
Abstract
Background:
Tobacco use is projected to cause more than 8 million deaths annually worldwide by 2030 and is currently linked to 1 million annual deaths in India. Very few workplaces provide tobacco cessation as a part of occupational health in India. In this study, we examined promoters and barriers to implementing an evidence-based tobacco cessation program in a workplace setting in India.
Methods:
In-depth interviews were conducted with all facilitators (two program coordinators and four counselors) of a workplace tobacco cessation intervention covering implementation efforts in five organizations, including three manufacturing units and two corporate settings.
Findings:
The identified promoters for implementation of the program were as follows: (a) workplaces that provided access to many individuals, (b) high prevalence of tobacco use that made the intervention relevant, (c) core components (awareness sessions, face-to-face counseling and 6-months follow-up) that were adaptable, (d) engagement of the management in planning and execution of the intervention, (e) employees’ support to each other to quit tobacco, (f) training the medical unit within the workplace to provide limited advice, and (g) efforts to advocate tobacco-free policies within the setting. Barriers centered around (a) lack of ownership from the workplace management, (b) schedules of counselors not matching with employees, (c) nonavailability of employees because of workload, and (d) lack of privacy for counseling.
Conclusion/Implications for Practice:
This study provided practical insights into the aspects of planning, engaging, executing and the process of implementation of a tobacco cessation intervention in a workplace setting. It provided guidance for an intervention within occupational health units in similar settings.
Background
The World Health Organization (WHO) put forth the Framework Convention on Tobacco Control (FCTC; WHO, 2005) to address the health impact of tobacco use, which is expected to cause more than 1 billion premature deaths in the 21st century (WHO, 2008). It is projected that globally tobacco will lead to 8 million deaths each year by 2030 (WHO, 2011). In India alone, 1 million deaths are associated with tobacco each year, which accounts for 9.5% of the total deaths in the country (WHO, 2018). In the WHO FCTC, Article 8 highlights the need to provide protection from exposure to tobacco smoke in indoor workplaces and Article 14 calls for designing and implementing effective programs to promote tobacco cessation within the workplace (WHO, 2005). India is a signatory to FCTC and based on the FCTC guidelines, India launched the Cigarette and Other Tobacco Products Act (COTPA) in 2003. Section 4 of the Act mandates “prohibition of smoking in public places” to protect people from Second Hand Smoke (SHS). As defined in COTPA, public places also include indoor workplaces (Government of India, Ministry of Health and Family Welfare, 2003). Studies undertaken to assess the implementation of COTPA and compliance with prohibition of smoking in public spaces showed that many workplaces in India have enforced a ban on smoking (Habbu & Krishnappa, 2015; Jain et al., 2016; Kummar et al., 2018). However, there is nothing in the Act that regulates use of smokeless tobacco within workplaces. This poses a challenge for interventions in India as the country is burdened with a high use of smokeless tobacco (Siddiqi et al., 2015) and tobacco cessation interventions in workplaces in India have shown employees largely using smokeless tobacco (Mishra et al., 2009; Ransing et al., 2016). While COTPA sets the foundation for smoke-free workplaces in India enabling many employees to abstain from use of tobacco (Lee et al., 2014), implementation of a multipronged workplace tobacco cessation intervention is required to enable employees to effectively quit use of all forms of tobacco (Mishra et al., 2009).
A Cochrane review of studies on workplace interventions for smoking cessation from 1966 to 2013 in 14 countries asserts workplaces to be the most effective setting for implementing tobacco cessation intervention (Cahill & Lancaster, 2014). Although most of the workplaces in low–middle income countries have smoke-free policies (Nazar et al., 2014), a deeper engagement with tobacco cessation was recommended within workplace settings (Seidel et al., 2017). There were limited studies published on tobacco cessation interventions implemented in workplace settings in India. These interventions were multicomponent; including behavioral counseling and Nicotine Replacement Therapy. Quit rates at the end of the intervention were higher compared with other settings, likewise reduction in the use of tobacco were observed (Mishra et al., 2009, 2010; Pimple et al., 2012; Ransing et al., 2016). These interventions suggested that the workplace, as a setting, provided easier access to employees where they could be monitored on multiple occasions (Pimple et al., 2012) and positive peer pressure among colleagues enabled participants to quit the use of tobacco (Mishra et al., 2009). The workplace setting was perceived to be less stigmatizing than community-based interventions for providing tobacco cessation (Mishra et al., 2009). For example, a randomized controlled trial conducted in manufacturing units in Mumbai demonstrated the efficacy of a tobacco cessation intervention in the workplace setting. The 6-month and 30-day cessation rates in the intervention arm were almost twice the rates in the control arm (Sorensen et al., 2017).
While it is clear that the workplace is a site for health promotion, specifically a platform for tobacco cessation, more information was needed on how to effectively implement such programs. For instance, we did not find studies conducted in India that explored factors influencing the implementation of tobacco cessation intervention in a workplace setting. Interestingly, the perspective of facilitators were less represented in the literature. This called for building evidence to use workplace settings for implementation of tobacco cessation interventions in India and the subcontinent. The purpose of this study was to explore promoters and barriers to implementation of an evidence-based tobacco cessation program through the facilitators’ perspective.
