
Abstract
Background
Wellness champion networks are deemed an important component to workplace wellness programs. By encouraging colleagues to engage in healthy behaviors, champions can help improve employee health and well-being outcomes, while reducing healthcare costs and increasing productivity. However, little evidence exists regarding factors that impact the effectiveness of a wellness champion. This study examined the relationship between employee engagement in a workplace wellness champion program and the direct manager’s support of the wellness champion role.
Methods
A descriptive study was conducted with a 15-item cross-sectional survey that was developed and disseminated to 470 wellness champions at a large academic institution. Survey questions addressed manager/supervisor support for the wellness champion, manager/supervisor support for faculty and staff direct reports participating in wellness activities, and demographic questions.
Findings
One hundred and ninety-nine (42%) wellness champions responded to the survey and responded to at least half of the questions. Wellness champions who reported a high level of manager support for their role were more likely to have high levels of engagement in communicating wellness initiatives (p = .0004), motivating and encouraging colleagues (p < .0001), and planning wellness activities (p = .04).
Conclusion/Application to Practice
Findings suggested that support wellness champions received from direct managers was a key determinant to their level of engagement in efforts to improve their colleagues’ health and well-being. As employers desire to impact the health and productivity of their employees and generate cost-savings, manager support of wellness champions is necessary to facilitate employee engagement in workplace wellness champion programs.
Background
Many organizations today are interested and invested in improving the health and wellness of their employees. Worksite health promotion (WHP) programs are used within organizations as a tool to promote or maintain the health and well-being of employees, which can lead to reduced healthcare costs and increased productivity (Kent et al., 2016). Establishing a sustainable and comprehensive WHP program within the workplace has a significant advantage over other health initiatives in communities or health care settings because of the extensive amount of time individuals spend at the workplace. Comprehensive sustainable WHP programs that aim to create a culture of wellness, achieving multiple positive outcomes, include the following components: (a) shared values, (b) leadership and management support, (c) frequent and clear communication, (d) metrics and measurement, (e) policies and procedures, (f) supportive built environment, (g) resource allocation, (h) rewards and recognition, (i) peer and champion support, (j) shared vision and mission, and (k) orientation, training and learning (Health Enhancement Research Organization, 2016). Although this is not an exhaustive list, these are important strategies to incorporate into a worksite wellness initiative.
One of the goals of WHP is to design a workplace environment in which individuals are connected to a larger group through which they find support and continue to be energized to lead healthier lifestyles (Spoonheim & Pronk, 2016). However, participation in workplace wellness program varies greatly due to several factors, including social influences, which can impact the effectiveness of wellness efforts (Safeer & Allen, 2019). In their recent article, Safeer and Allen (2019) stress that positive social influences on health and wellness practices include the following: (a) peer support to increase adopting healthy practices; (b) “touch points,” which are formal and informal social systems reinforcing healthy behaviors; and (c) key factors for building a positive social climate, such as leadership support at all levels. One strategy that bodes well for WHP efforts is the use of wellness champions. Wellness champions are employees who have a vested interest in improving the health and well-being of their colleagues and offering support for a healthy lifestyle through extending the reach of their organization’s WHP.
Wellness champions can be potential agents of change as many are invested in their own wellness and are interested in educating and supporting their colleagues (Wieneke et al., 2016). Wellness champions are a “grassroots” tactic used to improve employee participation in WHP programs, promote a culture of wellness, and positively impact healthy lifestyle behaviors and health outcomes. Linnan et al. (2013) define a wellness champion as a peer educator or peer advisor, an individual within the workplace who was “equal” in status to those who they are helping. Spoonheim and Pronk (2016) emphasized a peer-level support role in collaboration with leadership and management to ensure the “voice of the employee” was reflected in decision-making. Wellness champions play a role in the design principles because people are at the heart of all efforts that guarantee the program is successful. The authors further suggested that wellness champions appear at every level of the company and are intrinsically motivated to take on the role of champion. Safeer and Allen (2019) emphasized the importance of formal and informal leadership support at all levels to better support and encourage champions and their colleagues to engage in the WHP activities.
