
Abstract
Background:
Few studies are dedicated to understanding the extent and impact of sexual harassment among medical students. The aim of this study was to use behaviorally specific measures to examine prevalence of sexual harassment toward medical students. Associated mental health and academic impacts were also studied.
Methods:
A multisite survey was conducted at four medical schools. Sexual harassment was measured using the Sexual Experiences Questionnaire (SEQ), a valid and reliable instrument. Students were also surveyed about depressive and post-traumatic stress disorder (PTSD) symptoms and their level of academic engagement. We also assessed their perceptions of institutional response and whether they felt safe at their institution.
Findings:
The final sample included 524 medical students (response rate = 13%). Findings revealed that 36.6% reported sexual harassment by a faculty/staff member and 38.5% reported harassment by a fellow student. The odds of harassment by faculty/staff, as well as peers, were significantly higher for women with an adjusted odds ratio (AOR) = 9.83, 95% confidence interval (CI) = [3.74, 25.80] and multiracial students with an AOR: 2.93, 95% CI: [1.16, 7.39]. Those who experienced sexual harassment were more likely to report academic disengagement and symptoms of depression and PTSD.
Conclusion/Application to Practice:
Sexual harassment in medical schools can potentially limit a student’s academic success and negatively impact their mental health. Supportive services and efforts to address peer and professional cultures that promote harassment are needed. Experiences of harassment require swift and competent responses by medical school leadership in collaboration with occupational and/or student health services to mitigate detrimental impacts and support medical students throughout their training.
Keywords
Introduction
The proportion of women in medicine now exceeds 50% (Boyle, 2019; Sklar, 2016), and the increased focus on addressing gender and sexual harassment in universities nationally (National Academies of Sciences, Engineering, and Medicine [NASEM], 2018; White House Task Force to Protect Students from Sexual Assault, 2014) suggests that medical students’ sexual harassment experiences merit further investigation. Over the past several decades, research has indicated sexual harassment prevalence in medical schools is high (Fnais et al., 2014; Mavis et al., 2014) despite efforts to decrease sexual harassment and negative outcomes (Fried et al., 2012). Moreover, a recent report from the NASEM, using data from the present study, indicated that female medical students were 220% more likely to experience sexual harassment perpetrated by faculty and staff than female non-science, engineering, and math students (NASEM, 2018). Under Title IX of the Education Amendments of 1972 (United States Department of Education Office for Civil Rights [OCR], 2011) universities in the United States have a responsibility to provide students an education free from sex discrimination and harassment (OCR, 2011; Recupero et al., 2004). Due, in part, to the rise in student advocacy concerning institutional responses to Title IX violations, and with support from the Obama administration, sexual harassment and violence has continued to receive high media attention (Brubaker, 2019; Holland et al., 2019; Manning, 2018).
Prevalence of Sexual Harassment in Medical Schools
Medical students’ experiences of sexual harassment have been investigated in several studies using various methodological approaches (Fnais et al., 2014). While the field has witnessed some recent advancements, methodological inconsistencies impact the ability to determine an accurate prevalence of sexual harassment among medical students (A. F. Cook et al., 2014; Premadasa et al., 2011). For example, several studies have used different constructs to define and measure harassment such as belittlement, psychological abuse, physical abuse, sexual abuse, sexual harassment, and mistreatment, limiting the ability to compare findings across studies (Fnais et al., 2014; Frank et al., 2006; Mavis et al., 2014). Early approaches to measuring sexual harassment relied on a single item (Mangus et al., 1998), whereas other researchers used self-constructed instruments with unknown psychometric properties (Bursch et al., 2013; Maida et al., 2003). Rees and Monrouxe (2011) critiqued the sexual harassment questionnaires used in medical education research, calling them “fairly unsophisticated” and “providing little information to facilitate cultural change” (p. 1374). Of the few studies that have used reliable, validated tools, questions were preceded by various and often narrow definitions of sexual harassment or gender discrimination (Nagata-Kobayashi et al., 2009; Stratton et al., 2005), which bounds experiences by their definition rather than capturing specific behaviors that comprise sexual harassment.
The importance of behaviorally specific measurement tools for victimization has been underscored in violence research (Fisher et al., 2010; Rennison & Addington, 2014; Wood et al., 2016). In their seminal study on the theoretical and psychometric advances in measuring sexual harassment, Fitzgerald et al. (1995) advised that it is important to avoid using the actual term “sexual harassment” due to differences in perceived meaning; therefore, best practices in measurement are to use behaviorally specific questions. The Sexual Experiences Questionnaire (SEQ; Fitzgerald et al., 1995) includes a behaviorally specific approach to measuring harassment and has been used in workplace, military, and college campus settings (Chan et al., 2008; Street et al., 2008). For college settings specifically, the Administrator Researcher Campus Climate Collaborative (ARC3) survey was developed through collaborative efforts by sexual harassment and sexual assault researchers, campus administrators, students, campus advocates, law enforcement, and legal affairs to measure campus climate using the best scientific evidence (ARC3, 2016). Recently, Pennsylvania State University administered the ARC3 survey, which includes the SEQ, at their College of Medicine and found that 50.4% of women and 32.6% of men reported at least one incident of faculty/staff-perpetrated sexual harassment (Penn State Student Affairs, 2016). The current study used the same valid and reliable measure (SEQ) to measure sexual harassment among medical students, while also building upon our current understanding of student experiences with further analysis.
There has been a considerable amount of evidence addressing the risk of sexual harassment among students; however, there is a gap in the extant literature relative to understanding the extent of victimization associated with sexual harassment experiences of medical students. Similar to Wood et al. (2018) and Kammer-Kerwick et al. (2019), the current study addresses this gap by operationalizing the extent of sexual harassment victimization as the number (or count) of sexually harassing behaviors endured since enrolling in medical school perpetrated by peers, faculty, and/or staff. The study also explores an additional gap in extant literature by examining mental health and academic outcomes among medical students and the impact of sexual harassment victimization on these outcomes. The purpose of this study was to examine the predicted risk and extent of sexual harassment among medical students perpetrated by faculty/staff members and student peers as well as correlated mental health and institutional outcomes.
