
Abstract
The rate for musculoskeletal injuries among health care workers is one of the highest for all industrial sectors in the United States; these injuries often occur during manual handling (i.e., lifting, moving, transferring, and repositioning) of patients. The following article describes the process used to complete a comprehensive assessment, as well as the planning, implementation, and initial evaluation of a quality improvement program to reduce work-related musculoskeletal disorders (WMSD) among health care workers employed by a rural Midwest hospital. Key elements for WMSD injury reduction were identified and compared across literature sources, national standards, and current state and federal legislative requirements for hospitals. The program used a multi-factor design that included evidence-based interventions (i.e., those supported by emerging evidence) to create a comprehensive Safe Patient Handling and Mobility (SPHM) program intended to address the unique needs of the organization. Initial program results are reviewed as well as significant considerations and challenges for SPHM programs.
Keywords
Musculoskeletal injury rates for workers in the health care industry rank among the highest of all U.S. industries (Centers for Disease Control and Prevention [CDC], The National Institute for Occupational Safety and Health, 2013). These injuries often occur as a result of overexertion, with manual handling of patients during lifting, moving, transferring, and repositioning creating the greatest risk for sustaining this type of injury (CDC, 2014). The Bureau of Labor Statistics (2011) ranks overexertion as the leading cause of injuries among health care workers across the United States. The 2011 injury rate from overexertion for U.S. hospital employees was 6.8 per 100 full-time employees, almost twice the injury rate for workers employed in private industry, and also exceeding the injury rate for hazardous industries such as construction and manufacturing (Occupational Safety and Health Administration [OSHA], 2013). Contributing risk factors for health care workers include an aging workforce of registered nurses with an average age of 44 years, an ongoing nursing shortage, and the ever increasing rate of obesity among U.S. workers (CDC, 2014).
Hospitals are experiencing substantial changes in the delivery and reimbursement of health care services and are continuously seeking cost-effective strategies that will set them apart from their competitors, while bringing added value to their organizations. The program described here was initiated in a small, rural community hospital in the Midwest as a step toward decreasing the number of musculoskeletal injuries sustained by health care workers. The following article describes in detail the process of identifying the problem and then planning, implementing, and initiating a formative evaluation of a quality improvement program to reduce work-related musculoskeletal disorders (WMSD) for this organization.
Problem Identification
To aid in problem identification and gain an ecological perspective of the organization’s health, multiple data sources were examined, including health insurance annual summary reports, work injury data, and health risk assessment aggregate reports. The organization had recently implemented a corporate employee wellness program, and employee health data were collected through voluntary participation in on-site screenings and self-reported data. Initial data sources reviewed confirmed that musculoskeletal conditions and injuries were a leading health concern for employees in this organization.
To further define the problem, a comprehensive assessment was then conducted, which examined both qualitative and quantitative data sources, and organizational factors that could influence worker behaviors that hinder and promote workplace safety. Data sources included employee and stakeholder interviews, employee demographic and injury surveillance data, workers’ compensation claims and cost reports, workplace policy and procedure manuals, national data from the Bureau of Labor Statistics (2011), and a literature review. The results of this in-depth assessment included (a) inadequate and fragmented utilization of patient handling equipment and processes, (b) a lack of detailed and timely injury reporting and monitoring, and (c) missing or ambiguous policies and procedures relevant to employee safety and patient handling.
Although the organization had some equipment to decrease the need for manual patient lifting by employees, the equipment was often not used. Interviewed workers attributed this lack of equipment utilization to perceived lack of time, inconvenience, or limited available assistance from coworkers. A complete inventory of patient handling equipment and technology was not available, nor were any relevant ergonomic assessment data. Patient handling and mobility assessments were not completed, nor were decision algorithms or clinical decision pathways used to determine when and what type of handling and mobility equipment were appropriate for each individual patient. A formal policy or procedure aimed at providing limitations and guidance when lifting or mobilizing patients was also not available.