Whether formally or informally assigned to the role, champions should be considered an important modality of social support to others and have a powerful voice among all employees (Nunn & Terry, 2012). Linnan et al. (2013) emphasized that a wellness champion should provide support and facilitate social norms by enacting key functions, such as: social and emotional support to encourage disease management behaviors and coping with negative emotions, linkage to clinical care and resources, and support designed to sustain health behavior change. Desired qualities of wellness champions include: (a) commitment to the WHP program, (b) enthusiasm for the WHP program, (c) role modeling and leading by example, (d) participating in the WHP program, and (e) acting as an advocate for colleague participation in the WHP program (Michaels & Greene, 2013).
Although there is little agreement on the industry standard of wellness champion responsibilities, organization-specific examples have been described over time (Amaya et al., 2017; Bloom, 2008; Kuehl et al., 2013; Wieneke et al., 2016). For example, many wellness champions assume the responsibility to communicate health and wellness resources and activities, as well as motivate colleagues to participate in wellness opportunities. In addition, some organizations encourage their wellness champions to plan and implement departmental wellness activities.
Wellness champions are a low-cost strategy as they often self-select themselves into the program and volunteer their time and energy to the role. They are considered integral to a comprehensive WHP initiative. Wellness champions can provide critical peer support needed to improve healthy behaviors among coworkers (Wieneke et al., 2016). Numerous studies have reported the use and benefits of peer support in helping people adopt healthy behaviors in various settings, including the workplace, with proper training, support, and ongoing guidance and evaluation (Aoun et al., 2017; Edmunds & Clow, 2015; Leahey & Wing, 2013; Linnan et al., 2013; Umberson & Montez, 2010). A wellness champion program is common in many WHP programs. Companies and organizations of all sizes may utilize wellness champions, together they work with the employer-sponsored WHP program. The number of wellness champions at any one company can vary greatly—from a handful to hundreds, depending on the size of the worksite. A champion network can scale to any organization.
In addition to support provided by WHP program staff, managers are vital to the success of WHP programs (Passey et al., 2018). Managers have the ability to provide support through allocating financial resources or conveying that they value and care for their employees, which is crucial to implement and sustain a WHP program (Milner et al., 2015; Noblet & Rodwell, 2010). Leaders, like managers, have the ability to impact the success of WHP programs through determining what programs and policies are disseminated and provided to employees, which impact employee well-being (Milner et al., 2015). According to Wieneke et al. (2016), direct supervisor support of the wellness champion is essential to implement a successful network. Spoonheim and Pronk (2016) suggested that wellness champions who work together with management to facilitate employee well-being was a best practice design principle of successful WHPs. Safeer and Allen (2019) emphasized the importance of formal and informal leadership support for participation in a wellness initiative at all levels. This support, in turn, can be encouraging to champions and their colleagues to engage in the WHP activities. Managers and supervisors are essential to the success of wellness champions because they provide time allocation, support, encouragement and resources to employees, including the wellness champion, within their workplace department or unit. Katz and Kahn (1978) suggested that a manager’s perception of the wellness champion shaped, in part, the wellness champion’s perception of their role, and therefore could affect a wellness champion’s engagement in providing opportunities for their colleagues to engage in healthy lifestyle behaviors.
As little is available in the literature pertaining to the association between manager support and wellness champion engagement, the purpose of this study was to investigate the relationship between perceived level of direct manager support and the participation and engagement of wellness champions at a large Mid-west public land grant university. The research question for the current investigation was “Are there perceived differences in direct manager support among Buckeye Wellness Innovators (BWIs) who were engaged or less engaged in the Buckeye Wellness Innovator program?” We hypothesized that BWIs who were less engaged in communicating wellness information, encouraging colleagues to engage in healthy behaviors, planning wellness activities will have a lower level of perceived manager support.
Methods
We employed a cross-sectional descriptive study design that employed approximately 36,000 faculty and staff at the time of the study, including approximately 27,000 staff and 9,000 tenure, clinical, research, and associated faculty across six campuses. There were 22,310 females and 13,410 males. Caucasians made up 26,000 of the total employees, minorities and other ethnicities accounted for 10,000 additional faculty and staff.
