
Abstract
Workplace bullying (WPB) among nurses, especially newly licensed registered nurses (NLRNs), negatively affects nurse, patient, and organizational outcomes. Despite empirical evidence addressing the prevalence and impact of WPB, the behavior continues to persist within nursing work environments. Increased conceptual clarity of WPB is needed for interventions to be developed, executed, and evaluated. The purposes of this concept analysis, in which we used Rodgers’ evolutionary method, were to obtain a clearer understanding of WPB, to differentiate the concept from other forms of workplace violence, and to describe a definition of WPB consistently used in the literature. Three attributes specific to WPB included negative behaviors directed toward an individual who perceives themselves to be a target, a time frame of experiencing these negative behaviors (e.g., daily or weekly) for a prolonged period (e.g., several weeks), and the inclusion of a power gradient or hierarchy between the bully and target. Antecedents identified for WPB included a scarcity of resources and poor leadership and management. Consequences associated with WPB included adverse nurse, patient, and health care organizational outcomes. WPB was conceptually defined as any negative behavior, exhibited by a nurse of either perceived or actual power, that was repeatedly (i.e., daily or weekly) and persistently directed toward NLRNs who have difficulty defending themselves against the behavior. Implications for researchers, health care organizations, nurse leaders, and nurses are included.
Keywords
Currently, there are approximately 3.6 million registered nurses (RN) working in the United States (U.S. Bureau of Labor Statistics, 2018) with more than 500,000 experienced RNs expected to retire by 2022, creating a workforce deficit of nearly one million new RNs (U.S. BLS, 2018). Newly licensed registered nurses (NLRNs), defined as nurses with 1 year or less of nursing experience postgraduation, are expected to help fill the projected nursing demand (Weaver, 2013). However, nearly one in five NLRNs leave their first nursing job within a year (Fiester, 2013) costing health care organizations approximately US$1.4 to US$2.1 billion annually for replacement staff (Kovner, Brewer, Fatehi, & Jun, 2014). Research suggests that NLRNs are more apt to turnover when compared with experienced nurses (Kovner et al., 2014) due to multiple factors including poor communication among coworkers, decreased job satisfaction, diminished organizational commitment, and a negative work environment (Kovner et al., 2016; MacKusick & Minick, 2010).
Although frequently referred to as a caring profession (Ashker, Penprase, & Salman, 2012), nurses do not always model caring behaviors toward their nurse colleagues. “Nurses eat their young,” is a widely used phrase to depict workplace bullying (WPB) targeted at NLRNs within the nursing profession (Simons & Mawn, 2010). Literature reports WPB is most prevalent during the first year of practice making NLRNs particularly vulnerable (Flateau-Lux & Gravel, 2014). In this article, the concept of WPB specifically targeted toward NLRNs was analyzed and implications for researchers using the concept of WPB is provided.
Background
Over the past three decades, WPB has become a growing research topic of interest (Simons & Mawn, 2010). Both anecdotal and empirical evidence suggests that WPB is a serious and prevalent issue within the nursing profession (Laschinger, Grau, Finegan, & Wilk, 2010), resulting in poor nurse, patient, and health care organizational outcomes. When compared with experienced nurses, NLRNs are more susceptible to becoming targets of WPB considering the factors related to being both a new nurse and employee, including a lack of social belongingness, confidence in skill sets, and nursing experience (Berry, Gillespie, Gates, & Schafer, 2012; Simons, 2008). During the first year of nursing employment, WPB is often commonplace (Randle, 2003). Simons (2008) found that in Massachusetts, 31% (n = 511) of NLRNs experienced WPB and Laschinger et al. (2010) in a Canadian study found 33% (n = 415) of NLRNs reported being targets of WPB. Associated with profound psychological and physical consequences, burnout, decreased job satisfaction, and diminished organizational commitment (D’Ambra & Andrews, 2014), WPB exerts a significant influence on turnover decisions (Laschinger, Leiter, Day, & Gilin, 2009).
In the context of an aging nursing workforce and an increase in health care demands (e.g., technology and increased acuity of patients), recruitment and retention of NLRNs has become a topic of concern for health care organizations worldwide (Laschinger & Fida, 2014; Laschinger et al., 2010). Newly licensed registered nurses are essential in the creation and sustainment of a healthy nursing work environment (Moore, Sublett, & Leahy, 2017). Thus, careful attention to sufficiently supporting NLRNs during the transition process from student to nurse must be a priority of health care organizations (Laschinger et al., 2010). WPB threatens this transition, negatively affecting the well-being of NLRNs and contributing to decisions to leave current nursing jobs or the nursing profession entirely (Laschinger et al., 2010). According to NLRNs, the greatest time of need for leadership and collegial support is during the first 3 months postgraduation (Rush, Adamack, Gordon, & Janke, 2014). Research suggests that NLRNs who have experienced WPB, but provided consistent support in the workplace, have significantly lower depression scores and lower intent to leave their current nursing position when compared with NLRNs who did not have access to such support at work (Rush et al., 2014).
Unfortunately, the prevalence data regarding WPB directed toward NLRNs varies across countries, cultures, and research studies due to the lack of a consistent conceptual definition and operationalization of the concept (Berry et al., 2012). Greater clarification of how WPB is defined conceptually is needed to understand the phenomenon. Only with a more thorough understanding of WPB, will effective interventions be developed and sustained to eliminate the presence of bullying within various nursing work environments. We used the Rodgers’ evolutionary method to create a clear definition to provide greater understanding of the concept to better determine how to detect, manage, and prevent the occurrence of WPB targeted toward NLRNs working in various environments (e.g., hospitals, clinics, outpatient care facilities).
Method
Consistency among the definitions and measurement of key concepts is vital for researchers to efficiently and effectively conduct research and communicate findings. A concept analysis is the rigorous process used to bring clarity to the definition and understanding of concepts (McEwen & Wills, 2014). Rodgers’ evolutionary method was chosen for this concept analysis because it involves a systematic six-step method that can provide a meaningful understanding of WPB, utilizes a discovery approach to focus on the identification of relevant attributes of the concept, and views concepts as dynamic, context dependent, and cyclical (Rodgers, 2000).
