
Abstract
Background:
Promoting safe patient mobility for providers and patients is a safety priority in the hospital setting. Safe patient handling equipment aids safe mobility but can also deter active movement by the patient if used inappropriately. Nurses need guidance to choose equipment that ensures their safety and that of the patients while promoting active mobility and preventing workplace-related injury.
Methods:
Using a modified Delphi approach with a diverse group of experts, we created the Johns Hopkins Safe Patient Handling Mobility (JH-SPHM) Guide. This diverse group of 10 experts consisted of nurses, nurse leaders, physical and occupational therapists, safe patient handling committee representatives, and a fall prevention committee leader. The application of the tool was then tested in the hospital environment by two physical therapists.
Findings:
Consensus was reached for safe patient handling (SPH) equipment recommendations at each level of the Johns Hopkins Mobility Goal Calculator (JH-Mobility Goal Calculator). Expert SPH equipment recommendations were then added to JH-Mobility Goal Calculator levels to create the JH-Safe Patient Handling Mobility Guide. JH-Safe Patient Handling Mobility Guide equipment suggestions were compared with equipment recommendations from physical therapists revealing strong agreement (n = 125, 88%).
Conclusion:
The newly created JH-Safe Patient Handling Mobility Guide provides appropriate safe patient-handling equipment recommendations to help accomplish patients’ daily mobility goals.
Applications to Practice:
The Johns Hopkins Safe Patient Handling Mobility Guide simultaneously facilitates patient mobility and optimizes safety for nursing staff through recommendations for safe patient handling equipment for use with hospitalized patients.
Background
Despite the known harms of reduced physical activity levels, hospitalized patients generally spend the majority of their day in bed (Brown et al., 2004, 2009; Mudge et al., 2016; Tolles et al., 2020). This immobility can cause hospitalization-associated disability (HAD), impairing patients’ independent living skills and increasing their risk for complications such as pressure injuries, falls, pneumonia, and delirium (Brown, 2020; Gordon et al., 2019; Loyd et al., 2020). To decrease the occurrence of HAD and associated immobility related harms, many hospitals have implemented programs designed to promote mobility among hospitalized patients (Hoyer et al., 2016). These programs encourage patients to increase their physical activity and can lead to improved patient outcomes, such as decreased length of stay and patient satisfaction (Constantin & Dahlke, 2018; Cortes et al., 2019; Diwan et al., 2020; Hoyer et al., 2016; Schaller et al., 2016; Valenzuela et al., 2020).
Enhancing inpatient mobility is crucial but so is ensuring safety for both patients and staff when performing mobility activities exercises. After all, boosting patient mobility loses its value if it leads to patient injuries and musculoskeletal injuries to the staff. As such, mobility promotion programs should include education and guidance on safe patient handling (SPH) to ensure that patients are being mobilized in a way that protects both the patient being mobilized and the staff performing the mobilization session (“Safe Patient Handling Laws and Programs for Health Care Workers,” 2016). A key component of SPH is the appropriate use of SPH equipment (e.g., assistive devices, lifts), which can help to minimize the risk of injury to patients and staff. However, overutilization of SPH equipment, such as total assist lifts, may work against efforts to promote patient mobility as they allow patients to be moved passively (Rickelmann & Knoblauch, 2018; Wyatt et al., 2020). A reference guide, tailored to a patient’s mobility level, would aid clinicians in selecting suitable SPH equipment for patient mobilization while also promoting active participation (L. M. Klein et al., 2018).
Common methods for SPH equipment selection often involve a performance test in which the provider must take time to move a patient through a series of unique tasks of increasing difficulty and directly observe their performance. Only after the completion of these tasks does the performance test suggest an appropriate tool for safe patient handling (Boynton et al., 2014). Bedside Mobility Assessment Tool (BMAT) is one such tool that is utilized in clinical practice. It is used to assess tolerance and ability to perform mobility and provides SPH equipment recommendations based on patient performance of various tasks (Boynton et al., 2014). The BMAT generally requires about 2 minutes for the patient to perform various physical tasks and the BMAT scorer to assess mobility level on a scale of 1 to 4 (Boynton et al., 2014, 2020). Once a patient achieves a certain mobility level, the test is concluded and recommendations for the SPH equipment for that level are used for patient mobility. There is a risk for undermobilization of the patient if the patient-related barriers such as pain, limit the assessment of a higher mobility level. Performance tests may be underutilized due to the time needed for administration and the need for patients to complete all items during administration for scoring, especially by busy hospital nurses (Young et al., 2018). Using an assessment tool, that can be scored based on observation of routine patient activities combined with nurses’ clinical judgment of patients’ anticipated performance rather than task completion, would reduce the additional time required to complete all items on performance assessments (Hiser et al., 2022; Pottenger et al., 2019).
The Activity Measure for Post-Acute Care “6-Clicks” Inpatient Mobility Short Form (AM-PAC 6-Clicks) is one such tool, but to date, has not been used to help recommend specific SPH equipment (Haley et al., 2004). Although the BMAT and AM-PAC 6-Clicks demonstrate moderate levels of convergent validity, unlike the BMAT, the AM-PAC 6-Clicks can be scored without having the patient complete all the tasks (Lininger et al., 2021).
The utilization of the AM-PAC 6-Clicks Basic Mobility Inpatient Short Form for suggesting SPH equipment is grounded on research that reported its application for recommending precise mobility milestones using a tool known as the Johns Hopkins Mobility Goal Calculator (JH-Mobility Goal Calculator). The JH-Mobility Goal Calculator uses the Johns Hopkins Highest Level of Mobility (JH-HLM) and AM-PAC 6-Clicks to suggest minimum mobility goals for patients based on their level of function (Hoyer et al., 2023). The AM-PAC measures a patient’s mobility capability, based on the patient, a family member, or a clinician’s assessment to rapidly evaluate the level of assistance a patient requires to move out of bed, stand, or walk (Haley et al., 2004; Jette et al., 2014). AM-PAC 6-Clicks Mobility Short Form is a clinician or patient-scored questionnaire with a score ranging from 6 to 24 or complete functional impairment to independence (Arnold et al., 2021; Jette et al., 2014).
The JH-Mobility Goal Calculator suggests personalized daily mobility goals based on the AM-PAC 6-Clicks and offers updated goals each time the patient is evaluated using AM-PAC 6-Clicks (L. M. Klein et al., 2018). Research indicates that the JH-Mobility Goal Calculator is a practical and effective method to enhance patient mobility (Hoyer et al., 2023; L. M. Klein et al., 2018; McLaughlin et al., 2022). However, the current tool falls short in providing recommendations for SPH equipment, which is typically determined during the planning phase of daily mobility goals. Ideally, this information should be conveniently accessible alongside the recommended mobility goal.
