
Abstract
Workplace injuries, such as musculoskeletal injuries, needlestick injuries, and emotional and physical violence, remain an issue in U.S. hospitals. To develop meaningful safety programs, it is important to identify workplace factors that contribute to injuries. This study explored factors that affect injuries in a sample of newly licensed registered nurses (NLRNs) in Florida. Regressions were run on models in which the dependent variable was the degree to which the respondent had experienced needlesticks, work-related musculoskeletal injuries, cuts or lacerations, contusions, verbal violence, physical violence, and other occupational injuries. A higher probability of these injuries was associated with greater length of employment, working evening or night shifts, working overtime, and reporting job difficulties and pressures. A lower probability was associated with working in a teaching hospital and working more hours. Study findings suggest that work environment issues must be addressed for safety programs to be effective.
Keywords
Despite programs to reduce workplace injuries, they remain an issue in U.S. hospitals. Over half of all registered nurses (RNs) experience work-related musculoskeletal injuries (Gropelli & Corle, 2010). Needlestick injuries and workplace violence (emotional or physical) are also common (ALBashtawy, 2013; Wei, Chiou, Chien, & Huang, 2016). Workplace injuries create job and professional stresses, dissatisfaction, and burnout (Wang et al., 2012; Wei et al., 2016) that can culminate in leaving the profession (Sjostrom, Lopuszynski, & Bairan, 2010). Injuries also contribute to lower productivity (Butler & Johnson, 2009) due to unscheduled time off (Gropelli & Corle, 2010). Quality and safety of care may also be affected due to nurses working with injuries and personnel covering for injured workers on unfamiliar units (Charney & Schirmer, 2007). Therefore, workplace injuries are not only distressing to the nursing workforce but are also dangerous for patients, costly for the organization, and damaging to the future supply of nurses (Eatough, Way, & Chang, 2012).
For these reasons, the American Nurses Association (ANA; 2018) supports legislation to protect health care workers from injuries. The Occupational Safety and Health Administration (OSHA) and National Institute of Occupational Safety and Health (NIOSH) recommend a number of safety strategies (OSHA, n.d.-a, n.d.-b, n.d.-c, n.d.-d). Also, the Office of Disease Prevention and Health Promotion, U.S. Department of Health and Human Services (USDHHS) recognized the urgency of reducing work-related injuries in its prevention agenda Healthy People 2020 (USDHHS, 2016).
To implement meaningful safety programs, factors in the work environment that contribute to these injuries must be identified. A few research studies have identified work characteristics (e.g., workload, shift work, work hours, and overtime) as contributors to RN injuries. However, only the current study, an analysis of a large random sample of newly licensed registered nurses (NLRNs) across the state of Florida, has addressed the effect of these factors on NLRNs. The study examined the relationship between work environment factors and the incidence of workplace injuries and violence among NLRNs in Florida hospitals, controlling for NLRNs’ personal characteristics. It is the first study to examine a number of determinants simultaneously as well as the relationship between those determinants and different types of workplace injuries and violence. The authors posed a specific study hypothesis:
Literature Review
Most studies of workplace injury among RNs have focused on needlesticks, work-related musculoskeletal disorders (WMSDs), and verbal and physical violence. Needlestick injuries are reported to occur annually to semiannually in 11% of RNs (Rohde, Dupler, Postma, & Sanders, 2013); other studies report needlestick injuries occurring annually in 30% (Kasatpibal et al., 2016) to 70% (Cho et al., 2013). Newly licensed RNs are up to 2.6 times more likely to have a needlestick than experienced RNs (Yang et al., 2013), and 24% to 30% of NLRNs reported needlestick injuries in their current jobs (Stimpfel, Brewer, & Kovner, 2015).
Work-related musculoskeletal injuries affect tendons, muscles, nerves, and bursae (Eatough et al., 2012) in the back, neck, knee, foot, arm, and shoulder (Gropelli & Corle, 2011). In one survey study, 89.9% of the respondents reported some form of WMSDs during the previous 12 months (Barzideh, Choobineh, & Tabatabaee, 2014). Lower back problems were the most reported WMSD (Barzideh et al., 2014; Eatough et al., 2012).