Methods
We used a cross-sectional design and validated measures to examine prevalence and extent of sexual harassment experienced by students since enrollment in medical school. Four medical schools from a southwestern U.S. state were included in the study. In addition, correlated impacts including mental health outcomes and perceptions of institutional response and safety were explored.
Participants and Procedure
An anonymous online survey link was sent to all enrolled students in fall 2015 at four accredited Texas medical schools (a total of 4,056 students) via Qualtrics over a 5-week period, with four follow-up reminders. The survey was implemented with the support of president appointed stakeholders at each of the medical schools who worked in collaboration with the research team to obtain student emails through the registrar and support recruitment efforts. Participants were eligible for incentive drawings, which varied across institutions (e.g., parking passes, gift cards, cash prizes), by clicking on a new incentive survey link at the end of the survey that separated their contact information from their survey responses to maintain anonymity. Incentives were funded by each individual institution and drawing winners were selected by the institutional stakeholders (Busch-Armendariz et al., 2017b). The study was approved by the University of Texas at Austin’s Institutional Review Board (IRB).
Data collection
We used a modified version of the ARC3 survey (2016; see Busch-Armendariz et al., 2017b for complete methods report and modifications) that in turn uses the SEQ to assess sexual harassment. Demographic questions were adapted from the Johns Hopkins “It’s on Us” survey to increase diversity options for gender identity and sexual orientation (Campbell et al., 2017). Demographic questions included race/ethnicity, gender, sexual orientation, age, and year in school. Students were only asked to answer questions about experiences since enrollment at their current institution. Time at institution was measured as years since enrollment. For sexual orientation, participants indicated whether they were heterosexual, gay, lesbian, bisexual, asexual, queer, or a sexual orientation not listed; due to small sample sizes, sexual identities other than heterosexual were categorized as sexual minority.
Sexual harassment
Sexual and gender harassment was measured with a modified version of the Department of Defense Sexual Experiences Questionnaire (SEQ-DoD; Cortina et al., 2002; Fitzgerald et al., 1995). Using a 6-point scale (never, once, twice, sometimes, often, and many times), participants were asked about sexual harassment perpetrated by faculty/staff. Sixteen questions assessed four subscales on the SEQ-DoD: sexist gender harassment (e.g., displayed, used, or distributed sexist or suggestive materials), crude gender harassment (e.g., made unwelcome attempts to draw you into a discussion of sexual matters), unwanted sexual attention (e.g., continued to ask you for dates, drinks, dinner, even though you said “no”), and sexual coercion (e.g., made unwanted attempts to stroke, fondle, or kiss you). Using the same scale range above, participants were then asked 12 questions about these experiences with student peers. The study included a novel measure of sexual harassment via electronic communication (e.g., spread unwelcome sexual rumors about you by text, email, Facebook, or other electronic means). The extent of harassment was operationalized by calculating the sum of sexually harassing behaviors endured across all items separately for each scale (faculty/staff and peer, respectively) and for both scales combined (total). We described the study methodology and reported findings about the risk and extent of sexual violence and sexual harassment endured by students at academic institutions (Busch-Armendariz et al., 2017a; Kammer-Kerwick et al., 2019; Wood et al., 2018). We intentionally used extent instead of severity due to the subjective appraisal of severity (Cortina et al., 2002; Wright & Fitzgerald, 2007). The faculty/staff and student versions of the SEQ-DoD achieved reliability levels (Cronbach’s alpha) of .80 and .85, respectively.
Outcome measures
The ARC3 measured mental health (post-traumatic stress disorder [PTSD], depression) and academic environment (disengagement, safety, and perceptions of institutional response to intimate and interpersonal violence) impacts.
Depressive symptoms were measured with the 10-item Center for Epidemiological Studies Depression Scale (CES-D; Eaton et al., 2004; Radloff, 1977). Students were asked to indicate how often (rarely or none of the time [less than 1 day] through all of the time [5–7 days/week]) they felt or behaved in ways listed in the scale during the past week (e.g., I was bothered by things that usually don’t bother me; I felt depressed; my sleep was restless). Total scores were calculated using the sum of all items; scores ≥10 were considered symptomatic of depression, consistent with instrument design (Cronbach’s α = .67).
PTSD was measured using the 4-item Primary Care PTSD Screen (PC-PTSD; Prins et al., 2003) to assess the past month’s PTSD symptoms (e.g., had horrible nightmares about it or thought about it when you did not want to; felt numb or detached from others, activities, or your surroundings). Students were asked to answer yes/no (and those who answered “yes” to any three of the items screened positive for potential PTSD; otherwise, they were coded as “no”; Cronbach’s α = .83).
Satisfaction with institutions was measured using 2 items from the Scale of Academic Satisfaction were also used (Lent et al., 2007), in which students were asked whether they would recommend attending their university to others, and whether they had to do it over again would they still attend their current university. A 5-point scale was used with a higher score indicating greater satisfaction with the medical student’s institution (Cronbach’s α = .88).
Academic disengagement was measured from a tool adapted for use by ARC3 (ARC3, 2016; Lent et al., 2007). Students were asked the number of times they had engaged in a range of behaviors that indicated disengagement (e.g., missed class, late for class) in the past semester at their university. The adapted measure used a 5-point scale with a calculated mean of all items; higher mean scores represent a greater degree of academic disengagement (Cronbach’s α = .64).
Perceptions of environmental/school safety was measured using an 8-item adapted version of ARC3 (2016). Students were asked, on a 5-point scale (0 = Strongly Disagree, 4 = Strongly Agree), to indicate the degree to which they agreed with statements, such as “On or around this campus, I feel safe from sexual harassment.” Higher mean scores represent a greater perception of safety from sexual violence on campus (Cronbach’s α = .68).