The Johns Hopkins Safe Patient Handling Mobility (JH-SPHM) Guide aims to improve upon existing tools that help guide clinician selection of SPH equipment. The purpose of this study was to describe the development of the JH-Safe Patient Handling Mobility Guide, which recommends specific SPH equipment for each level of the JH-Mobility Goal Calculator. We also sought to clinically test the JH-Safe Patient Handling Mobility Guide for agreement in the hospital setting.
Methods
Design and Process
To develop the JH-Safe Patient Handling Mobility Guide, we employed a modified Delphi approach as a methodological structure (Barrett & Heale, 2020). Our foundational objectives included: (a) suggesting SPH equipment that aligns with the patient’s mobility capability and daily mobility goal, (b) minimizing the assessment and documentation load on clinicians, and (c) enhancing the patient mobility promotion strategy by increasing adherence to mobility assessments, setting mobility goals, and utilizing SPH equipment.
Study Participants
Given the interprofessional nature of activity and mobility promotion, the first step in developing the guide was to form an interprofessional expert panel to include experts who utilize SPH equipment in their clinical practice, mobilize hospitalized patients, are responsible for procuring and/or maintaining the equipment, and engage in decision-making of policies and procedures to promote patient and staff safety in the hospital setting to provide input to the content of the guide. Therefore, we sought representation from frontline nursing, rehabilitation therapists, nursing leaders, rehabilitation therapy leaders, and fall prevention and safe patient-handling committee members. To ensure a wider perspective we recruited panel members from multiple acute care hospitals. Fifteen experts who were familiar with the AM-PAC 6-Clicks and JH-AMP tools or had strong mobility/safe patient-handling programs were invited through email. Ten of the experts responded agreeing to participate. These experts included two frontline nurses (with mobility & safe patient-handling expertise), two nurse leaders, two physical therapists, one occupational therapist, two safe patient-handling committee representatives/program leaders, and one fall prevention committee leader. On average, members of our panel had more than 10 years of clinical experience and more than 5 years of specific SPH or mobility promotion experience.
The modified Delphi approach uses a series of “rounds” where a panel of experts is asked to provide their opinions on a particular problem (Eubank et al., 2016; Slade et al., 2016; Souto-Miranda et al., 2023). After each round, participants are provided with the results of the previous round and can comment on the opinions provided by other panel experts and adjust their initial feedback as needed. In this study, a consensus was reached when the majority of the expert panel agreed to the decision. Our study consisted of two rounds, including a survey and a follow-up focus group.
Data Collection
Round 1
During the first round of meetings held virtually in May 2020, experts were introduced to the project and educated about the Johns Hopkins Activity and Mobility Program (JH-AMP) to provide background for the project (McLaughlin, Friedman, et al., 2023). The JH-AMP is an interprofessional program that uses a systematic approach to increase hospitalized patients’ mobility. The program uses common tools such as AM-PAC 6-Clicks to assess the patient’s function and the JH-HLM Scale to document the patient’s mobility performance. The JH-Mobility Goal Calculator (Figure 1) provides individualized daily mobility goals for hospitalized patients, based on their most recently recorded AM-PAC 6-Clicks score. Previous studies have found the JH-Mobility Goal Calculator to increase overall patient mobility levels when implemented on acute nursing units and to set realistic goals for patients admitted to the hospital following surgery (L. M. Klein et al., 2018; McLaughlin et al., 2022). Previous studies have found the AM-PAC 6-Clicks to be valid and to have excellent interrater reliability between nurses and physical therapists (Capo-Lugo et al., 2023; Hoyer et al., 2018; Jette et al., 2014, 2015). Mobility goals are set on the JH-HLM, an eight-item ordinal scale that indicates a patient’s highest level of observed mobility. The JH-HLM is valid and reliable among hospitalized patients (Hiser et al., 2021; Hoyer et al., 2016). Each of these tools is a core component of the JH-AMP program which has been described in detail previously (McLaughlin, Friedman, et al., 2023).
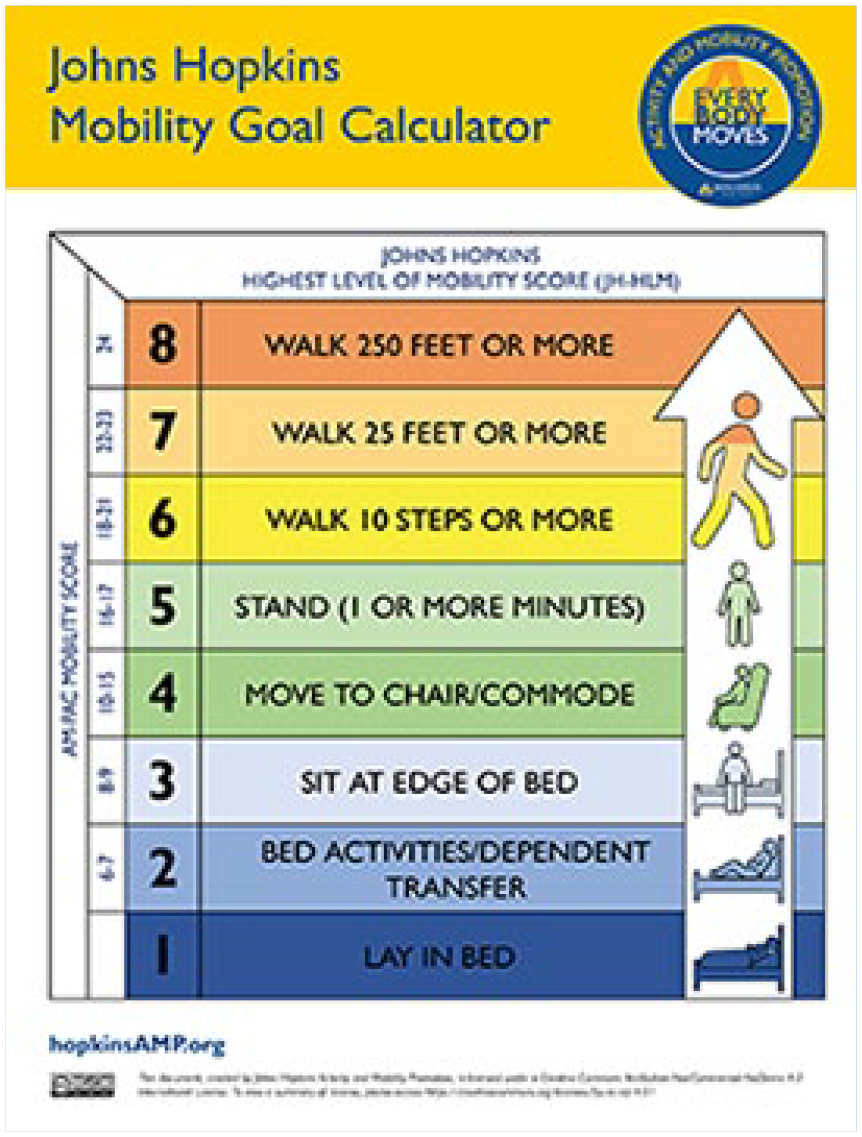
The Johns Hopkins Mobility Goal Calculator
During Round 1, these tools were reviewed, and the group was educated on the JH-Mobility Goal Calculator, which would provide the foundation for the JH-Safe Patient Handling Mobility Guide. Once introduced to the project, all panel members received a link to an online survey that asked them to provide their recommendations individually and independently for the SPH equipment most appropriate for patients at each level of the JH-Mobility Goal Calculator. Experts were provided with the opportunity to engage in a question-and-answer session.