Violence toward nurses is a worldwide problem. Verbal (emotional, nonphysical) violence appears to be more prevalent than physical (ALBashtawy, 2013; Al-Omari, 2015; Jiao et al., 2015; Pai & Lee, 2011; Roche, Diers, Duffield, & Catling-Paull, 2010; Shields & Wilkins, 2009; Wei, Chiou, Chien, & Huang, 2016). Some studies find colleagues to be the primary perpetrators of verbal violence (Celik, Celik, Agirbas, & Ugurluoglu, 2007), but other studies have reported that patients are the primary perpetrators (ALBashtawy, 2013). Patients’ relatives have also commonly been identified as the source of physical attacks (Celik et al., 2007).
Several demographic (personal) and work characteristics have been associated with these types of injuries. In the following subsections, we review these studies, including those that use the constructs of job difficulties, demands, and control. In the final subsection, we examine the particular vulnerability of NLRNs and summarize the factors that could contribute to the injuries among NLRNs assessed in this study.
Factors Associated With Needlestick Injuries
Prior studies have explored the association between demographic factors and needlestick injuries. Younger age was associated with needlestick injuries in several studies (Clarke, 2007; Rohde et al., 2013; Stimpfel et al., 2015). However, one study found that older nurses had more needlestick injuries (Martins, Coelho, Vieira, Matos, & Pinto, 2012). Females were less likely to have needlestick injuries than males in one study (Kasatpibal et al., 2016), but in other studies, gender was not significantly related (Martins et al., 2012; Stimpfel et al., 2015). The relationship between race/ethnicity and needlestick injuries has been understudied, but one study found that ethnicity was not significantly related to needlesticks (Stimpfel et al., 2015).
The relationship between needlestick injuries and education is mixed (Rohde et al., 2013; Stimpfel et al., 2015). Most studies have found that less tenure/experience was related to needlestick injuries (Cho et al., 2013; Clarke, 2007; Kasatpibal et al., 2016; Patrician, Pryor, Fridman, & Loan, 2011; Rohde et al., 2013), but one study reported the opposite finding (Martins et al., 2012).
Prior studies have also examined the relationship between work environment and needlestick injuries. Needlesticks have been found to occur more often with consecutive shifts (Hopcia, Dennerlein, Hashimoto, Orechia, & Sorensen, 2012), shifts other than day shift (Hopcia et al., 2012; Trinkoff, Le, Geiger-Brown, & Lipscomb, 2007), variable shifts (Rohde et al., 2013), long work hours (Clarke, 2007; Hopcia et al., 2012; Kasatpibal et al., 2016; Trinkoff et al., 2007), and overtime (Stimpfel et al., 2015). However, Stimpfel and colleagues (2015) found no significant differences in needlestick injuries by type of shift, length of shift, and number of hours worked. Finally, several studies have found high workload or inadequate staffing to be related to needlesticks (Cho et al., 2013; Kasatpibal et al., 2016; Patrician et al., 2011; Stimpfel et al., 2015).
Factors Associated With Musculoskeletal Injuries
Several studies have examined the association between individual and workplace factors and WMSD. In terms of individual factors, older age was associated with WMSDs in one study (Heiden, Weigl, Angerer, & Müller, 2013), but not in other studies (Sorour & El-Maksoud, 2012; Stimpfel et al., 2015). Similarly, females were more likely to have WMSDs in some studies (Hoe, Kelsall, Urquhart, & Sim, 2012; Trinkoff, Lipscomb, Geiger-Brown, Storr, & Brady, 2003), but not in others (Sorour & El-Maksoud, 2012; Warming, Precht, Suadicani, & Ebbehøj, 2009). Race was not a significant factor in one study (Trinkoff et al., 2003). Experience (professional tenure) has not been significantly related to WMSDs (Sorour & El-Maksoud, 2012), but nurses holding a bachelor of science in nursing degree had fewer WMSDs (Stimpfel et al., 2015). Poorer health was significantly related to more WMSDs in two studies (Alexopoulos et al., 2011; Stimpfel et al., 2015).
Regarding the work environment, one study found that scheduling issues (i.e., working more than 13 hours/day or 40 hours/week, fewer breaks, on-call, working weekends, consecutive shifts, while sick, on a scheduled day off, mandatory overtime, or 6 or more days in a row) were significantly related to WMSDs (Trinkoff, Le, Geiger-Brown, Lipscomb, & Lang, 2006). Type of shift in general was not related to WMSDs. However, Stimpfel and colleagues (2015) found that RNs working night shifts had more WMSDs. Stimpfel and colleagues (2015) and Trinkoff and colleagues (2003) also found that higher workloads were related to more WMSDs.