Methods
We conducted a qualitative study consisting of in-depth interviews using the Consolidated Framework for Implementation Research (CFIR; Damschroder et al., 2009). The study adopted the purposive sampling method. The sample size with respect to this study was six adult participants who covered implementation in five organizations; it included all the current facilitators of the intervention (i.e. facilitators responsible for planning and coordination; (n = 2) and facilitators responsible for providing tobacco cessation counseling (n = 4). This study was a balanced representation of all facilitators who were coordinators and counselors of the intervention, implementing, and executing the intervention respectively in the context of a workplace setting.
The CFIR is a well-studied implementation science framework, which draws together the unique and common elements of 19 different theories and frameworks and offers a common taxonomy for exploring the effectiveness of implementation within a specific context (Smith et al., 2015). It offers a list of constructs that help in understanding the intervention across multiple settings, that is, what works, where and why (Kirk et al., 2016). A systematic review published in 2020 reported that existing CFIR constructs are largely compatible for use in low- and middle-income countries (LMICs). And that the CFIR is a highly useful framework for global implementation science practitioners as it allows identification of implementation facilitators and barriers across settings (Means et al., 2020). The given study was executed in the post-implementation phase of the intervention.
Program Description
This study examined implementation of the LifeFirst tobacco free workplace program, an evidence-based program, based on programs developed in North America and Europe using the 5A’s framework (Fiore et al., 2008). Please refer to Table 1 for details of the program. The study incorporated experiences of the facilitators instrumental in implementation of tobacco cessation intervention in manufacturing units and corporate settings (Research and Development lab, Corporate head office).
Details of LifeFirst Tobacco Free Workplace Program
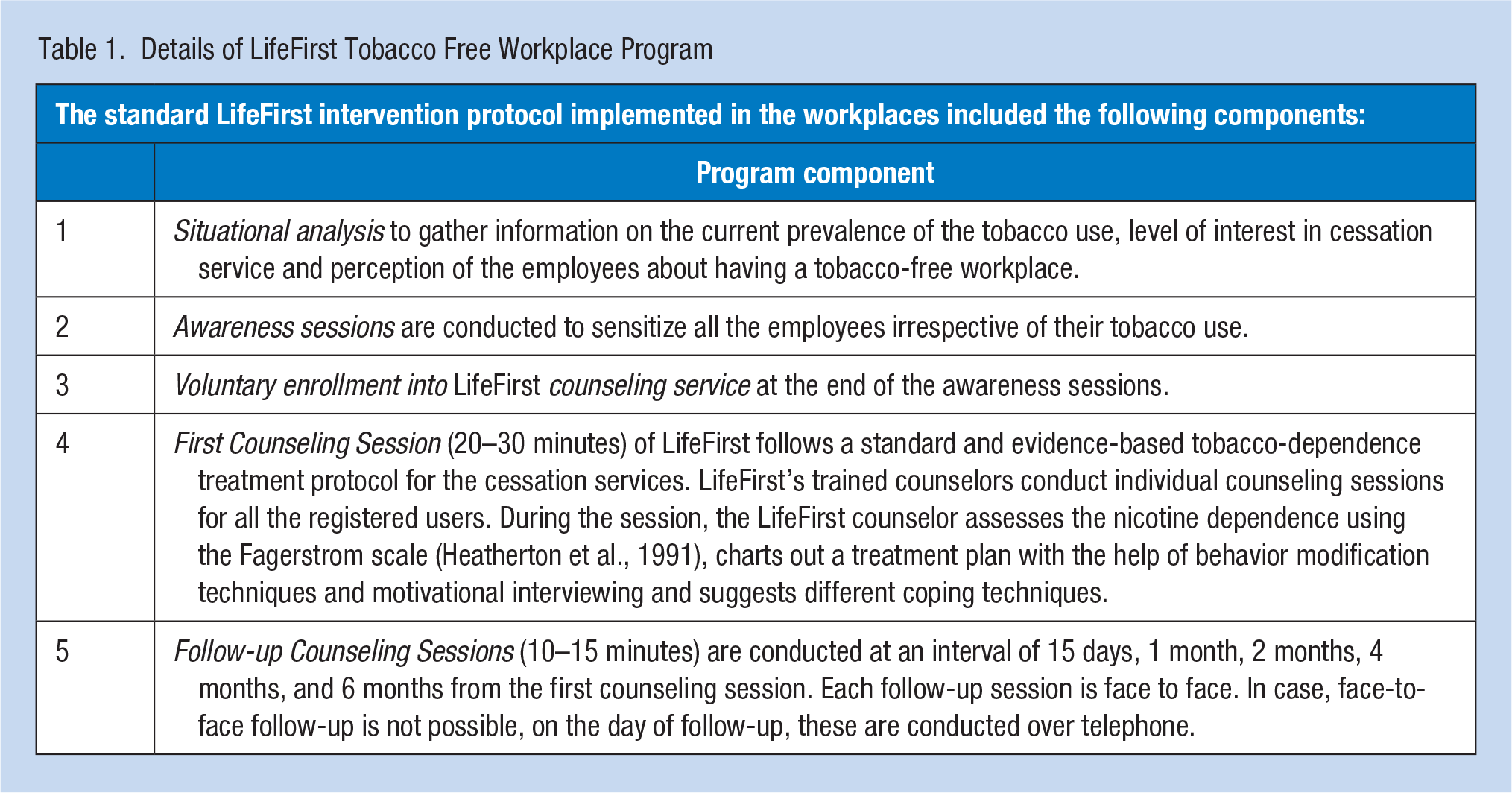
The LifeFirst tobacco-free workplace program was implemented in five workplaces by the team of four counselors and coordinated and managed by two coordinators (program managers) during the period July 2015 to March 2018. Of the total 5300 employees, 4058 were given information about the harmful effects of tobacco and the benefits of quitting by conducting group awareness sessions using PowerPoint presentations and videos. Of the 4058 employees who were given information, 889 of them joined the LifeFirst cessation program. After regular in-person follow-up sessions for more than 6 months, 584 (66%) of the participants self-reported to have stopped using tobacco products. The tobacco-free workplace policy was implemented at the conclusion of the program in one of the workplaces.