Round 2
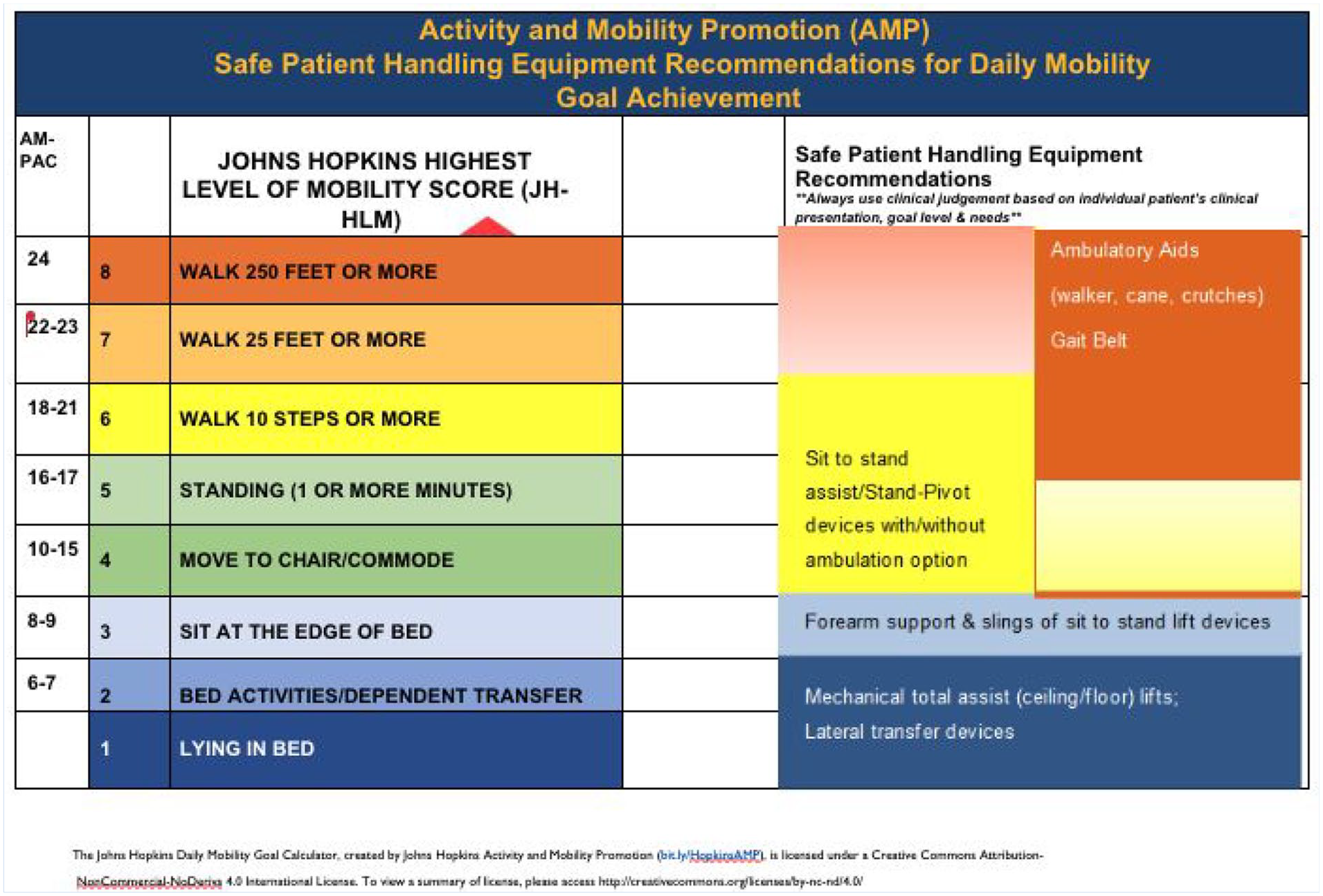
Once the survey was completed by all study panel members, the results of the survey were exported into a spreadsheet and the group was reconvened for a second video conference meeting in August 2020 (see section “Results”). The purpose of this meeting was to review the results of the survey and to reach a consensus on the final SPH equipment recommendations for each level of the JH-Mobility Goal Calculator. The meeting was recorded and shared with panel members unable to attend the video conference live. The study team showed the group a draft of the JH-Safe Patient Handling Mobility Guide with their recommendations at each level. The group discussed the rationale behind the recommendations including the pros and cons of grouping the recommendations into three levels—bed mobility/lateral dependent transfers, out of bed to chair, and ambulation. Discussion included equipment that could be utilized for transitional levels such as the JH-HLM goal of 6 as some panel members were concerned about safety and recommended moving a JH-HLM goal of 6 to the out-of-bed level versus the ambulatory level. The differences were reconciled by adding sit-to-stand devices with an ambulatory option and leaving the JH-HLM goal of 6 with the ambulatory level. Terminologies for the equipment, the number of people required for each level, or equipment recommendations were discussed and a consensus was reached. In addition, panel members discussed equipment availability, patient clinical presentation, workflow, and implementation challenges during planned versus unplanned mobility tasks in clinical practice. These recommendations and concerns were included when designing the user guide for the JH-Safe Patient Handling Mobility Guide.