Perceptions of institutional response to intimate and interpersonal violence was measured using a scale adapted from Rutgers University #iSPEAK campus climate survey (McMahon et al., 2014). Students’ perceptions of institutional response were assessed using the 12-item measure that included statements such as “The institution would take the report seriously.” The perceived likelihood of each statement was indicated with a 5-point scale anchored by very unlikely (0) to very likely (4) (Cronbach’s α = .93).
Data Analysis
Descriptive statistics were used to describe the study sample which were calculated using SPSS Version 26. Frequencies, percentages, and 95% confidence intervals (CIs) were calculated to determine the prevalence of sexual harassment incurred by students. We initially constructed a hurdle model to examine the odds of victimization to sexual harassment among this student cohort as well to estimate the number (or count) of harassing behaviors endured once victimized. Hurdle models partition a process into a sequence of two stages; the first generates the first occurrence of an event of interest (the hurdle) and the second generates the reoccurrences of the event. Specifically, hurdle models include both a binary logistic regression for the hurdle and a count-based regression for reoccurrences (Kammer-Kerwick et al., 2019; Wood et al., 2018). We constructed both the risk and count stages of the hurdle model as generalized linear mixed models (GLMMs) that included random intercepts to properly account for variability across the multisite sample. Specifically, a logistic regression was used to estimate the odds of victimization (yes/no) and extent (number of times or count) of victimization by or predictors, included gender, sexual orientation, and race/ethnicity. For the model examining the extent of victimization, a truncated negative binomial regression model was specified for the count (or extent of victimization) process to mitigate over dispersion, and adjusted odds ratios (AORs) and 95% CIs were calculated to estimate risk. Years since enrollment was included as a control for cumulative time in the environment; an interaction between years and gender was also included to better control for possible differences in exposure rates between women and men. Select interactions assessed the degree of moderation of sexual orientation, ethnicity, and gender relative to predicting sexual harassment experiences.
We then examined the effects of victimization on students’ mental health using the same approach as described above. Specifically, the outcomes of PTSD, depression, academic disengagement, feelings of safety, and impressions of institutional response were analyzed separately using random intercept GLMMs, also fit with glmmTMB. In addition to victim demographics, we also examined type of perpetrator who harassed the student, as well as years since enrolling in the academic program. For categorical outcomes (PTSD), we calculated AOR and 95% CIs, and for continuous outcomes (depression, academic disengagement, feelings of safety, and impression of institutional response), we calculated linear model coefficients (b) and 95% CIs.
Results
Descriptive Summary of Analytic Sample
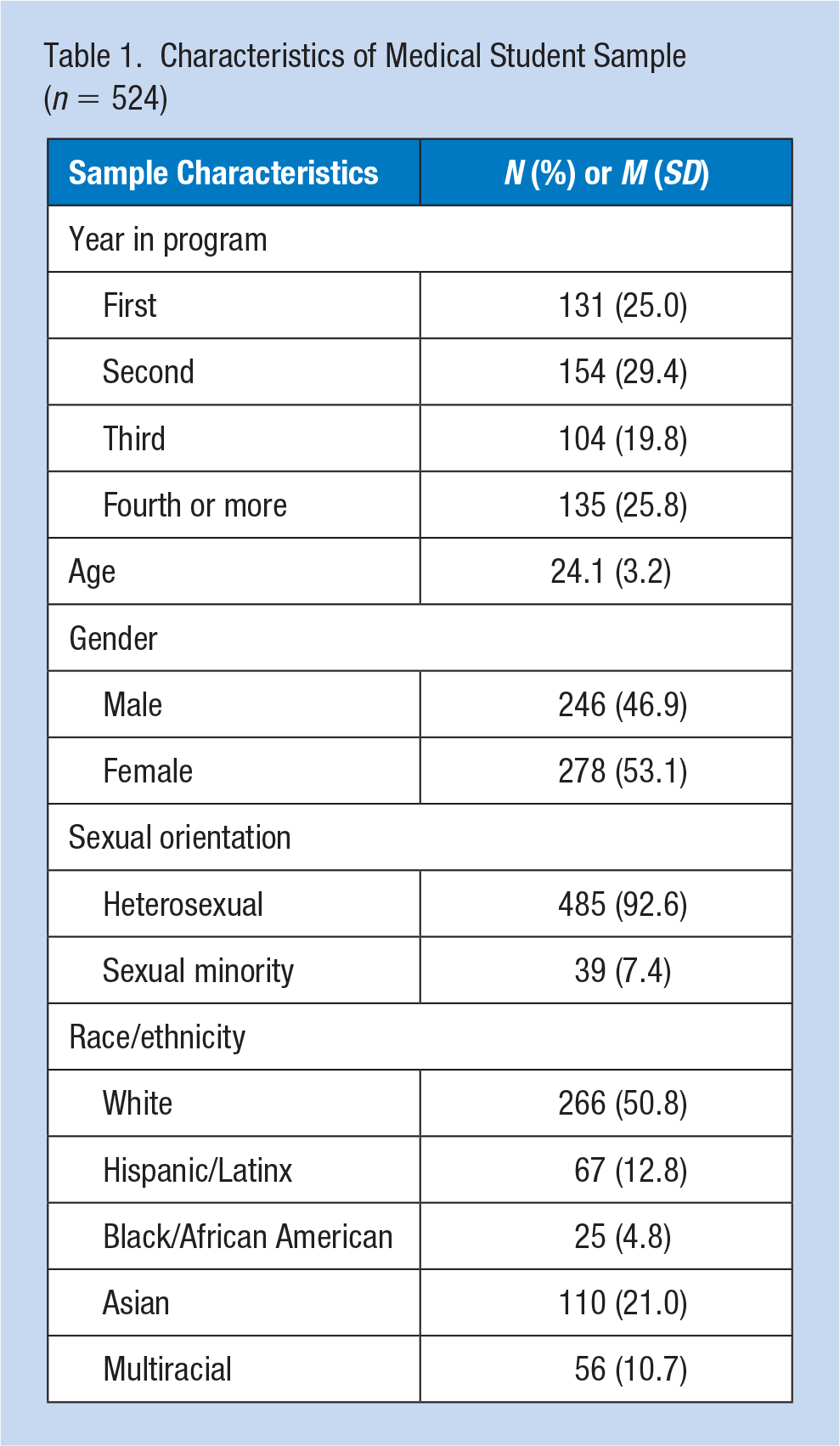
Table 1 characterizes the study sample. The study recruited 524 medical students. Institutional response rates across the four sites varied between 9% and 19%, with an average of 13%. Participants had a mean age of 24.1 years at enrollment. Year in program was distributed by year as follows: first (25.0%), second (29.4%), third (19.8%), and fourth or more (25.8%). Participants were 53.1% female, 92.6% heterosexual, and 50.8% White. Additional races and ethnicities were represented as follows: 12.8% Hispanic or Latinx, 4.8% Black/African American, 21.0% Asian, and 10.7% multiracial.