Due to its conventional use, the definition of WPB has become ambiguous (Rodgers, 2000), resulting in unclear definitions of the concept throughout the literature. Identifying the attributes most commonly associated with WPB using an inductive approach, without imposing predetermined criteria or expectations of the concept, is necessary (Rodgers, 2000). Rodgers’ call for a continuous refinement of concepts is appealing considering phenomena, goals, and needs of concepts that evolve over time (McEwen & Wills, 2014). Defining WPB without including contextual variation or its dynamic nature limits the ability to generate a useful definition of the concept. After identifying the concept of interest, WPB targeted toward NLRNs, and selecting an appropriate realm for data collection, the third step of Rodgers’ evolutionary method is to collect data to identify the attributes and contextual basis of the concept (Rodgers, 2000).
Literature Search
A literature search was conducted using four databases covering a 10-year time span (2008-2018): PubMed, CINAHL, Scopus, and PsychINFO. Although interest in WPB has grown over the past three decades, the majority of relevant articles were published within the specified 10-year time frame. The search used keyword phrases: “workplace bullying” and “new nurses,” “new graduate nurses,” “novice nurses,” or “NLRNs.” Keywords including incivility, horizontal or lateral violence, and harassment were not searched for this concept analysis. Articles were included in this review if they met the following criteria: (a) published within the 10-year time frame with the exception of three resources published prior to 2008, (b) written in English, and (c) discussed NLRNs and WPB specifically.
Results
The initial search yielded 55 full-text articles that were published from 2008 to 2018 in the English language. Twenty-three duplicates were removed, resulting in 32 articles for title and abstract review. Upon reviewing titles and abstracts, an additional 23 articles that did not pertain to WPB and NLRNs were removed. This resulted in a total of nine articles. Reference lists from the nine articles were then used to identify an additional 19 resources, three of which were published outside the date range (Einarsen, Hoel, Zapf, & Cooper, 2003; Leymann, 1996; Matthiesen & Einarsen, 2001), but met our other study criteria and we chose to include. In total, 28 resources were used in this concept analysis (Figure 1).
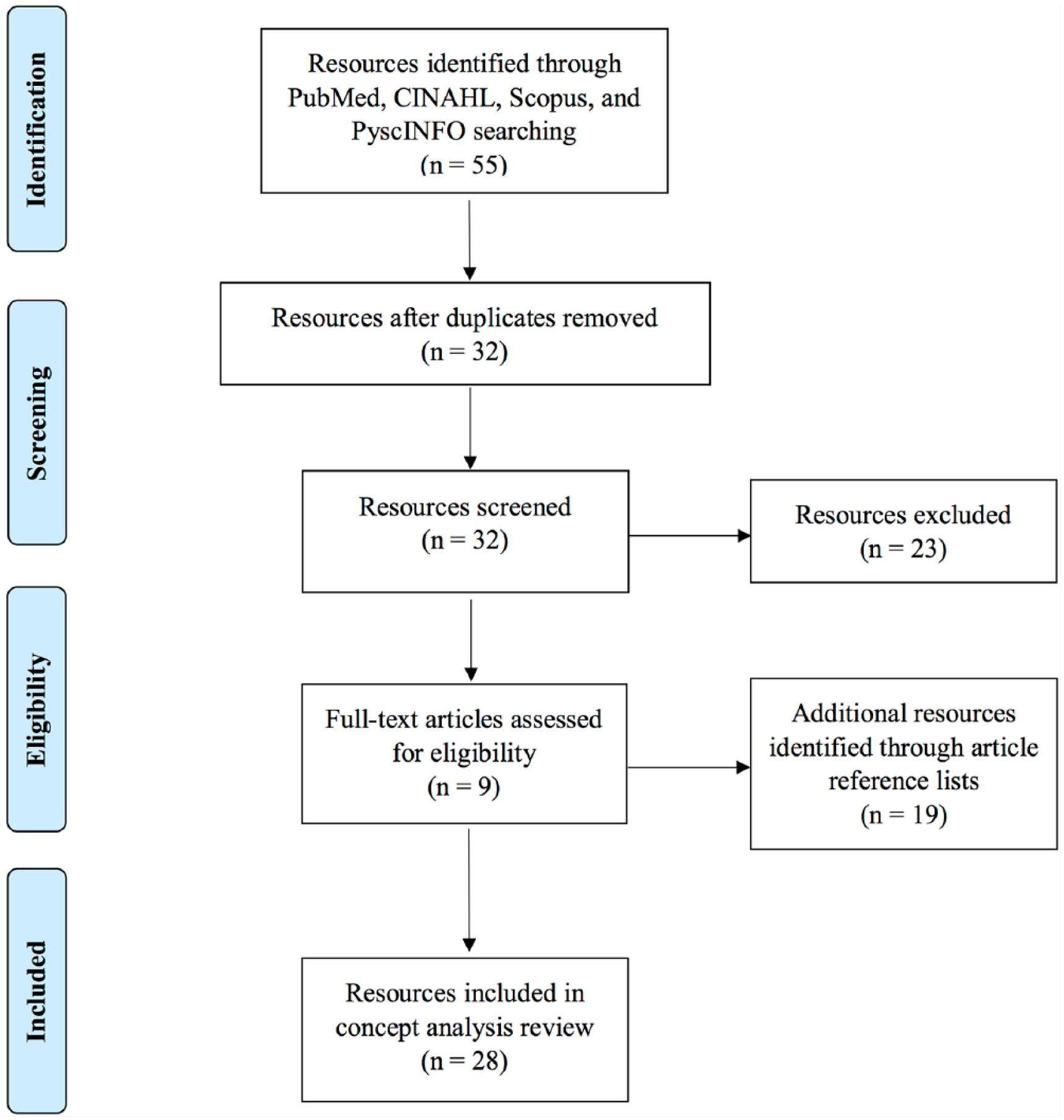
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram.
To bring clarity to the multidimensional nature of WPB among NLRNs, specific elements explored throughout the resulting resources were collected. These elements included (a) definitions of WPB, (b) examples of WPB behaviors, (c) time frame indicators, and (d) mention of a power gradient or imbalance of power (Table 1). Defining attributes, characteristics, surrogate and related terms, antecedents and consequences, and an exemplar of WPB are identified and discussed to obtain greater clarity of the concept (Rodgers, 2000).