The study team met with the institution’s graphic designer to draft some examples of the JH-Safe Patient Handling Mobility Guide as depicted in Figure 2. Based on the Round 2 discussion and suggestions, statements and disclaimers were added to use clinical judgment and follow the institutional policy for application to include wider patient populations and different institutions. These drafts were reviewed by the study team and a version was finalized that not only incorporated the expert panel recommendations but also was visually legible as a crosswalk.
The Johns Hopkins Safe Patient Handling Mobility Guide Draft
Clinical Testing
To validate the JH-Safe Patient Handling Mobility Guide, equipment recommendations from the guide were compared with rehabilitation therapist recommendations to nursing staff for equipment usage in clinical practice. In a 1,146-bed tertiary care hospital, 106 hospitalized patients were seen for 125 physical therapy sessions; thus, some patients received multiple therapy sessions. Two full-time staff therapists performed clinical testing of the JH-Safe Patient Handling Mobility Guide. The two therapists did not participate in the modified Delphi rounds or serve on the expert panel. The therapists had 3 years of experience in the hospital setting. The therapists continued to treat their regular patients, per standard of care, across cardiac, medicine, oncology, neurology, and orthopedics floors. After each routine physical therapy session, the therapists recorded the AM-PAC 6-Clicks and JH-HLM based on the mobility level achieved during the therapy session. Therapists also documented their recommendations for SPH equipment for nursing and other clinical staff to use. For SPH equipment, therapists selected from a list that included a rolling walker, cane, crutches, Sara Stedy (Arjo Inc., Addison, IL, USA), Sara Plus (Arjo Inc.), pink slip (Wy’East Medical, Clackamas, OR, USA), or AirPal (Arjo Inc.); Arjo Total Assist Lift (Arjo Inc.), or “other” (Table 2). These were the specific types of equipment available at the institution. This information was documented separately for study use and completed in adherence to IRB-approved study protocol IRB00395329.
During the analysis of study data, the therapists’ equipment recommendation was compared with the JH-Safe Patient Handling Mobility Guide recommendations. An agreement was defined as the therapist’s recommendation matching the JH-Safe Patient Handling Mobility Guide recommendation. A recommendation was deemed more conservative when the JH-Safe Patient Handling Mobility Guide recommendation suggested a higher level of assistance than the therapists’ recommendation.
Results
Round 1
Survey Results