At the time of this study, the wellness champion program, entitled the Buckeye Wellness Innovator (BWI) program, included approximately 470 faculty and staff members. The BWIs were faculty and staff who volunteered to be a BWI representative in their respective department or unit. The BWI program, which began in January 2012, had the mission to facilitate a wellness culture and environment in their colleges or units. An extensive description of the BWIs has been published previously (Amaya et al., 2017). BWIs reported to a program facilitator, in addition to their primary manager, who oversaw their day-to-day role at the university. The primary manager approved both the time and resources that accompanied the BWI role and are what was referred to as “manager support” in this study.
All BWIs participating in the program at the time of the study were eligible to participate (n = 470). An anonymous Qualtrics survey link was emailed to all current BWIs in January 2017, including the consent form and confidentiality information. These emails were exchanged on a secure network and storage system through the university. One additional reminder email was sent out 10 days after the initial request, encouraging non-respondents to respond to the survey. The survey was accessible to participants for a total of 1 month. Data were reported aggregately. Respondents consented to participate in the study. Once they consented, they were directed to complete the survey.
A 15-item survey was developed with representatives from the university’s WHP program, BWI program facilitators, and faculty from the university’s Colleges of Nursing and Public Health. Items were created based on an extensive review of the literature and on the university wellness program’s requirements for a BWI. For the purposes of this study, an engaged BWI is a champion who communicated wellness opportunities with colleagues a minimum of once per month, and planned wellness-related activities in the department a minimum of three times per year. Supportive manager/supervisors were those who allowed the BWI time on the job and resources, such as space, funding, and communication opportunities, to engage in the role.
Question topics included: demographics (age, gender, race, ethnicity, education level, and job classification), length of time as a BWI, self-perceptions of engagement in his or her role as a BWI, and perceived level of support from the direct manager/supervisor. Self-perception of BWI engagement was assessed for three domains: (a) communication, (b) motivating and encouraging colleagues, and (c) planning wellness activities in their respective department. These domains were assessed using a 5-point Likert-type scale with response options ranging from “1 = I am not engaged” to “5 = I am extremely engaged.” Two questions addressed manager support using 5-point Likert-type scale: perceived support for the BWI role (“How supportive is your direct manager of your role as an Buckeye Wellness Innovator?”) and support for the engagement of the manager’s direct reports in health and wellness during the workday/shift (“How supportive do you feel your direct manager is of your colleagues’ health and wellness efforts during the work day or shift?”). Response options ranged from “1 = not supportive at all” to “5 = extremely supportive.”
Three additional survey questions were included for BWI program quality improvement purposes and not used in the analysis. These questions asked about factors that influenced the decision to become a BWI, factors that influenced the decision to remain a BWI, and departmental barriers to facilitating wellness. The study was reviewed and approved by The Ohio State University Institutional Review Board.
Data Analysis
Mean and standard deviation were used to summarize the distribution of age in the sample. Frequencies and percentages were used to summarize the distribution of responses to multiple choice questions. Chi-square tests and ANOVAs were used to compare demographics across groups defined by manager support and by engagement level. Chi-square tests were used to test for associations between manager support and levels of engagement. Due to low counts in some extreme response categories for the Likert-type items (the upper and lower ends of the scales), support and engagement questions were collapsed into three levels for analyses. For example, level of engagement was collapsed into three levels: Not engaged/slightly engaged, moderately engaged, and Very engaged/extremely engaged.
Findings
Two hundred twenty seven (n = 227) respondents partially or fully completed the survey (48% response rate). Twenty-eight of these respondents completed less than half the survey and were excluded from analysis, leaving an analysis sample of 199 (42% response rate). Importantly, the entire analysis sample (n = 199) had complete data for the questions related to our research question (engagement with and manager support of the BWI program); missing data occurred only for the demographic questions.
A demographic summary of the BWI sample who responded is shown in Table 1; characteristics of those who responded follow. The average age of respondents was 43 years (SD = 11). The sample of respondents was primarily female (86%), White (88%), of Non-Hispanic/Latino ethnicity (98%), and held a Bachelor’s degree (87%). There was a wide range of self-reported job classifications, with the largest proportions being administrative staff (39%), clinicians (18%), and managers (12%). The majority of respondents had been a BWI for 2 years or less (62%).
