
Abstract
The health status and health behaviors among support staff providing daily support for people with intellectual and developmental disabilities (IDD-SS) in community-based organizations (CBOs) have not been systematically studied. This study examined the health impact of IDD-SS workers who participated in a HealthMatters Program: Train-the-Trainer Certified Instructor Workshop followed by implementing a 12-week HealthMatters Program for people with intellectual and developmental disabilities (IDD) that they care for as part of their employment. A total of 48 IDD-SS were enrolled into either an intervention (n = 28) or control group (n = 20). IDD-SS in the intervention group received an 8-hour HealthMatters Program: Train-the-Trainer Workshop immediately prior to teaching a 12-week HealthMatters Program for people with IDD. Assessments were conducted with IDD-SS before and after completing the 12-week HealthMatters Program to evaluate whether IDD-SS experienced any benefit of the training and teaching the program on their own health and health behaviors. Relative to the control group, the IDD-SS in the intervention group showed significant improvements in social/environmental supports for nutrition (F = 4.92, p = .032), exercise outcome expectations (F = 6.58, p = .014), nutrition outcome expectations (F = 8.87, p = .005), fruit and vegetable intake (F = 13.62, p = .001), knowledge of fruit and vegetable intake recommendations (F = 11.25, p = .002), and stages of change for eating fruits and vegetables (F = 6.86, p = .012). Results demonstrated that IDD-SS benefited from the health education programming. Findings support the need to develop programs and organizational policies for health promotion activities for direct care staff.
Keywords
Introduction
The health status and health behaviors among support staff providing daily support for people with intellectual and developmental disabilities (IDD-SS) in community-based organizations (CBOs) have not been systematically studied. However, limited research to date suggests that these workers face unique and growing challenges including poor financial compensation, high stress, high job turnover rates, and expanding roles (Bogenschutz, Hewitt, Nord, & Hepperlen, 2014; Hewitt & Larson, 2007; Khatutsky et al., 2011; Zontek, Isernhagen, & Ogle, 2009). IDD-SS provide an increasingly wide range of supportive services to people with intellectual and developmental disabilities (IDD) on a day-to-day basis. These include the management of their personal care and hygiene, job support, transportation needs, recreational activities, housekeeping and other home management-related supports and services, and their complex health needs. Their service allows people with IDD “to live and work in their communities” and “to lead a self-directed family, community, and social life” (Congressional Direct Support Professional Recognition Resolution in 2003).
Health Status of IDD-SS
Gray-Stanley & Muramatsu (2011); Gray & Muramatsu, (2013); Hatton et al., (2001); and Larson & Hewitt, (2005) report that work stress is endemic among IDD-SS who support people with IDD. This contributes to their intentions to quit, as well as their high turnover rates in residential, community, and vocational settings. Improving IDD-SS health status can improve their quality of life and productivity (Hewitt & Larson, 2007; Hickey, 2014). Staff supporting people with IDD are often exposed to occupational hazards that may affect their health. For example, IDD-SS have the following types of exposures: (a) physical (e.g., ergonomic hazards from lifting and repetitive tasks, poor body mechanics, limited flexibility, falls, physical attacks from clients “acting out,” adverse effects from shift work such as sleep deprivation); (b) biologic (e.g., bacterial infections, viral infections, fungal infections, blood-borne pathogens, such as, scabies, pinworm, pink eye, ringworm, lice, which are common in group-living situations); and (c) stress (e.g., shift work stress, psychosocial induced issues including verbal threats from service recipients who are “acting out”) (Gray-Stanley & Muramatsu, 2011; Gray-Stanley et al., 2010; Marks, Sisirak, Heller, & Hsieh, 2005). Available research on IDD-SS health has focused on stress, job burnout, and psychological well-being (Ejaz, Noelker, Menne, & Bagaka’s, 2008; Hickey, 2014). In one of the few studies on health status of support staff, Marks & Sisirak (2012) reported that 64% of respondents were overweight and 32% were current smokers.
Employee Health and Workplace
Implementing workplace interventions to promote health is imperative to sustain employability for IDD-SS. Health problems and subsequent impairments can result in productivity losses at work (Alavinia, Molenaar, & Burdorf, 2009). However, for IDD-SS working in CBOs that involve providing day, residential, and employment services for people with IDD, workplace health promotion has not been a priority until recent documentation of their high levels of work-related stress (Gray & Muramatsu, 2013). Similar to research among other shift workers, IDD-SS may also have an increased risk for reduced job productivity, increased obesity, and more injuries and a wide range of chronic diseases (Caruso, 2014). In addition, shift work and long hours among IDD-SS may harm people with IDD, as research among other shift workers has reported fatigue-related errors with long work hours (Folkard & Lombardi, 2006).
Worksite Health Promotion
The need to expand health promotion and disease prevention measures to reduce harm to IDD-SS is supported by the cost of injuries and illnesses among workers in low-wage occupations to the United States which was estimated to be US$39 billion in 2010 (Leigh, 2012) compared with a total of US$250 billion across all workers (Leigh, 2011). To date, few studies show the benefits of educational and exercise programs for staff in increasing long-term workforce stability. With decreasing financial resources in CBOs and concomitant high staff turnover rates and high service recipient to support staff ratio (Hewitt & Larson, 2007), CBO directors anecdotally report high worker compensation claims and increases in sick leave. Researchers note the relationship between caregivers stress and burnout to poor health, unhealthy lifestyles, and reduced quality of life (Berry, Mirabito, & Baun, 2010; Gray-Stanley & Muramatsu, 2011; Gray-Stanley et al., 2010). For people with IDD, reducing IDD-SS stress may improve their community participation and quality of life. High turnover rates not only translate into vacancies but they are very costly for CBOs and decrease the availability of support for people with IDD (Hewitt & Larson, 2007).
Workplace health promotion can improve self-perceived health, worker productivity, and a decline in sick days (van Rijn, Robroek, Brouwer, & Burdorf, 2014). In addition, wellness programs can reduce absenteeism (Lechner, de Vries, Adriaansen, & Drabbels, 1997) and lower employees perceived stress among study participants who attended a wellness program compared with those who did not attend wellness program (Abdullah & Lee, 2012).