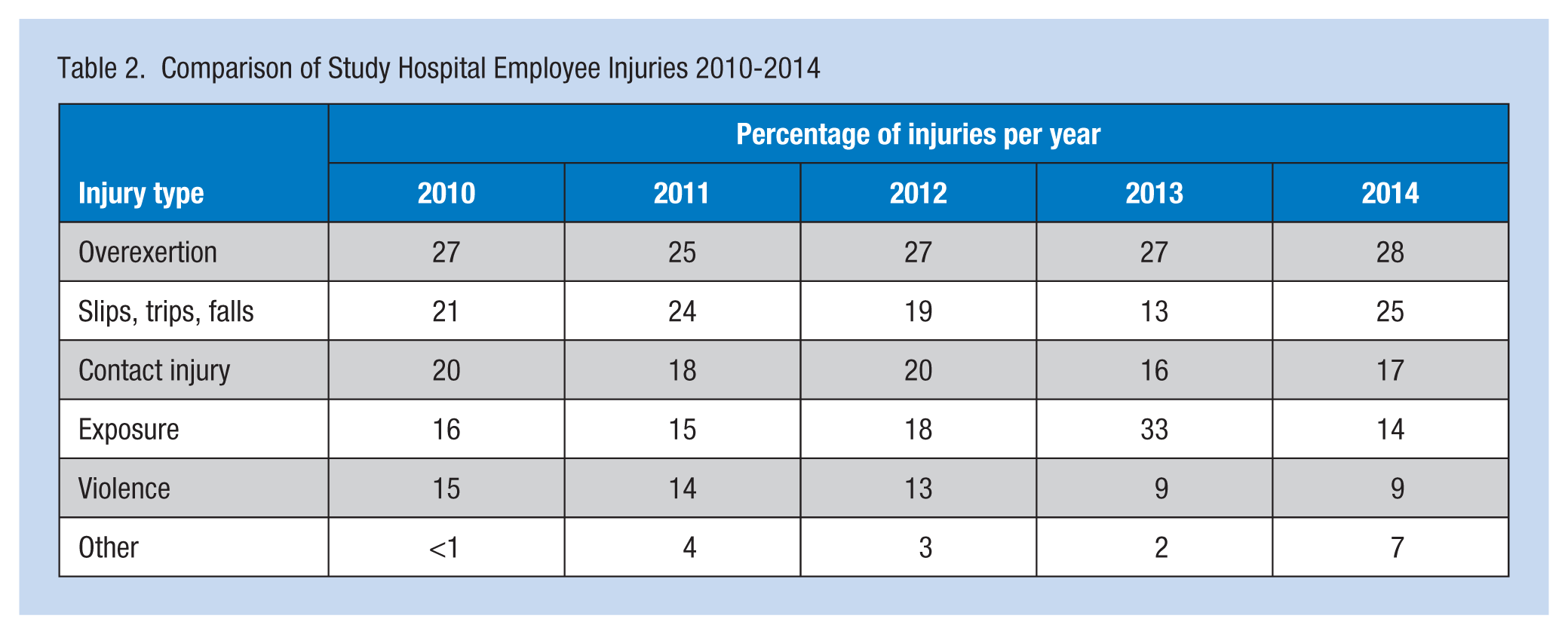
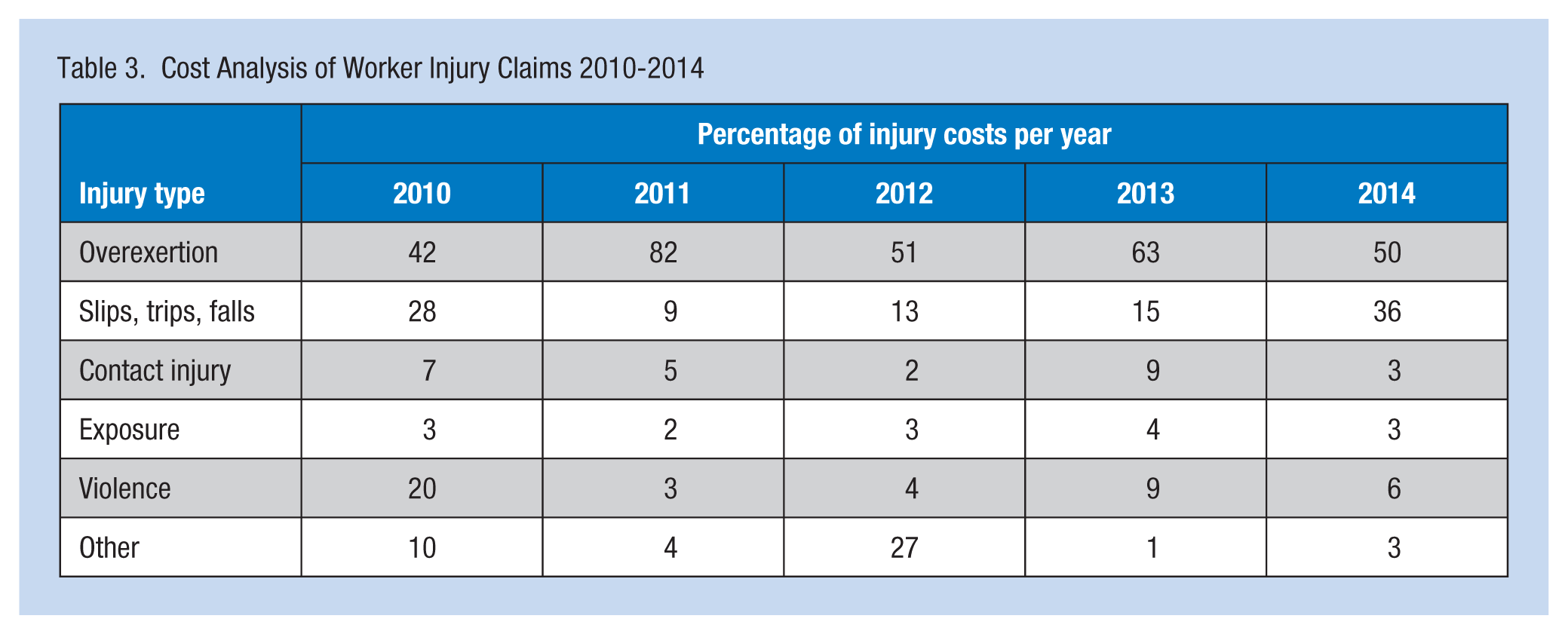
In addition, this organization (a) lacked a formal policy regarding the reporting and handling of employee injuries, (b) did not include any provisions for employee safety in the patient safety program, and (c) did not address employee injuries via either the employee health or safety departments. A part-time nurse working in the Human Resources Department provided case management services for workers’ compensation claims, but was not tasked with any post-injury trending or analysis. The OSHA Total Case Incident Rates (TCIR) and Days Away, Restricted, or Transferred (DART) scores for work injuries were not calculated or monitored. The OSHA summary reports for 2010 to 2014 were accessed and reviewed: TCIR and DART scores were calculated and compared across years as were OSHA TCIR rates for U.S. hospitals (see Table 1). Although the TCIR for this hospital was below the median, the DART score, an indicator of severity, exceeded the national median for U.S. hospitals. Days Away, Restricted, or Transferred scores are the most useful indicator when examining injury data because DART scores are based solely on those injuries severe enough to require days away from work or restriction of regular job duties and should be lower than the TCIR. A comparison of annual injury and cost data was completed for years 2010 to 2014, and results indicated that musculoskeletal injuries accounted for 40% or more of employee injuries each year since 2010, with 25% or more annually being related to overexertion (see Table 2). Annual injury costs for WMSD accounted for 40% or more of total costs for each year from 2010 to 2014 (see Table 3). A random sampling (n = 82) of open WMSD injury cases for 2014 were examined for contributing factors; results of this review confirmed that work practices (e.g., lifting or repositioning patients) were a contributing factor in 65% of the cases.