All members of the expert study panel (N = 10) responded to our survey asking for SPH equipment recommendations for each level of the JH-Mobility Goal Calculator. The full results of this survey are provided in Supplemental Table 1. For patients with a JH-HLM goal between 6 and 8, the most common recommendations were for assistive devices that could assist with balance, weight-bearing, and/or energy exertion while allowing the patient to ambulate with the greatest level of independence. For example, the most frequent recommendation for patients in this range was rolling walkers, followed by a cane, and no assistive device. For a JH-HLM goal of 4–5, the recommendations were for sit-to-stand devices that would also provide balance support for patients once in a standing position. For patients with a JH-HLM goal of 3, participant responses varied. Recommendations included sit-to-stand devices, mechanical dependent lifts, and items such as draw sheets to assist with in-bed repositioning. For patients with a JH-HLM goal of 1–2, the recommendations were for dependent/mechanical lifts and items such as draw sheets and wedges that could assist staff with in-bed repositioning.
Round 2
The Round 2 video conference meeting was attended by eight members of the expert panel where survey results were discussed and to work toward consensus on SPH equipment recommendations for each level of the JH-Mobility Goal Calculator. The meeting was recorded and viewed later by the other two expert panel members. During this meeting, consensus was reached on recommendations for SPH equipment (Figure 2). A draft of the JH-SPHM Mobility Guide was created and depicted the AM-PAC, JH-HLM, and SPH equipment recommendations as a visual cross-walk. The two other panel members provided their recommendations after viewing the recording of the meeting. Their recommendations were compared with the rest and found to be the same as those in the majority consensus.
Visual Display of the JH-Safe Patient Handling Mobility Guide
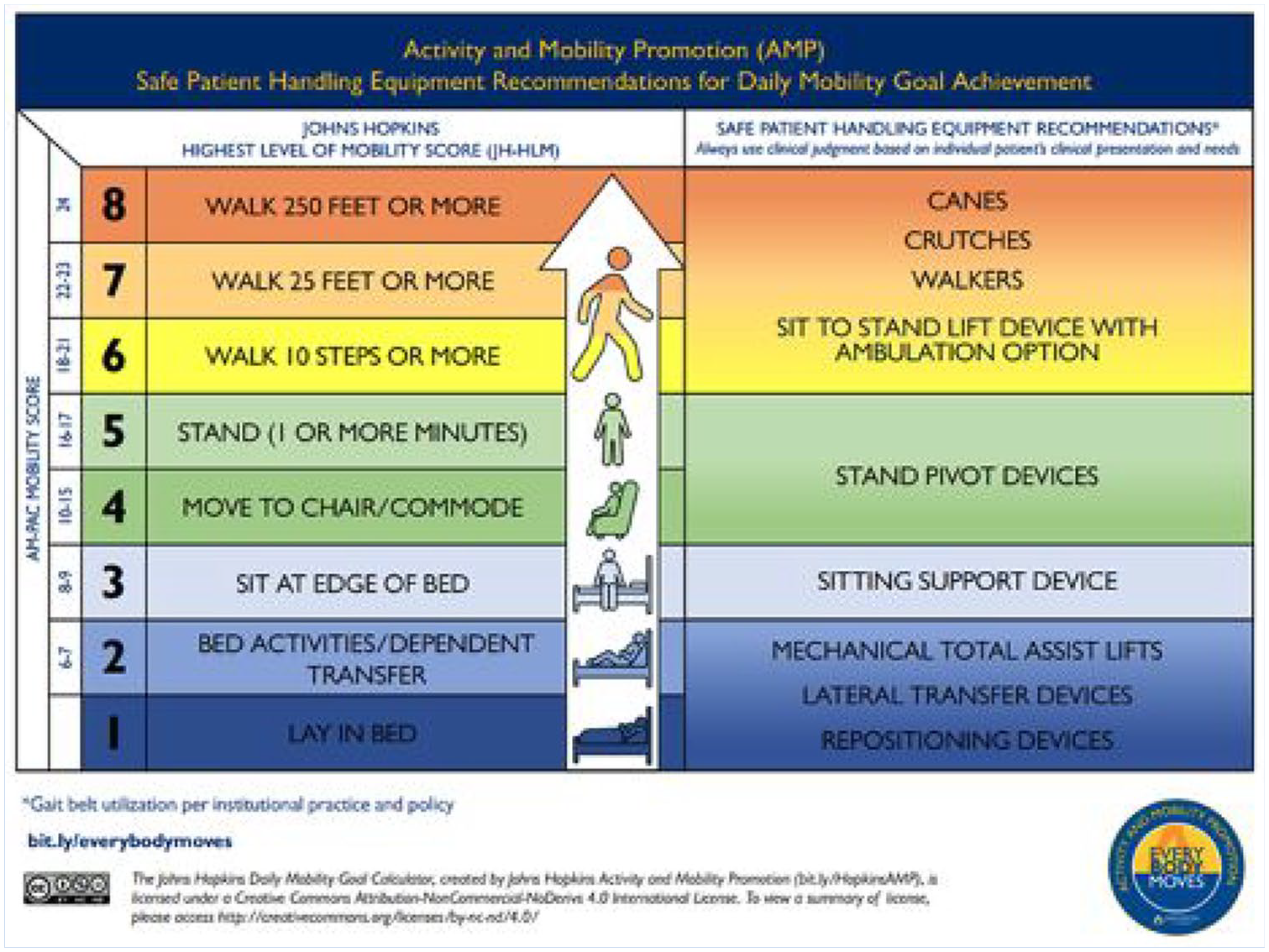
With consensus reached on recommendations for SPH equipment that corresponded with each level of the JH-Mobility Goal Calculator, the study team and a graphic designer reviewed the recommendations to determine the best way to display the recommendations from the expert panel for staff reference. They determined it was important that these recommendations be displayed alongside the JH-Mobility Goal Calculator to allow for quick reference prior to mobilization sessions, simultaneously when identifying patients’ daily mobility goals. The result of this meeting was the JH-Safe Patient Handling Mobility Guide (Figure 3). Figure 3 depicts the finalized JH-SPHM Guide, in which the reader can visualize the patient’s mobility goal based on AM-PAC 6-Clicks and JH-HLM, and the correlating SPH equipment recommendations. Once the JH-Safe Patient Handling Mobility Guide was created, it was shown to the 10 members of the expert panel for review, which they approved. The study team members developed a user manual with operational definitions, use instructions, and frequently asked questions (Supplemental Appendix 1). The manual describes the JH-Mobility Goal Calculator and JH-Safe Patient Handling Mobility Guide, accompanied by case studies and operational definitions for reference. When subsequently reviewing the JH-Safe Patient Handling Mobility Guide with study team members at our institution, it was recommended that a blank column be added so nursing personnel could add the brand names of specific SPH equipment available on their units, as equipment available among institutions may vary. Figure 4 illustrates the finalized JH-SPHM Guide with a blank column for staff to write names of locally available equipment for reference.