Factors Associated With Verbal or Physical Violence
A few studies examined individual determinants of verbal or physical workplace violence. Younger age was associated with verbal violence (Pai & Lee, 2011) or violence in general (Wei et al., 2016). Female nurses more frequently experienced violence (both verbally and physically) than male nurses (Al-Omari, 2015); another study found the opposite (Shields & Wilkins, 2009). Studies are mixed on the association between education and verbal violence (Jiao et al., 2015; Pai & Lee, 2011; Roche et al., 2010) and experience and physical or verbal violence (Celik et al., 2007; Jiao et al., 2015; Rodwell & Demir, 2012; Shields & Wilkins, 2009).
Work environment factors have also been associated with workplace violence. Studies have shown that nurses working rotating shifts (Jiao et al., 2015) or nonday shifts (Shields & Wilkins, 2009) experience more verbal and physical violence than nurses working other shifts or single shifts. Night shifts have been related to sexual harassment (Pai & Lee, 2011). Working more than 40 hours per week has been associated with a greater likelihood of physical violence (El Ghaziri, Zhu, Lipscomb & Smith, 2014). In several studies, inadequate staffing or staffing resources was associated with physical violence (Roche et al., 2010) or either physical or verbal violence (Shields & Wilkins, 2009). Lower skill mix was also associated with more physical violence (Roche et al., 2010).
Role of Job Difficulties, Demands, and Control in Workplace Injuries
The constructs of job difficulties, demands, and control have been used in a number of studies that examined the impact of work environment factors on nurse satisfaction, burnout, and other nurse outcomes such as workplace injuries. Job difficulties include inadequate resources, role conflict, inadequate support, supervisory issues, and workload that could prevent nurses from adequately performing their jobs (Kovner et al., 2007). Job demands increase when nurses feel pressured to perform their jobs due to heavy workloads, working too fast or too hard, or time pressures (Karasek, 1979). Job control, with an attribute of autonomy, is the ability to make and carry out decisions (Karasek, 1979) and may reduce negative effects of job demands (Häusser, Mojzisch, Niesel, & Schulz-Hardt, 2010).
These constructs have also been used in studies about nurse injuries and workplace violence. Job difficulties (e.g., high role conflict; Eatough et al., 2012) and low support (Bernal et al., 2015; Hoe et al., 2012) have been associated with musculoskeletal strains. In contrast, nurses who have better supervisor and coworker support experience less emotional violence (Rodwell & Demir, 2012).
Regarding job demands, high physical demands, haste, and a sense of urgency have been associated with needlestick injuries (Rohde et al., 2013; Kasatpibal et al., 2016; Loerbroks, Shang, Angerer, & Li, 2015). High psychosocial demands (Azma, Hosseini, Safarian, & Abedi, 2015; Barzideh et al., 2014; Bernal et al., 2015), high psychological and physical demands (Azma et al., 2015; Barzideh et al., 2014; Heiden et al., 2013; Sorour & El-Maksoud, 2012; Trinkoff et al., 2003), and demanding physical work tasks (Harcombe, McBride, Derrett, & Gray, 2010; Hoe et al., 2012) have been associated with WMSDs. One paper, however, did not find a significant relationship between time pressure and WMSDs (Warming et al., 2009). Job demands have also been associated with a greater threat of assault and emotional violence (Rodwell & Demir, 2012).
Low job control has also been related to WMSDs (Azma et al., 2015; Bernal et al., 2015; Eatough et al., 2012), emotional violence, and sexual harassment (Rodwell & Demir, 2012). Specifically, lack of job control (e.g., lack of autonomy) has been associated with needlestick injuries (Stimpfel et al., 2015).
NLRN Vulnerability and Summary of Hypothesized Determinants of Workplace Injuries
The prior research reviewed above points to some factors that contribute to workplace injuries and violence that are particularly relevant to newly licensed nurses. These nurses are less experienced and tend to be younger than RNs in general, and the literature suggests these two characteristics contribute to workplace injuries and violence. As Stimpfel and colleagues (2015) explain, “inexperienced or younger nurses may incur more needlesticks because they are still developing skills, habits, and learning how to manage work demands” (p. 1687). Given these vulnerabilities, personal and workplace influences on nurse injuries and violence discussed above could be accentuated.