Literature (n = 28) Regarding WPB that Included Elements of WPB Definition, Behavior, Time Frame, and Power Gradient.
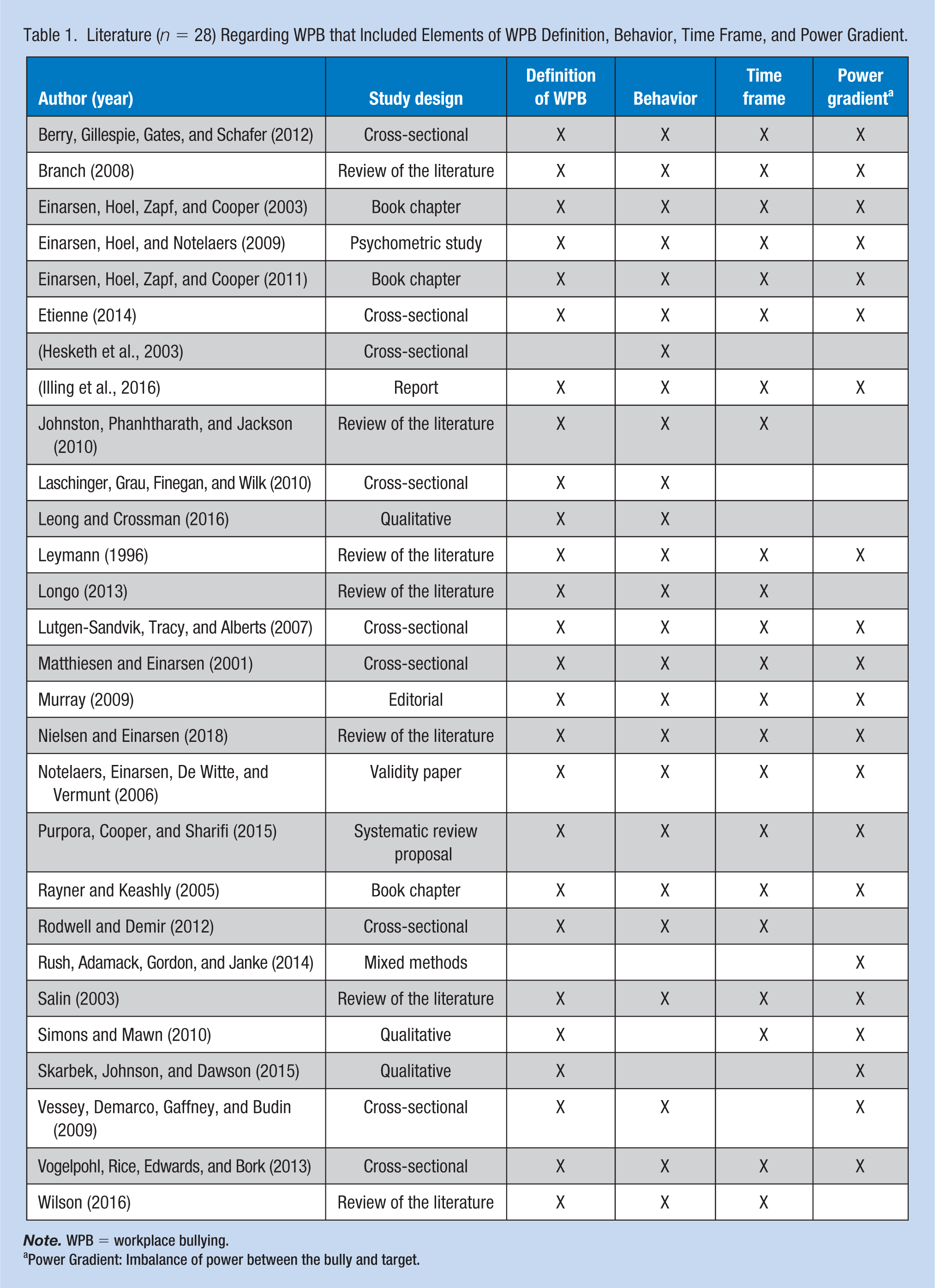
Note. WPB = workplace bullying.
Power Gradient: Imbalance of power between the bully and target.
Attributes of Behavior, Time Frame, and Power Gradient
Behavior
Workplace bullying was found to manifest in a variety of ways. According to research conducted by the Bergen Bullying Research Group (BBRG), a research team at the University of Bergen in Norway devoted to research on WPB, harassment, destructive leadership, and emotions within organizations, there were three behaviors, or factors, associated with WPB. These factors included (a) work-related bullying, (b) person-related bullying, and (c) physically intimidating bullying (Einarsen, Hoel, & Notelaers, 2009). To clarify, in the context of nursing, examples of work-related bullying directed toward NLRNs were found to include assigning an NLRN too many, or too few, patients, or continual criticism of an NLRN’s work, whereas person-related bullying involved false accusations, rumors, gossip, or social exclusion (Einarsen et al., 2009). Physically intimidating bullying, another form of WPB, was defined as overt physical violence or threats of violence (Einarsen et al., 2009).
Workplace bullying was noted to involve an individual’s perception of being the target of deliberate, inappropriate, or negative acts of behavior (Etienne, 2014; Johnston, Phanhtharath, & Jackson, 2010; Matthiesen & Einarsen, 2001) and found to be frequently carried out as indirect psychological acts. Researchers reported that the passive nature of WPB often made it challenging for targets to confront the behavior as the behavior was subtle and nonaggressive (Einarsen et al., 2009; Lutgen-Sandvik, Tracy, & Alberts, 2007). Although commonly passive or covert in nature, bullying behaviors could also be directly verbal or physical (Etienne, 2014). For example, direct verbal or physical bullying behaviors were determined to typically manifest as verbal abuse, overt exclusion of the worker being targeted, spreading of rumors, and/or withholding of information that could affect work performance (Etienne, 2014). Workplace bullying was determined to possibly lead to the undermining of the target’s personal and professional reputations in the workplace (Etienne, 2014; Salin, 2003). Bullying behaviors, such as continual criticism of the target’s work, sarcasm, and social isolation are utilized to intimidate or lower the target’s confidence was observed (Einarsen, Hoel, Zapf, & Cooper, 2011; Johnston et al., 2010), creating both personal and professional distress for the target (Leong & Crossman, 2016).