The Johns Hopkins Safe Patient Handling Mobility Guide
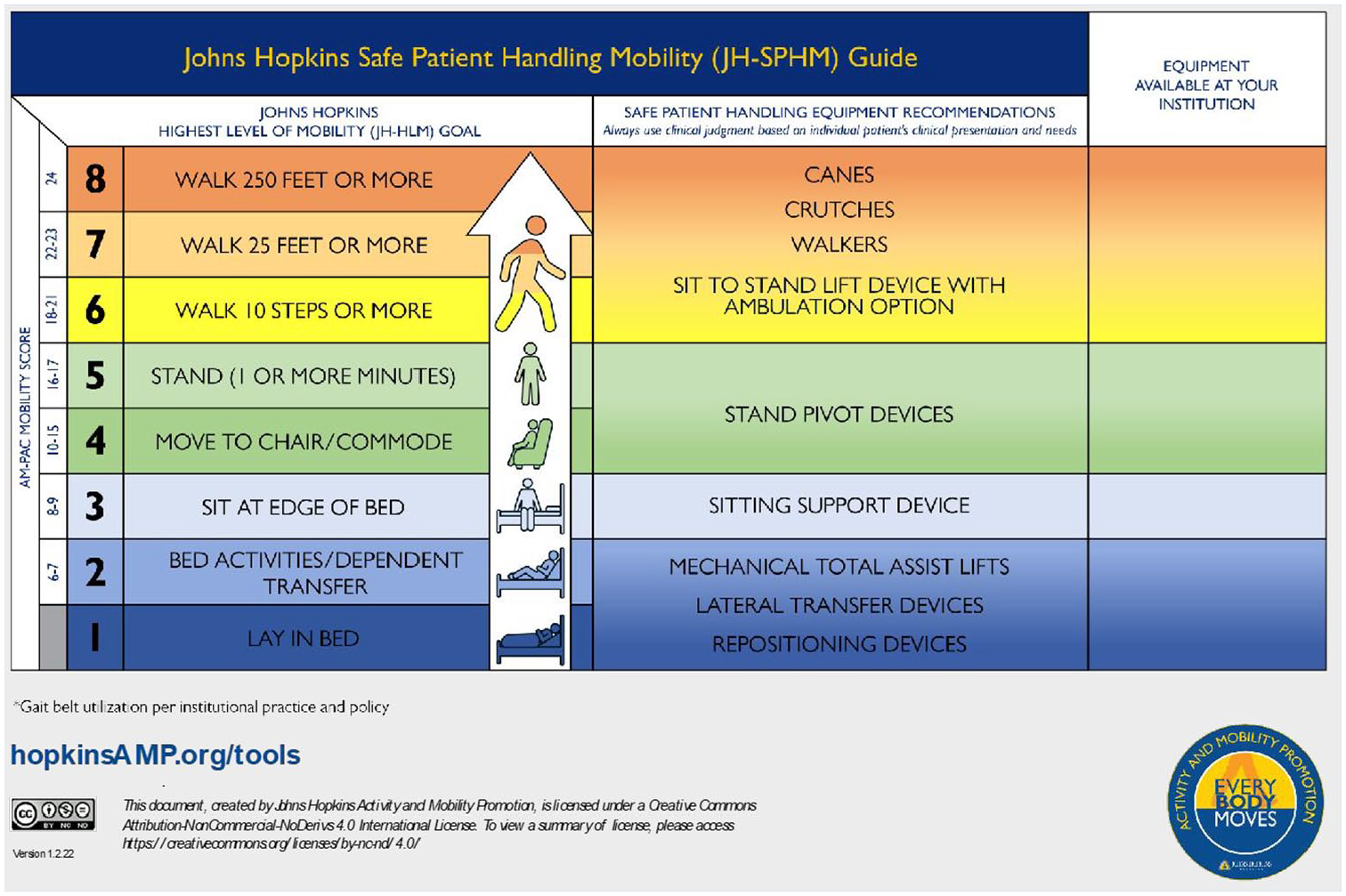
The Johns Hopkins Safe Patient Handling Mobility Guide With Blank Column for Institution Specific Equipment
Clinical Testing of the JH-Safe Patient Handling Mobility Guide
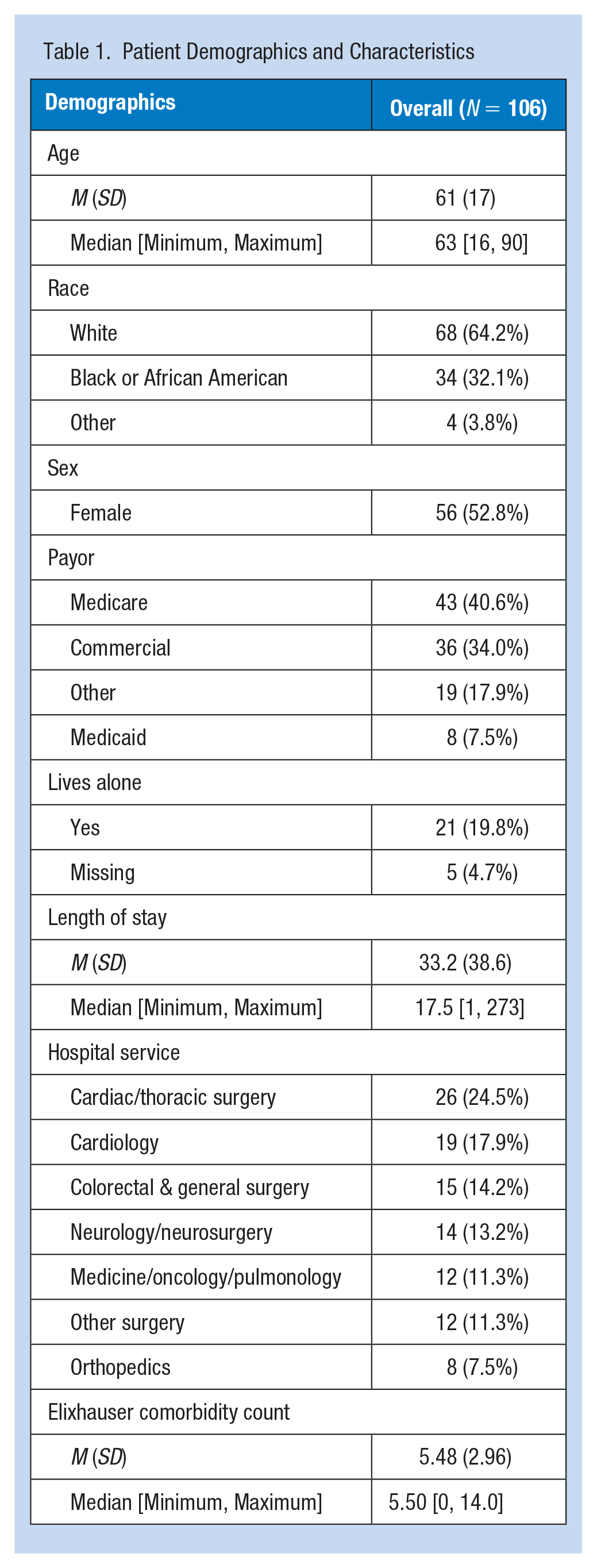
The agreement between therapist-documented recommendations and recommendations made by the Guide has been depicted in Table 2. There were 106 unique patients seen for a total of 125 routine physical therapy sessions, thus, some patients were seen for multiple sessions. Patients were admitted to intensive and non-intensive care settings (Table 1). Patients in our sample had a mean length of stay of 33.2 days (SD: 38.6). Hospital service lines included cardiac and thoracic surgery (24.5%), cardiology (17.9%), colorectal and general surgery (14.2%), and others (11.3%). Patients were aged an average of 61 years. Slightly greater than one-half were female (52.8%). Approximately two-thirds were White (64.2%). Patients were primarily insured by Medicare (40.6%) or commercial insurance (34.0%). Patients had an average of 5.48 comorbidities according to the Elixhauser comorbidity count.
Patient Demographics and Characteristics
The JH-Safe Patient Handling Mobility Guide groups AM-PAC scores as 6–7, 8–9, 10–15, 16–17, and 18–24, as AM-PAC Mobility Short Form scores range from 6 to 24 (Figure 3). AM-PAC 6-Clicks scores for the patients included in clinical testing were aligned in Table 2 to match the structure of the JH-Safe Patient Handling Mobility Guide. The highest agreement was observed between the physical therapists’ recommendations and JH-Safe Patient Handling Mobility Guide recommendations of AM-PAC 6-Clicks scores between 18 and 24. For AM-PAC 6-Clicks scores of 16–17, JH-Safe Patient Handling Mobility Guide recommendations agreed or were more conservative than therapist recommendations for all patients (Table 2). Overall, the recommendations of the JH-Safe Patient Handling Guide agreed with the therapist’s recommendations for 70.4% of patients. The Guide agreed or was more conservative than the therapist’s recommendations 96% of the time. The percentage of agreement subsequently varied based on AM-PAC 6-Clicks values, with the highest agreement seen for AM-PAC 6-Clicks values of 18 to 24. For AM-PAC 6-Clicks scores between 10 and 15, the lowest percentage of agreement was observed (34.5%), with JH-Safe Patient Handling Mobility Guide recommendations reflecting more conservative options than therapist recommendations. For AM-PAC 6-Clicks scores of 8–9 and 6–7, JH-Safe Patient Handling Mobility Guide recommendations were comparatively more conservative.