Demographic Summary of the Sample of Buckeye Wellness Innovators (n = 199)
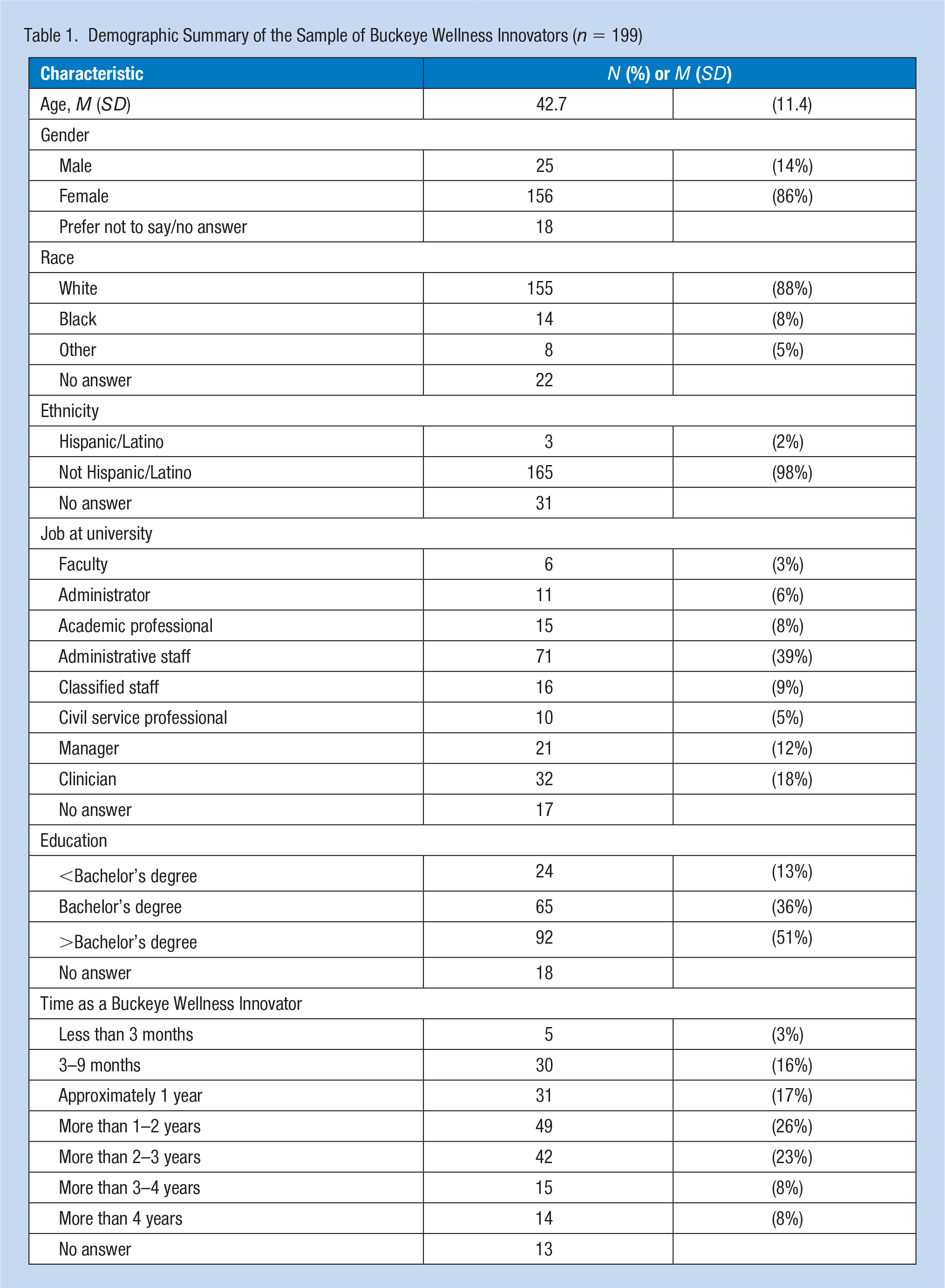
Table 2 shows the distribution of reported perceived manager support and BWI program engagement for the sample. A large majority (67%) of BWIs felt their manager was very or extremely supportive of their participation in the program as well as encouraging of their colleagues’ health and wellness efforts (63%). However, BWI program engagement was moderate, with less than half of respondents reporting being very or extremely engaged in each of the three areas of the BWI role (communication: 33%; motivating colleagues: 40%; planning activities: 38%). Only 18% of BWIs reported being very or extremely engaged in all three areas.