Method
RNs who were first licensed between 1 year and 2.5 years prior were randomly selected from Florida Board of Nursing licensure data. Only respondents who were working in hospitals (N = 414) at the time of the survey were eligible for the current study. To assess for self-selection bias due to the low response rate, the authors compared respondents’ and nonrespondents’ individual and geographic information based on Florida’s licensure database. The sample was found to be representative of the entire NLRN population in Florida in terms of practice location and most demographics.
Measures
The survey was composed of questions about individual characteristics of the nurses, work environment characteristics of the organizations where they work, and the NLRN’s work injury and violence experience. Demographic characteristics included age, gender, Hispanic ethnicity, race (White, African American, other), self-perceived health, level of basic nursing degree, prior work experience in health care, and professional tenure (months of employment since graduation). Workplace characteristics included the type of hospital (academic medical center, community teaching, or community nonteaching), shift length (8-hour or 12-hour), shift time (day shift or other), the number of shifts in the previous month that the respondent “floated” (worked on a unit different than the usual one), actual hours worked in the past week, whether the respondent’s hospital had mandatory overtime, and the number of patients the respondent cared during the most recent shift.
Three scales encompassing job difficulty, job demands, and job control, were tested and used in a number of prior studies (Brewer, Kovner, Greene, Tukov-Shuser, & Djukic, 2012; Elovainio et al., 2005; Gurney, Mueller, & Price, 1997; Karasek, 1979; Kovner et al., 2007; Kovner, Brewer, Greene, & Fairchild, 2009; Parker & Sprigg, 1999; Spector & Jex, 1998; Unruh, Chisholm, & Zhang, 2016; Unruh & Nooney, 2011; Unruh, Raffenaud, & Fottler, 2016; Unruh & Zhang, 2013, 2014). Cronbach’s alpha values are generally reported as >.8 (Kovner et al., 2007; Unruh & Nooney, 2011).
Perceptions of job difficulties (nine questions) and demands (four questions) were measured using a 6-point Likert-type scale that indicated the frequency at which the job was difficult or demanding, ranging from never to 5 or more times a week. Perceptions of job control (three questions) were measured using a 5-point Likert-type scale from none at all to a great deal. Composite scores were created by summing the values of the individual items and dividing by the number of items.
Newly licensed registered nurses’ work-related injuries were measured with five questions regarding needlesticks, cuts or lacerations, bruises or contusions, strains or sprains (including back injury), and other injuries not listed. Workplace violence was measured with one question about verbal violence and one question about physical violence. Both were on a 4-point Likert-type scale that asked how often the participant experienced injuries or violence at their current jobs, from never to 3 or more times. A composite measure of workplace injury was also created by summing the values from all seven items and dividing by the number of items.
Data Collection
Using Dillman’s (2000) tailored design method, an initial mail survey was sent to a 40% random sampling of the listed NLRNs (n = 3,027), with postcard reminders to nonrespondents and a second survey to the remaining nonrespondents with a response rate of 18%.
Data Analysis
Descriptive analyses were performed on all variables. Logistic multiple regressions were calculated for each of the single-item dependent variables (seven separate workplace injury items), and ordinary least squares multiple regression was calculated for the composite injury scale dependent variable. Independent variables for all regressions were the demographic and workplace characteristic measures described above. Because the job difficulties and job demands scales had a few items that were similar (excessive workload in the job difficulties scale was similar to all of the job demand items [Table 1]) and to avoid correlated independent variables, the authors ran separate regressions using the job difficulties scale in one set of regressions and job demands and job control scales in the other set of regressions. Analyses were performed using Statistical Analysis Software (SAS; SAS Institute, Inc., Cary, NC, USA) version 9.4. Statistical significance was set at an alpha level of less than .05.
Demographic and Work Characteristics of NLRN Respondents (N = 414)

Note. NLRN = newly licensed registered nurse.
Scale from never to 5 or more times a week (range: 1-6).
Scale from none at all to a great deal (range: 1-5).
Results
Table 1 shows that close to 90% of respondents were non-Hispanic and over 75% were White. Over 90% were female, the average age was 35 years, and nearly 70% self-reported very good to excellent health. Most respondents had an associate’s degree, and just over one-half had worked in health care prior to obtaining their RN licensure. At the time of the survey, respondents had been employed approximately 2 years since their initial licensure. Almost one-half of the participants worked in community nonteaching hospitals. Nearly all worked 12-hour shifts, 62% worked day shifts, and they worked an average of 38 hours per week, floated 1 shift per month, and cared for an average of five patients on their most recent shift. Only 8% had mandatory overtime policies where they worked.