Data Collection
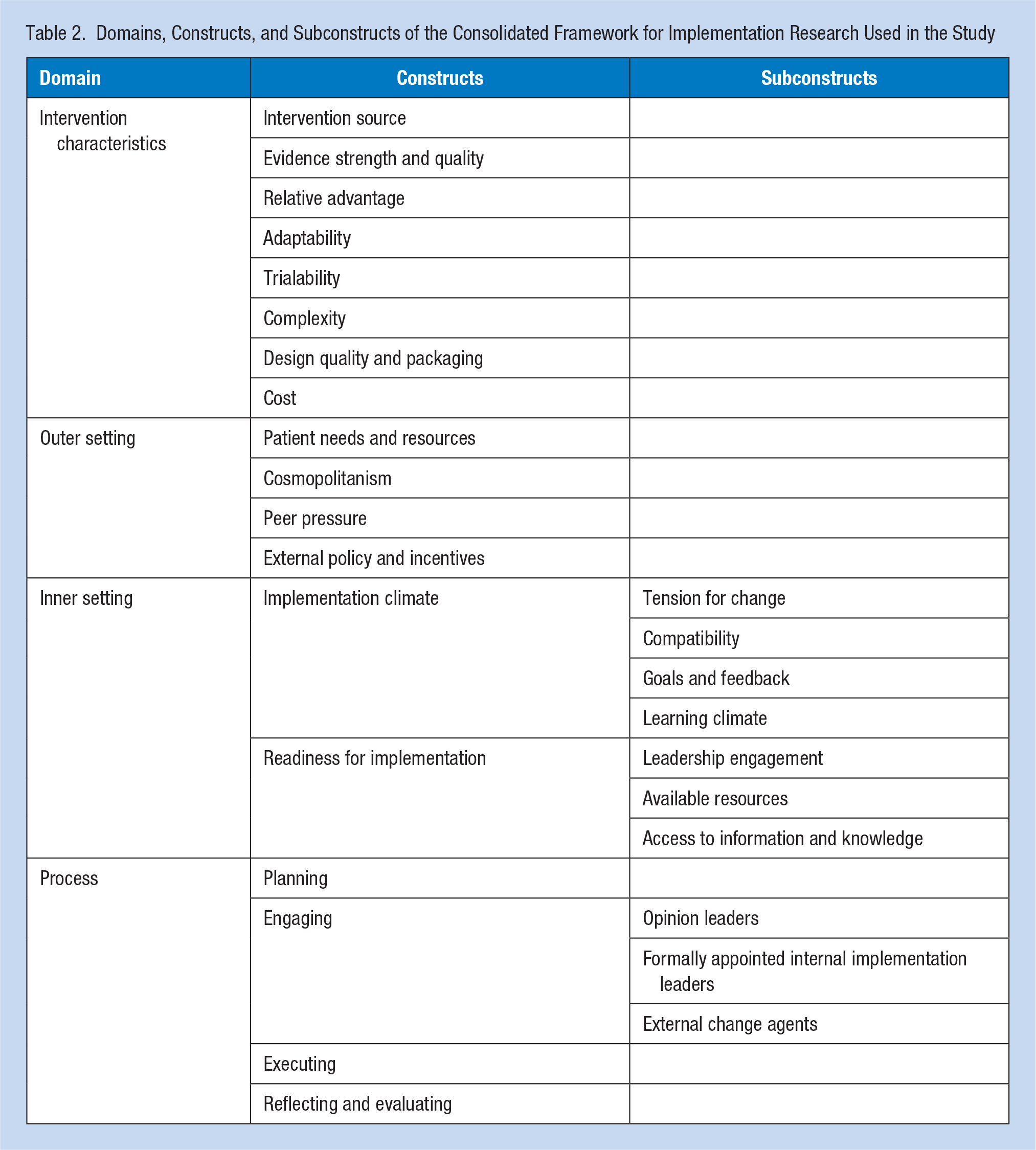
CFIR is comprised of five major domains and specified a list of constructs within these domains. We chose the domains of Intervention: Characteristics, Inner Setting, Outer Setting, and Process. Within these four domains we further identified 18 constructs and 10 subconstructs which were relevant to the study (Table 2). The domain of Individual Characteristics was not included in the study to avoid bias of the facilitators in reflecting on their own capabilities of implementing the intervention.
Domains, Constructs, and Subconstructs of the Consolidated Framework for Implementation Research Used in the Study
Identified CFIR domains and constructs were used to develop in-depth interview guides. Two in-depth interview guides were developed, one for the coordinators and the other for the counselors, given their differing roles in the context of the given intervention.
We pilot-tested the interview guide with three nonparticipants of the study: one coordinator of a health intervention and two counselors who provided tobacco cessation service within other settings. After the pilot, we eliminated a few CFIR constructs and subconstructs from the counselors’ interview guide that were not relevant to the study. We also simplified and contextualized the terminologies of CFIR for the facilitators. The study proposal and the study methodology were reviewed and approved by the Scientific Review Committee and the Joint Ethics Committee of Narotam Sekhsaria Foundation and Salaam Bombay Foundation. Written consent was obtained from the participants for in-depth interview and for audio recording of the interviews.