Distribution of Perceived Levels of Manager Support for Buckeye Wellness Innovator Role and Program Engagement Among Buckeye Wellness Innovators (n = 199)
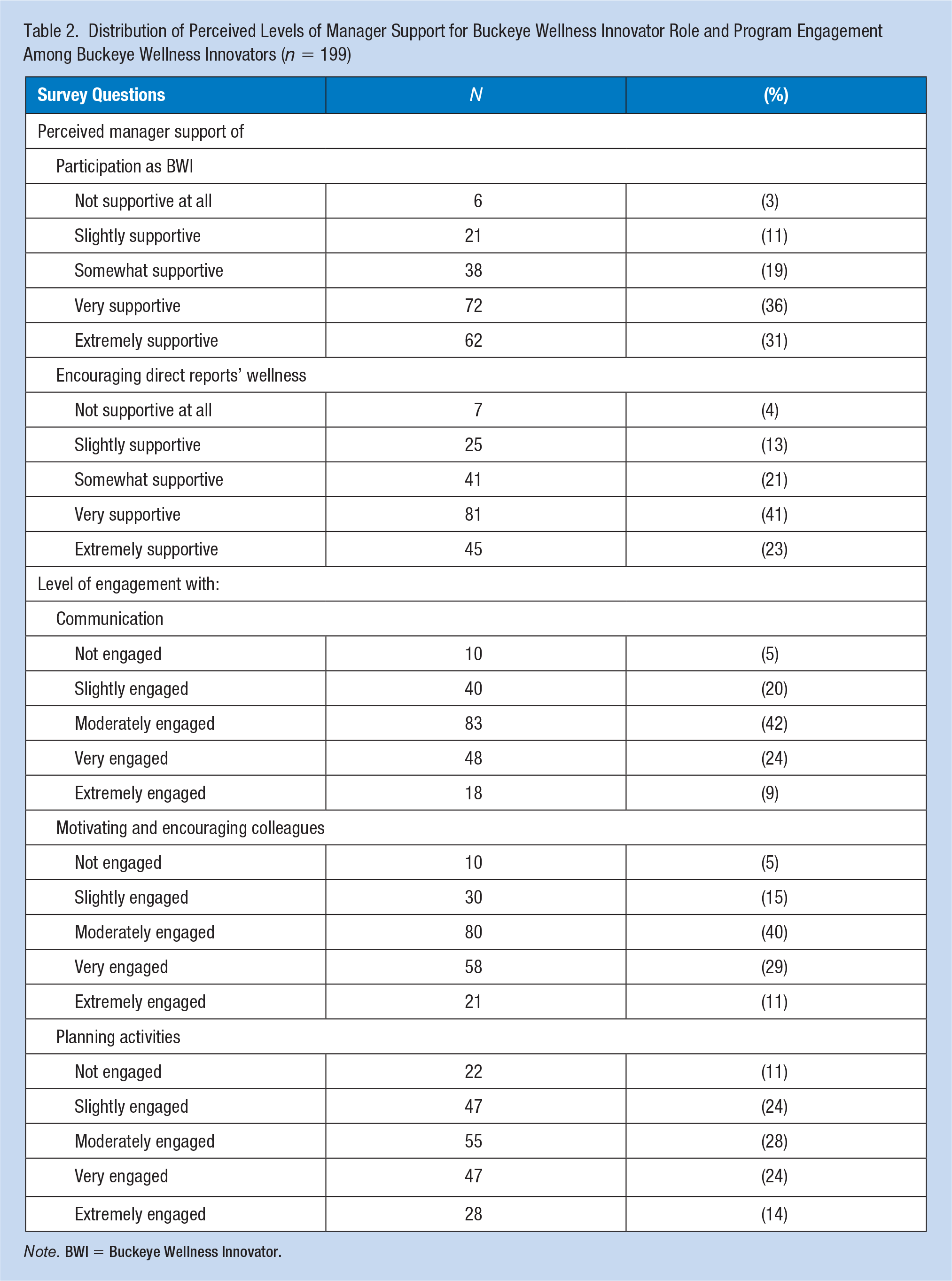
Note. BWI = Buckeye Wellness Innovator.