Characteristics of Medical Student Sample (n = 524)
Descriptive Summary of Prevalence
Table 2 provides the prevalence of sexual harassment. Across the four medical schools, 36.6% of students reported experiencing at least one sexual harassment behavior perpetrated by a faculty/staff member, 38.5% reported experiencing at least one sexual harassment behavior perpetrated by a student, and 51.1% had experienced some form of sexual harassment from either a member of faculty/staff or a student. Sexist gender harassment was the most frequently experienced form of sexual harassment (33.8% faculty/staff, 34.9% student, and 47.3% combined), followed by crude gender harassment (15.3% faculty/staff, 17.9% student, and 25.8.3% combined). Sexual harassment via electronic communication was reported by 8.0% of student respondents. Importantly, roughly half of students who experienced some form of sexual harassment experienced those behaviors from both faculty/staff and from students (24.0% from both, 12.6% from faculty/staff only, and 14.5% from students only; data not shown).
The Prevalence of Victimization of Faculty/Staff and Student-Perpetrated Sexual Harassment Overall and by SEQ Subscales a
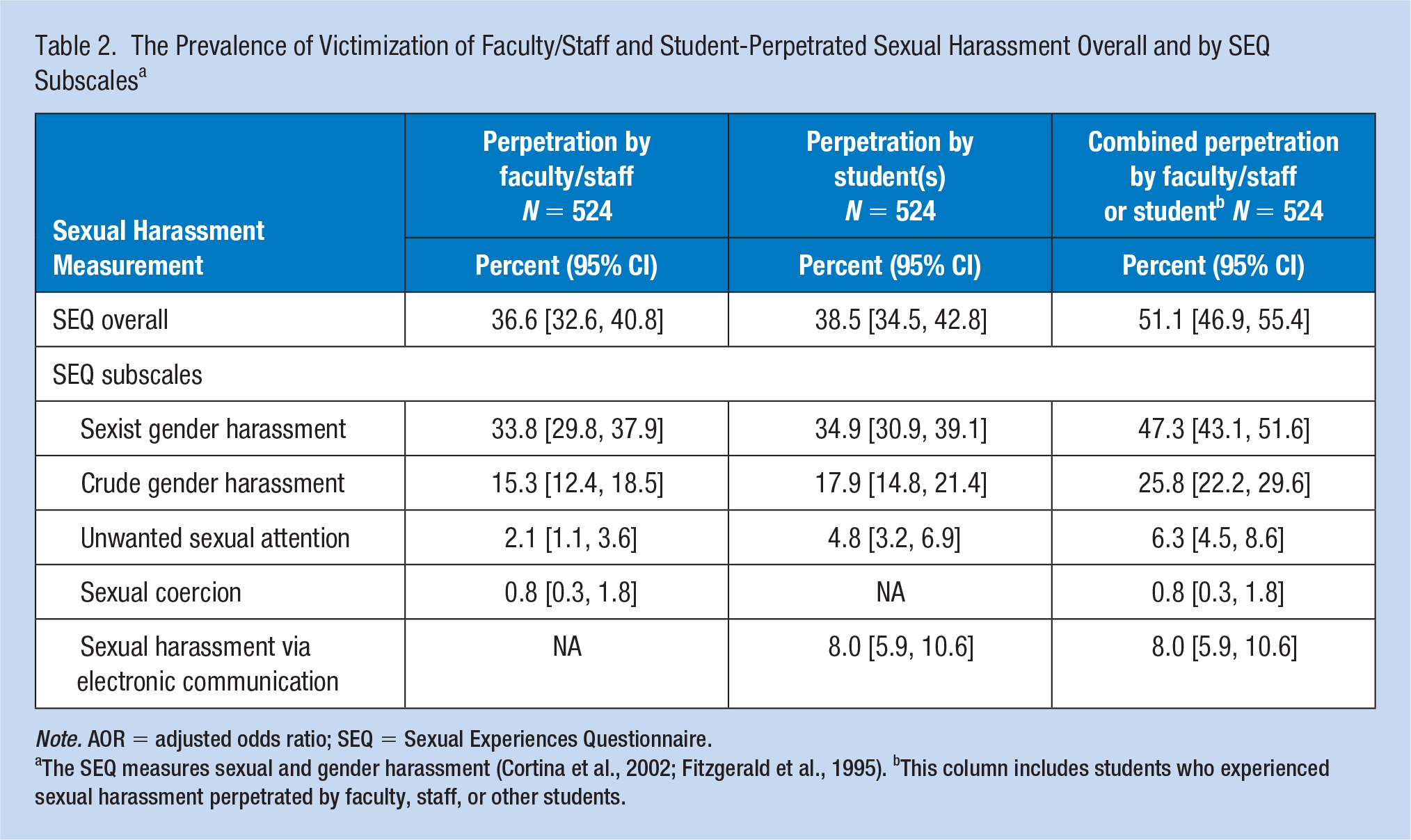
Note. AOR = adjusted odds ratio; SEQ = Sexual Experiences Questionnaire.