This study aimed to examine the impact of a HealthMatters™ Program intervention on IDD-SS’s psychosocial health status. We examined the effects of IDD-SS participating in a workshop in which they first learned to train on the subject matter, and then they implemented a 12-week HealthMatters Program for people with the IDD who were receiving services. More specifically, we examined the effects of both the workshop intervention (aimed at IDD-SS) and a 12-week health promotion program (aimed at participants with IDD, led by IDD-SS caregivers who were trained) on IDD-SS.
Methods
Study Intervention
The IDD-SS included in the intervention group attended an 8-hour HealthMatters Program: Train-the Trainer Workshop for staff to gain skills to lead a 12-week HealthMatters Program for people with IDD. This study examined the effects of their involvement with the initial workshop, followed by their leadership of the 12-week program for IDD that they cared for. For clarity, both programs are referred to as HealthMatters Program, unless specified otherwise.
HealthMatters Program: Train-the-trainer workshop for staff
IDD-SS in the intervention group attended an 8-hour, small group (7-10 staff), on-site HealthMatters Program: Train-the-Trainer Workshop (HMP: TtT Workshop) (Marks, Sisirak, & Chang, 2013) lead by the Principal Investigator and the Project Coordinator. The HMP: TtT Workshop objectives consisted of the following: (a) reviewing the importance of physical activity, exercise, and nutrition for people with IDD; (b) identifying barriers and social and environmental supports for motivating and engaging people with IDD in physical activity and health education; (c) discussing teaching strategies to convey core concepts of physical activity, exercise, and nutrition to people with IDD (e.g., heart rate, blood pressure, use of equipment, and safety) using the Health Matters: The Exercise, Nutrition, and Health Education Curriculum for People with Developmental Disabilities (Health Matters Curriculum) (Marks, Sisirak, & Heller, 2010); (d) implementing customized physical activity, exercise, and nutrition activities tailored to the needs of adults with IDD; and (e) supporting people with IDD to sustain a health promotion program in their day/worksite programs.
The HMP: TtT Workshop, developed through focus groups with staff in CBOs and pilot tested through large statewide trainings, was divided into five interactive modules based on the Transtheoretical Model of Behavior Change (J. O. Prochaska & DiClemente, 1983; J. O. Prochaska, DiClemente, & Norcross, 1992; J. O. Prochaska et al., 1994) and the principles of Bandura’s Social Cognitive Theory (Bandura, 1977, 1986) to provide staff with the theoretical underpinnings for adopting health behaviors. The transtheoretical approach to behavior change uses five stages in which one gains knowledge, skills, motivation, and readiness which modify or change a particular behavior. The five stages are as follows: (a) Precontemplation, (b) Contemplation, (c) Preparation, (d) Action, and (e) Maintenance. The principles of Bandura’s Social Cognitive Theory (Bandura, 1977, 1986) guided this study and were integrated throughout all of the workshop modules. A comprehensive overview of the HMP: TtT Workshop and the 12-week HealthMatters Program is described elsewhere (Marks et al., 2013).
IDD-SS attended the HMP: TtT Workshop immediately before they implemented the 12-week HealthMatters Program for people with IDD. Technical assistance from the research team was provided to IDD-SS participants throughout the duration of the 12-week program via phone, email, and site visits.
12-week HealthMatters program for people with IDD
As a part of the intervention group, IDD-SS participants also taught the 12-week HealthMatters Program (12-week HMP) for people with IDD immediately following their HMP: TtT Workshop. During the evidence-based HMP: TtT Workshop, IDD-SS participants in CBOs, along with the research team’s guidance, developed a tailored physical activity program for participants with IDD to engage in an hour of physical activity and an hour of health education using the theoretically driven, evidence-based Health Matters: The Exercise, Nutrition, and Health Education Curriculum for People with Developmental Disabilities (Health Matters Curriculum) (Heller, Hsieh, & Rimmer, 2004; Marks et al., 2013; Marks et al., 2010), 3 days a week for 12 weeks.
Design and Participants
This study employed pretest–posttest control group design. Experienced and trained research team implemented the same standardized research protocol and intervention at each CBO research site, described below. The HMP: TtT Workshop training that the IDD-SS attended took place at each CBO research site. This was followed by a 12-week HMP that was delivered at each CBO day program and led by the trained IDD-SS intervention participants.
Study Sites—CBOs
IDD-SS were recruited from six CBO day programs in two metropolitan areas in the Midwest and Southwest of the United States. CBOs are community organizations that provide a variety of long-term residential, day, and employment services and supports to children and adults with IDD. CBOs may have day and residential services or both, transition, employment, and mental health services. Selection of CBOs was completed via active recruitment and advertising through Listserv, online, and word of mouth. CBO sites were selected if they were service providers to people with IDD and had day or residential services.
Study Participants and Recruitment
IDD-SS participants who took part in the study were employees from the recruited CBOs. IDD-SS participants were eligible for the study (both intervention and control) if they met the following criteria: aged 18 years and over, currently working with people with IDD, a commitment to devote time to program (i.e., 6 hours per week), and able to read, understand, and/or speak English.
CBO administrators designated a recruitment coordinator, who was not involved with the research project (avoiding potential “implicit pressure” in the recruitment process), to initiate the recruitment and consenting process for IDD-SS participants. The information and training on ethical principles for research provided by researchers to each CBO Recruitment Coordinator is described in detail elsewhere (Marks et al., 2013). The research team invited IDD-SS at each CBO to a 1-hour recruitment presentation reviewing the research purpose, study protocol, study risks, and anticipated benefits. An opportunity was provided for everyone to ask questions about the research project. IDD-SS participants who expressed an interest and met the criteria were given a consent package explaining the study aim, required data collection, and intervention details.
