recordable patient handling injuries pre–post implementation of SPH program.
Concurrently, workforce development, led by human resources and executive leadership, was investigating issues affecting recruitment and retention of experienced caregivers at the bedside. Focus groups were held with caregivers to solicit their opinions on a variety of issues. Several themes emerged from the focus groups including concerns about the physical demands of manually lifting and moving patients, injuries to coworkers, the impact of injuries on their units, the increasing size of patients and challenges associated with moving these patients safely, and lastly, how long they, as experienced caregivers, could practice at the bedside due to these issues.
A continuing increase in patient handling injuries and feedback from the caregiver focus groups regarding concerns about both their safety and patient safety were the catalysts for considering an SPH program. A critical component of this effort was accurate data analysis of caregiver injuries from patient handling. The data selected for analysis were OSHA-recordable patient handling injuries that served as the baseline for ongoing analyses and outcome measurements. The analyses conducted for each patient handling injury used the same criteria for consistency and validity of data, which would be used for future analyses of these types of injuries. Components of the analyses included identification of the root causes of each injury, contributing factors, and whether the injury could have been prevented by using patient handling equipment. Severity of these injuries (i.e., number of lost workdays and/or restricted duty days) was tracked via the OSHA log. Workers’ compensation claims data and loss runs for each of these injuries were used for cost analysis.
The patient handling injury data analysis was required to objectively substantiate the need for an SPH program and secure leadership support. A critical role in securing executive leadership support for a culture of safety was the senior vice president of human resources who championed the program system-wide (Figure 2).
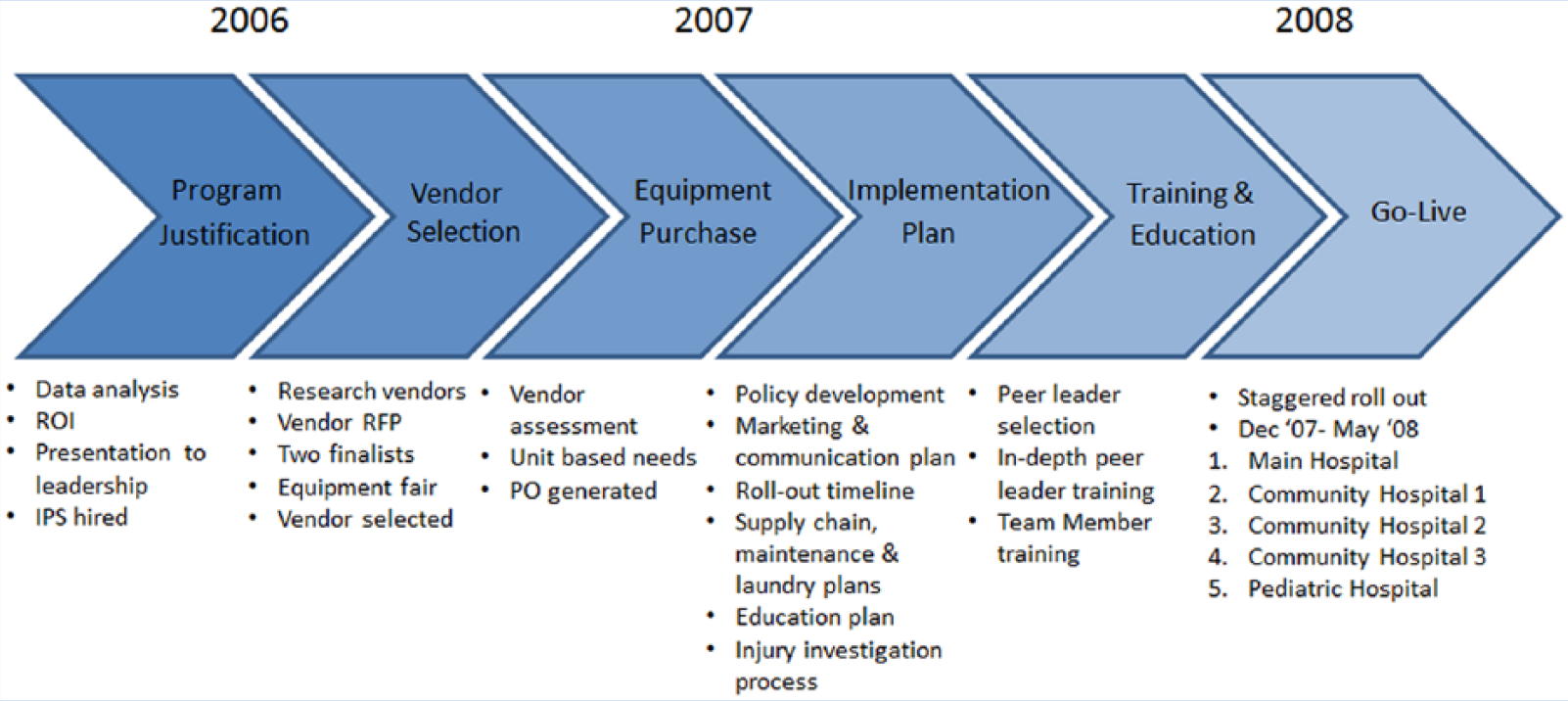
SPH program implementation timeline.
An interdisciplinary group of interested stakeholders was recruited to develop a proposal for the SPH program, which would change the culture of how caregivers safely lift and move patients, thus reducing patient handling injuries and WC costs and promoting patient safety. The team was comprised of an occupational health nurse, staff nurses, nurse leaders, and representatives from rehabilitation, infection control, environmental services, materials management, risk management, finance, and administration. The team also addressed the patient handling needs of an increasing bariatric patient population and specialty areas (e.g., endoscopy, surgery, and rehabilitative services).