The SEQ measures sexual and gender harassment (Cortina et al., 2002; Fitzgerald et al., 1995). bThis column includes students who experienced sexual harassment perpetrated by faculty, staff, or other students.
Female medical students (47.1%, 50.7%) were significantly more likely than their male counterparts (24.8%, 24.8%) to report faculty/staff and student sexual harassment, respectively. Sexual minority students (51.3%) were significantly more likely than their heterosexual counterparts (35.5%) to report experiencing sexual harassment by faculty/staff. No significant differences emerged by race/ethnicity. The median number of faculty/staff-perpetrated sexual harassment behaviors was 4.0, with an average of 5.7 behaviors (data not shown). The median number of students-perpetrated sexual harassment behaviors was 6.0 with an average of 7.7. Of the faculty/staff-perpetrated sexual harassment incidents that had the greatest impact, students identified the perpetrator as male in 88.2% of cases, with the majority of incidents occurring on campus (81.9%) and involving a faculty member (67.1%). The remaining 32.9% of perpetrators were student employees (18.5%) and staff (14.5%). Of the student-perpetrated sexual harassment incidents that had the greatest impact, 90.5% of perpetrators were male, with 70.7% of incidents of student-perpetrated sexual harassment occurring on campus (data not shown).
The Risk and Extent of Victimization Model
Table 3 reports the results for both the risk and extent portions of the adjusted models. Years since enrollment, as a measure of exposure during medical school, was significant with an AOR = 1.51 (95% CI = [1.21, 1.88]) and an adjusted rate ratio [ARR] = 1.38, 95% CI = [1.15, 1.66]. In addition, female medical students were at higher risk of experiencing sexual harassment relative to male students with an AOR = 9.83, 95% CI = [3.74, 25.80] and, once victimized, had a greater rate of sexually harassing experiences with an ARR = 3.24, 95% CI = [1.41, 7.44]. Multiracial students were at slightly higher risk of experiencing sexual harassment than white students, AOR = 2.93, 95% CI = [1.16, 7.39]. No interactions of race by gender were significant.
Multivariate Models of Sexual Harassment Occurrence and Extent of by Faculty/Staff and Students
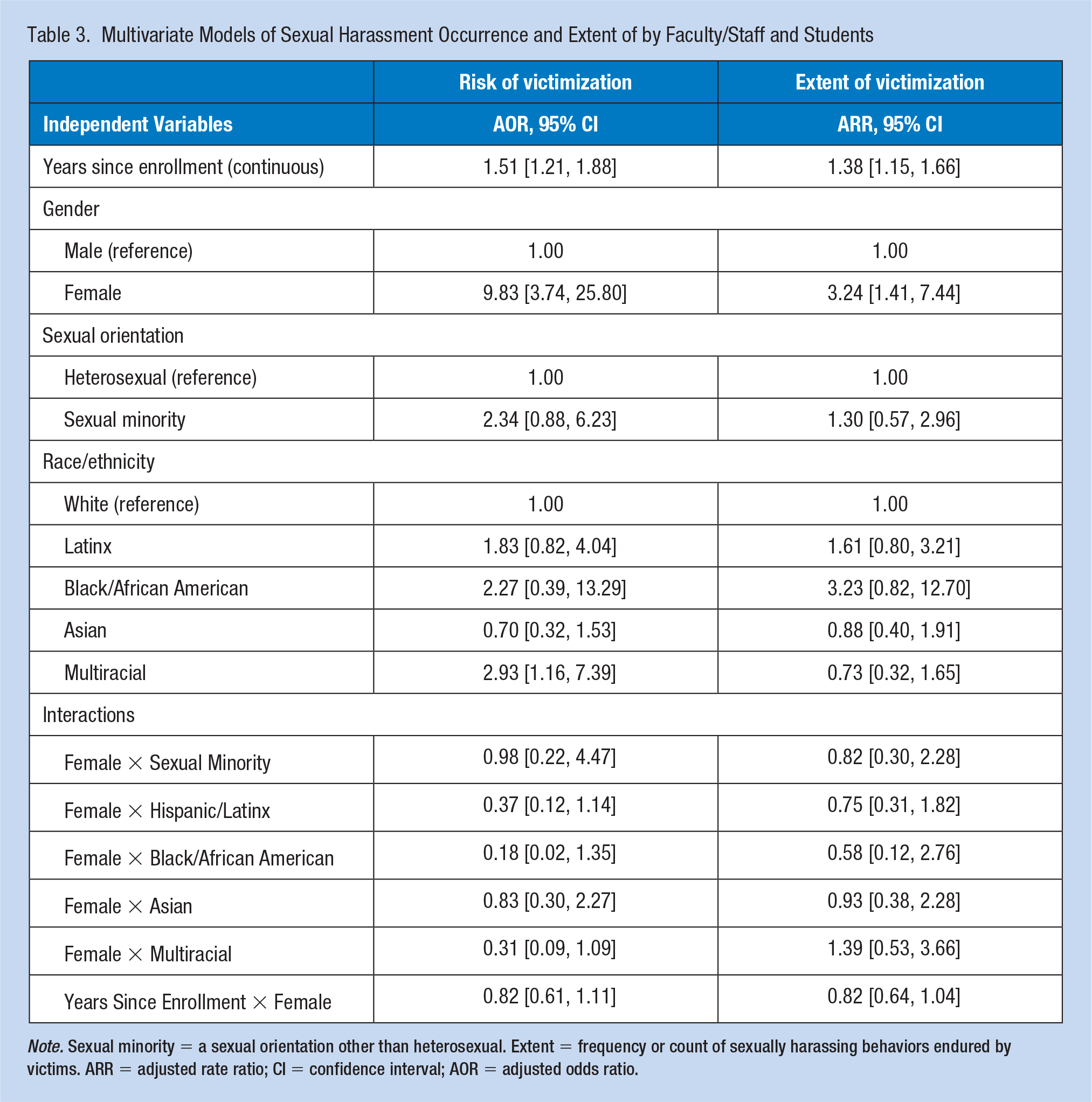
Note. Sexual minority = a sexual orientation other than heterosexual. Extent = frequency or count of sexually harassing behaviors endured by victims. ARR = adjusted rate ratio; CI = confidence interval; AOR = adjusted odds ratio.