With a range of 1 to 6, respondents rated the frequency of their job difficulties on average 2.9 overall (see Table 1). Specific job difficulties ranged from “problems with supervisor” at an average of 2.1, “too high workload” at 3.5, and “interruptions” at 3.7. Job demands were rated an average of 4.2 from a range of 1 to 6. Specific job demands were scored from “requires doing more than can be done well” at 3.6 to “requires working very hard” at 4.6. Job control scores ranged from 1 to 5, were rated as 4.0, and had all three separate indicators close to that mean.
Percentages of NLRN workplace injuries and violence are presented in Table 2. Verbal violence occurred the most frequently. A full 70% of respondents experienced verbal violence at least once. Bruises or contusions occurred at least once among 49% and 40% experienced a strain or sprain at least once. Twenty-six percent of NLRNs experienced a needlestick at least once, and 25% experienced physical violence at least once. Cuts or lacerations occurred the least frequently.
NLRN Work Injuries (N = 414)
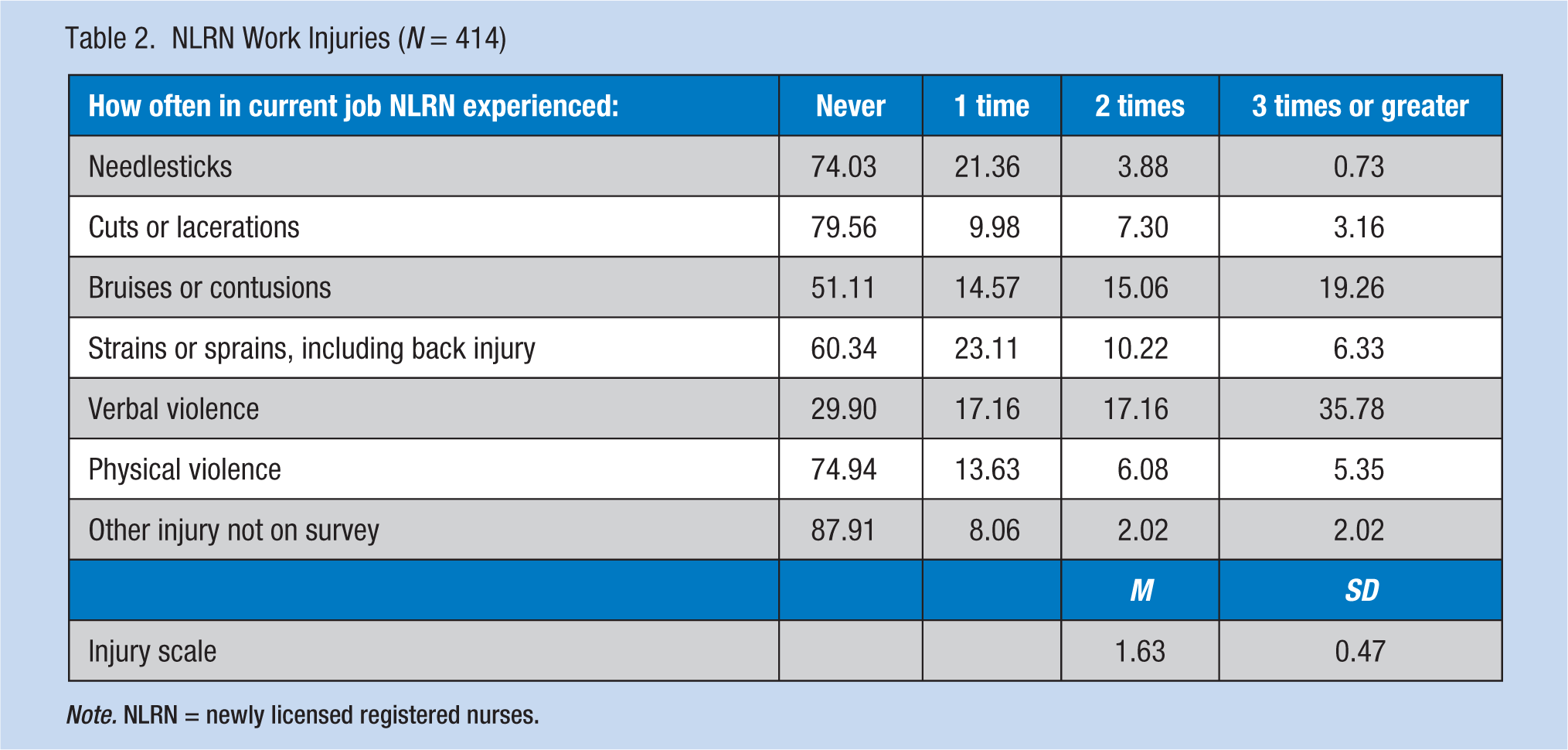
Note. NLRN = newly licensed registered nurses.