Comparison of OSHA TCIR and DART Scores for Project Hospital
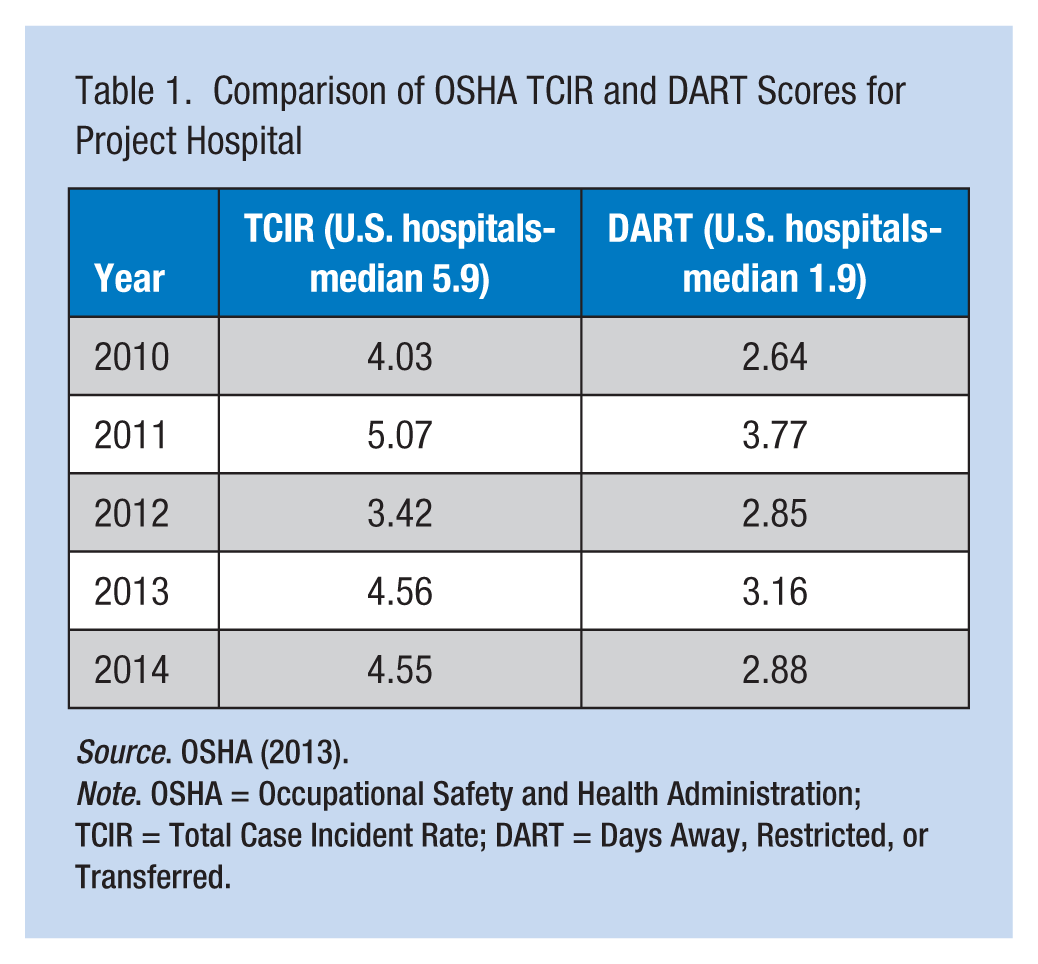
Source. OSHA (2013).
Note. OSHA = Occupational Safety and Health Administration; TCIR = Total Case Incident Rate; DART = Days Away, Restricted, or Transferred.
Comparison of Study Hospital Employee Injuries 2010-2014
Cost Analysis of Worker Injury Claims 2010-2014
The next step in the assessment process was to identify best practices in preventing overexertion injuries and compare the practices to those of the organization. As most overexertion injuries are related to patient lifting and moving, implementation of a comprehensive Safe Patient Handling and Mobility (SPHM) program to reduce these injuries was well supported by the literature (American Nurses Association, 2011; Cohen et al., 2010; Miner, Laramie, Davis, & Tran, 2013; OSHA, 2013). Key program elements were identified (VISN8 Patient Safety Center of Inquiry, 2013) and compared across literature sources, national standards, and current state and federal legislative requirements for hospitals. These next steps include a formal SPHM program with an organization-wide policy restricting the manual handling of patients; a comprehensive risk analysis; inclusion of engineering design, technology, and equipment; initial and ongoing staff training; use of patient assessment tools and decision algorithms to guide clinicians; and building a culture of safety that includes monitoring of key performance indicators for both employees and patients that are leadership driven (American Nurses Association, 2013; Illinois General Assembly, 2010; OSHA, 2013; VISN8 Patient Safety Center of Inquiry, 2013). A comparison of key program elements to hospital data revealed various standards and requirements were not currently met by the hospital. For example, a formal SPHM program had not been implemented by the hospital, a safe patient handling policy was lacking, risk analysis and control processes were not in place, and SPHM training was provided only at time of hire to select employees and not on an annual or ongoing basis. Safe patient handling and mobility training for newly hired employees was conducted on the employee’s unit supervised by preceptors who had not received formal annual SPHM training. The organization also lacked a SPHM committee to address employee safety issues and a program coordinator to facilitate compliance.