Due to the size of the health system and the complexity of the initiative, an injury prevention specialist (IPS) role was developed, approved, and recruited to assist with this effort (Figure 3.) This individual’s primary responsibility was to coordinate the SPH effort from program development to implementation. The IPS eventually focused on other injury prevention efforts in the health system while still maintaining oversight of the SPH.
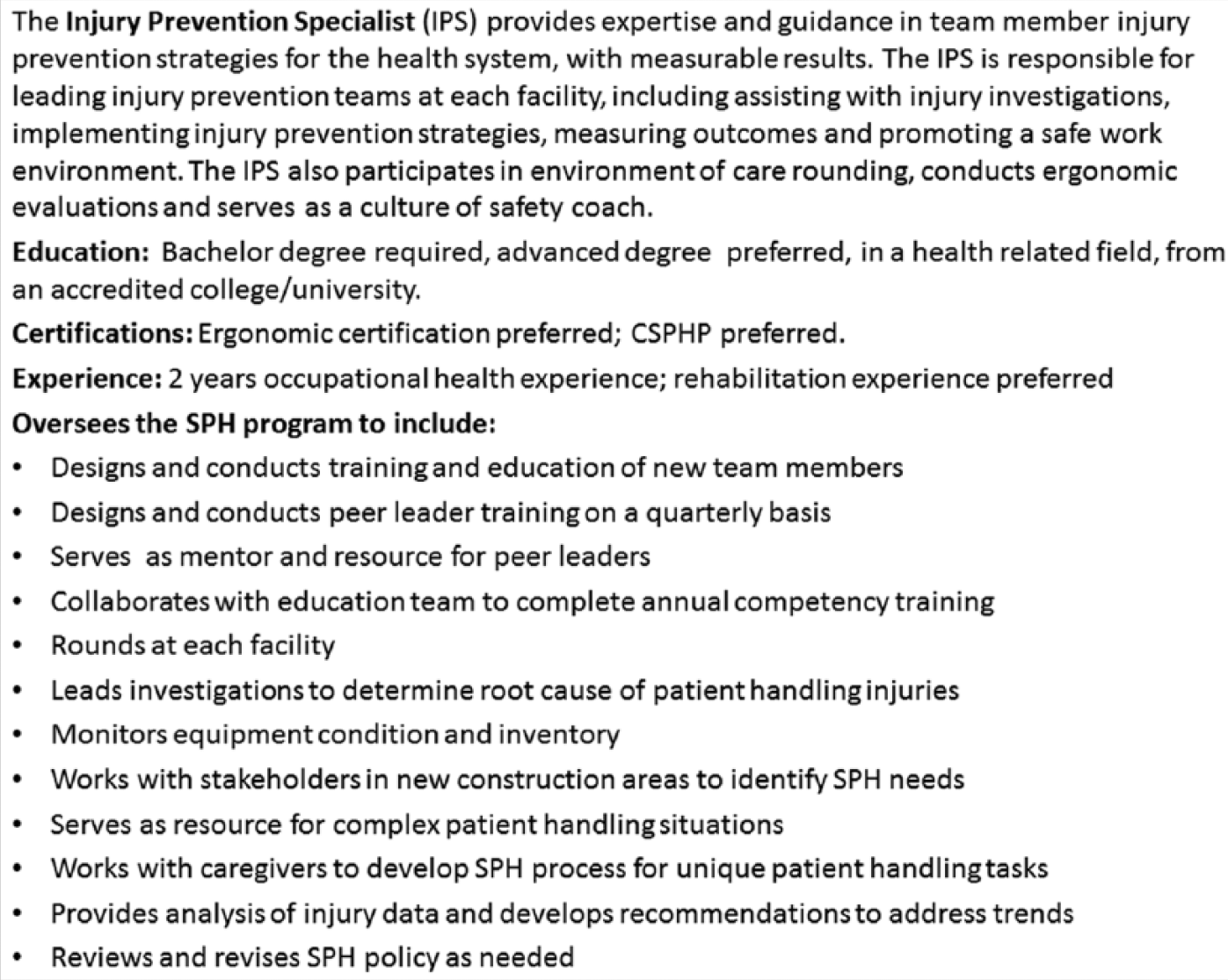
Injury prevention specialist job description.
A literature search on SPH programs was conducted to identify organizations that had successfully implemented SPH programs and how they achieved success. The team chose to use the Patient Care Ergonomic Resource Guide: Safe Patient Handling and Movement, based on best practices and program elements tested by the Veterans Health Administration (VHA; Nelson, 2001).
The team completed a worksite analysis to identify departmental needs for SPH equipment. Taken into consideration were the following components: type of patient population in each department, requirements for lifting and repositioning, and needs of specialty areas. An inventory of current lift equipment, equipment condition, and equipment utilization by staff was also documented. Staff input was essential to gain insight into issues that could interfere with proper use of available equipment (AOHP, 2014). Staff identified several barriers to equipment use. Frequently, equipment was inaccessible or parts were missing, and caregivers reported the equipment was not easy to use and, therefore, posed a safety hazard to both patients and staff.
The equipment and patient handling injury analyses were incorporated into a business plan predicting return on investment and included estimated equipment and training costs, and resulting potential injury reduction with projected cost savings. Cost projections were included to illustrate potential cost outcomes if patient handling injuries continued to increase without intervention. The final proposal was presented at a meeting of senior executive leadership and then submitted to the Board of Directors. The proposal was unanimously approved by the executive team and board.
Goals established for the first year were a 70% reduction in OSHA-recordable patient handling injuries, a 75% reduction in lost workdays, and a 75% reduction in restricted duty days from the previous year. A concomitant reduction in WC costs could be realized from the aforementioned goals.
In the next phase, system personnel identified a vendor who could assist with changing the long-standing safety culture and providing a broad range of equipment to meet the identified needs of the health system. A proven track record for the successful implementation of SPH programs in facilities of comparable size was a central consideration.