Time Frame
Workplace bullying was found to involve repetitive (e.g., daily or weekly) and prolonged exposure to adverse behavior (Einarsen et al., 2011; Rodwell & Demir, 2012). Although the negative and unsolicited actions experienced by the target were essential attributes of WPB, it was determined that the persistency of the behaviors delineated WPB from other forms of disruptive work behavior (e.g., incivility or horizontal violence; Einarsen et al., 2003). Most notably, a one-time incident of exposure to a negative behavior was not considered WPB (Einarsen et al., 2003; Zapf & Gross, 2001). Additional time frame descriptors of WPB included frequent, regular, or enduring negative acts (Einarsen et al., 2011; Lutgen-Sandvik et al., 2007; Simons & Mawn, 2010). Although the unwanted and negative behaviors associated with WPB were key to defining the concept, great emphasis was placed on the persistency of experiencing WPB (Einarsen et al., 2009). The frequency and prolonged time frame of exposure to WPB was what tended to deplete the target of coping mechanisms and resources, perpetuating the increasing powerlessness, or defenselessness of the target (Leymann, 1996). Over time, the potentially diminishing coping strategies combined with loss of social support may lead to the target’s inability to control their situation, helping in explaining the detrimental impact WPB may have on the target, even if bystanders may view the behaviors as subtle and indirect (Einarsen, Hoel, Zapf, & Cooper, 2011).
Power Gradient
An imbalance of power between the bully and target was deemed a central attribute of WPB (Einarsen et al., 2009). The power imbalance may be formal, representing organizational structure, or informal, and thus related to factors such as experience and existing social support in the workplace (Einarsen et al., 2003). This power differential distinguished WPB from other types of workplace violence (Branch, 2008). Reported among all levels within the nursing profession, perpetrators of WPB ranged from clinical staff nurses to administration (Johnston et al., 2010; Longo, 2013), therefore, transcending the actual or perceived hierarchical structure within the nursing profession (Einarsen et al., 2011; Murray, 2009; Skarbek, Johnson, & Dawson, 2015). The power gradient was noted to typically elicit feelings of humiliation, vulnerability, defenselessness, or intimidation within the target, undermining the target’s confidence, limiting their capacity to successfully self-defend, and interfering with their ability to develop competency and skill consolidation (Murray, 2009; Rush et al., 2014; Vessey, Demarco, Gaffney, & Budin, 2009).
Characteristics of the Concept
Surrogate and Related Terms
Numerous terms have been used to describe interpersonal hostility that may occur between nurses (Simons & Mawn, 2010). Surrogate terms are ways to express the concept other than by the term of interest—which in this case is WPB (McEwen & Wills, 2014). Workplace bullying was originally coined “mobbing” when it was first acknowledged by Swedish psychologist, Heinz Leymann, in the 1980s (Einarsen et al., 2003). Leymann reserved the term “bullying” to describe physical aggression among school-aged children (Purpora, Cooper, & Sharifi, 2015). During the 1990s, researchers in the United Kingdom used the term “bullying” to depict behavior that terrorizes adults in the workplace (Purpora et al., 2015; Rayner & Keashly, 2005). Mobbing, the only surrogate term identified in this literature review, is occasionally used interchangeably with WPB in some countries (Purpora et al., 2015). However, a few scholars posit that these terms should not be used interchangeably, but instead be placed on a continuum of lesser to greater intensity (Purpora et al., 2015).
Multiple terms have been used to describe disruptive workplace behaviors, including incivility, horizontal or lateral violence, harassment, and verbal abuse (Simons & Mawn, 2010). Although WPB and these related terms have commonalities, subtle distinctions exist that differentiates each form of behavior (Simons & Mawn, 2010; Figure 2). As its name implies, horizontal or lateral violence was considered violence perpetuated at the same social level, and therefore, does not include an imbalance of power or hierarchy, which was a distinguishing attribute of WPB. In addition, horizontal or lateral violence occurs as a one-time incident, whereas WPB must occur frequently and over at least 6 months (Simons & Mawn, 2010).
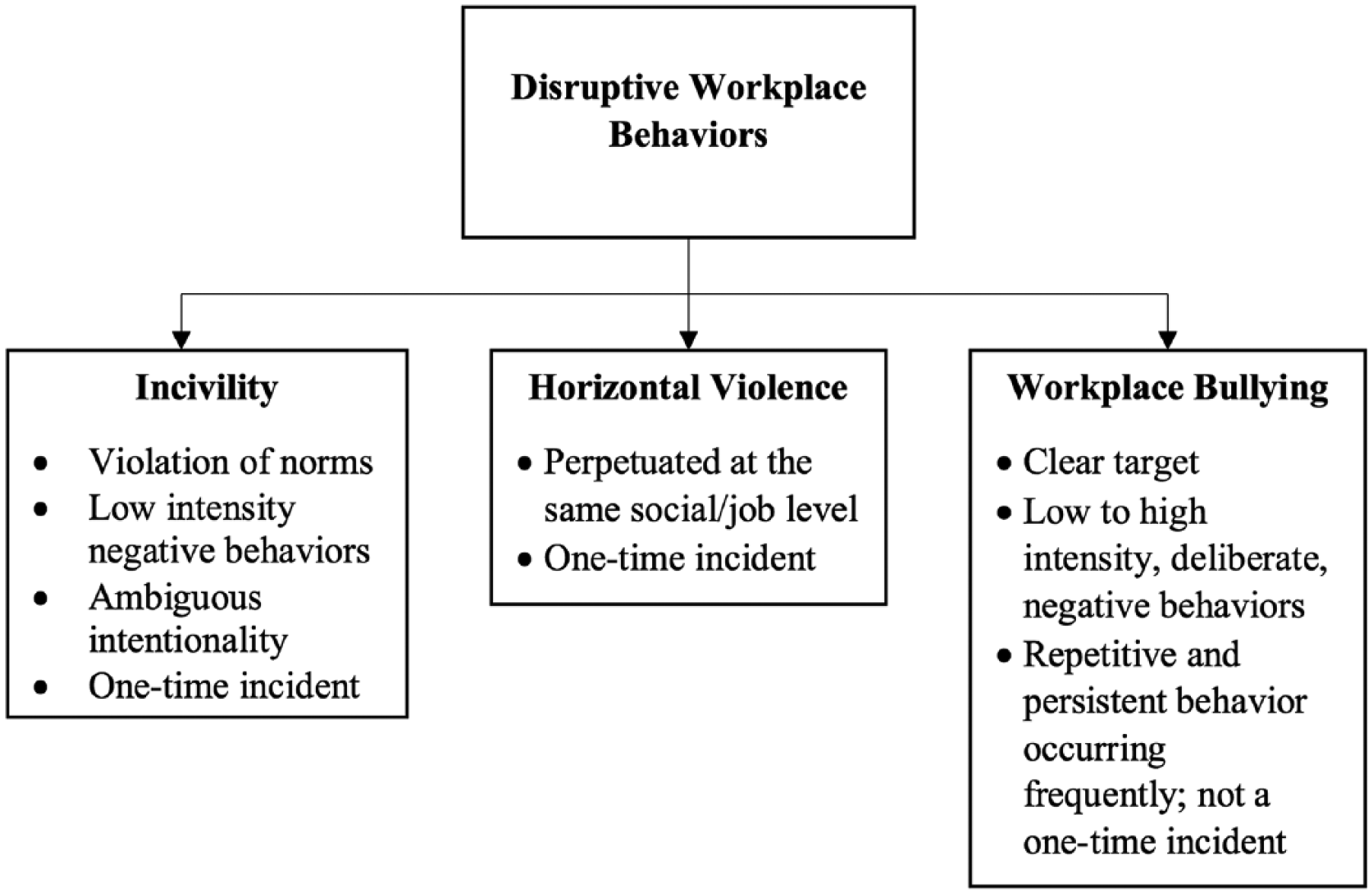
Differences between disruptive workplace behaviors: Incivility, horizontal violence, and workplace bullying.