Participant Randomization Procedure
IDD-SS were randomized into intervention or waiting list control group based on the randomized assignment for people with IDD whom they were directly supporting. For example, if a participant with IDD was randomly assigned to intervention group, the IDD-SS assigned to that participant with IDD was automatically enrolled in the intervention group. The purpose of this assignment was multifaceted: (a) to prevent cross contamination of intervention and control groups and (b) to ensure that the program was run by IDD-SS who were familiar to participants with IDD in the intervention group. IDD-SS in the intervention group were immediately trained. Waiting list control group participants were asked to maintain their normal work and lifestyle behaviors. After 6 months, IDD-SS participants who were in the waiting list control group were offered the HMP: TtT Workshop. IDD-SS in the intervention group attended the 8-hour HealthMatters Program: Train-the-Trainer Workshop (HMP: TtT Workshop) (Marks et al., 2013) and the led 12-week HealthMatters Program (12-week HMP) for People with IDD.
Measures
All IDD-SS participants completed measures at the same time points: at baseline (T1) and at 12 weeks (T2), immediately after the 12-week HealthMatters Program. Measures described below were administered at both data collection points.
IDD-SS participants responded to each of the following measures in paper format.
Demographic variables included age, gender, race and ethnicity, marital status, and education. Perceived General Health Status (1 item) measured participants perceived health status (Idler & Benyamini, 1997; Kawada, 2003; Lawton, Moss, Fulcomer, & Kleban, 1982; Ware & Sherbourne, 1992). Response options were 1 = Poor, 2 = Fair, 3 = Good, 4 = Very Good, and 5 = Excellent. Higher score represents better general health condition.
IDD-SS reported their energy level (5 items, Cronbach’s α = .94; e.g., level of pep and energy [Lorig et al., 1996; Stewart, Hays, & Ware, 1992]) and Well-Being / Distress Scale (5 items, Cronbach’s α = .80; e.g., worn out, tired, level of fatigue [Medical Outcomes Study Mental Health Index III; Stewart, Hays, & Ware, 1988; Stewart et al., 1992; Ware, Kosinsk, & Dewey, 2000; Ware & Sherbourne, 1992]) during the past month. Response options for both scales were 0 = none of the time, 1 = a little of the time, 2 = some of the time, 3 = a good bit of the time, 4 = most of the time, and 5 = all of the time. Item scores were summed to yield the total score. The higher the total scores, the higher IDD-SS participant’s energy level and well-being.
Pain (2 items, Cronbach’s α = .64) measured the degree to which participants reported bodily pain and how much the pain interfered with their normal work, during the past 4 weeks (Jette, 1980). Item scores were summed to yield a total score with a higher total score indicating greater pain—5-point and 6-point Likert-type scale, from 1 = not at all to 5 = extremely and 1 = none to 5 = very severe, respectively.
Barriers to Exercise Scale (18 items, Cronbach’s α = .92) (Heller, Hsieh, & Rimmer, 2002; Heller et al., 2004; Heller, Rimmer, & Rubin, 2001) and Barriers to Eating Fruits and Vegetables (14 items, Cronbach’s α = .89) (Marks et al., 2010) assessed participant’s perceived barriers to exercising and eating fruits and vegetables using two separate scales with a similar format. A higher total score indicates encountering more barriers. Both scales used a 5-point Likert-type scale, from 1 = strongly disagree to 5 = strongly agree.
The Social/Environmental Supports for Exercise Scale (15 items, Cronbach’s α = .88) and the Adapted Social/Environmental Supports for Nutrition Scale (10 items, Cronbach’s α = .67) (Marks et al., 2010; Sallis, Grossman, Pinski, Patterson, & Nader, 1987) are two separate scales that used the same rating format to assess the amount of support for exercising and eating fruits and vegetables. IDD-SS participants were asked the frequency that someone (i.e., family, friends, or health care provider) provides support for exercising or eating healthy. A higher total score indicates more perceived support. The response options were 0 = none, 1 = rarely, 2 = a few times, 3 = often, and 4 = very often.
Body mass index (BMI; calculated as weight in kilograms divided by height in meters squared—kg/m2) was calculated based on IDD-SS participants’ self-report of weight (kg) and height (m). The response options were 1 = underweight, 2 = normal, 3 = overweight, 4 = obese, and 5 = extremely obese.
The Exercise (12 items, Cronbach’s α = .90) and Nutrition Outcome (7 items, Cronbach’s α = .92) Expectation Scales assessed participant’s level of positive expectations regarding the benefits of exercising and eating fruits and vegetables. For both the Exercise Outcome Expectations Scale (Heller & Prohaska, 2001) and the Nutrition Outcome Expectations Scale (Baranowski et al., 2000; Baranowski et al., 2007), a higher total score represents more positive outcome expectations about exercise or nutrition. Both scales used a 5-point Likert-type scale, from 1 = I disagree very much to 5 = I agree very much.
The Self-Efficacy Scale also contains two subscales. The 15 items (Cronbach’s α = .95) Self-Efficacy to Exercise Scale (Sallis, Pinski, Grossman, Patterson, & Nader, 1988) and the 8 items (Cronbach’s α = .92) Self-Efficacy to Nutrition Scale (Baranowski et al., 2000) measured the degree of IDD-SS participant’s confidence to exercise and eat fruits and vegetables, respectively. A higher total score represents more confidence. Both subscales used a 5-point rating scale, from 1 = not at all confident to 5 = totally confident.
Exercise/Physical Activity Participation was measured by two scales (Centers for Disease Control and Prevention [CDC], 2005). The first scale (7 items, Cronbach’s α = .72) lists participation in exercises (e.g., stretching and walking). IDD-SS participants were asked how much time they spend on these specific activities per week. A higher total score indicates higher physical activity participation. Response options were 0 = none, 1 = less than 30 minutes/week, 2 = 30 to 60 minutes/week, 3 = 1 to 3 hours/week, and 4 = more than 3 hours/week. The second scale (7 items, Cronbach’s α = .82) asked IDD-SS participants how often they engaged in types of physical activities (e.g., climbing stairs). A higher total score indicates higher activity participation. Response options were 0 = 0 days/week, 1 = 1 to 2 days/week, 2 = 3 to 4 days/week, 3 = 5 to 6 days/week, and 4 = 7 days/week.