On-site equipment fairs from two vendor finalists were offered to obtain feedback from staff. Caregiver support, as stated previously, was essential to the success of the culture change (MacPhee, 2007). In December 2006, the team submitted a vendor recommendation based on a comprehensive review of vendor criteria, formal vendor presentations, and staff feedback.
Program Implementation
An interdisciplinary group from the health system worked with the vendor to complete the implementation plan. The first key aspect of the plan was a clinical policy that outlined the purpose of SPH; described how personnel were to move and transfer patients to protect both the employee and the patient; how, when, and where to document patient assessments and infection control issues; and how to address noncompliance. The policy also delineated exceptions to using equipment (e.g., when a caregiver is presented with a life-threatening patient situation). Addressed in the policy was the use of a patient assessment tool (Figure 4) to determine patients’ needs for equipment and how frequently to use the assessment tool (Nelson, Owen, et al., 2003).
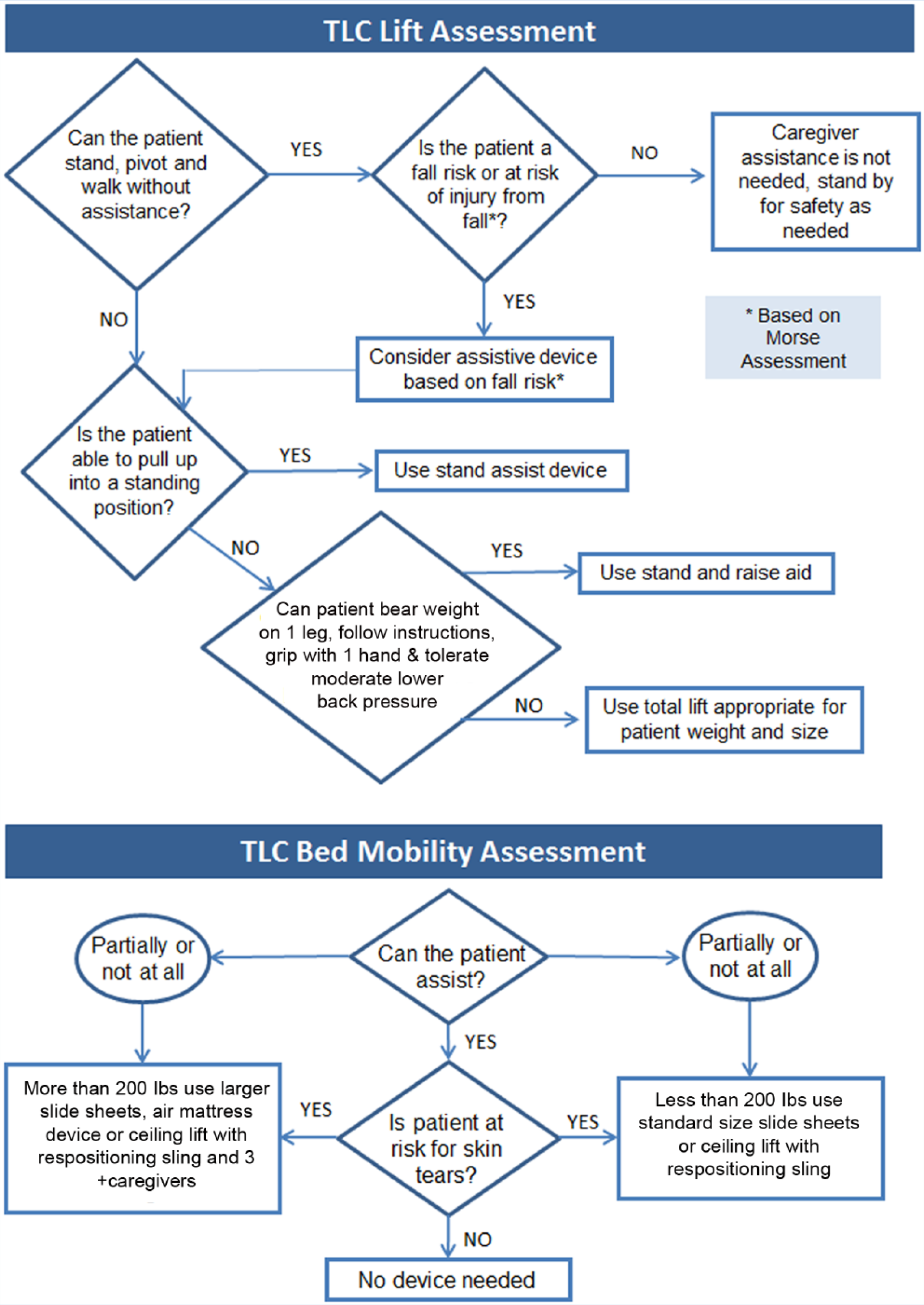
SPH patient assessment and electronic medical record documentation.
The education and training plan for the staff was formulated to include the policy, the assessment tool, use of equipment, and documentation. Department managers chose peer leaders from each unit to serve as experts for the department. They received extensive training to facilitate education in their departments. Peer leaders were key players in all aspects of program implementation and sustainability.
The implementation plan included the management of equipment and supplies as well as equipment maintenance and repair. The most challenging aspect of the implementation was the laundry process for reusable supplies. The manufacturer provided the specifications for laundering of reusable items to ensure proper cleaning and prevent damage. As a result, the third-party laundry vendor, who processes all soiled linen from the health system, developed a process to segregate these items from the regular linen and launder them separately. In turn, due to this process change, additional inventory of reusable supplies was needed to account for the time these items were in the laundry cycle and not available for use. Also, a greater potential for loss of these supplies was related to the items leaving the facility for off-site laundering.