Incivility was determined to involve the violation of norms, making it similar to WPB; however, the purposefulness of the perpetrator of uncivil behaviors is ambiguous (Branch, 2008). Furthermore, incivility was associated with low intensity, milder forms of negative behaviors whereas WPB often escalates in intensity (Einarsen et al., 2009). In addition, WPB behaviors are directed toward a specific target and occur for an extended period of time, whereas behaviors that occur in isolation may more commonly be labeled uncivil (Einarsen et al., 2009; Vogelpohl, Rice, Edwards, & Bork, 2013).
Workplace bullying may involve intentionality by the perpetrator; however, intentionality was not considered a defining attribute of WPB (Einarsen et al., 2009; Nielsen & Einarsen, 2018). To bring greater clarity to the intentionality of WPB behavior, researchers noted the importance of the notion that the target either subjectively or objectively experiences WPB. The subjective experience referred to the target’s perception that WPB behaviors were intentionally being directed toward them (Einarsen et al., 2009). In contrast, the objective experience of WPB must be verified or validated by observers of the behavior directed at the target (Einarsen et al., 2009). It was well recognized that one individual may consider particular behaviors to be WPB, whereas another may not, which has led to debates regarding the intentionality and operationalization of WPB. The concept of intentionality was noted to assist in delineating WPB from other forms of disruptive work behaviors by distinguishing WPB from careless, thoughtless acts or the misperception of either innocent or perhaps legitimate workplace behaviors (Einarsen et al., 2011). There were three main issues regarding the inclusion of intentionality within the definition of WPB. First, intentionality was considered difficult to prove (Nielsen & Einarsen, 2018). Typically, the only individual who can attribute that the behavior experienced by the target was intentional was the perpetrator, creating a situation where the bully has the power to deem whether the behavior is to be considered WPB (Einarsen et al., 2011). Second, the lack of self-awareness or unskilled social behavior may result in harming a coworker even though there was no true intent to harm (Nielsen & Einarsen, 2018). Third, intent was deemed difficult to measure (Nielsen & Einarsen, 2018).
Although intentionality was not considered a primary attribute of WPB, the perception of intent may determine whether the target labels the situation as bullying or not (Einarsen et al., 2011). In addition, it has been argued that the subjective experience of WPB is what manifests negative outcomes among the target (Einarsen et al., 2009). Thus, the intentionality of WPB may not always be clear or apparent; however, if the target perceives the behaviors to be intentional, in combination with the presence of additional WPB attributes, the behaviors qualify as WPB. The presence or lack of intent does not alter the situation or potential consequences for the target (Einarsen et al., 2011).
Antecedents and Consequences
Healthy nursing work environments consisting of positive staff and administrative relations, structural empowerment, and adequate staffing and resources have been linked to higher job satisfaction, decreased rates of WPB, and retention of NLRNs (Laschinger et al., 2010; Rush et al., 2014). In contrast, nursing work environments characterized by a scarcity of resources (e.g., equipment, staffing, and support) and poor leadership and management were associated with an increase in prevalence rates of WPB (Berry et al., 2012). WPB was discovered to be common among units with untrained preceptors or those who orient NLRNs frequently, as this creates additional stress on the preceptor (Berry et al., 2012). Similar to hazing, NLRNs begin to recognize and accept this phenomenon as a cultural norm when experienced nurses role model WPB, perpetuating the issue further (Berry et al., 2012).
The consequences of WPB were determined to harm not only the new nurse, but also patients and health care organizations. Newly licensed registered nurses who experienced WPB were at risk of developing poor psychological (i.e., depression, anxiety, emotional exhaustion, posttraumatic stress disorder, and suicidal ideation) and physical (i.e., headaches, eating disorders, onset of chronic diseases, and sleep disturbances) symptoms (Berry et al., 2012). If exposed to WPB consistently, NLRNs’ intent to leave their current nursing position increased as their job satisfaction decreased, ultimately resulting in turnover or leaving the nursing profession entirely (Wilson, 2016), negatively affects health care organizations financially. Due to a decline in psychological and/or physical health, studies reported NLRNs may become distracted mentally, experience decreased cognitive abilities, withdraw from nursing tasks, and show reduced commitment to work and diminished work productivity (Berry et al., 2012). These consequences may each result in poorer patient outcomes including medication errors and patient injuries due to falls (Hesketh et al., 2003; Laschinger et al., 2010).