Fruit and Vegetable (F&V) Intake and Recommendation was measured by two questions (Beresford et al., 2001). IDD-SS were asked how many servings of fruits and vegetables they eat per day and how many servings of fruits and vegetables they “should” eat per day for good health. Response options for both items were 0 = 0, 1 = 1, 2 = 2, 3 = 3, 4 = 4, 5 = 5 to 9.
Health behavior stages of change were measured for exercise (Nigg et al., 2005) and fruit and vegetable intake (Beresford et al., 2001). Using the Transtheoretical Model of Behavior Change, the two scales assessed IDD-SS participant’s readiness to change a health behavior for physical activity (4 items) and health behavior stage fruit and vegetable intake (4 items) through five stages that represent incremental increases in preparedness to change (e.g., do you currently engage in regular physical activity, do you intend to engage in regular physical activity in the next 6 months, in the next 30 days, or have you been regularly physically active for the past 6 months) across the following five stages: (a) precontemplation, (b) contemplation, (c) preparation, (d) action, and (e) maintenance (J. O. Prochaska & DiClemente, 1992). Response options were 1 = pre-contemplation, 2 = contemplation, 3 = preparation, 4 = action, 5 = maintenance.
Data Analysis
To determine the existence of group differences, independent t test was used to compare age of IDD-SS participants in intervention group to control group at baseline (T1). The differences between the groups for categorical demographic variables (e.g., gender and race) were measured using chi-square tests. A significance level of .05 was used. T1 scores were treated as covariates to assess the differences in the posttest means after accounting for pretest values. To investigate the effectiveness of the intervention, the difference of the score changes (T1 to T2) between intervention and control group participants was examined by analysis of covariance (ANCOVA) with the dependent variable as the posttest measure. SPSS for Windows, version 22.0 (2013), software was used for data analysis.
Ethical Review
This study was reviewed and approved by the University of Illinois at Chicago Institutional Review Board (IRB). Each CBO was deemed a performance site, which required participating CBOs to obtain a Federalwide Assurance (FWA) for the Protection of Human Subjects and to secure IRB approval. Each CBO obtained a FWA number through a formal application submitted to the U.S. Department of Health and Human Services (HHS), Office for Human Research Protections (OHRP).
Results
IDD-SS Participants
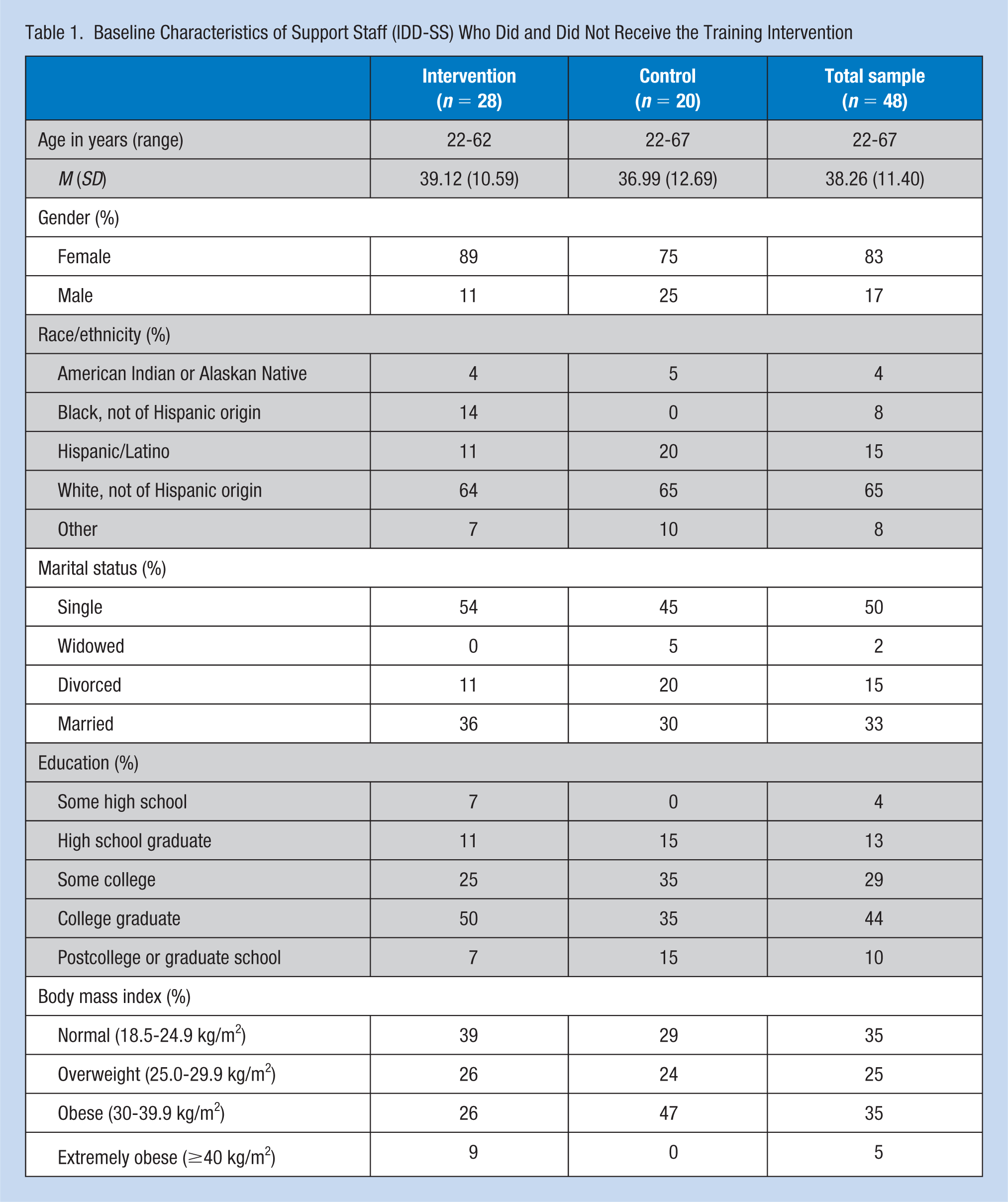
The study included 48 IDD-SS participants. The sample size in the intervention group was 28 and the 20 IDD-SS in the control group. The average age for the 48 IDD-SS participants was 38.26 years (SD = 11.40; Table 1). The majority of participants were female (83%) and White, not of Hispanic origin (65%). Half of participants were single and 33% were married. Regarding education attainment, most participants had some college or a higher degree (83%). Finally, 65% of participants’ BMI was in the range of either overweight or obese. Intervention and control groups did not show significant differences in age or any other demographic variables and were not included as covariates in subsequent analyses.