The design of a consistent, nonpunitive process for investigation of patient handling injuries was another key component (American Nurses Association, 2013). All patient handling injuries are investigated to determine whether the resulting injury could have been prevented by using lift equipment. It was crucial to communicate to caregivers that the goal of the investigative process was not to assign blame, but to analyze the details of the situation surrounding the injury and determine what could have been done differently in that particular situation to prevent the occurrence (Table 2). Consistency in the investigative process to determine whether the injury met the criteria for a patient handling injury was essential for valid comparisons with patient handling injury results from previous years. Monthly reporting of injuries, review of patient handling injuries, and dissemination of injury data were reported to leadership and safety committees at each respective hospital site and trends were monitored.
Questions to Be Answered During Investigation Process
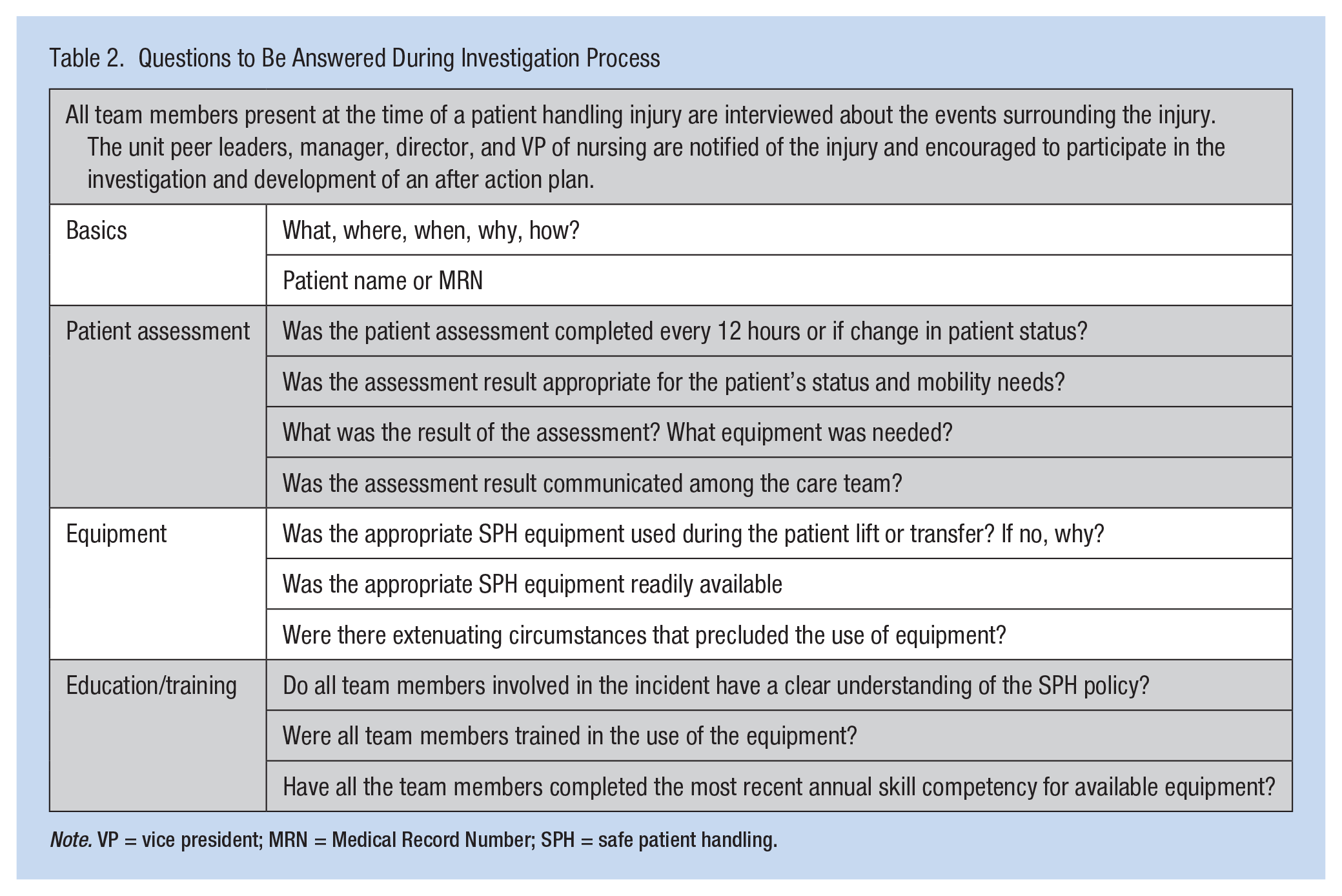
Note. VP = vice president; MRN = Medical Record Number; SPH = safe patient handling.
Marketing of the SPH program was another key aspect of successful implementation. The team worked with the public relations department to communicate, publicize, and promote the new program. A contest was held to name the SPH program. TLC: Transfer and Lift With Care was selected for the program name, abbreviated TLC, and a logo was developed. Resources for peer leaders and staff were identified and easily accessed on the facility’s intranet.
Ongoing communication about program results was shared with staff via internal communication publications, and at leadership and staff meetings. Managers supported, encouraged, and recognized department peer leaders. Certificates were awarded to newly trained peer leaders, and each hospital developed recognition programs for their peer leaders.
After initial training, the IPS introduced the SPH program during orientation of new employees, including more in-depth presentations to nurses, reviewing the SPH policy, expectations, and future training in the use of SPH equipment by their unit peer leaders. Employees are expected to demonstrate competency as part of orientation on their units.