Face-to-face in-depth interviews were conducted in May 2018 by one of the authors who was a trained anthropologist. Interviews were conducted at an office where only the researcher and the participant were present. The interviewer was not part of the implementation which minimized any potential bias. Written consent was taken for in-depth interview and audio recording before the interview. We also clarified to the participants that their responses were not to judge the intervention’s effectiveness or evaluate their performance. We assured them that their responses were critical in enhancing their own work and further creating value for those who implemented or will implement a similar intervention within a similar setting. The average length of the interviews was 90 minutes. All in-depth, audio-recorded interviews were transcribed verbatim. None of the participants dropped out during the course of the study. There were no repetitions of in-depth interviews. Transcripts were not returned to the participants for checking.
Preliminary codes and themes were identified using an inductive approach. Furthermore, the CFIR codebook (Consolidated Framework for Implementation Research, n.d.) was used as a starting point for deductive coding. Coding was done separately for facilitators (coordinators and counselors). Codes that did not fit under any construct were coded as “emergent” codes. Code interpretation for the respective code values were done separately by two investigators involved in the study and later merged as one after discussion. After drafting initial results and interpretations, we conducted member-checks (Lincoln & Guba, 1985) with participants and refined our interpretations based on their feedback. No software was used for data management or data analysis.
The code values and code interpretations from both the coordinators and counselors were analyzed and reported together. We identified factors within the constructs, which acted as promoters and barriers in the implementation of the intervention, and used them to affirm the influences. We then mapped the constructs of CFIR to identify patterns and generate themes for the study. We also identified challenges experienced by coordinators and counselors in their respective roles during implementing the intervention within the setting. Finally, we have complied with the COREQ guidelines (Tong et al., 2007) for reporting this qualitative study.
Results
Study participants were the facilitators of the LifeFirst workplace tobacco cessation intervention. The study included all the six current facilitators of the intervention. Out of the four counselors, three worked in three factories and one worked in two corporate offices. They had implemented the specified intervention in the workplace setting for at least 2 years.
Initiation Phase
Setting: Context for implementation of the intervention
Facilitators identified the workplace to be a closed setting (limited by time, place, and persons) that facilitated in reaching out to many individuals at the same time. Behavior modification of individuals in such a setting can be effectively regulated through follow-ups because of their easy availability during the working hours. One of the coordinators (Participant 5) mentioned that “Employees spend more than 8 hours at workplace; if we are able to keep them away from tobacco during these (working) hours, the chances of them abstaining from tobacco use even after those 8 hours is much higher.”
Tobacco cessation intervention within the workplace setting was found to be compatible only with the existing workflows and systems that were related to the health and safety aspect of the employees. Its positive impact on the health of the workers was seen as a tangible value of the intervention by the management.
Packaging the intervention
As the facilitators were already implementing the intervention in other settings, the workplace became an extension of the same. Facilitators noted that the existing cessation protocols were applicable to the workplace setting which made transition to a new setting easier. In the interviews, all the facilitators acknowledged that the lack of rigor in approaching the workplaces and promoting the intervention on the program website acted as a barrier in effectively reaching new workplace management, which was something they recommended to other facilitators.
We face immense pressure in terms of pitching our program to the management at these workplaces, as tobacco cessation is a niche area . . . when you have to pay for a program which is for your employees and you are not sure of the outcome, then this is not well accepted by the companies. (Coordinator, Participant 5)
The gateway to implement a tobacco cessation service within a workplace setting was to influence the management of the respective workplaces to accept the intervention.
Facilitators shared the following factors that acted as promoters and barriers in this context.
Credibility of the Intervention: The credibility of the intervention was built upon the expertise and experience of the facilitators in the area of tobacco cessation which was demonstrated by the outcomes of implementing the same program in other workplaces and settings. The other aspects which built credibility for the program were the fact that there is an Act of the Parliament of India called Cigarettes and Other Tobacco Products Act (COTPA), 2003 which states that smoking within the workplace is banned and hence implementation of this program was in line with the statutory guidelines. They emphasized that the intervention itself was based on the American Cancer Society Workplace Tobacco Free Guidelines. Facilitators explicitly mentioned their intention to work toward implementing a tobacco-free workplace policy and to sustain the intervention through capacity building of key stakeholders within the setting were aspects which improved credibility. Facilitators ensured that the quality of the intervention was maintained through ongoing training of the counselors, enhancing resource materials and monitoring the data from the counseling sessions. While the facilitators shared a structured plan for the intervention, they believed that offering a flexible approach to adapt the intervention to the needs of the setting and to ensure follow-up for 6 months with each individual enrolled in the cessation service was influential in building the credibility of the intervention.
Communicating Goals: Goals of the intervention were communicated formally to the workplace management teams through a formal proposal document sent via email. If the management teams were interested, a formal presentation of the proposal was made along with an on-site visit. Upon acceptance of the proposal, the roles of the coordinators and counselors were described. While the coordinators shared the goals of the intervention to the management team; the counselors played a critical role in translating the goals to the receivers of the intervention at an individual level through awareness sessions and during first counseling sessions. The facilitators aligned the goals of the intervention to build the credibility and benefits of the intervention.