Predictors of workplace injuries and violence among NLRNs are shown in Table 3. Each column in this table presents the results for one dependent variable (e.g., needlesticks). Each row represents the independent variable producing the result. Because two regressions were calculated for each dependent variable, one that includes job difficulties and one that includes job demands and control, with everything else identical, the odds ratio or coefficient value presented in these cells is the highest value found for that variable in the 2 regressions for that dependent variable.
Determinants of Workplace Injuries in NLRNs
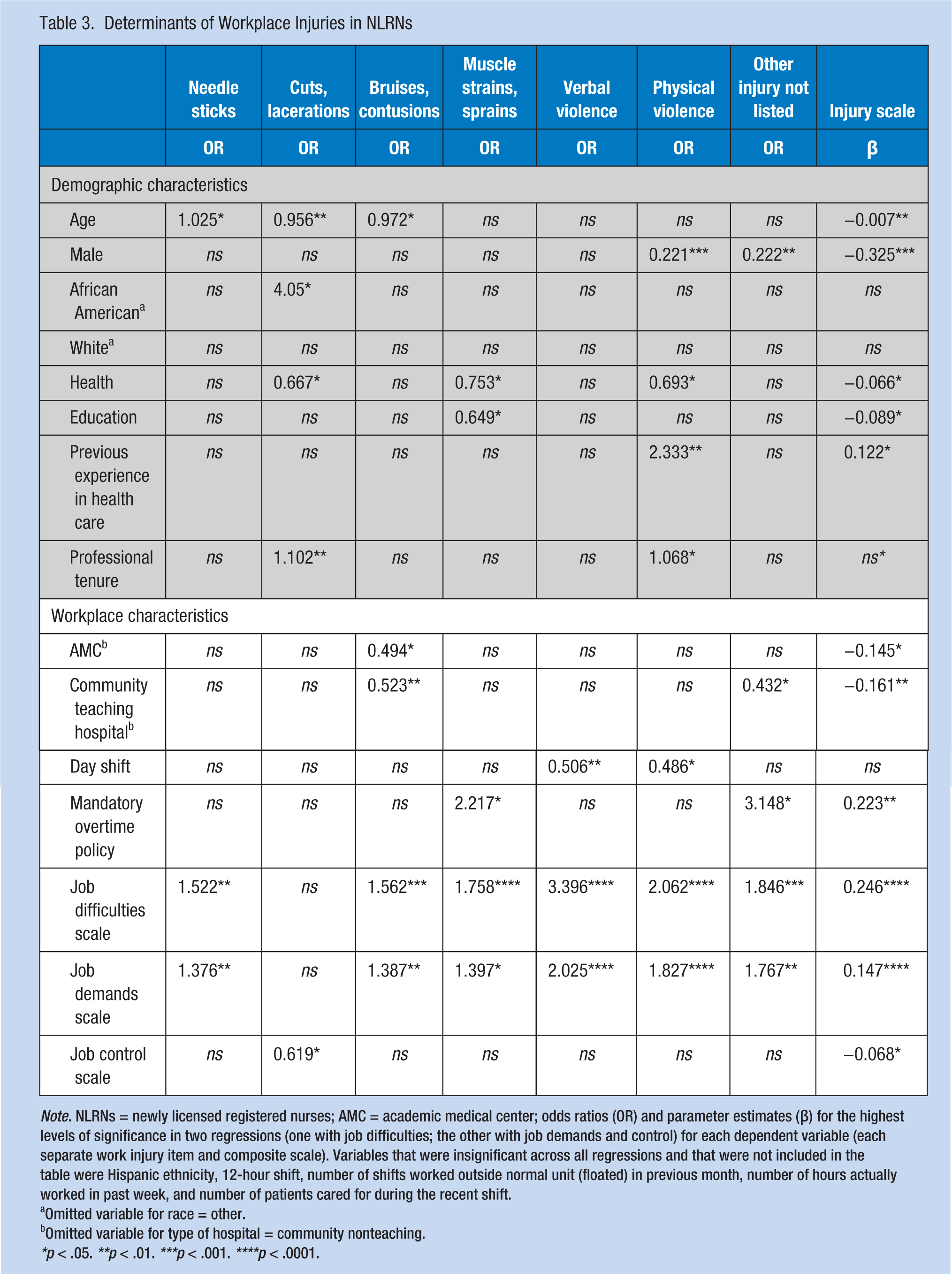
Note. NLRNs = newly licensed registered nurses; AMC = academic medical center; odds ratios (OR) and parameter estimates (β) for the highest levels of significance in two regressions (one with job difficulties; the other with job demands and control) for each dependent variable (each separate work injury item and composite scale). Variables that were insignificant across all regressions and that were not included in the table were Hispanic ethnicity, 12-hour shift, number of shifts worked outside normal unit (floated) in previous month, number of hours actually worked in past week, and number of patients cared for during the recent shift.