Results
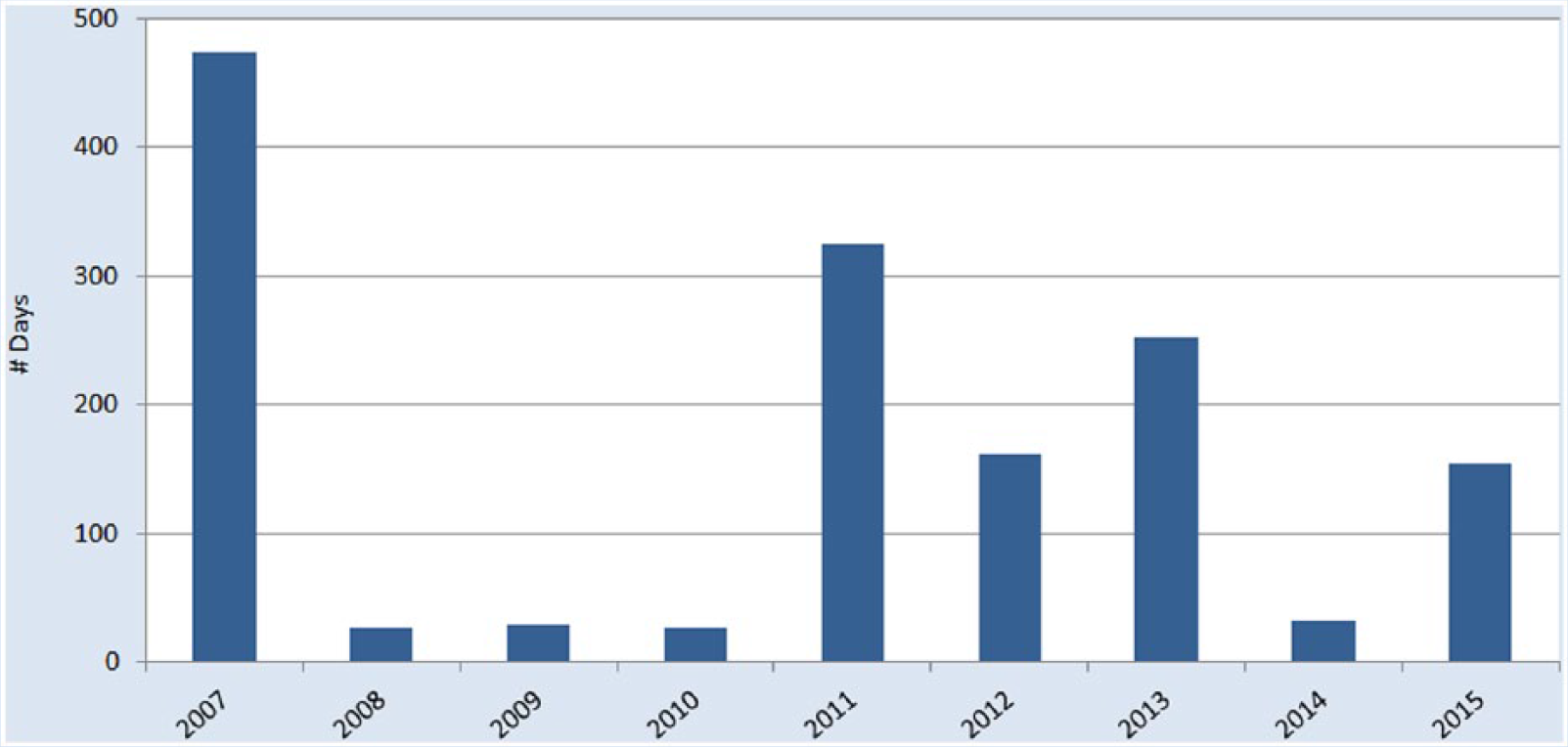
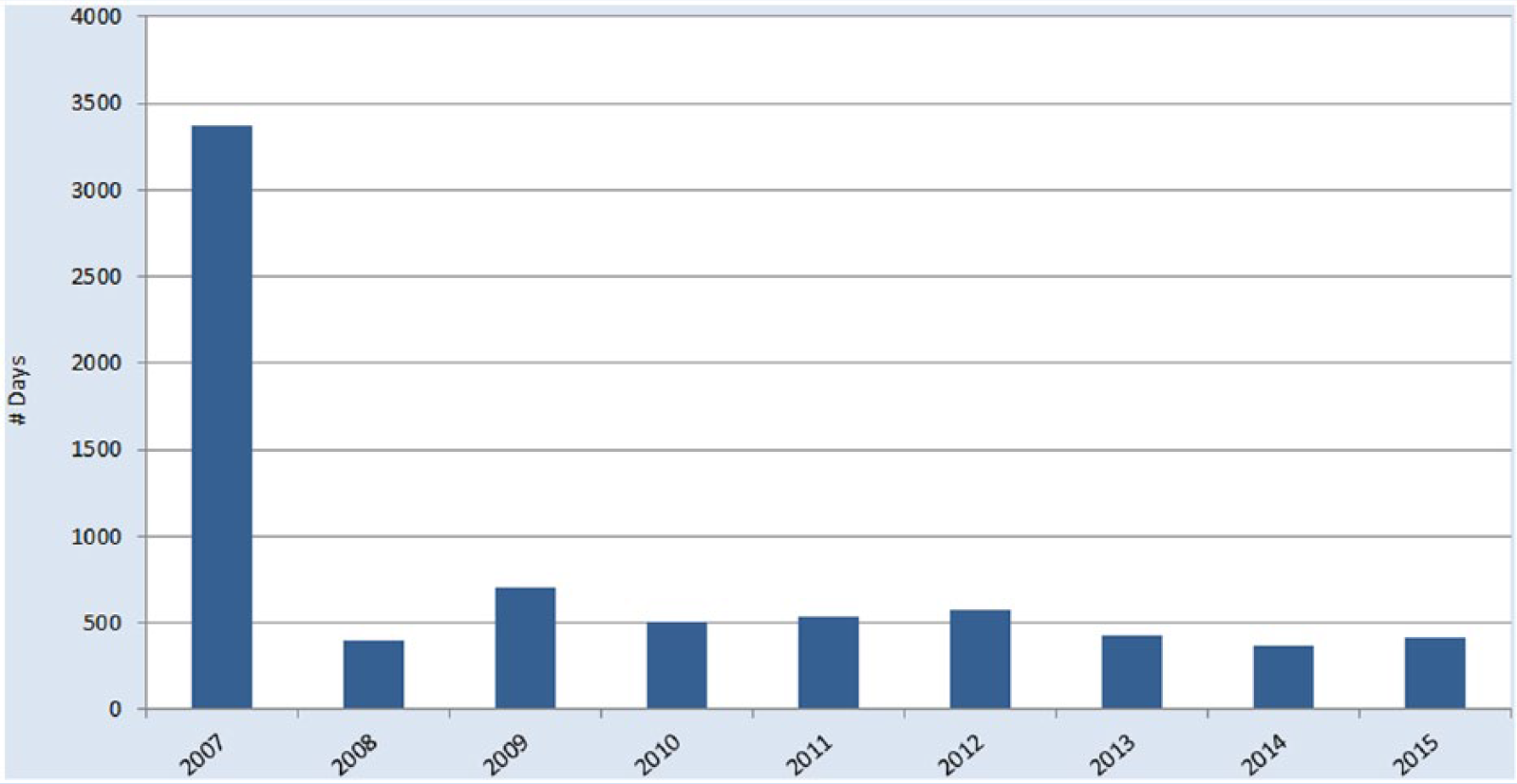
In the first year following implementation of the SPH program, an overall reduction of 82% in OSHA-recordable patient handling injuries, a 94% decrease in days away from work (Figure 5), 85% reduction in restricted duty days (Figure 6), and an 82% reduction in incurred WC costs (Figure 7) were realized. At the end of 2014, the total OSHA-recordable patient handling injuries for the health care system was 18, which resulted in 33 days away from work and 362 restricted duty days. Total incurred cost for WC was US$20,108. The results exceeded the established goals for the program.