Figure 1 summarizes the model predictions over 4 years of medical education, averaging over sexual orientation and race/ethnicity. Both the risk of experiencing sexual harassment and the total number of sexually harassing behaviors endured once initially victimized increased among students with more years in medical school. Female students were at significantly greater risk experiencing sexual harassment and, once victimized, experienced significantly more sexually harassing behaviors than their male peers.
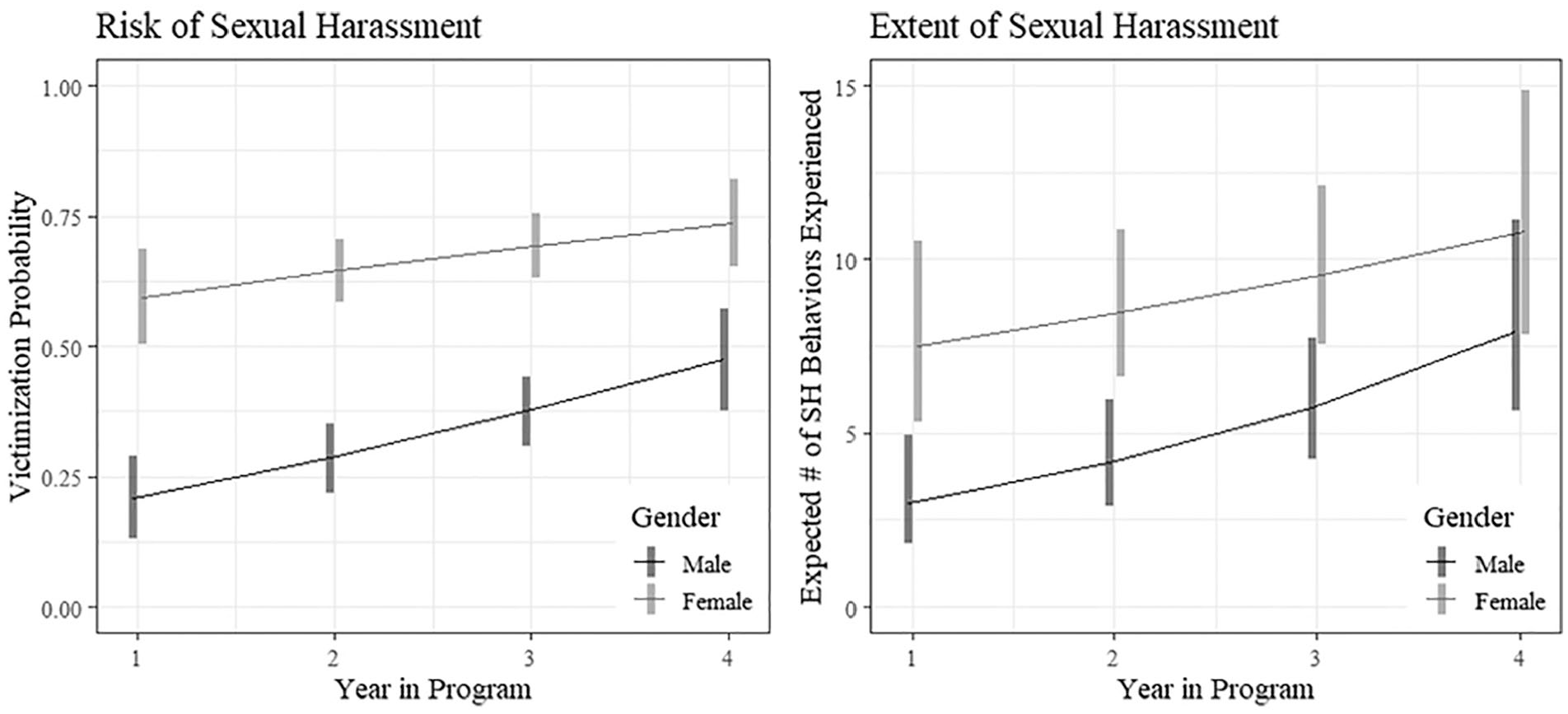
Gender difference in risk of and extent of sexually harassing behaviors as perpetrated by faculty/staff and peers.
Impact of Sexual Harassment on Mental Health and Academic Outcomes
As shown in Table 4, experiencing sexual harassment by both members of faculty/staff or by peers increased the likelihood of a positive screen for PTSD symptoms, AOR = 2.25, 95% CI = [1.10, 4.58]; increased the expected level of depression, b = 3.30, 95% CI = [2.16, 4.43]; decreased satisfaction with the institution, b = −0.40, 95% CI = [−0.56, −0.24]; increased academic disengagement, b = 0.22, 95% CI = [0.11,0.33]; decreased perceptions of safety, b = −0.16, 95% CI = [−.24, −.08]; and decreased perceptions of institutional response, b = −0.55, 95% CI = [−0.70, −0.40]. Experiencing sexual harassment from members of faculty/staff without any sexual harassment from students increased the expected level of depression, b = 1.24, 95% CI = [−0.14, 2.62], p = .077; decreased satisfaction, b = −0.25, 95% CI = [−0.45, −0.05]; and decreased perceptions of institutional response, b = −0.17, 95% CI = [−0.35, 0.02], p = .076. Experiencing sexual harassment from students without any sexual harassment from members of faculty/staff increased depression, b = 1.98, 95% CI = [0.68, 3.28], and decreased perceptions of institutional response, b = −0.19, 95% CI = [−0.36, −0.01].