Planning
The program was designed based on evidence from the literature on effective interventions to reduce patient handling injury rates, and meet legislative requirements and current standards. The Agency for Healthcare Research and Quality publication, Patient Safety and Quality: An Evidence-Based Handbook for Nurses (2008), examined interventions for safe patient handling that were either evidence-based or supported with emerging evidence. Incorporating patient handling equipment and devices, minimal or no-lift policies, ongoing training, and lift teams are examples of evidence-based interventions. Interventions supported by emerging evidence include peer leader education, patient assessment tools, algorithms, and after-action reviews following an injury or when near-miss events have occurred. A study by Powell-Cope and colleagues (2014) reported that evidence supporting a multiple component approach should include comprehensive training and the use of equipment. Training aspects found to be significant included peer leader training, demonstrated competency in the selection and use of SPHM technology and equipment, and incorporation of evidence-based training into new hire orientation. Findings also included organizational factors (i.e., lack of leadership support and equipment availability and supply) that were associated with patient handling injuries (Powell-Cope et al., 2014). The American Nurses Association (2013) incorporated training, equipment, and other evidence-based interventions into the publication, Safe Patient Handling and Mobility: Interprofessional National Standards. The literature suggests that multi-factor interventions (e.g., administrative, engineering, and behavioral controls) are more effective in reducing injury rates and costs (Stevens, Rees, Lamb, & Dalsing, 2013) than single factor interventions. Inclusion of such interventions as injury analysis, use of decision algorithms, and reinforcement of training support program effectiveness. In a study by Sorenson et al. (2011), “an integrated approach, that attends to workers’ health behaviors as well as the potential for exposures on the job, holds promise for bolstering the impact of interventions” (p. 9). Implementation of an organization’s wellness program suggests hospital leadership support can optimize the health and well-being of the workforce.
Based on the review completed, necessary elements of a SPHM program designed for this hospital should include the following:
Education and training
Maintaining competence in the use of equipment and technology
Post-injury analysis
A formal SPHM policy, which must include a “right to refuse” procedure for staff to decline patient handling activities with unacceptable risk of injury.
Education and training was addressed through development of a computer-based learning (CBL) module, and initially piloted with a select group of program “champions” or trainers, to allow for the testing and identification of any process issues. On full implementation of the program, both new and existing employees with patient handling responsibilities were trained using the CBL module. Additional training was also required for those employees who had patient handling, moving, or repositioning responsibilities, and included SPHM assessments, use of algorithms for selecting appropriate equipment, and a unit-specific equipment competency.
To initiate a post-injury analysis, the reporting process for injuries sustained and near-miss incidents was completed in a timely manner and with sufficient detail that corrective and preventive actions could be identified and an action plan developed to avoid future injuries.
Templates and sample policies specific to SPHM were used to draft the organization’s policy. The draft policy was compared with current standards and legislation to assure the final policy met all necessary requirements, prior to submission for leadership approval.
In addition, a SPHM marketing brochure for patients providing information on SPHM principles was recommended as an education and safety promotion tool and a way to promote communication between health care workers, patients, and their families.
The program targeted a multidisciplinary group of employees representing 63% (n = 1,452) of the organization’s staff whose job responsibilities included lifting, moving, transferring, or repositioning patients. Professional, White females accounted for 70% of the organization’s employee population, largely composed of nurses. Obesity among employees reached 42% of the entire workforce in 2014, and although age-related data were not available for the organization, as of 2011, the median age of hospital employees in the U.S. rose to 43.6 years (OSHA, 2013). Both age and obesity are known to increase workers’ vulnerability for musculoskeletal injuries.