Omitted variable for race = other.
Omitted variable for type of hospital = community nonteaching.
*p < .05. **p < .01. ***p < .001. ****p < .0001.
Table 3 shows that several demographic characteristics were related to workplace injuries and violence. Age was a significant predictor for needlesticks, cuts or lacerations, bruises or contusions, and the injury scale. Older age was related to higher odds of needlesticks, but lower odds of cuts or lacerations and bruises or contusions. Older age predicted a lower injury scale. Being male was predictive of lower odds of physical violence or other injuries, and a lower injury scale. Being African American was significantly related to higher odds of cuts or lacerations. NLRNs with better health had lower odds of cuts or lacerations, muscle strains or sprains, and physical violence; better health was significantly related to a lower injury scale. Participants with higher education had lower odds of muscle strains or sprains and physical violence, and a lower injury scale. Previous experience in health care was associated with higher odds of physical violence and contributed to a higher injury scale. More professional tenure was related to higher odds of cuts or lacerations.
Several workplace characteristics were also related to workplace injuries and violence. Working in an academic medical center or community teaching hospital was related to lower odds of bruises or contusions and a lower injury scale. NLRNs who worked day shifts were less likely to experience both physical and verbal violence compared with those NLRNs who worked evenings or nights. Mandatory overtime policies were related to higher odds of muscle strains and other injuries, and a higher injury scale. Respondents who perceived high job difficulties and demands had higher odds of every type of workplace injury and violence and a higher injury scale. NLRNs who perceived higher job control had lower odds of having cuts or lacerations and a lower injury scale.
A number of hypothesized predictors were not significantly related to any type of occupational injury or violence: Hispanic ethnicity, White race, 12-hour shift, the number of shifts floated in the previous month, the number of hours worked in the past week, and the number of patients cared for during the most recent shift.
Discussion
Results indicated that NLRNs experienced various types of job injuries early in their careers. Verbal violence was reported by an astounding 70% of NLRNs; bruises, contusions, strains, and sprains were also common. Needlesticks and physical violence were reported by a quarter of the respondents. Verbal violence occurred more frequently than physical violence which concurred with previous studies of RNs. A quarter of study respondents experienced needlesticks in their current job which was slightly lower than the 30% to 70% annual percentage of RNs found in previous literature. Likewise, 40% of study NLRNs reported WMSDs, slightly below the 50% to 89% of RNs who reported WMSDs in prior studies.
With regard to the two prior studies of NLRN injuries, this study’s findings agreed with the findings of Stimpfel and colleagues (2015) who found that 24% to 30% of NLRNs experienced needlestick injuries, but were much lower than the Yang et al. (2013) study that reported NLRNs were up to 2.6 times more likely to experience a needlestick than experienced RNs.
What is new about these findings is the discovery of the extent to which injuries and violence are part of NLRNs’ workplaces. It is disturbing that 70% of NLRNs have experienced verbal violence in their short careers. Also disconcerting are the rates of WMSDs and lacerations. These are problems likely to create dissatisfaction with work and the profession and could lead to leaving one or both. Given the need to better retain NLRNs in their jobs and in the profession, these issues must be addressed and the incidence of injuries among NLRNs reduced.