Cost Involved: As per the design of the intervention, the cost of the intervention was to be completely covered by the management of the workplace where the intervention was being implemented. The costs of the intervention were negotiated by the management in the budget section of the intervention proposal, as one participant indicated:
One of the management staff said that they could not afford the cost of the intervention. As a for-profit company they calculate the cost per head. They are not looking at 500 employees getting awareness, they are looking at those potential 100 employees voluntarily enrolling into the program which is divided by the total cost. And if the cost for per beneficiary is Rs.500/- (about US$7) then they say I cannot spend 500 on one employee. (Coordinator, Participant 6)
Facilitators asserted that the intervention is human resource–driven, especially the counselors who accounted for the maximum component of the budget. Fees for the counselors were often negotiated by the management, as they failed to understand the critical role of the counselors in bringing about behavioral change. In addition to the counselors’ fees, their travel costs, the resource materials that are developed, documentation, monitoring, and coordination are a part of the proposed budget. The workplace management, most of the time did not want to cover these peripheral costs in their budget. The total cost varied for each site depending on the location of the workplace, number of employees, proportions of management, workers etc. The acceptable range was Rs. 400 (US$6) to Rs. 700 (US$10) per employee. Hence, some workplaces negotiated to support financially only the awareness sessions and not the full cessation service (to reduce the costs to about Rs. 100, that is, US$1.5 per employee) which the program did not agree upon. Facilitators acknowledged cost involved to be a barrier in approving the intervention proposal, where either the cost was negotiated impacting the facilitators’ budget plans or the intervention was simply rejected either by the management or the facilitators.
Facilitators requested the management teams to provide the following resources: financial resources (covering the costs of the intervention), physical resources (offering physical space for awareness sessions and counseling sessions, providing technical devices like laptops and projectors), and human resource support (senior staff from the organization to support implementation of the intervention).
Core Components of the Intervention
Facilitators identified three core components of the intervention, which were essential and were interconnected to each other. The three components were: Awareness Sessions, Behavioral Counseling, and Follow-up Sessions.
Awareness sessions
According to the facilitators, awareness sessions were known to build a strong context to seeking cessation service. Awareness sessions also prompted individuals to quit and register for cessation service. These sessions also enabled non-tobacco users to continue abstaining from tobacco use. Overall awareness session sensitized all the employees (no judging etc.). As one coordinator indicated:
It is not training; we (coordinators) provide a sensitization session and then awareness about tobacco use. The content is different for the management. This is for them to understand the context of the intervention and support us in a better way. (Coordinator, Participant 5)
After the awareness sessions, opportunity to register into the cessation program was made available to the employees at a front desk. In the corporate setting, provisions were made for employees to register by email if they were not comfortable registering in front of their colleagues or if they were contemplating to register. No incentives for joining the program or successfully quitting tobacco use were involved in the implementation of the program either from the implementers or the workplace management team.
Behavioral counseling
Immediately after registration into the intervention, the first counseling session was conducted face-to-face. This was the first time the counselor interacted with the employee for a brief duration of 20–30 minutes. Facilitators expressed that the counseling component was new to the setting. Many workplaces were curious to understand the role of the counselors and the approach in counseling. One of the facilitator’s shared:
The counseling concept is new to management in both these setups, within a factory setup the education level of the employees is low and they cannot relate much to this concept. At the corporate level a sense of taboo is attached to counseling, something where one feels they have a problem and that is why one has to go to a counselor. (Coordinator, Participant 5)
According to the facilitators, the counseling component was one of the core components of the intervention. Emphasizing on the benefits of face-to-face counseling, one of the counselors (Participant 1) said, “Face-to-face counseling is very important. Because one can have phone follow-ups but it does not have much impact. But when we meet them face-to-face a lot of things come to the surface in our conversations, that has more advantage.” Another counselor (Participant 3) said that “The counselor should be prepared to work in any situations or circumstances at the given work setting. They should have good communication skills, they should be sensitized on this issue” to highlight that the environment does not matter much if the counselor is skilled. However, the need for privacy and an enabling environment was suggested to be important by most of the participants, with one indicating:
In counseling the only comfort they have is that we are talking to them in the process. So, there is a need of a good environment which is required for counseling, some workplace we had a room available for counseling. If we visit their work stations to provide counseling, it is not a quality one because of the sound of the machines and lack of privacy. (Counselor, Participant 2)
Stigmatization of seeking help to quit tobacco use was mentioned to be prevalent within the employees; more commonly at the corporate offices (white collared, i.e., among the more educated and higher socioeconomic group) as compared with the factories (blue collared). Corporate employees were of the opinion that they were well equipped and did not need support of cessation counseling to quit their use. They were confident that they could quit the use of tobacco whenever they wished.