Operationalization
Throughout the literature, there was consistency regarding the notion that WPB involves a power gradient, is not a one-time incident, and that the targeted individual perceives being on the receiving end of negative, unwanted actions. However, the lack of a standardized instrument to measure the prevalence of WPB and the distinction between objective and subjective experiences of WPB has led to conceptual confusion of the phenomenon (Einarsen et al., 2009). Yet, many scholars have argued that it is the subjective experience of the bullying actions as perceived by the target that will manifest as mental and/or physical health issues (Einarsen et al., 2009).
Multiple instruments were used throughout the literature to determine the presence and prevalence of WPB. However, the BBRG has developed several valid and reliable instruments to measure the perception of being the target of WPB over a 6-month time frame (i.e., Negative Acts Questionnaire, Negative Acts Questionnaire-Revised, and the Bergen Bullying Indicator). The Negative Acts Questionnaire (NAQ) is the original 23-item instrument developed to determine the perception of work- and person-related bullying behaviors. The NAQ was noted to high internal consistency, but the subjective perspectives of severely harmed targets of WPB overly influenced its items (Einarsen et al., 2009). In addition, the NAQ was developed during a time when bullying research was predominantly being conducted in Nordic countries and, therefore, its validity was tested in a limited Scandinavian cultural context (Einarsen et al., 2009). Furthermore, the NAQ only measured work- and person-related bullying factors and was, therefore, not inclusive of all three bullying factors (i.e., work-related, person-related, and physically intimidating; Einarsen et al., 2009). In an effort to overcome the issues associated with the NAQ, the BBRG developed the Negative Acts Questionnaire Revised (NAQ-R). The NAQ-R, a 22-item inventory, is inclusive of all three factors of WPB (i.e., work-related [seven items], person-related [12 items], and physically intimidating [three items]), with all items written in behavioral terms, avoiding the use of the terms “bullying” and “harassment,” to provide a more objective measurement (Berry et al., 2012; Einarsen et al., 2009; Illing et al., 2016). Moreover, the NAQ-R has been shown to provide a more accurate estimate of bullying than the one-item self-labeling Bergen Bullying Indicator (BBI; Notelaers, Einarsen, De Witte, & Vermunt, 2006), which utilizes the BBRG’s conceptual definition of WPB and then asks the worker to identify how often they experience such behaviors. The BBI however, provides a more objective estimate of one’s perception of being the target of WPB (Einarsen et al., 2009). The NAQ-R is frequently used alongside the BBI (Illing et al., 2016).
Discussion
This concept analysis examined WPB, targeted toward NLRNs, using Rodgers’ evolutionary method. Defining antecedents, attributes, and consequences specific to WPB were explored, offering greater conceptual clarity (Figure 3). The two antecedents identified for WPB included a scarcity of resources (e.g., equipment, staffing, and support) and poor leadership and management. The three attributes specific to WPB included negative behaviors directed toward an individual who perceives themselves to be a target, a time frame of experiencing these negative behaviors (e.g., daily or weekly) for a prolonged period (e.g., at least 6 months), and the inclusion of a power gradient or hierarchy between the bully and target. Finally, three consequences were associated with WPB, including (a) nurse (e.g., poor psychological and physical health, decreased job satisfaction, increased absenteeism, and increased intent to leave), (b) patient (e.g., medication errors and patient injuries secondary to falls), and (c) health care organizational (e.g., financial strain related to poor nurse and patient outcomes).
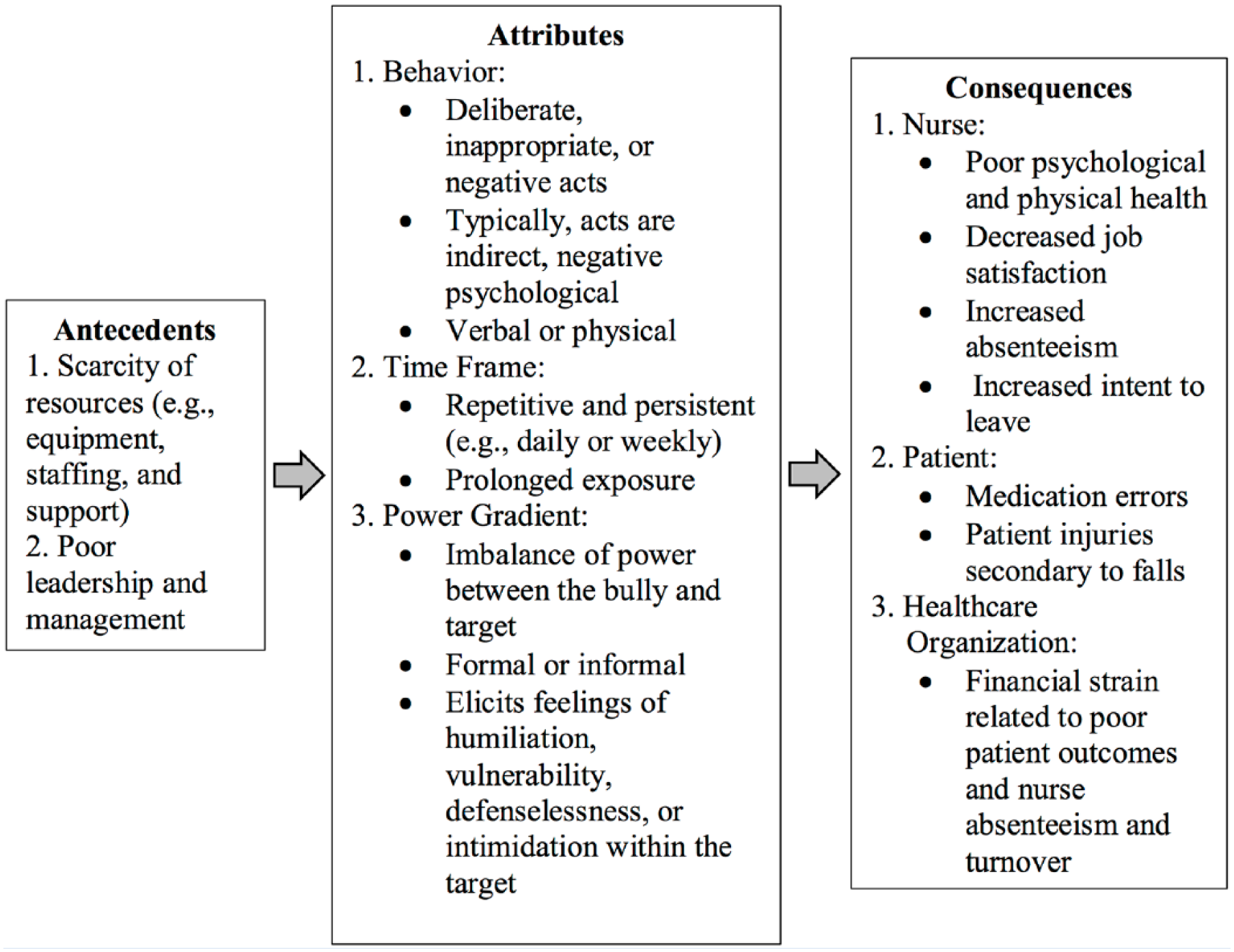
Antecedents, attributes, and consequences of workplace bullying.