There were no demographic differences across groups defined by perceived manager support or engagement. For all five possible groupings (two based on support, three based on engagement), there were no differences across groups in terms of age (p > .25), gender (p > .09), race (White vs. non-White, p > .18) or education (p > .37). Surprisingly, there was also no association between length of time as a BWI and either perceived manager support (p > .36) or engagement levels (p > .49).
There was a significant association between the perceived level of manager support for the BWI role and level of engagement in communicating wellness activities (p = .0004), motivating and encouraging colleagues (p < .0001), and planning wellness activities (p = .04; Table 3). BWIs who indicated very or extremely supportive managers tended to be moderately or very/extremely engaged in all three aspects of their champion role. Nearly half of BWIs who reported extremely supportive managers reported being very/extremely engaged in communication (47%), compared with closer to one quarter of BWIs with less supportive managers (very supportive: 26%; not supportive: 28%). This pattern was similar for the other two areas of engagement, with a much larger percentage of BWIs with extremely supportive managers reporting high engagement with motivating colleagues (56%) and planning activities (48%) compared with those with lower levels of perceived manager support (31%–35%)
Association Between Perceived Level of Manager Support for Buckeye Wellness Innovator Role and Perceived Level of Manager Support for Their Direct Reports’ Engagement in Wellness Program
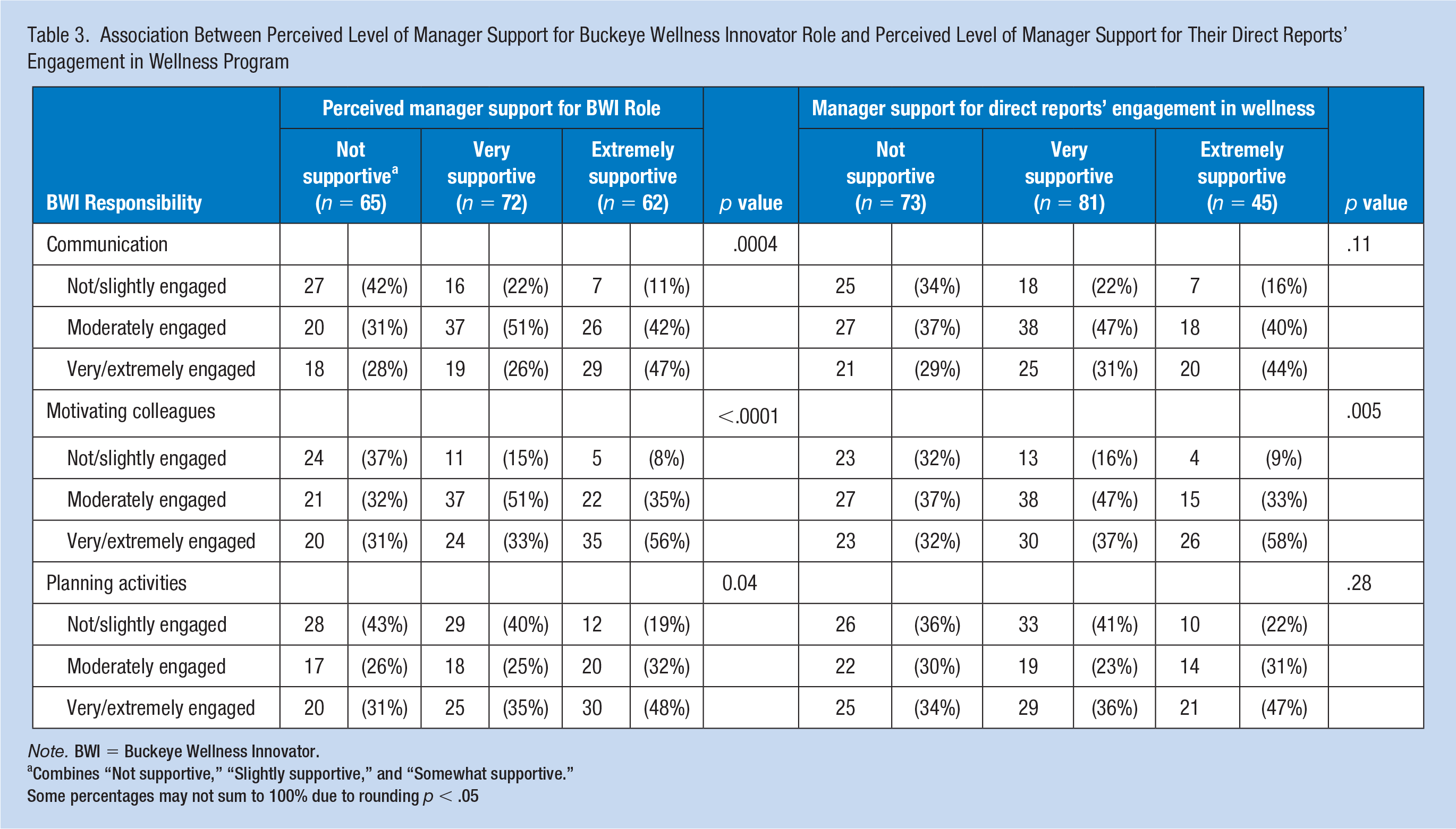
Note. BWI = Buckeye Wellness Innovator.
Combines “Not supportive,” “Slightly supportive,” and “Somewhat supportive.”
Some percentages may not sum to 100% due to rounding p < .05
The other domain of managerial support, perceived level of support for health and wellness activities during the workday, was less strongly related to BWI engagement (Table 3). Only engagement in motivating the direct reports of the manager was significantly associated with perceived manager support for wellness activities (p = .005), with 58% of BWIs with extremely supportive managers reporting being very/extremely engaged, compared with 37% of BWIs with very supportive managers and 32% of BWIs with non-supportive managers. There was not a significant association between the perceived level of support and level of BWI engagement for colleague communication (p = .11) or for planning wellness activities (p = .28).