One of the counselors (Participant 4) implementing the program at the corporate offices mentioned that “There were some female employees who were smokers but none of them registered for the cessation service due to the social stigma towards smoking among women.” The management grade employees were of the opinion that the intervention was beneficial for their employees, however, they were reluctant to enroll for counseling in the same program where their subordinates were also participating. Hence, they offered the cessation service to their employees but refrained from joining the cessation service even though they were smokers. One participant indicated:
At the corporate level a sense of taboo is attached to counseling . . . where one feels they have a problem and that is why I have to go to a counselor. In corporate they feel that—I am well equipped and I don’t need counseling, I can quit on my own. (Coordinator, Participant 5)
Follow-up sessions
Follow-up sessions were mentioned as a key component of the intervention. One participant . . . even if he makes all the effort to quit but if it is not supported by a follow-up it is of no use. Follow up is needed in the cessation service to keep them motivated and show them the end goal. (Counselor, Participant 4). They also indicated:
One advantage is that we are available in their office premises for counseling and we do follow-ups. Otherwise, many people do not come again for a follow-up session on their own. Since we are available in the office premises they are motivated to come and see us again. (Counselor, Participant 4)
Counselors reported facing challenges with the receivers of the intervention during the follow-up phase of the intervention. Following the first session some individuals resisted quitting tobacco use and some hesitated to come for the follow-up session. At times individuals in the factory setting were concerned about their shifts and could not afford leaving their work stations as they would lose time especially if it was a huge worksite. In the corporate setting, the counselor expressed that if the phone numbers were wrong or the individuals did not respond, they would be helpless as they could not approach the management due to the protocol to maintain confidentiality.
Counselors shared that when the worker does not come at the scheduled time for the counseling session, the person scheduled for the following session had to wait which would not be acceptable by the worker especially in a corporate setting.
Availability of the workers during the working hours was challenging when they were absent, or they had left the job. The lack of coordination with the management for scheduling counseling sessions causing interruptions in execution of the intervention.
Implementation Process
After acceptance of the intervention, the facilitators began work toward the implementation of the intervention in the stages of planning, engaging, executing, and evaluation. The stages are described as follows:
Planning
On the acceptance of the intervention, facilitators made a site visit along with the management staff. Meetings were scheduled with the stakeholders within the setting such as the human resource head, plant head, unit/department head and others.
Facilitators insisted taking into consideration the following aspects during planning the implementation of the intervention: (a) Understanding the nature of the workplace in terms of the business involved and the nature of work that happens within the setting. (b) Understanding the use of tobacco in the geographical region of the setting. (c) Understanding the prevalence of tobacco use (smoke and smokeless products) within the setting. (d) Understanding the dependency level on tobacco product by the potential receivers. (e) Learning the structure of the organization to systematically cover all workers within various departments. (f) Systematic approach to schedule awareness sessions, counseling session and follow-up sessions. (g) Considering the organizations’ schedule for leaves and annual work shut downs. (h) Ratio of number of individuals to be covered within the setting for counseling sessions compared with ratio of the counselors recruited.
Engaging
The facilitators mentioned engaging individuals within the setting such as the senior management staff, head of departments and units, human resource head and few such individuals within the setting who could influence the implementation positively. Later, individuals who were part of the cessation service and were excelling as champions in the cessation efforts were identified and nominated by the management and were trained additionally by the facilitators to facilitate the implementation and also to sustain it further. Positive peer pressure influenced employees to engage in the program and provided motivation and support in the process of quitting. The intervention had a program manager and a project coordinator who were involved in designing and planning the intervention; and the counselors were involved in execution of the awareness session and conducting counseling sessions. Facilitators were of the opinion to engage members carefully and thoughtfully as per the needs of the setting.
Facilitators reported that the management of the workplace were resistant to be stakeholders in the execution of the intervention. According to the experience of the facilitators, while the management resisted few ideas which involved their participation, they were at the same time flexible and supportive for changes that were manageable for the smooth execution of the intervention.
The management was involved in the role of decision making, planning the execution of the intervention within the setting and acted as facilitators between the employees and the counselors. Engagement of the leaders within the setting was prioritized by the facilitators as a critical factor that influenced the implementation of the intervention.
Executing
Facilitators were involved in coordinating with the respective management staff to execute the steps in the implementation process. They presented the execution plan to the workplace management. A Gantt chart was prepared to specify the timeline for the execution of the intervention. Assessment at the level of execution was done on a regular basis with the intention to augment the implementation process and to assure quality. This assessment was done by monitoring intake sheets, follow-up sheets and counseling sessions. Execution of the core-components of the intervention within the setting was done by the counselors, specifically: conducting awareness sessions, registering individuals for cessation services, scheduling counseling sessions with the enrolled individuals, conducting counseling sessions and providing follow-up.
Evaluation
Facilitators acknowledged not undertaking any formal evaluation study of the intervention. However, the emphasis was more on the regular reports of the follow-ups, which enabled the facilitators to evaluate the progress of the intervention. The counselors and coordinators did a personal and team debriefing on their progress and experience while executing the intervention within the setting.
Facilitators acknowledged not having any provision for formal feedback from the receivers of the intervention. Although the facilitators were open to receive feedback from the management and the receivers of the intervention informally, they acknowledged the gap of not engaging in a formal procedure for the same. Facilitators also suggested providing feedback to the workplace management in terms of what worked and what did not work during the implementation process.
The factors influencing the implementation of a tobacco cessation program in workplaces is summarized in (Table 3).