Baseline Characteristics of Support Staff (IDD-SS) Who Did and Did Not Receive the Training Intervention
Health Status, Barriers, and Supports
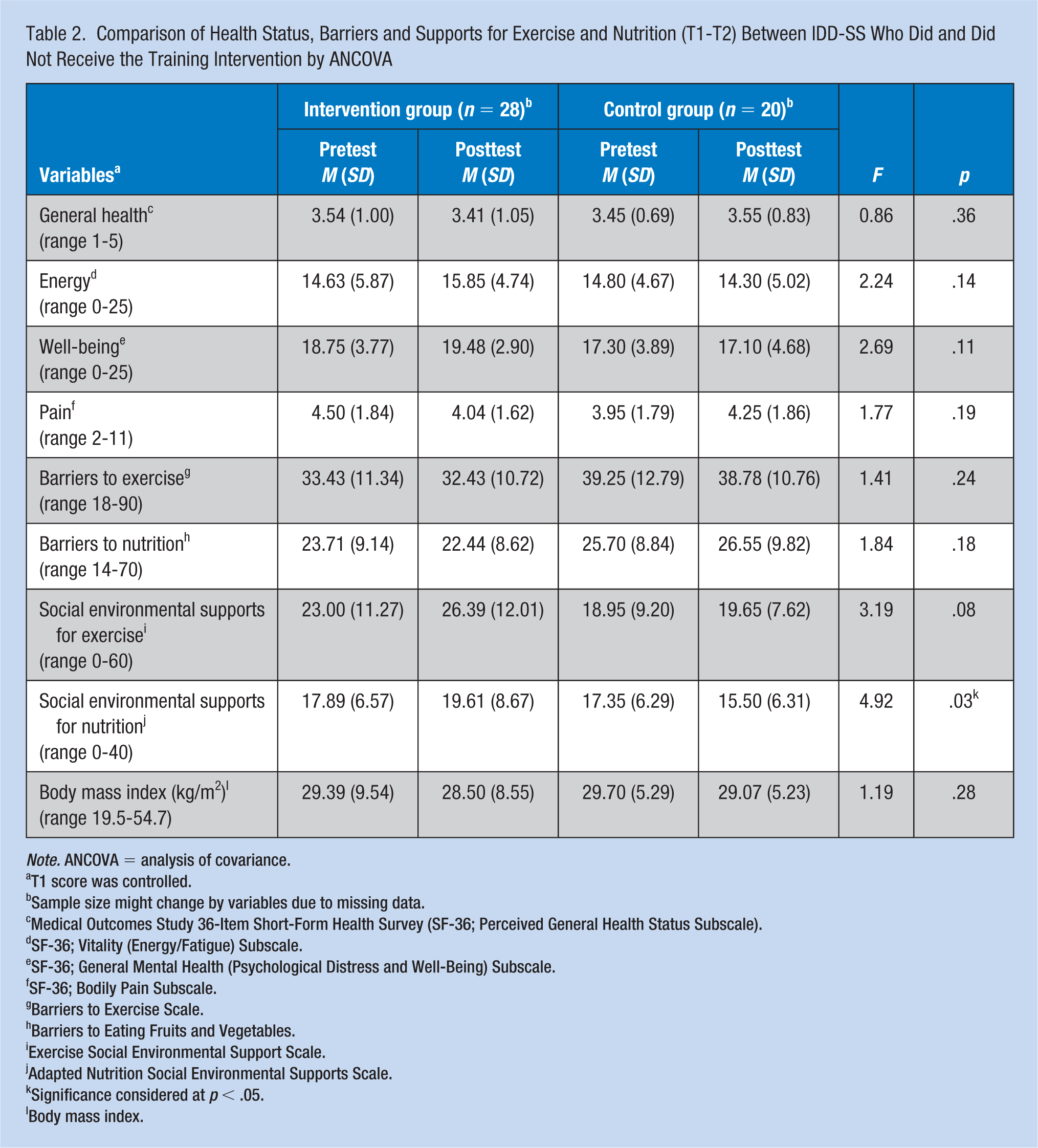
Over 92.8% of the intervention group reported that their health was either excellent or very good compared with 95% of the control group at baseline (data not shown). Neither group reported a significant change in their general health self-rating score at posttesting (81% for intervention and 90% for control group). After taking the HM: TtT Workshop and teaching the 12-week HealthMatters Program, the intervention group showed significant improvement in social/environmental supports for nutrition (F = 4.92, p = .03) when controlling for pretest mean scores (Table 2).
Comparison of Health Status, Barriers and Supports for Exercise and Nutrition (T1-T2) Between IDD-SS Who Did and Did Not Receive the Training Intervention by ANCOVA
Note. ANCOVA = analysis of covariance.
T1 score was controlled.
Sample size might change by variables due to missing data.
Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36; Perceived General Health Status Subscale).
SF-36; Vitality (Energy/Fatigue) Subscale.
SF-36; General Mental Health (Psychological Distress and Well-Being) Subscale.
SF-36; Bodily Pain Subscale.
Barriers to Exercise Scale.
Barriers to Eating Fruits and Vegetables.
Exercise Social Environmental Support Scale.
Adapted Nutrition Social Environmental Supports Scale.
Significance considered at p < .05.
Body mass index.