Overall, the literature analyzed in this concept analysis was fairly inclusive of each attribute discussed in this article. The greatest clarification needed regards the differences between WPB and the related terms often associated with WPB (e.g., incivility, horizontal or lateral violence, harassment, and verbal abuse). Although similarities exist between these terms, subtle distinctions (i.e., an individual’s perception of being the target of deliberate, inappropriate, or negative acts of behavior; a prolonged time frame; and the presence of a power gradient) differentiate WPB from other types of disruptive workplace behaviors (Simons & Mawn, 2010). Markedly, many researchers and nurse leaders have questioned whether delineating these concepts (e.g., horizontal or lateral violence, incivility, and WPB) is helpful in regard to conceptual clarity and interventions seeking to eliminate negative workplace behaviors (Hershcovis, 2011; Nielsen & Einarsen, 2018). Perhaps differentiating the concepts has led to greater confusion in which researchers are studying almost identical forms of disruptive workplace behaviors but with different terminology (Hershcovis, 2011; Nielsen & Einarsen, 2018). Yet, in an attempt to decrease conceptual confusion among audiences, it is important for researchers to utilize the proper terms when conducting research, writing publications, and discussing the varying types of disruptive workplace behaviors.
Due to its subjective nature, WPB is a complex concept to measure. However, based on the synthesis of the current literature and this analysis, an inclusive definition of WPB was determined and is as follows: WPB involves any negative behavior, exhibited by a nurse of either perceived or actual power, that is repeatedly (i.e., daily or weekly) and persistently (i.e., at least 6 months), directed toward an NLRN who has difficulty defending himself or herself against the behavior.
The proposed definition of WPB has the potential to facilitate proper identification of the phenomenon, a greater ability to determine prevalence rates, and ultimately assist in the elimination of WPB within the nursing profession. Clear understanding of the concept is not only important for researchers and authors, but for those working in and among the nursing profession, including nursing executives, frontline nurse leaders (e.g., charge nurses or nurse managers), and nurses themselves.
Limitations for this concept analysis include the potential for missed references as the search was not exhaustive and did not include non-English articles. This analysis is also limited by the difficulty in synthesizing studies due to differing definitions and measurements used to determine the prevalence and impacts of WPB targeted toward NLRNs. In addition, this analysis focused on WPB directed at NLRNs specifically and thus, did not explore WPB targeted toward nursing students, nurse faculty, and seasoned nurses who also experience WPB.
Implications and Recommendations
The final step of Rodgers’ evolutionary method is to identify an exemplar (Table 2) and discuss implications for further concept development. Currently, the state of the science on the concept of WPB directed toward NLRNs demonstrates the need for researchers to employ a consistent definition of the phenomenon and utilize the NAQ-R to generate comparability of results.
Exemplar.
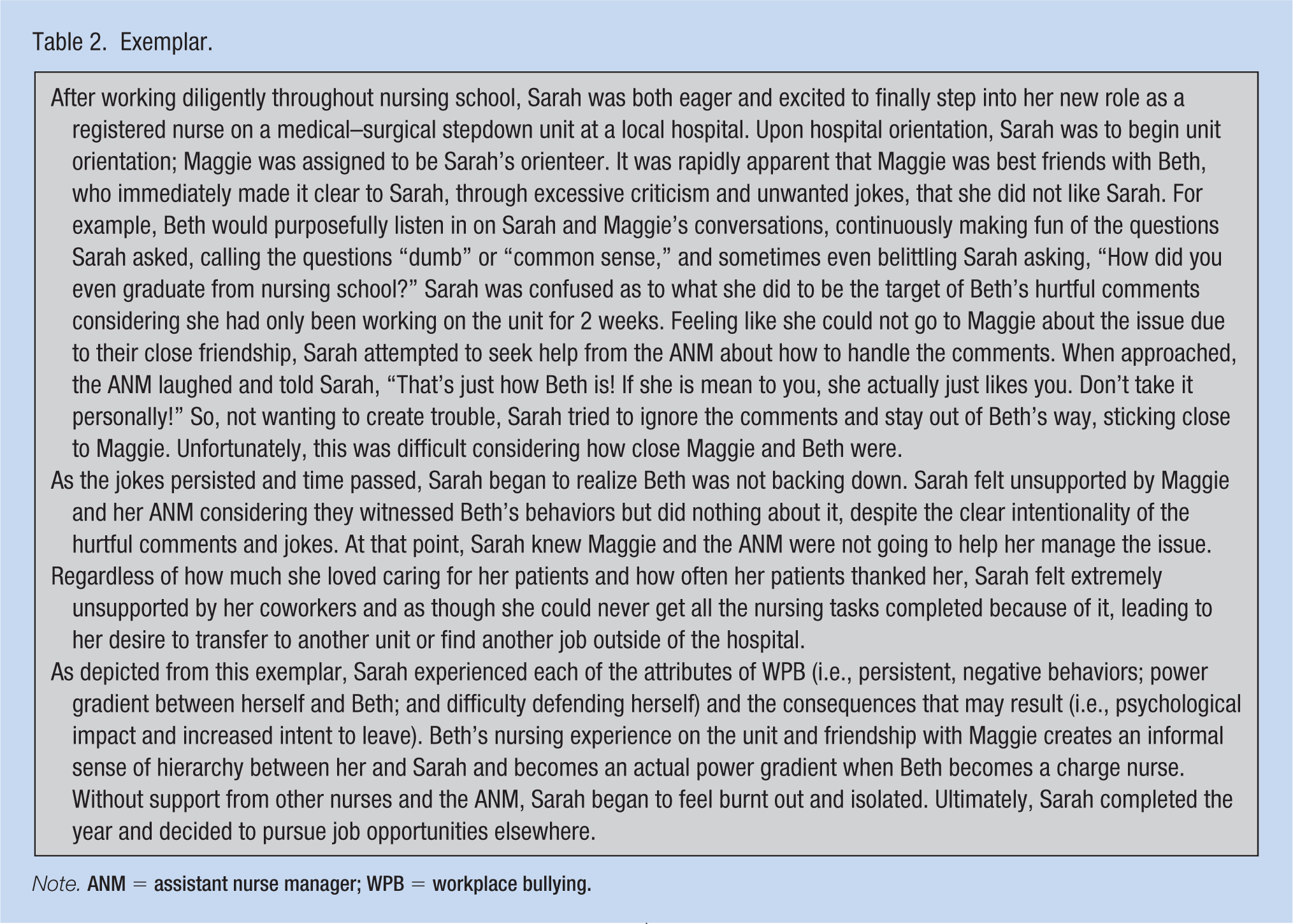
Note. ANM = assistant nurse manager; WPB = workplace bullying.