Days away from work due to patient handling injuries.
Restricted duty days due to patient handling injuries.
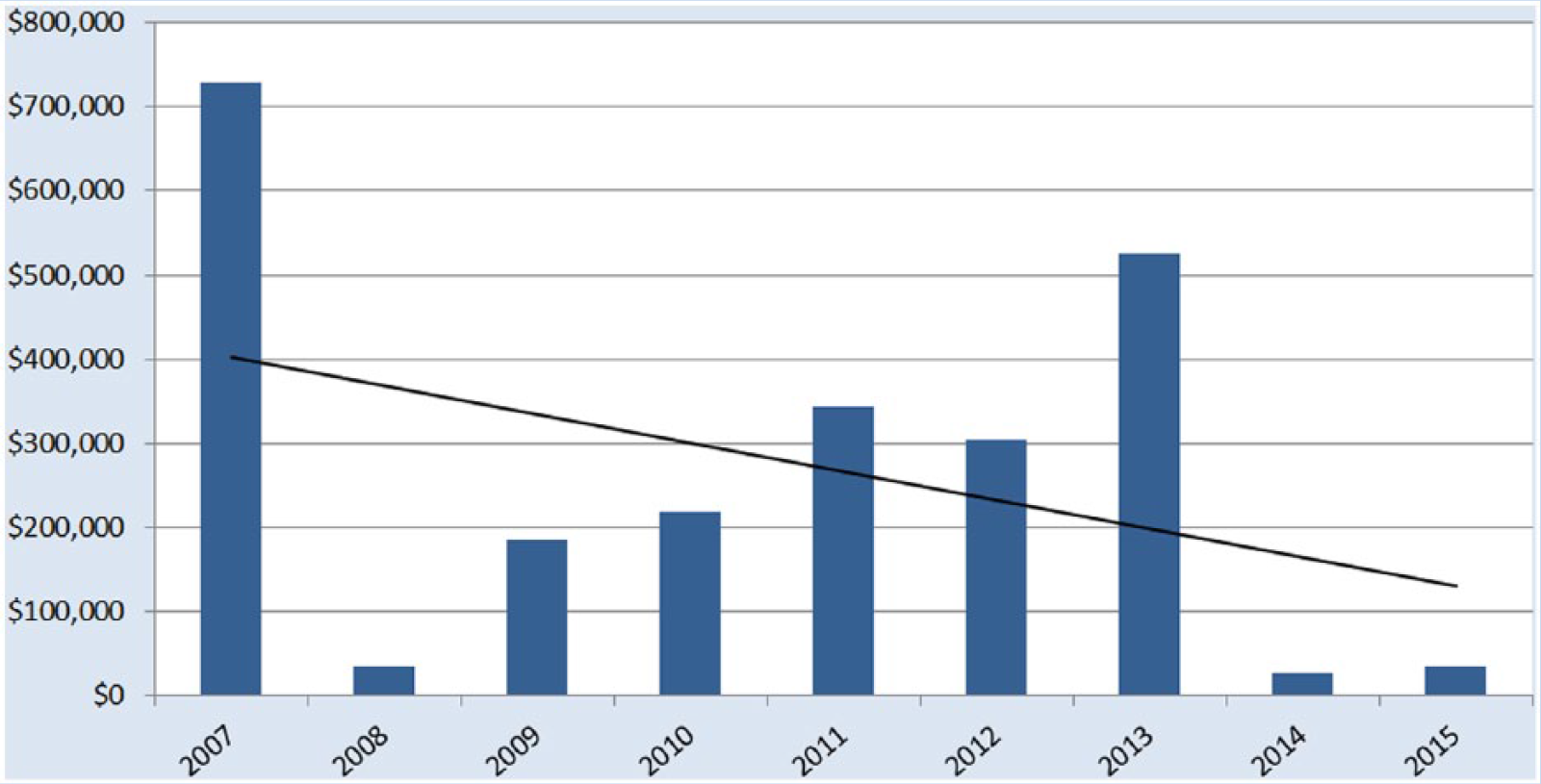
Incurred WC costs due to patient handling injuries, as of January 30, 2016.