Agreement Between Physical Therapist-Documented Recommendations and JH-Safe Patient Handling Mobility Guide (N = 125)
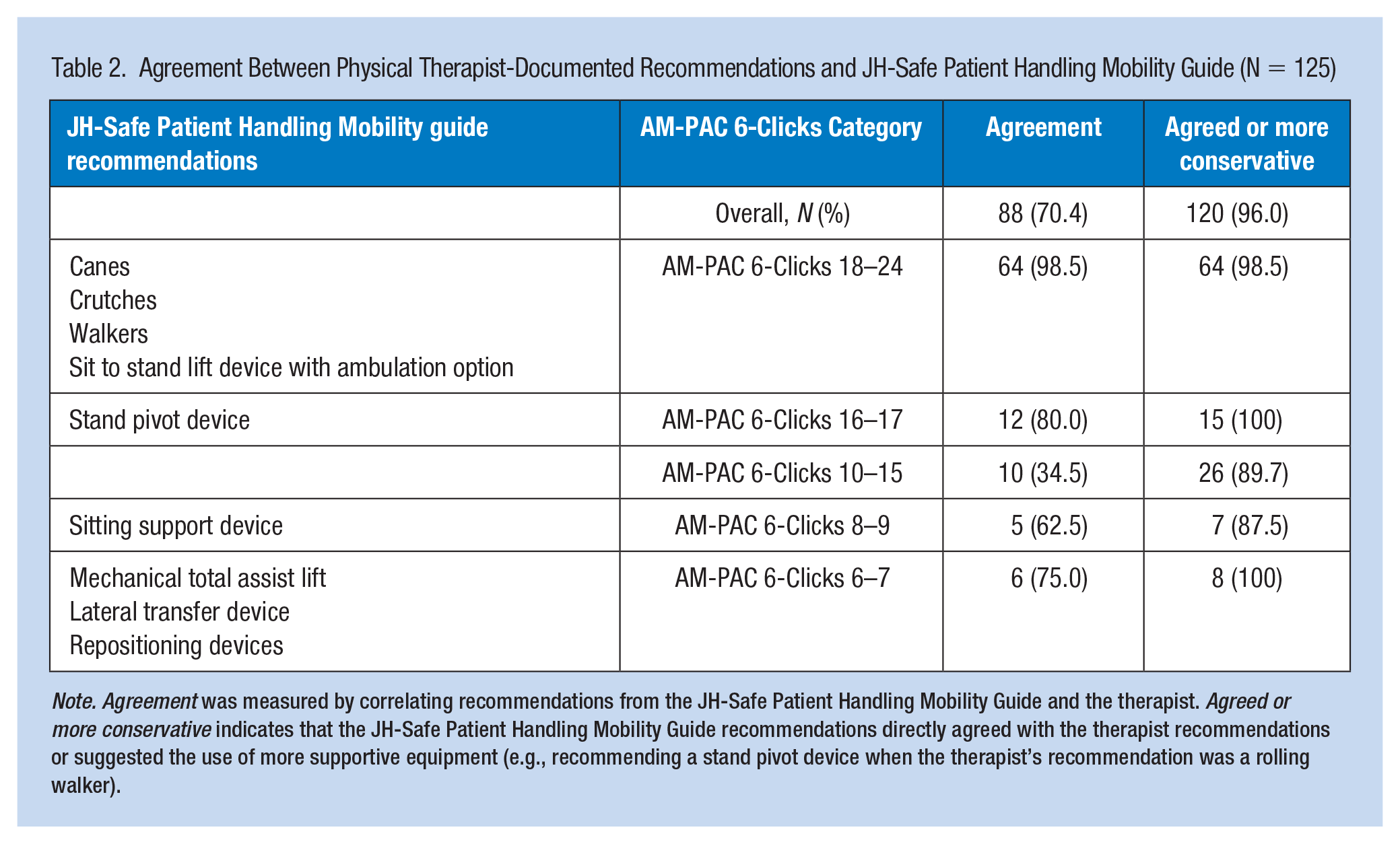
Note. Agreement was measured by correlating recommendations from the JH-Safe Patient Handling Mobility Guide and the therapist. Agreed or more conservative indicates that the JH-Safe Patient Handling Mobility Guide recommendations directly agreed with the therapist recommendations or suggested the use of more supportive equipment (e.g., recommending a stand pivot device when the therapist’s recommendation was a rolling walker).
Discussion
In this study, we detailed the creation of a tool that combines the overlapping goals of promoting mobility and informing the appropriate use of SPH equipment. Through input from an expert consensus panel, which included nurses, physical and occupational therapists, and members of the hospital safe patient-handling and falls committee, we observed that SPH equipment recommendations could be mapped to the levels of the JH-Mobility Goal Calculator. The resulting tool, the JH-Safe Patient Handling Mobility Guide, is now a free resource within the JH-AMP Tools User Manual, available to health care systems at HopkinsAmp.org. To our knowledge, there is no other tool that efficiently combines a mobility capacity assessment, a mobility goal, a mobility performance assessment, and the equipment likely to be required to reach that mobility goal. Through completion of real-world testing, a high agreement was found between therapist-recommended equipment and equipment recommendations depicted by the JH-Safe Patient Handling Mobility Guide with a mobility goal greater than JH-HLM of 6.
The JH-Safe Patient Handling Mobility Guide has several important clinical implications. First, providing staff with a quick guide to SPH equipment selection is likely to improve the confidence of staff when selecting equipment, who may otherwise be hesitant to mobilize patients with mobility problems. This has been listed as a barrier to nurse-led mobilization during previous studies, and we anticipate that reducing this barrier may allow for greater mobilization of hospitalized patients (Anekwe et al., 2019; Hoyer et al., 2015; Young et al., 2018). The guide facilitates a synergistic relationship between patient safety and mobility for clinical staff. This is important as these two important aspects of patient care are often viewed as competing priorities (Growdon et al., 2017). Using appropriate SPH equipment has been reported to decrease the risk of patient and staff injury during patient transfers and mobilization (Nelson et al., 2006; Powell-Cope et al., 2014). While it is always important to protect the physical health of nursing staff, it is especially important during times when there is a shortage of nursing staff such as experienced during the COVID-19 pandemic (Gorges & Konetzka, 2020; Mhawish & Rasheed, 2022; Xu et al., 2020). Given this shortage, hospitals are likely to face challenges meeting staffing requirements should any of their nursing staff miss prolonged periods of work time due to injuries they experience on the job. Team members responsible for occupational health and safety in the hospital play an important role in proactively preventing musculoskeletal injuries associated with patient handling. They should be engaged to coordinate the identification of site-specific equipment corresponding with levels of the JH-Safe Patient Handling Mobility Guide and then facilitate implementation of routine tool use that promotes safe patient mobility.
A recent study found that 83.3% of patients surveyed felt that early mobility was a helpful component of recovery, and 69.2% agreed or strongly agreed that early mobility should be routinely performed (Najjar et al., 2022). Daily nursing assessment of AM-PAC 6-Clicks suggests a minimum mobility goal for the patient which helps the nursing staff to promote goal-oriented mobility that can be easily integrated into daily care activities. Once the goal is set, the JH-Safe Patient Handling Mobility Guide provides the SPH equipment recommendations that can then assist nursing staff in identifying appropriate equipment to help patients meet their mobility goals safely. Furthermore, the AM-PAC 6-Clicks is already used routinely in many hospitals, meaning that it may not require any additional assessments to be completed by nursing staff.