Although not statistically significant, several other variables showed a positive increase in mean posttest scores for the intervention group as compared with the control group, suggesting a general positive impact of the HealthMatters Program on the health and health behaviors of staff supporting adults with IDD. For example, participants in the intervention group reported increased energy and well-being, decreased pain, decreased barriers to exercise and barriers to nutrition, increased social/environmental supports for exercise, and decreased BMI. Conversely, analyses of several variables showed negative changes in posttest mean scores for the control group. For example, perceptions of energy level and well-being decreased, pain increased, barriers to nutrition increased and social/environmental supports for nutrition decreased.
Outcome Expectations, Self-Efficacy, Health Behaviors, and Stages of Change
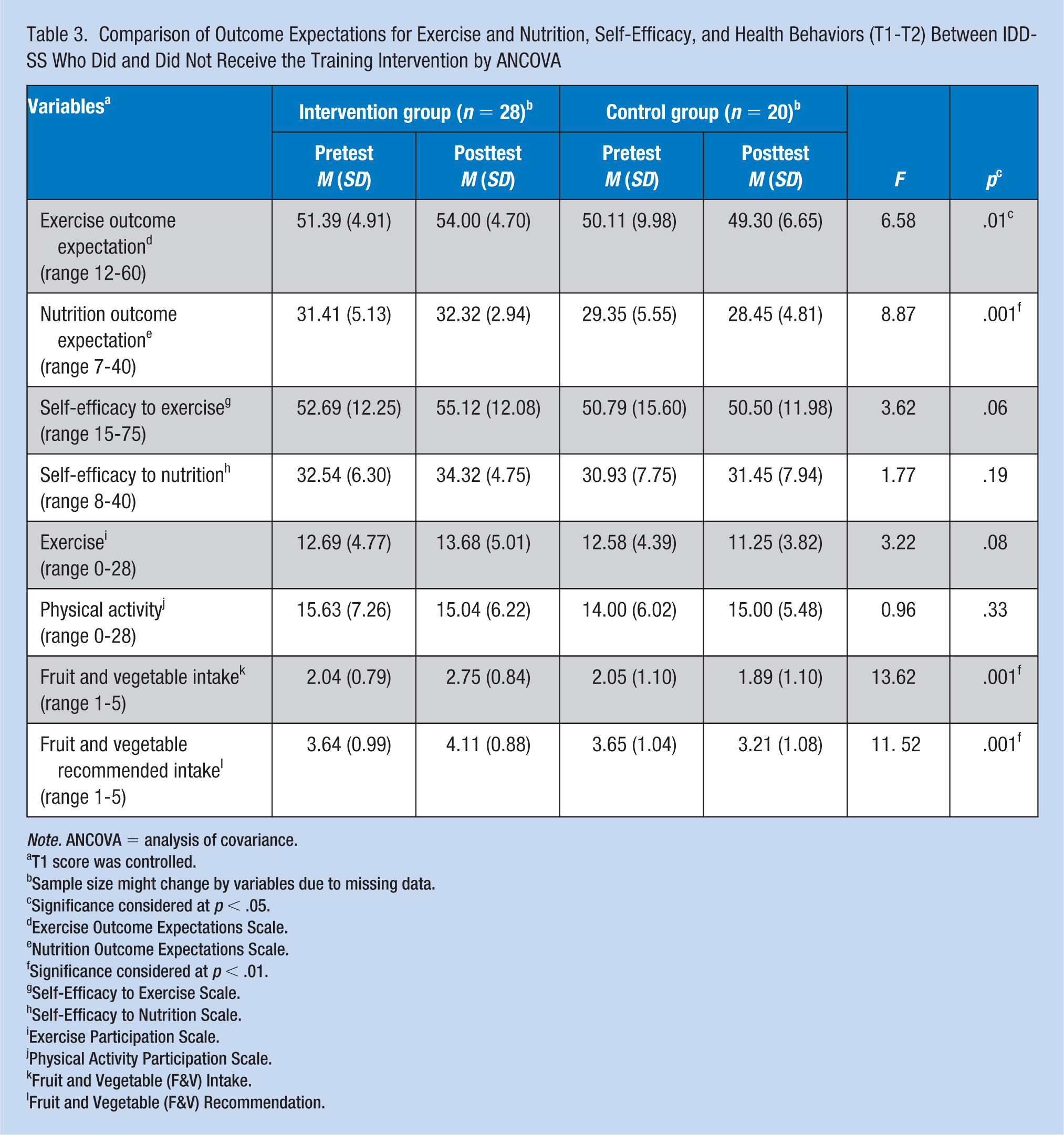
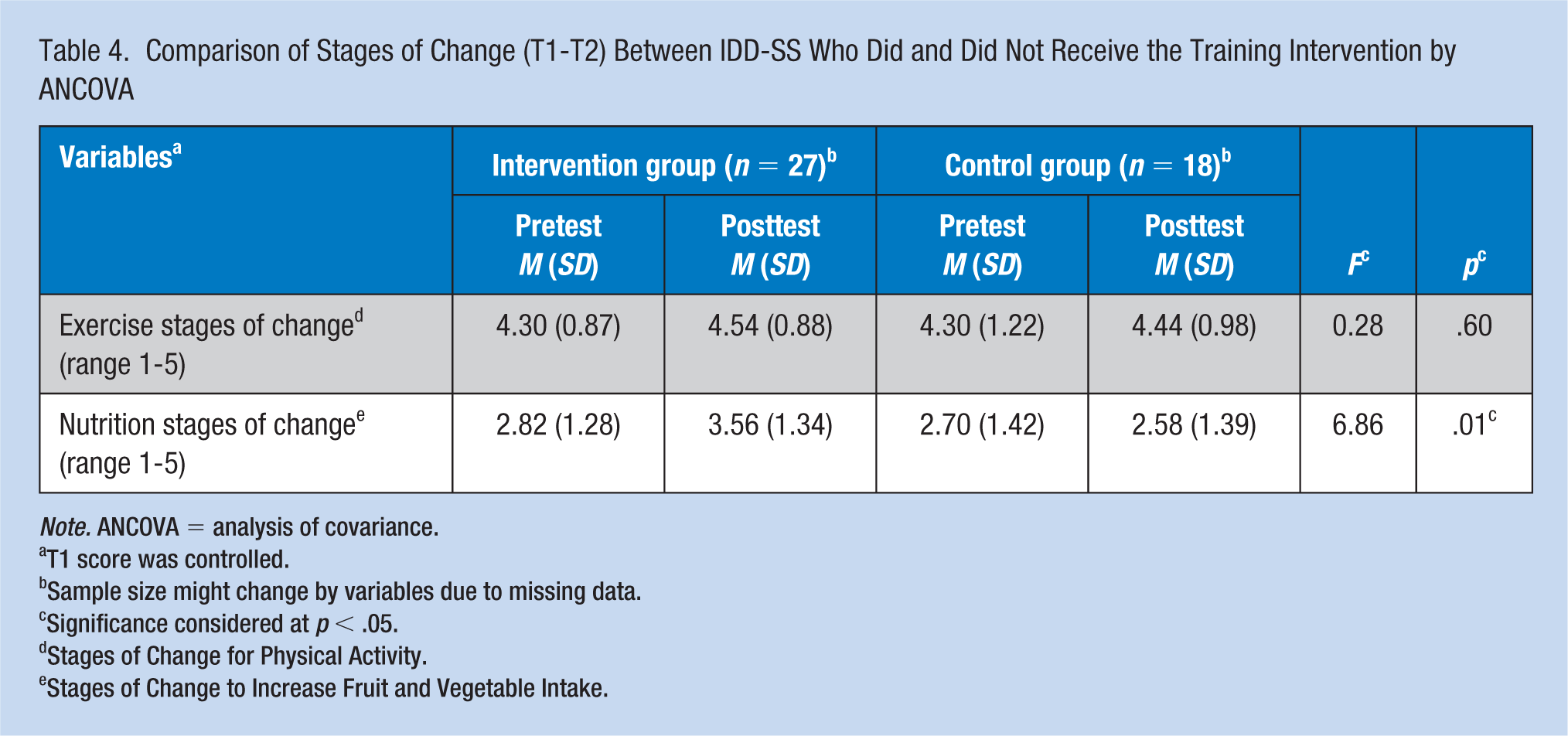
The intervention group showed significant improvements across several variables after taking the HM: TtT Workshop and teaching the 12-week Health Promotion Program. When controlling for pretest mean scores, the following improvements were noted (Tables 3 and 4): (a) increased exercise outcome expectations (F = 6.58, p = .01) and nutrition outcome expectations (F = 8.87, p = .00), (b) greater intake of more fruits and vegetables (F = 13.62, p = .00) and knowledge of recommended fruit and vegetable intake (F = 11.25, p = .00), and (c) improved readiness to eat more fruits and vegetables (Nutrition Stage of Change) (F = 6.86, p = .01)
Comparison of Outcome Expectations for Exercise and Nutrition, Self-Efficacy, and Health Behaviors (T1-T2) Between IDD-SS Who Did and Did Not Receive the Training Intervention by ANCOVA
Note. ANCOVA = analysis of covariance.
T1 score was controlled.
Sample size might change by variables due to missing data.
Significance considered at p < .05.
Exercise Outcome Expectations Scale.
Nutrition Outcome Expectations Scale.
Significance considered at p < .01.
Self-Efficacy to Exercise Scale.
Self-Efficacy to Nutrition Scale.
Exercise Participation Scale.
Physical Activity Participation Scale.
Fruit and Vegetable (F&V) Intake.
Fruit and Vegetable (F&V) Recommendation.
Comparison of Stages of Change (T1-T2) Between IDD-SS Who Did and Did Not Receive the Training Intervention by ANCOVA
Note. ANCOVA = analysis of covariance.
T1 score was controlled.
Sample size might change by variables due to missing data.
Significance considered at p < .05.
Stages of Change for Physical Activity.
Stages of Change to Increase Fruit and Vegetable Intake.