Implications for Researchers
Employing an inclusive definition of WPB is vital to eliminate existing conceptual confusion and facilitate greater comparability of study results both within the United States and internationally. In addition, because there is no standardized instrument that measures perceived exposure to WPB, the BBRG has proposed that the NAQ-R be used in future WPB studies, also increasing the ability to compare questionnaire results across varying cultures and organizational settings (BBRG, 2018).
Disruptive workplace behaviors, including incivility, horizontal or lateral violence, and WPB, each create unhealthy nursing work environments and often result in poor nurse, patient, and health care organizational outcomes. Yet, understanding the nuanced differences in these disruptive behaviors may lead to more effective strategies to eliminate them. Recently, there has been a shift toward developing interventions targeted at improving the nursing work environment or organization rather than focusing on interpersonal and intrapersonal characteristics of nurse bullies and targets (Einarsen et al., 2003; Georgakopoulos, Wilkin, & Kent, 2011; Keashly & Jagatic, 2003). Although each behavior may result in negative nurse, patient, and health care organizational consequences, the ability to understand the behavioral differences among each behavior could potentially assist nurse executives, leaders, and researchers in the development of interventions targeted at eliminating WPB directed toward NLRNs.
Conclusion
Despite the growing awareness and research interest regarding WPB within the nursing profession, WPB, especially directed toward NLRNs, continues to persist. The result of this concept analysis provides clarity and greater understanding regarding what constitutes WPB. Furthermore, this concept analysis addresses the antecedents that may facilitate WPB and its potential consequences. Results from this analysis suggest that nurse leaders and health care organizations should make efforts to eliminate bullying behavior in the nursing work environment by (a) appropriately determining the behaviors exhibited by nurses to guide the development of effective strategies, and (b) focusing on the improvement of organizational characteristics, rather than individual nurse characteristics, to decrease WPB. With increased clarity of the antecedents and attributes WPB, the elimination of such behavior is within closer reach, allowing the transition period of many NLRNs to become increasingly more positive.
Implications for Occupational Health Nurses
As providers and deliverers of health and safety programs and services to workers and worker populations through (a) promoting and restoring worker health, (b) preventing illness and injury, and (c) protecting workers from work-related and environmental hazards (American Association of Occupational Health Nurses, 2018), OH nurses have a role in combating WPB among nurses. Outside of promoting the core values of health care organizations and being familiar with the organization’s policy regarding WPB, skilled OH nurses have responsibilities of recognizing and confronting WPB, while also empowering nurses to do the same (Berry, Gillespie, Fisher, & Gormley, 2016). A practical strategy in recognizing potential WPB issues involves injury and illness surveillance to identify potentially at-risk workers or units (Berry et al., 2016). Furthermore, if made aware of a WPB situation, OH nurses should provide the targeted nurse(s) with support through advocating for the safety and rights of an employee while the matter is being addressed. If the targeted nurse(s) show signs of adverse outcomes commonly associated with being bullied (e.g., depression or anxiety), the OH nurses should implement the organization’s policy while also initiating medical intervention.
Occupational health nurses focus on workforce health but also collaborate and consult with organizational stakeholders (e.g., nurse leaders, human resource departments, and organizational professionals; Berry et al., 2016). Thus, OH nurses should be sensitive to organizational and unit culture and actively communicate with stakeholders any concerns that may arise regarding WPB or an uncivil environment. In addition, OH nurses can advocate for WPB interventions and advance intervention implementation within health care organizations. Confronting WPB within the nursing profession requires effort among nurses, nurse leaders, administrators, and additional health care staff. Occupational health nurses, through collaboration with each health care worker group are in a unique position to assist in managing the organizational changes necessary to reduce the prevalence of WPB (Berry et al., 2016).
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: First author was supported by doctoral study funding through the Robert Wood Johnson Foundation Future of Nursing Scholars Program (Grant: 72592) and UAB School of Nursing Doctoral Scholarship.
Author Biographies
Colleen V. Anusiewicz, BSN, RN, is a full-time nursing PhD student and Robert Wood Johnson Foundation Future of Nursing Scholar at the University of Alabama at Birmingham (UAB). Her research interests include exploring relationships among the nursing work environment, workplace bullying, missed nursing care, and nurse, patient, and organizational outcomes.
Maria R. Shirey, PhD, RN, FAAN, is an internationally recognized expert in nursing leadership and management. She teaches leadership, management, health policy, and scholarly writing in the DNP and PhD programs at UAB. A prolific author and editor, she is a mentor to developing authors.
Patricia A. Patrician, PhD, RN, FAAN, is the Rachel Z. Booth Endowed Chair in UAB’s School of Nursing. She served 26 years in the U.S. Army Nurse Corps, where she held clinical, administrative, educational, and research positions and now teaches at UAB in the Nursing and Health Systems Administration and PhD Programs.