Summary of Factors Influencing the Implementation of the LifeFirst Tobacco Free Workplace Program According to the Domains of CFIR
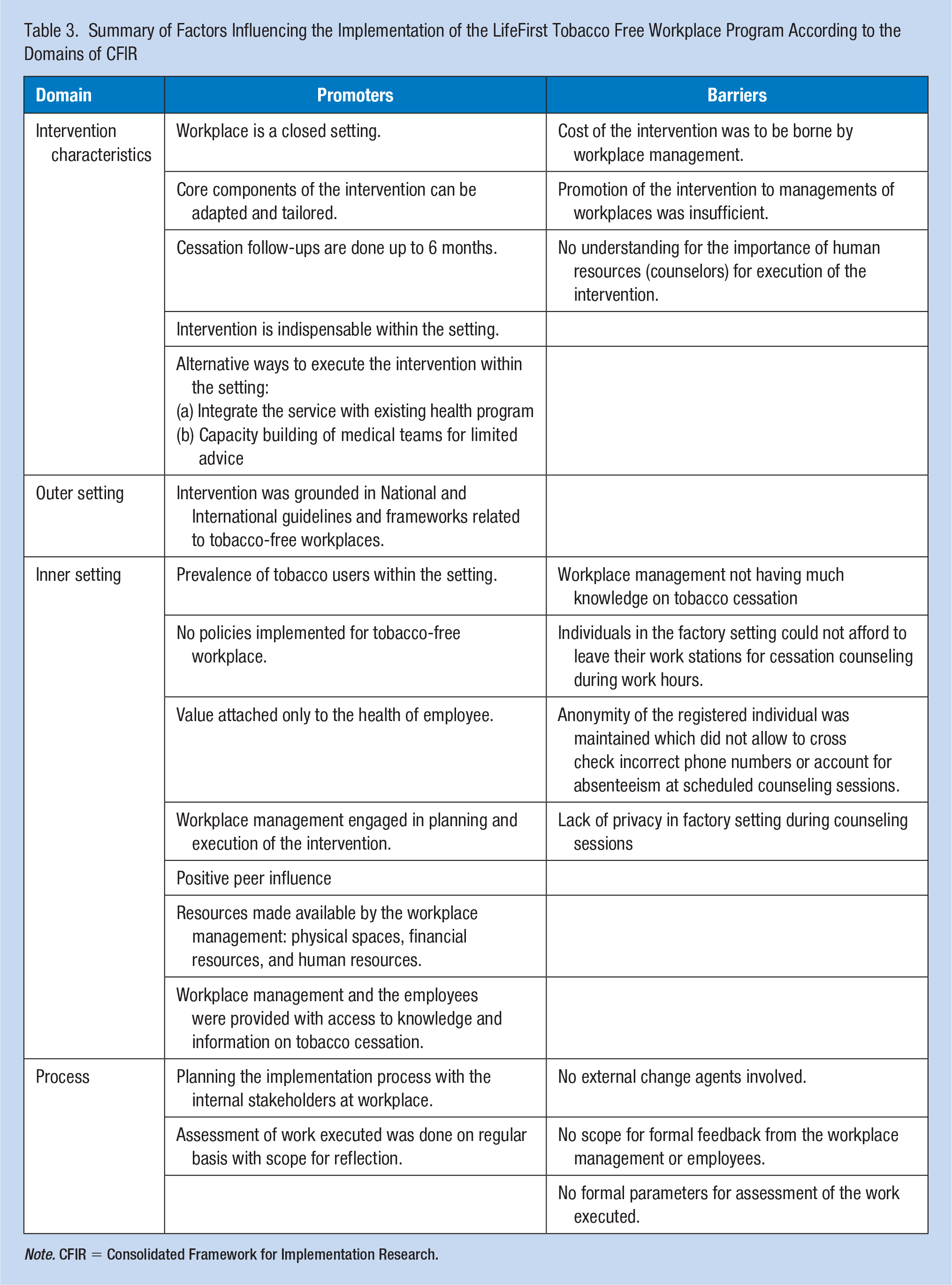
Note. CFIR = Consolidated Framework for Implementation Research.
Discussion
We identified a number of important promoters for implementation of the workplace-based tobacco control program: benefits of a closed system for intervention; framing the program to management in terms of health and safety; addressing norms by creating a tobacco-free environment, utilizing champions, and encouraging employees to support each other; supporting adaptation; and a sense of urgency based on high rates of tobacco use in the company. Important barriers centered around management buy-in, as they did not place value on the use of an intervention, had difficulty reconciling the need with the costs, and were uncertain about the benefit to the company. Other practical challenges related to difficulty executing the intervention for employees who travel for work or cannot leave their work stations, lack of appropriate space for private counseling session, insufficient staffing of counselors, and challenges of working in complex systems.
These findings were consistent with the broader literature highlighting that the workplace setting provided access to many individuals at the same time (Cahill & Lancaster, 2014; Pimple et al., 2012), positive peer pressure from colleagues motivated one to quit the use of tobacco (Cahill & Lancaster, 2014; Mishra et al., 2009; Ransing et al., 2016; Van den Brand et al., 2018), engagement from the workplace management ensured smooth implementation of the intervention (Mishra et al., 2009), cost for implementation of the intervention acted as a barrier (Kava et al., 2018), high attrition rates impacted the cessation follow-ups (Mishra et al., 2010) and tobacco cessation follow-ups played a critical role in enabling individuals to quit (Pimple et al., 2012).
Our findings diverged from the literature in which smaller workplaces had fewer anti-tobacco policies (Kava et al., 2018), workplaces built alternative healthy lifestyles as an extension to tobacco cessation services (Mishra et al., 2010) and that integrating the intervention into the occupational health and safety department of the workplace was challenging (Sorenson et al., 2017).
These findings suggested that the implementation of the LifeFirst tobacco cessation intervention in the workplace setting was acceptable, adoptable, appropriate, feasible, had good coverage, and was sustainable. We were able to describe the implementation cost and demonstrate fidelity of the intervention as per implementation research outcomes (Proctor et al., 2011).