Additional variables showed a positive trend in mean posttest scores for the intervention group, such as improved self-efficacy for exercise and self-efficacy for nutrition, increased exercises and daily activities, and improved readiness to exercise more (Exercise Stage of Change). Conversely, control group participants reported negative changes in mean posttest scores across several variables. For example, IDD-SS participants in the control group reported less knowledge of recommended fruit and vegetable intake, decreased exercises and daily activities, reduced readiness to eat more fruits and vegetables (Nutrition Stage of Change).
Discussion
This study is one of the first intervention studies examining the efficacy of a staff-led exercise and health education program on health and health behaviors among staff supporting people with IDD in community settings. Results provide evidence supporting the benefits of health promotion education for IDD-SS to improve health status and health behaviors using a train-the-trainer model. While the HealthMatters Program aimed to provide IDD-SS participants with knowledge, resources, and skills to teach and support service recipients with IDD to improve their health status, IDD-SS participants were able to transfer this information to make improvements within their own social and environmental networks and make health behavior changes. The significant improvement related to IDD-SS’s expectations toward eating more fruits and vegetables and being more physically active is an outcome that can have a positive impact on themselves and the people they support.
About two thirds of the IDD-SS participants in this study were overweight and obese, which is similar to the United States adult data, and reveals a critical obesity issue among staff in CBOs warranting further study. The significant improvement in IDD-SS participant’s nutrition-related outcomes, including social-environmental supports for nutrition, nutrition outcome expectations, fruits and vegetables intake, and knowledge of recommended fruits and vegetables intake is an interesting finding and calls for a well-planned, behavior-focused nutrition education intervention. As only one exercise-related outcome, exercise outcome expectation, showed significant improvement, this raises several considerations for researchers and practitioners in regard to the benefits of asking IDD-SS to change more than a single behavior at a time with a worksite health promotion program. Although research has documented the benefits of intervening on multiple health behaviors (J. J. Prochaska, Spring, & Nigg, 2008), people may be feel confused and overwhelmed about changing multiple behaviors at the same time (Sweet & Fortier, 2010). Furthermore, while a combination of improved diet and increased physical activity leads to a healthier lifestyle, changes to diet may be easier to make than the changes to physical activity, as food and eating are already a part of everyday life and increasing physical activity requires additional effort to incorporate in a busy schedule.