It has been reported that goal-directed mobility improved mobility-related outcomes in hospitalized patients (Heinzmann et al., 2022). BMAT provides SPH equipment recommendations based on the mobility level performed which could often be restricted by patient-related factors such as pain or refusal. Alternatively, the JH-Mobility Goal Calculator sets a target goal for mobility based on the patient’s AM-PAC 6-Clicks score, and adding SPH equipment recommendations to the JH-Mobility Goal Calculator through the JH-Safe Patient Handling Guide allows the clinician to implement a plan that integrates and facilitates mobility goal achievement safely.
During clinical testing, there was a high agreement overall between JH-Safe Patient Handling Mobility Guide recommendations and therapists’ equipment recommendations. The lowest agreement was observed at AM-PAC 6-Clicks scores of 8–15 where the JH-Safe Patient Handling Mobility Guide recommendations were comparatively more conservative (e.g., the therapist recommended a walker, but the JH-Safe Patient Handling Mobility Guide recommended a standing aid). Although good agreement was seen across multiple AM-PAC 6-Clicks values, more conservative recommendations were made by the JH-Safe Patient Handling Mobility Guide for some patients. A more conservative recommendation indicates a more restrictive therapeutic device. As the JH-Safe Patient Handling Mobility Guide is intended to improve staff and patient safety, it is appropriate that when a perfect agreement was not observed, the difference was in the direction of more conservative recommendations by the new tool. It should also be noted that the recommendations were made by physical therapists, who may feel more confident in mobilizing patients with mobility difficulties using less supportive equipment compared with the nursing staff. This was also observed during Rounds 1 and 2 of expert panel discussions with nursing panel members sharing similar concerns.
Limitations
Like all work, ours has some limitations. The newly developed JH-Safe Patient Handling Mobility Guide was created using a modified Delphi framework with expert recommendations from various disciplines. Our panel of experts was a diverse group with representation from different areas of practice and leadership from different institutions; however, as a sample of convenience, they may not represent the views of all potential experts. Our experts did not include nursing assistants, who are often involved in lifting or moving patients, and did not include patients, who are important stakeholders in the utilization of SPH equipment. During Round 2 of the expert panel discussion, two experts were unable to attend the video conference; therefore, viewing the recorded discussion may have impacted their recommendations. The JH-Safe Patient Handling Mobility Guide is built onto the existing JH-Mobility Goal Calculator; therefore, using this guide would require institutions that do not use the JH-Mobility Goal Calculator currently to adopt it. In addition, future studies will be needed to examine the tool in other patient populations in different hospitals.
Future Research
Future research on this tool will need to evaluate its effectiveness on staff confidence, staff satisfaction, patient satisfaction, staff injuries, patient falls, or other mobility-related adverse events. An association was identified between impaired patient mobility and increased risk of injury to clinical staff (McLaughlin, Young, et al., 2023). SPH programs were identified as significantly decreasing health care worker injury rates (Teeple et al., 2017). Education and training in simulated environments should reinforce the utilization of these tools (L. Klein & Kumble, 2022). A reduction in recorded neck and shoulder-related injuries was found after the incorporation of a safe patient-handling and mobilization program in a direct comparison of two hospitals, one with an SPHM program, and one without (Dennerlein et al., 2017). Multiple prior studies have highlighted a reduction in staff injury through the use of safe patient-handling equipment and incorporation of SPH programs (Abdul Halim et al., 2023; Powell-Cope et al., 2014). These areas need to be further studied to fully understand the clinical utility of the JH-Safe Patient Handling Mobility Guide in routine clinical practice.
Implications for Occupational Health Practice
Promoting patient mobility that is safe for providers and patients is a high priority in the inpatient setting. Using a modified Delphi approach with a diverse group of experts, we have created the JH-Safe Patient Handling Mobility Guide. The newly created JH-Safe Patient Handling Mobility Guide provides evidence-based safe patient-handling equipment recommendations for frontline nursing staff to facilitate patient mobility while ensuring the safety of patients and staff.
Applying Research to Occupational Health Practice
Patient mobility in the hospital setting must maximize both patient and nursing staff safety. With input from a panel of experts including frontline nurses, nurse leaders, and rehabilitation therapists, the JH-Safe Patient Handling Mobility Guide was created through a modified Delphi approach. Guide recommendations were then validated during routine care of hospitalized patients. The new guide provides evidence-based equipment recommendations for frontline nursing staff to readily implement with hospitalized patients and prevent work-related musculoskeletal injuries.
Supplemental Material
sj-docx-1-whs-10.1177_21650799241268745 – Supplemental material for Development of a New Tool to Combine the Promotion of Patient Mobility With Safe Patient Handling Equipment: The Johns Hopkins Safe Patient Handling Mobility (JH-SPHM) Guide
Supplemental material, sj-docx-1-whs-10.1177_21650799241268745 for Development of a New Tool to Combine the Promotion of Patient Mobility With Safe Patient Handling Equipment: The Johns Hopkins Safe Patient Handling Mobility (JH-SPHM) Guide by Sowmya Kumble, Kevin H. McLaughlin, Karli Funk, Steven Dekany, Daniel Ludwig, Holley Farley, Anita M. Stone, Nozomi Tahara, Erica Newkirk, Erik Hoyer and Daniel L. Young in Workplace Health & Safety
Supplemental Material
sj-xlsx-2-whs-10.1177_21650799241268745 – Supplemental material for Development of a New Tool to Combine the Promotion of Patient Mobility With Safe Patient Handling Equipment: The Johns Hopkins Safe Patient Handling Mobility (JH-SPHM) Guide
Supplemental material, sj-xlsx-2-whs-10.1177_21650799241268745 for Development of a New Tool to Combine the Promotion of Patient Mobility With Safe Patient Handling Equipment: The Johns Hopkins Safe Patient Handling Mobility (JH-SPHM) Guide by Sowmya Kumble, Kevin H. McLaughlin, Karli Funk, Steven Dekany, Daniel Ludwig, Holley Farley, Anita M. Stone, Nozomi Tahara, Erica Newkirk, Erik Hoyer and Daniel L. Young in Workplace Health & Safety
Footnotes
Acknowledgements
The authors acknowledge Lydia Vincent, PT, DPT, for her assistance with clinical testing.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.