Discussion
The findings in this study suggested that BWIs’ level of engagement in the three core areas of their role (communicating wellness initiatives, motivating and encouraging colleagues to participate in wellness activities, and planning wellness activities) was associated with perceived manager support. BWIs with higher levels of perceived manager support were more likely to report higher levels of engagement across multiple domains.
Qualities that help a wellness champion succeed in their role can be greatly influenced by the individual’s manager, which is consistent with Spoonheim and Pronk (2016). The results from this study suggested that perceived managerial support likely influenced a wellness champion’s level of engagement. In the study conducted by Wieneke et al. (2016), supervisors identified high-quality wellness champions as an essential resource for supporting the health and well-being of their employees. However, if the manager was perceived as being unsupportive of wellness champion efforts, this lack of support had the potential to lessen the impact wellness champions had on improving the health and well-being of their colleagues. Managers may be more willing to support wellness champion efforts, particularly if their performance in supporting WHP efforts opens up opportunities for salary increases and promotions (Robbins & Wansink, 2016). By recognizing the importance of manager support in wellness champion team efforts, managers can be given tools and strategies to allow them to better support a wellness champion team member. The wellness champion can then in turn continue their engagement in all facets of their roles and responsibilities, and champions and their colleagues both can participate and engage in the wellness program.
Although there were nonsignificant results for the association between perceived level of colleague support and level of BWI engagement for colleague communication or for planning wellness activities, motivating and encouraging colleagues to engage in wellness activities was significantly associated with perceived manager support. This is important to note because the more supportive a manager is perceived to be about the wellness champion encouraging their colleagues, the more likely a colleague may be to participate in wellness and self-care activities.