Multivariate Models of the Effects of Sexual Harassment Victimization on Mental Health and Academic Outcomes Among Medical Students (- = 524)
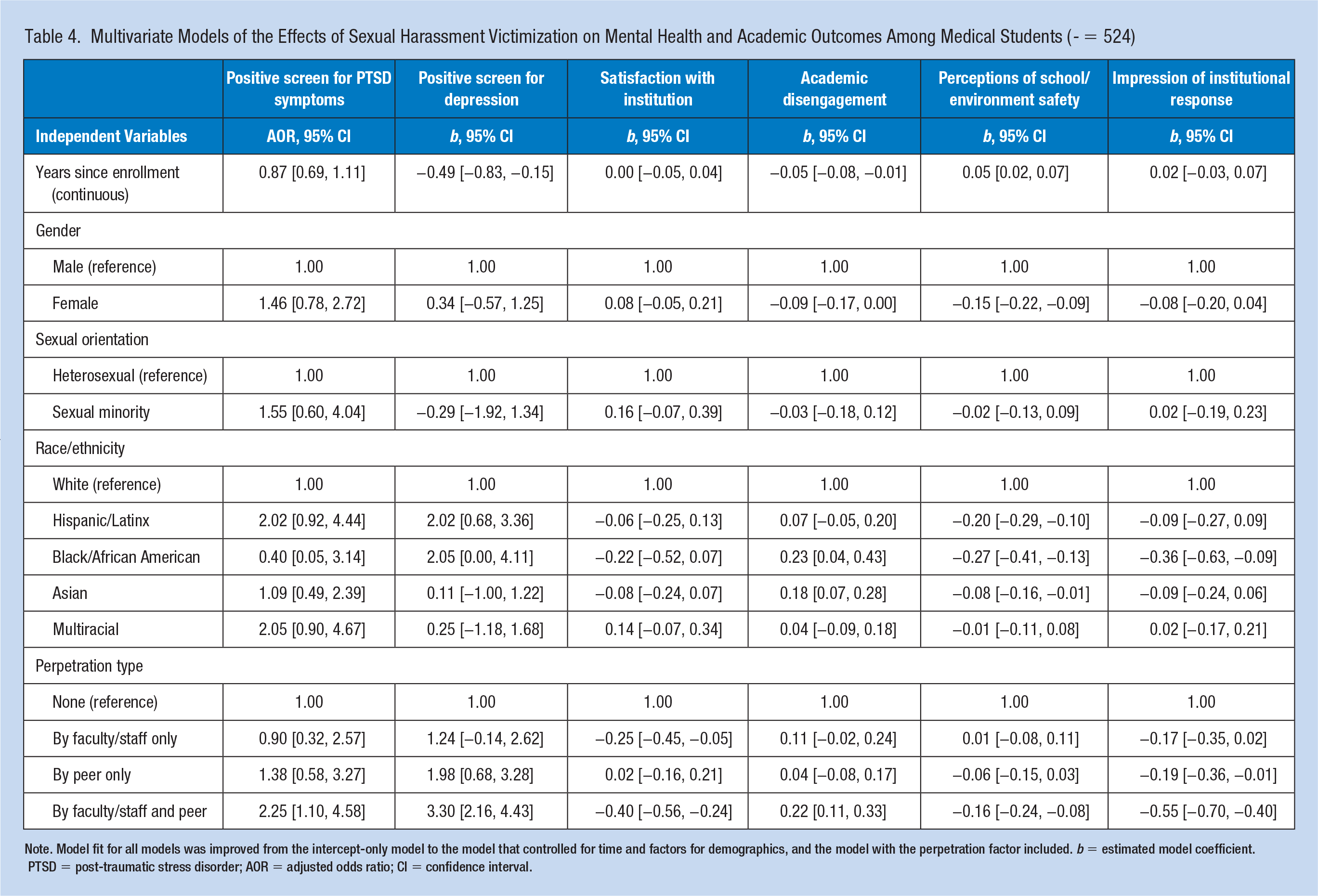
Note. Model fit for all models was improved from the intercept-only model to the model that controlled for time and factors for demographics, and the model with the perpetration factor included. b = estimated model coefficient. PTSD = post-traumatic stress disorder; AOR = adjusted odds ratio; CI = confidence interval.
It is worth noting that independent of enduring any sexually harassing behaviors, women had greater academic disengagement and lower perceptions of safety than men. In addition, independent of enduring sexually harassing behaviors, having a minority racial/ethnic status also corresponded with worse outcomes on several measure compared with White medical students.
Discussion
Medical students experience high rates of sexual harassment perpetrated by faculty/staff members and student peers. The most significant risk factor for experiencing sexual harassment is being female. Being multiracial or a sexual minority is also significant. Being female is also the most significant predictor of the number of sexually harassing behaviors endured. Unsurprisingly, time at the institution increased both risk for and extent of experiencing sexual harassment.
These findings confirm the gendered nature of sexual harassment and suggest future research is needed to better understand the unique experiences of each race and ethnicity collapsed into the “multiracial” category. Consistent with limited existing research (Bosmans & van der Velden, 2017; Huerta et al., 2006; Rosenthal et al., 2016; Yoon et al., 2010), students who experienced sexual harassment, relative to those who did not, reported more symptoms of depression and PTSD, were less academically engaged, and were less satisfied with their institution. This is concerning given research showing that female medical students can become marginalized by programs with unequal gendered experiences and a lack of representation and are less inclined to choose a specialty where they had experienced or observed high rates of discrimination and harassment (Hill & Vaughan, 2013; Stratton et al., 2005).
The most reported types of sexual harassment experienced were sexist gender harassment and crude gender harassment, echoing previous research about the impact of sexism and hostile environments on medical education (Fnais et al., 2014; Witte et al., 2006). The addition of electronic forms of harassment provided an initial assessment of how technology is used for harassment and points to the need for future research to explore cyber abuse among medical students. A recent report (NASEM, 2018) makes a case for a broader emphasis on micro, mezzo, and macro cultural change. Given the high endorsement of sexist gender harassment found in this study, programming to prevent harassment should use a multidimensional approach to target the range of sexual harassment behaviors. These recommendations can be applied at medical schools to reduce sexual harassment and create safer learning environments.