Sustainability
It is difficult to change human behavior (AOHP, 2014); resistance to change is natural and, if key components of a program are not put into place, the culture will revert to old habits. Manual patient handling has been part of health care culture for generations (Virani et al., 2009). Therefore, SPH programs must change the organizational culture if these programs are to be successful. Change management professionals have identified key errors made during change initiatives that can cause programs to fail: not establishing an urgent need for the change, not creating a powerful coalition to guide the change, lacking a clear mission and not effectively communicating that mission, not removing obstacles, not planning for and celebrating short-term wins, declaring success too soon, and not incorporating the change into the organizational culture (Kotter, 1995; MacPhee, 2007). Many components of this SPH program, implemented both initially and over the past 8 years, have contributed to overcoming these common mistakes.
Urgent Need for Change
Identifying the trend of increasing patient handling injuries among staff in the years preceding program implementation demonstrated the urgent need for intervention. The patient handling injury data revealed several common circumstances leading to these injuries. Repositioning patients, assisting patients out of bed, relying on family members to assist with repositioning, unanticipated patient movement due to fear or discomfort, patient combativeness or resistance, and insufficient number of caregivers for the patients’ size were the major categories identified. During the year prior to implementation, four caregivers from one nursing unit sustained back injuries within days of each other due to the care required for a 656-pound patient.
In addition to presenting a logical case for change, the need for change must also appeal to human emotion. For example, WMSD affected caregivers’ ability to perform their jobs and dramatically changed the course of their lives outside of work. They experienced guilt and blame for their injuries, suffered chronic pain, and feared reinjury or permanent disability. Work-related musculoskeletal disorders can affect employees’ quality of life and force unwanted career changes (Nelson, Owen, et al., 2003). Some of the caregivers who sustained injuries during the study period could not return to bedside nursing and some left nursing due to permanent restrictions. Many injured caregivers who recovered from their injuries and were released to full duty voiced realistic concerns about potential future injuries.
Establishing a Guiding Coalition
The guiding coalition at this facility included senior leadership, midlevel leadership, direct caregivers from various professions, occupational health professionals, and the IPS. Leadership support is critical for program success. Leaders are not only essential in the initial adoption of programs, but true cultural transformation requires engaged leaders who learn and reaffirm expected safety behaviors (MacPhee, 2007). Specifically, nurse managers set the expectation that caregivers will appropriately assess patients, communicate the need for SPH equipment, and use the equipment appropriately. If the nurse manager is engaged in the process, caregivers will be engaged (Cadmus et al., 2011).
Direct caregiver support of the SPH program was achieved through participation in equipment selection, training, and peer leadership. Several peer leaders, called “TLC coaches,” were selected from each department and served as additional resources to program staff during initial implementation and beyond. Resistance to change was anticipated. Therefore, TLC coach training incorporated the concept of change management, resistance to change, and how to work with staff who were not in support of the program. Several TLC coaches accepted the role of site champion at each hospital location. In addition to acting as a TLC coach, they work closely with the IPS to investigate injuries and conduct regular rounds to solve problems unique to their facilities.
Finally, to endure sustainable change, it is important to have a system to track and report performance and a project manager to oversee the program (Agrawal, Berlin, Grote, & Scheidler, 2012). The IPS served a key role in both these functions. The IPS was instrumental in training staff to use the equipment and continuous training of TLC coaches. In addition, the IPS regularly conducted rounds in all departments participating in the program and reported the results of these rounds to leadership. The IPS monitored patient handling injuries and conducted in-depth investigations of all patient handling injuries with departmental leadership. The corrective actions resulting from these investigations were then shared across the health system to prevent similar injuries in the future. The IPS continues to serve in the role of consultant during sustainability of the program, continually monitoring program elements and looking for areas for improvement.
Communicate the Vision
By engaging direct caregivers and leadership throughout the planning process, the vision of preventing patient handling injuries was communicated across the organization. Initial training consisted of 1- to 2-hour sessions for all direct caregivers. In addition, TLC coaches completed an additional 6 hours of training. After the first year, the training focus shifted to sustainability. An annual competency program was established, which included a skill checklist for all equipment. In addition, a program was developed to ensure all new employees were aware of SPH policies and trained to use the equipment. The creation of a name and logo for the program aided in communicating the vision throughout the organization.
Empower Others to Act and Remove Obstacles
Again, by engaging caregivers in the selection and naming of the program, a sense of ownership was fostered. The TLC coaches and facility champions were given the tools and responsibility to act as liaisons between staff and leadership. This empowerment of peer leaders removed obstacles at the department level in a timely manner (Moore & Buchanan, 2013). If barriers were not addressed, especially prior to implementation of the program, employees would not have been fully engaged (Koppelaar, Knibbe, Miedema, & Burdorf, 2009). Wardell (2007) found that caregivers defer to patients’ needs without considering their own safety. Therefore, if any barriers to using the SPH equipment arise, staff will revert back to manual methods of moving patients (Rich, 2006). Finally, caregivers must be accountable for the appropriate use of SPH techniques, making it their responsibility to safely move patients (Wardell, 2007). However, caregivers are encouraged to seek assistance from peer leaders and the IPS when faced with complex or difficult patient handling situations.
Plan for and Create Short-Term Wins
At the conclusion of the first year of the program, the reduction in employee injuries was communicated throughout the health system. It was vital that not only leadership but also front line staff could celebrate that the 70% injury reduction goal was exceeded. The organization continues to set annual goals and communicate the results to staff. In addition, the system recognizes and rewards TLC coaches and facility champions for their roles in program success.
Continual Improvement to Support Change
Continuing to develop annual goals, offer ongoing training and education, and participate in regular rounds ensures sustainability by reminding workers about the vision. The objectives and content of annual competency and goal setting vary each year to address the issues identified in the previous year.