With regard to factors associated with NLRN injuries, regression analyses indicated that a number of personal (i.e., age, gender, race, educational level, health, prior experience in health care, and professional tenure) and workplace characteristics (i.e., overtime, shift work, job difficulties, job demands, and job control) could contribute to these injuries.
These regression results were similar to the results of prior studies for some types of injuries, but not for others. Older NLRNs in this study were more likely to have needlestick injuries, but less likely to have other injuries. Prior studies were mixed as to whether older or younger nurses were more likely to have various types of injuries. Prior studies of RNs were also mixed with regard to gender; this study of NLRNs found that males were less likely to have specific types of injuries. This study was similar to other studies of RNs finding significant relationships between race/ethnicity and workplace injuries, with the exception of cuts and lacerations. It was also similar to studies that found education to be related to a lower risk of injury.
Surprising findings were that previous experience in health care and longer professional tenure was related to higher odds of several types of injuries. These findings run counter to much of the literature as cited in this study’s literature review. It is possible that NLRNs with greater experience care for higher risk patients, with more potential for injury. One study suggested that more nursing experience is not necessarily an indicator of competence in nursing environments where nurses are given little feedback from leadership, little knowledge is shared among staff, and continuing education is limited (Zarchi, Latif, Haugaard, Hjalager, & Jemec, 2014). Nurses with more work experience may also carry heavier workloads and feel additional job strain, which has been linked to increased risk for injury (Lee, Faucett, Gillen, Krause, & Landry, 2013). On the contrary, NLRNs with higher education were less likely to be injured, as was found in most previous studies of RNs. This finding may be due to a link between higher education and managerial positions, with less direct patient care. Additional research on the relationship between experience, education, the nursing environment, and risk of injuries should be pursued.
Study limitations included lack of data regarding institutional efforts to reduce workplace injuries (e.g., workplace injury and violence prevention programs) or how these interventions may reduce injuries in the presence of the other factors. This level of analysis would best be accomplished through an interventional study rather than survey approach. A multisite study with interventions to reduce workplace injury would also be beneficial. The authors did not assess whether verbal violence was primarily from colleagues or patients and their relatives. This information could assist researchers in determining whether workplace culture or patient interaction practices should be reevaluated to address this significant issue.
Study findings point to some areas for improvement. Most significant is the need to reduce job difficulties and demands and improve job control. As reported, these scaled measures were significantly related to nearly every type of workplace injury and violence, and they were the only predictors to be so related. Separate job difficulties and job demands indicators, described in Table 1, had higher means that could provide indications of priority areas: reducing interruptions, improving supervisor support, and reducing workload. Workload appears to be especially key to a number of injuries (Cho et al., 2013; Kasatpibal et al., 2016; Lee, Faucett, Gillen, Krause, & Landry, 2013; Patrician et al., 2011; Stimpfel et al., 2015).
Along with appropriate resources and sufficient time to complete tasks, training could be another factor in reducing workplace injuries (D’Arcy, Sasai, & Stearns, 2012) for NLRNs. Structured training increases knowledge and changes behaviors. Easily accessible online courses have been found successful in educating nurses about a variety of topics such as workplace violence (Brann & Hartley, 2017) and could be easily adapted for topics such as preventing needlesticks and falls.
Applying Research to Practice
This research finds that workplace injuries and violence toward nurses continue to be significant issues in hospitals, and that a higher probability of these injuries is associated with greater length of employment, working evening or night shifts, working overtime, and reporting job difficulties and demands. Age, gender, race, education, and experience also play roles in injuries. Results suggest that work environment issues, especially job difficulties and demands, must be addressed for safety programs to be effective. Reducing interruptions, improving supervisor support, and reducing workload are specific areas for improvement.
Footnotes
Authors’ Note
This study was approved by the University of Central Florida Institutional Review Board (IRB Approval No. SBE-08-05588).
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Florida Center for Nursing and the Blue Cross and Blue Shield of Florida Foundation.
Author Biographies
Lynn Unruh is a professor of health services administration in the Department of Health Management and Informatics at the University of Central Florida. A nurse and health economist, her research focuses on health care workforce and quality issues at the micro and macro level.
Yara Asi is a lecturer in the Department of Health Management and Informatics in the College of Health and Public Affairs at the University of Central Florida. Her research focuses on health care delivery in vulnerable populations, health care workforce issues, and global health and development.