The results from this research study provide insight into advancing wellness champion programs. Continuous quality improvement, through the use of program evaluation and feedback from wellness champions, are needed to achieve a high performing wellness champion program. As a university-centered worksite wellness initiative, universities are unique settings that differ from, for example, corporate wellness settings. University pace tends to be slower than industry and, due to academic structures, silos can create situations where colleagues across campus do not communicate with one another. One of the reasons this wellness champion program was developed was to have a group of individuals sharing the same important health-related information with the entire university community. This purpose fulfilled one of the main reasons why a WHP was implemented: to create a culture of wellness where individuals are connected to the larger group, finding support, and encouragement to engage in healthy lifestyle behaviors.
Unfortunately, there is little in the literature to compare these results when it comes to wellness champion teams. To our knowledge, this is the first study that attempted to determine how perceived manager support was related to dependent variables we studied. In addition, demographics of worksite wellness champion teams have not been reported in any published study. The results may have been different if the program had greater racial/ethnic diversity and a greater proportion of males and faculty. With a response rate of 42% (excluding incomplete surveys), it is possible that selection bias may have influenced our results; BWIs who were more engaged or perceived greater manager support may have been more likely to complete the survey.
With all self-report surveys, response bias poses a threat. Answers may be exaggerated, respondents may not accurately reveal private details, and responses can be biased by the participant’s feelings or behaviors at the time they filled out the questionnaire. In addition, BWIs on-boarded in more recent years may have responded differently than those in the program from its inception, 6 years ago. Further, only BWIs that wanted to participate did. It was not a random sample, therefore, difficult to generalize the results to all participants in the BWI program.
The survey itself was not tested for validity and reliability. The study was implemented by a Masters of Public Health student completing a culminating project; therefore, the investigative team did not have the time to test the survey prior to dissemination. The goal was to test the survey tool for validity and reliability if disseminated in the future.
While the data provided the program facilitators with valuable information, a question regarding which factors influenced a decision to disengage from the program would have been helpful to understand among those who were not at all or less engaged. To minimize this threat, we evaluated and reported findings on potential confounders, including the distribution of time spent as a BWI. As previously stated, this study did not include a random sample. Results were limited to only those who responded.
Implications for Occupational Health Practice
WHP programs that contain wellness champion networks are still relatively new to the field of health promotion. The literature suggests their value, but only one study has attempted to determine wellness champion effectiveness (Wieneke et al., 2016). In addition, there is little to no documentation on the impact of managerial support on the fulfillment of a wellness champion’s role as a part of the WHP effort. Health promotion practitioners need to evaluate champion efforts, quantitatively and qualitatively, and share those results with the field at large. Managers need to be given the resources to better support a wellness champion in their department. Additional research in the field is needed to better determine the effectiveness of wellness champions as an evidence-based strategy to sustain a culture of wellness.
Application to Professional Practice
Wellness champion networks are an important component to workplace wellness programs. Little evidence exists regarding factors that impact wellness champion participation and effectiveness, including management support of the role. When managers and supervisors support and encourage wellness champions to engage in the role, wellness champions are more likely to communicate wellness initiatives and encourage colleagues to participate in activities to improve their overall health and well-being. As employers look to impact the health and productivity of their employees, and generate cost-savings, the findings from the present study demonstrate the use and support of wellness champions to help facilitate employee engagement in workplace wellness programs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Leah Mitchell, MPH, is a wellness program manager for Huntington Bank.
Megan Amaya, PhD, CHES is an assistant professor of clinical nursing and director of health promotion and wellness at The Ohio State University College of Nursing.
Lauren Battista, MPH, is a wellness program manager at The Ohio State University.
Bernadette Melnyk is Vice President for Health Promotion, University Chief Wellness Officer and Dean, College of Nursing, The Ohio State University.
Rebecca Andridge, PhD, is an associate professor at The Ohio State University College of Public Health.
Gail Kaye, PhD, is an associate professor at The Ohio State University College of Public Health.