Implementation
Program implementation began in May 2015. The SPHM CBL training module used a slide presentation format requested by leadership, resulting in a training module of 67 slides; participants reported a completion time of 30 minutes to 45 minutes. Content development was based on learning objectives, comprehensive SPHM training for applicability to all employees, and current training recommendations gleaned from a literature review. A post module learning assessment was created in collaboration with the nursing education department and administered directly to participants following completion of the CBL module. Additional steps included stakeholder approval of material, partnership with the IT department to identify CBL module processes, selection of the pilot group, identification of reporting structures for tracking module completion, and assessment scoring.
The equipment competency process involved selecting and approving the SPHM patient assessment tool and SPHM algorithms for equipment decision, training logs and checklists, and formal “champion” training on SPHM. To establish a baseline inventory of equipment and ergonomic data, survey questionnaires were created to inventory currently available equipment, ergonomic issues or space constraints, patient distribution by dependency levels, and clinical staff characteristics for each unit. Surveys were completed by unit managers or directors and returned for data compilation. Patient assessment tools, decision algorithm examples, and training logs were compiled and submitted to leadership for review. Local and national training options for “champions” were researched and compiled.
The injury investigation plan included submission of all injury reports within 48 hours of injury occurrence. A questionnaire specific to SPHM injuries was created and received approval from the Human Resources and Quality Departments. The questionnaire required detailed information on patient characteristics, activities at the time of injury, patient handling methods and/or equipment being used, and the level of assistance received from the patient or other staff members. The preferred process for questionnaire distribution and submission was the new online reporting system. However, a temporary process was initially implemented during the creation of the questionnaire in the online system. All new injury reports were reviewed by the workers’ compensation nurse, then the questionnaire was emailed to the unit manager with a 48 hour turnaround time approved by leadership.
A SPHM policy was created by using policy templates and samples obtained from exemplar organizations, sources of literature, and a review of applicable legislative requirements. These documents were used to guide the drafting of the written SPHM policy; key stakeholders were also included in the policy development process. The final policy included statements on its purpose, definitions, the policy’s audience, and procedures and responsibilities detailed in the document. The SPHM policy also included a “right to refuse” provision as required by state legislation (Illinois General Assembly, 2010). This provision allows workers to refuse patient handling or movement that places the health care worker or patient at an unacceptable risk of severe injury.
Evaluation
A formative evaluation was completed for program components implemented to date, focusing on whether a comprehensive SPHM program’s processes (i.e., education and training, equipment and technology components, post-injury analysis, and formal SPHM policy enactment) had been fully initiated. In terms of education and training processes, the CBL module was assigned to a pilot group that included nurses, physical therapists, unit managers, and nurse educators (n = 25); the pilot group reported an 80% completion rate. Results of a satisfaction survey using a 5-point Likert-type scale completed at the end of the module revealed that 78% of the pilot participants were dissatisfied with the length of the module, although highly satisfied with the content of the slides. This feedback led to a program variance regarding how initial training was provided; required training should be offered as a live in-person, interactive training session. The initial training and equipment competency was completed during a live 4 hour training session scheduled for the following fall as part of a planned safety fair. The safety fair also included SPHM equipment vendors, allowing employees to explore and rate potential SPHM equipment options. Unfortunately, no commitment to champions training was made.
The results of the equipment competency evaluation confirmed that the organization selected the following tools for staff use at the onset of training: (a) a patient SPHM assessment tool, (b) equipment decision algorithms, and (c) training checklists/logs. Of the equipment inventory and ergonomic surveys submitted to the clinical units, 88% of the surveys were completed and returned. Of the surveys received, all clinical units reported SPHM equipment needs, 67% reported that storage of SPHM equipment was an issue, and units reporting the highest rates of patient dependency paralleled the units with the highest frequency of WMSD injuries.