Our findings also suggested a set of adjustments that would support implementation of the intervention: engaging support of the management, integration of the program into the company’s health program; training company personnel to conduct the intervention; implementing a Tobacco-Free Workplace Policy; considering alternate modes of delivery for the behavioral counseling (when face-to-face is impractical).
The team found that CFIR provided a useful framework to guide the retrospective implementation assessment in a workplace setting and was conducive to building a comprehensive, multilevel interview guide. This framework was not widely used in India and to our knowledge, this was the first study grounded in CFIR for workplace-based tobacco cessation interventions in India.
The cost of the intervention also featured among the factors influencing the implementation of the program. As this was an external program, the workplaces had to bear a minimal cost of around US$7 per employee. However, in workplaces already equipped with a medical team or an Occupational Health Nurse, no additional expenditure would be needed. The expenses of a tobacco cessation program were low as compared with the benefits of implementing the program—improved health, reduced occupational accidents, reduced absenteeism, reduced insurance expenses, and all this leading to increased productivity (American Cancer Society, n.d.; Cahill & Lancaster, 2014; Halpern et al., 2001).
It is important to note that India has nearly 90% of the workforce in the informal sector employment (Government of India, Ministry of Finance. (n.d.)). Individuals employed in the informal sector are exposed to various occupational hazards and do not have access to any organized occupational health services (Kishore et al., 2017). Thus, implementation of such an intervention can be crucial in informal sectors, considering that implementation of the given intervention was adaptable in a closed setting.
A limitation of this study was that the number of respondents was small; however, we believe these individuals represented the universe of facilitators for this program. In addition, the inquiry for this study was grounded in a unique initiative and thus the patterns that emerged may be unique to this group of companies or program, limiting the generalizability of the findings. A strength of this study was that it was also grounded in an implementation science framework that took a multilevel perspective on planning, engaging, executing, and process aspects of implementation. The practical nature of this approach offers an important contribution to the limited implementation science literature in India and other LMICs. This study captured perspectives of facilitators, who have rich firsthand expertise with the program. The opinions of the facilitators were based on their experiences in a set of workplaces varying in their size and nature (corporate offices, manufacturing factories, and pharmaceutical laboratory), offering insights across a mix of settings.
Implications for Occupational Health Practice
The findings of this study have implications for occupational health practices globally. They provide a blueprint for implementing a tobacco cessation program in all kinds of workplaces having a closed setting and especially cater to contexts with multiple types of tobacco products. The role of counselors can be effectively taken over by occupational health nurses and there is existing evidence that tobacco cessation provided by nurses is highly effective. Engagement of certified counselors, Paramedical officers or Medical Social Workers can be an alternative in places that lack certified health professionals.
Based on the findings of the study, workplace tobacco cessation programs can be designed specifically for LMICs where tobacco prevalence is high and the proportion of working population is also high. The program can be adapted to various kinds of workplaces in other contexts, especially addressing the gaps in occupational health services in informal sectors where the employees are vulnerable to use of tobacco products.
Applying Research to Occupational Health Practice
Based on the learnings and suggestions of the study, the workplace cessation program can be designed and enhanced to various workplaces settings. A study to assess its effectiveness can be carried out using implementation research, particularly CFIR (Consolidated Framework for Implementation Research) can be used as a tool to effectively study various aspects of implementation of cessation programs in pre-implementation, during-implementation, and post-implementation phases, applying the findings in other contexts even in resource-limited settings.
Tobacco cessation can be integrated into the routine health and safety activities as an integral component of employee wellness. Occupational Nurses and/or counselors can be trained to provide limited advice and pharmacotherapy including nicotine replacement therapy. Employees joining the counseling service can be followed routinely. Findings of the study can be useful for setting up the service and also for ongoing implementation of the service.
Footnotes
Acknowledgements
The authors would like to acknowledge the Program Coordinators and Counselors of LifeFirst Tobacco Cessation Program for their cooperation and wholehearted participation in the interviews. This research study was a part of ongoing monitoring and evaluation of the program implemented by Salaam Bombay Foundation and supported by Narotam Sekhsaria Foundation.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Himanshu A. Gupte, general manager at Narotam Sekhsaria Foundation, is a public health expert with an expertise in implementing large scale programs for tuberculosis control and tobacco control. He specializes in establishing protocols for and implementing tobacco cessation interventions in a variety of settings like health care settings, workplaces, schools, etc. with a special focus on smokeless tobacco.
Marina D’Costa is a research executive at Narotam Sekhsaria Foundation. She is a trained anthropologist interested in the field of Qualitative Research and Medical Anthropology. Her current focus is qualitative evaluation of tobacco cessation interventions in various settings.
Shoba Ramanadhan is an assistant professor of Social and Behavioral Sciences at Harvard T.H. Chan School of Public Health. She is a behavioral scientist with expertise in implementation science, cancer disparities, and community-based participatory research. Her work focuses on strengthening systems and organizations to design practice-focused guidelines for strategic adaptation so that the implementing organizations can increase the impact of available interventions by leveraging practice- and research-based expertise.
Kasisomayajula Viswanath is Lee Kum Kee professor of Heath Communication in the Department of Social and Behavioral Sciences at the Harvard T.H. Chan School of Public Health and in the McGraw-Patterson Center for Population Sciences at the Dana-Farber Cancer Institute. He holds various leadership positions, to delineate a few, he is the faculty director of the Health Communication Core of the Dana-Farber/Harvard Cancer Center and director, Harvard Chan India Research Center.