Strengths and Limitations
In addition to the known constraints associated with cross-sectional designs, our results should be considered in light of several limitations. The low survey response rate is a methodological challenge faced by many similar studies (C. Cook et al., 2000; Fosnacht et al., 2017). While concerns about response bias in campus violence surveys are largely unfounded (Rosenthal & Freyd, 2018), future research should strive for larger and more representative samples. The SEQ-DoD may lack sensitivity measuring intersectional experiences of sexual harassment and other forms of oppression (Cortina et al., 2002). Future iterations of this measure could better address these intersectional experiences, while also being tailored for specific populations (e.g., medical students).
Implications for Occupational Health Practice
Sexual harassment, especially sexism and sexist humor, is commonly experienced by medical students from faculty, staff, or fellow student perpetrators who are most commonly male. Findings from the current study are aligned with the findings from similar research on sexual harassment among faculty and staff at medical schools (Vargas et al., 2020) as well as research among graduate students broadly (Lorenz et al., 2019). Therefore, practitioners should be aware that sexual harassment, especially in the forms of sexism and sexist humor, is common and has broad detrimental impact on the health and success of medical students during their training. Experiencing mistreatment, including sexual harassment, has been shown to negatively impact medical students’ work satisfaction and quality of life (Gan & Snell, 2014; Kassebaum & Cutler, 1998; Nagata-Kobayashi et al., 2006; Rademakers et al., 2008) consequently increasing the potential for empathy decline, which can affect a physician’s ability to appropriately diagnose and care for patients (Neumann et al., 2011).
Interventions for sexual harassment should also be informed by the fact that minority (race/ethnicity) status is also part of the climate in medical education that is associated with similar detrimental experiences for students. As medical students continue to work in health care settings with medical and occupational health professionals, measures to prevent and address experiences of harassment are necessary for students, patients, and the workplace. Specifically, occupational health professionals who conduct investigations should be well informed of the prevalence of sexual harassment among medical students and receive trauma-informed training when dealing with victims. Education and annual policy training should also include identifying racial biases, preventive solutions, and addressing offenders of harassment, especially those with high-power differentials (Robinson, 2019). Furthermore, workplace violence policies and interventions should address the broader climate of institutional tolerance for sexual harassment in medical schools and hospitals (Walsh & Magley, 2019).
Conclusion
Sexual harassment is a pressing concern in medical school, especially for female, multiracial, and sexual minority students. Measuring prevalence and exploring predictive factors improves the understanding of sexual harassment and associated impacts, but more work is needed to create culture change and ensure safe learning environments. Supportive services and efforts to address peer cultures that promote harassment are needed. Medical school deans and other leaders must be determined to improve the institutional experiences through policy, training, and practice. In addition, they should be dedicated to building relationships with occupational health professionals in clinical settings where medical students will spend half of their education. Such culture change will improve student experiences, confidence in their career trajectories, and ultimately the provision of health care.
Applying Research to Occupational Health Practice
Sexual harassment, especially sexism and sexist humor, is commonly experienced by medical students and perpetuated by faculty, staff, and peers. Among those students victimized, about half were by both faculty/staff and students with high prevalence rates among gender and racial/ethnic minorities. The culture of medicine historically has involved mistreatment and abuse of power with low costs associated with perpetration, especially when perpetrators are disproportionately clinical clerkship faculty residents (Fnais et al., 2014). Such tolerance and lack of punitive action reinforce fundamental structures that enable and maintain opportunities for abuse and little perceived room for challenging abuse as a student. Therefore, workplace harassment interventions should address the broader climate of institutional tolerance for sexual harassment in addition to providing training for individuals grounded in culturally competent practices. Experiences of harassment require in medical students requires swift and considerate responses by academic leadership in collaboration with student and occupational health services to mitigate detrimental impacts and support medical students throughout their training.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
T’Shana McClain, MSW is a PhD student at the University of Denver Graduate School of Social Work. Her work explores alternative justice approaches for survivors of interpersonal violence and how those approaches mitigate racial/ethnic health disparities for survivors, offenders, and communities. She is a co-principle investigator of a Restorative Justice Pilot Implementation study for the Colorado Restorative Justice Council.
TMatt Kammer-Kerwick, PhD, is a senior research scientist at the Bureau of Business Research at the IC2 Institute at The University of Texas at Austin. He is the principal investigator of the study Disrupting Exploitation and Trafficking in Labor Supply Networks: Convergence of Behavioral and Decision Science to Design Interventions (NSF 2039983), which is exploring the use of stochastic multi-actor network models, reinforcement learning algorithms, and agent-based models to assess and develop disruptive interventions for labor exploitation and trafficking. He is also a co-principal investigator on projects with the Institute on Domestic Violence & Sexual Assault in the Steve Hicks School of Social Work.
Leila Wood, PhD, MSSW is an assistant professor in the Department of Obstetrics and Gynecology, Behavioral Health and Research (BHAR) team, at The University of Texas Medical Branch. Dr. Wood’s program of research focuses on college campus and community-based interpersonal violence intervention and prevention efforts.
Jeff R. Temple, PhD, is a professor, licensed psychologist, and Director of the Center for Violence Prevention at the University of Texas Medical Branch. His research focuses on interpersonal relationships, with a particular focus on adolescent relationship abuse. His work has been funded by the National Institute of Justice, National Institutes of Health, Centers for Disease Control and Prevention, and the Hogg Foundation for Mental Health.
Noël Busch-Armendariz, PhD, LMSW, MPH is a nationally recognized expert in sexual assault, human trafficking, and domestic violence. She has conducted research funded by a variety of federal and state agencies such as the National Science Foundation, Department of Justice’s, National Institute of Justice, Office of Victims of Crimes, and the Office on Violence and Women, the Texas Office of the Attorney General and the Governor of Texas, Criminal Justice Division. As IDVSA’s director, Busch strives to put her research findings into the hands of game-changers, which led to her serving as a member of the White House Task Force to Protect Students from Sexual Assault.