The post-injury analysis process, including both the SPHM injury questionnaire and summary report, was approved and implemented for all new injury reports 1 month into the implementation process. A TCIR/DART tracker was created, and the nurse responsible for workers’ compensation claims calculated scores annually. The 2014 TCIR/DART was used as the baseline injury rate, and a decreased injury rate of 10% was based on the injury analysis. An injury summary report was created by extracting data fields from the injury questionnaire to facilitate tracking and monitoring of reported injuries. Morning safety huddles, implemented in response to patient safety issues, also included reporting on employee injuries. In addition, a formal employee safety committee was formed to review all injury reports and monitor corrective action plans and injury trends.
A SPHM policy was drafted and revised with stakeholder input; the final version was approved by Human Resources, Quality, and Nursing Administration prior to receipt of executive approval. The SPHM policy was communicated to employees during the fall safety fair and incorporated into new employee orientation.
Discussion
Program implementation and sustainability could be negatively affected by some environmental challenges within the organization. The organization’s leadership is experiencing multiple competing priorities (e.g., upcoming reaccreditation). Recently, the organization underwent significant changes in an already volatile health care environment: adapting to a new facility, implementing a new electronic health record, and key personnel changes. New key leaders may necessitate extending the original program timeline to re-establish critical partnerships.
Several steps were taken to enhance the likelihood of program sustainability: adopting a cost minimization approach to program development, building diverse partnerships during program planning, aligning the program with other initiatives such as patient safety, promoting quality care initiatives, and aligning with becoming a high-reliability organization. Key to sustainability includes building leadership awareness of current and proposed legislation related to employee and patient safety, and the substantial cost savings to the organization that could be realized by reducing or eliminating SPHM-related injuries.
Defining fiscal considerations for the organization during program implementation included (a) a budget adjustment to accommodate live session training, (b) a capitol budget for the purchase of additional equipment, and (c) an annual cost projection for the maintenance and replacement of equipment and supplies. These cost considerations should be compared with potential and actual injury expenditures and cost savings to calculate the organizations return on investment (ROI). The use of program champions will provide both employees and new hires with needed support and training for the competent use of SPHM equipment, while providing a local resource for questions or issues. The commitment to identifying and training program champions is a crucial next step. Going forward, the integration of algorithms and decision tools into patients’ plans of care could increase accountability and should be carefully considered. Although training and competency measurements will continue on an annual basis, and new hires will complete SPHM training during their orientation periods, it must still be determined who will provide new hire training and how this training will be delivered.
The application of a process such as Corrective Action Preventive Action (CAPA) should be added to the post-injury analysis. The CAPA process is aligned with the PDCA (Plan-Do-Check-Act) Cycle (Bulsuk, 2009) that is currently used by the organization. Use of these tools in the injury investigation process could support the development of action plans specifically aimed at injury reduction and prevention. Finally, although the SPHM marketing brochure was not considered core at the time of program initiation, the brochure could be considered for development and implementation at a later date.
In conclusion, continuous ongoing reevaluation of program effectiveness in reducing WMSD injuries in the workplace should be conducted. A critical step is to assure additional tools and processes receive adequate consideration and are tailored to the unique needs of this organization to promote continuous quality improvement of the SPHM program design.
In Summary
Musculoskeletal injury rates for workers in the health care industry rank among the highest of all industries within the United States, often resulting from overexertion when handling patients.
Results of a comprehensive assessment were used to develop a multi-factor Safe Patient Handling and Mobility (SPHM) program based on a literature review, standards, and current legislative requirements.
Results of a preliminary formative evaluation indicated implementation of a comprehensive SPHM program that has been initiated within the organization, and factors influencing sustainability and continuous quality improvement had been successfully linked with other current initiatives being monitored by executive leadership.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Linda Przybysz is currently the health services director NA [North America] for the Kimberly-Clark Corporation in Neenah, Wisconsin, and is a member of the organization’s strategic team for workplace health and wellness on regional and global levels. She completed a DNP in advanced public health nursing from Rush University and also serves in an Adjunct Faculty role.
Pamela F. Levin is a professor in the Department of Community, Systems, and Mental Health Nursing at Rush University College of Nursing, Chicago, Illinois. Her background is in public health and occupational health nursing. Her scholarship focus is on public health nursing workforce development and violence prevention in healthcare settings.