Injury investigations are valuable in identifying specific education needs. The investigations include identifying root cause, reviewing patient assessments, and verifying that caregivers have demonstrated competencies. Injury investigations have resulted in the development of new techniques to address unique patient handling tasks not covered by initial training. For example, in 2009, a nurse sustained a back injury in the process of positioning an orthopedic surgical patient. The injury resulted in 180 days of restricted duty, and a cost of more than US$125,000. As a result of the investigation, the nurse manager, surgical staff, orthopedic physician, and IPS developed a technique using SPH equipment to position patients for this type of surgery. This new technique has prevented further injuries related to this procedure.
Injury investigations paired with regular rounds have identified outcomes that can occur when using or failing to use appropriate equipment. Regular rounds include patient chart reviews, inspection of equipment, caregiver interviews, and observation of patient lifts and transfers in progress. Staff monitor equipment condition and recommend the purchase of new or replacement technology when appropriate. New technology has also been incorporated as the health system grows. The addition of ceiling lifts to new construction has made it easier and more convenient for caregivers to transfer patients.
Institutionalize Changes
Changes stick when they become “the way we do it here” (Pluye et al., 2004). The new behaviors must be rooted in the shared values of the organization (Kotter, 1995). The IPS has served on several committees (e.g., fall prevention, patient safety, facility coordination, and education) throughout the organization, which has served to align SPH goals with other organizational goals. The IPS, as the role of project manager, is also aware of potential areas to expand the program as the organization grows. Strategic efforts, such as department ownership of equipment, integration with the electronic medical record, and standardizing new hire training, have disseminated the SPH program and vision throughout the organization.
Challenges and Limitations
Given the success of the TLC program, challenges still occurred that could have adversely affected program sustainability. Some challenges were identified through injury investigations or rounds, including accurate assessment of patient needs, use of slide sheets for repositioning and lateral transfers, and supply issues that created barriers to equipment use.
The first challenge was accurate patient assessments. Assessments must be accurate and consistent; when a change occurs in patients’ conditions that could affect mobility, the assessment must be repeated. The challenge was creating an efficient way for caregivers to complete and document each assessment. Then, the assessment must be communicated to all caregivers. Although the frequency of assessment was included in the policy, the mechanism for communicating the assessment was vague.
Recently, the IPS incorporated tracer methodology with regular rounds on all units at each facility. The tracer is a chart review with the manager or caregiver to determine whether assessments have been completed and whether they are consistent with each patient’s activities of daily living, fall risk, and skin condition. At the conclusion of tracer rounds, areas for improvement are identified, and the nurse manager is able to immediately share the information with staff in real time. This approach has been well received by managers and staff and is seen as a more positive approach to making changes and reinforcing the nonpunitive culture of safety. The success of this effort is currently being monitored.
The second challenge is using friction-reducing slide sheets for bed mobility tasks. The most difficult change for seasoned nurses was to use slide sheets, rather than draw sheets, to move patients up in bed. Draw sheets have long been used to reposition patients in bed; however, this technique poses a high risk of injuries (Lloyd & Baptiste, 2006). In 2015, 80% of root cause in this health system was using a draw sheet rather than slide sheet. Because patients are already lying on draw sheets, it is convenient for caregivers to use it to move patients (Fragala & Fragala, 2014; Weiner, Alperovitch-Najenson, Ribak, & Kalichman, 2015). However, slide sheets reduce the force needed to move patients, minimizing their discomfort and decreasing the sheering force on patients’ skin (Lloyd & Baptiste, 2006). Sometimes availability of slide sheets can contribute to nurses’ decisions to use a draw sheet (Wardell, 2007). Slide sheets should be in patients’ rooms to avoid delay in repositioning them (Rich, 2006).
The final ongoing challenge for this health system was a laundry and supply issue for slide sheets and slings. These items are reusable and must be laundered between patients. If the laundry process results in the items not being available when needed, caregivers are frustrated and resort to manual methods of moving and repositioning patients (Rich, 2006).
Conclusion
Implementing an SPH program can improve safety for patients and caregivers. The challenge is sustaining the initial benefits of the program and creating culture change within the organization. The keys to success are the IPS’ vigilant oversight of the program, addressing issues as they arise, thoroughly investigating each patient handling injury, engaging staff in discussions without fear of blame, making improvements and changes to the program based on the results of rounds and investigations, and sharing the results with both staff and leadership. Sustainability is a complex issue and is only possible when an SPH program becomes an integral part of organizations’ overarching culture of quality and safety.
In the 8 years since the implementation of this SPH program, a significant reduction in caregiver injuries related to patient handling has been documented. The system has also realized a dramatic decrease in injury severity and WC costs. The return on investment, regardless of how it is measured, is substantial. Although caregiver injuries have decreased since implementation of the program, the injury trend is now flat. The complexity of human behavior and myriad of variables that can affect injury occurrence may preclude the goal of zero patient handling injuries in a large health system. However, complacency due to goal attainment can move focus to the next initiative and a once successful program may falter. This program is worth the focus and resources because every injury prevented is a career potentially saved and that is the most valuable outcome of all.
Applying Research to Practice
The use of safe patient handling equipment may initially reduce injuries to caregivers and lower workers’ compensation costs. However, purchase of equipment alone will not ensure long-term success. The organization, highlighted in this article, has demonstrated that a Safe Patient Handling program can be sustained by utilizing key components proven effective in creating organizational change. These components include establishing a clear need for change, involving key stakeholders, communicating the vision for change, empowering people to act, removing barriers to change, measuring outcomes, responding quickly to issues, celebrating successes, and continually striving for improvement. Safe Patient Handling can become an integral part of the organizational culture, keeping both patients and caregivers safe.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Christine Olinski is the senior consultant for occupational health and leave administration at Baptist Health System in Jacksonville, Florida. At the time of TLC program inception, she was the director of employee health for Baptist Medical Center Jacksonville.
Christine E. Norton is the injury prevention specialist for Baptist Health System in Jacksonville, Florida.