Another consideration with the intervention showing greater nutrition-related benefits may be the limitations of focusing solely on educational and motivational programs for individuals and a need to consider behavioral influences beyond the person, such as the built environment (Sallis, Floyd, Rodríguez, & Saelens, 2012). At work, IDD-SS could likely control their food options and engage colleagues for social support. However, changing behavior related to physical activity or exercising while working may be more challenging without organizational support for access, time, and/or space. Research supports the impact of enhancing the built environment to improve physical activity levels among disadvantaged populations (Benton, Anderson, Hunter, & French, 2016). Worksite health promotion programs for staff supporting people with IDD may consider organizational/environmental approaches to promoting health for all (e.g., people with IDD, employees, family members). With organizational support, the sustainability of changing health behaviors among IDD-SS may have more potential for success.
Although not a significant finding, intervention group participants reported a slight increase in exercise and physical activity after the intervention compared with controls with the mean exercise scores in both groups ranging from low to moderate. Of note is that both groups reported being in either the action or maintenance stage for engaging in regular exercise. Researchers document that differences in one’s level of awareness of his or her activity level may therefore have important implications related to health status. For example, people who overestimate their physical activity level have been found to be healthier than people who are aware of their low activity level (van Sluijs, Griffin, & van Poppel, 2007) and have a lower BMI (Watkinson et al., 2010). Health promotion strategies may need to first focus on interventions that increase one’s awareness about how physically active he or she is. With increasing access to low cost wearable technology devices, worksite health promotion programs may provide employees with wearable devices to help people to get more accurate data to assess and track their daily health-related behaviors, such as number of steps walked, heart rate, steps climbed, and intensity of activity versus physical activity.
Study Limitations
Like many worksite health promotion research (Rongen, Robroek, van Lenthe, & Burdorf, 2013), our sample size was small and likely reduced our power to detect statistical differences and finding an effect. As noted by Rongen et al. (2013), the effectiveness of a workplace health promotion programs is often dependent on the study population, intervention content, and methodologic quality of the study. This study did not develop a targeted intervention for support IDD-SS. Moreover, while we found that IDD-SS could benefit from health promotion education, translating these results across other CBOs to achieve reach, adoption, implementation, and maintenance is limited due to the small sample size. Future research would benefit from focusing on employee health with more CBOs and a larger sample size. Although our study population is representative of the workforce in many community organizations across the country, generalizability is restricted to IDD-SS participants within this study.
Implications for Future Studies
Worksite health promotion research in CBOs providing day and residential supports for people with IDD lags decades compared with research within the general population. Future studies may evaluate the impact of the HealthMatters Program with a larger sample of IDD-SS to evaluate outcomes over a longer period of time. Intervention may be broadened to address specific health promotion needs and supports for IDD-SS. Research may also include more CBOs in different geographic areas to systematically evaluate IDD-SS’s perceived barriers and outcome expectations related to physical activity and nutrition and develop new strategies to incorporate built environment within the workplace with social/environmental supports for healthier lifestyles. Studies show that the built environment can enrich the necessary resources to affect health, health promotion, and disease prevention in the general population and other underserved/under-represented populations (Lee & Rubin, 2007). Future research should develop and evaluate best practices for implementing and sustaining worksite policies and procedures that encourage employees to exercise and provide easy access to healthier food choices.
Future studies may examine correlations across various job titles to provide useful data for tailoring worksite health promotion interventions for employees depending on their needs and job responsibilities. One example is to build an ANCOVA model with a composite endpoint of posttest scores regressed against both prior performance and demographic variables (e.g., age, job title, stage of change) to get at an “Overall Impact” of the HealthMatters Program.
Many CBOs struggle with access to face-to-face training, such as lack of consistency due to skill levels in trainees, high IDD-SS turnover rates, scheduling difficulties, and high costs. Future studies may assess the impact of web-based health promotion training to IDD-SS as an alternative to face-to-face training. Evaluating innovative pedagogical methods of teaching can provide needed information on how to improve health status and health behaviors among employees. Addressing the health needs and behaviors of support staff provides an opportunity to examine effective strategies to improve their health so that they can better care for people with IDD. With the multitude of work expectations for IDD-SS, improving their health and health behaviors is critical in achieving better health outcomes for people with IDD.
Implications for Occupational Health Nursing Practice
Employees who support people with IDD in day, residential, and employment settings often receive little to no resources that can be used to promote their health. Providing nurses employed within CBOs with educational resources on best practices related to health and safety within the context of CBO wellness committees has the potential to improve the health of IDD-SS and people with IDD. In addition, understanding occupational health principles will support nurses to assume a leadership role to implement organizational health and wellness programs that create an organization-wide culture of health for everyone.
By having a conceptual understanding of occupational health nursing (OHN) principles and evidence-based and evidence-informed practices, nurses may be better prepared to advise management on strategies that can be considered and implemented for people with IDD in the labor force. Further research on an expanded role that incorporates OHN best practices can evaluate whether IDD-SS and people with IDD experience improved health status, along with a reduction in health insurance rates, sick days, and emergency department visits. Finally, research can assess the benefits of teaching IDD-SS to consider their own health when working with service recipients using a comprehensive occupational health and safety model to frame CBOs’ policies and procedures.
Applying Research to Practice
Support staff providing daily support for people with intellectual and developmental disabilities (IDD-SS) in community-based organizations (CBOs) represent a large, underserved workforce in need of health and wellness activities within worksite health promotion programs. The health impact of IDD-SS who participated in HealthMatters Program Workshop and implemented a 12-week HealthMatters Program for people with IDD was examined. Significant improvements related to social/environmental supports for nutrition, nutrition outcome expectations, fruit and vegetable intake, knowledge of fruit and vegetable intake recommendations, and stages of change for eating fruits and vegetables were noted. Occupational health nurses could develop and/or support programs and organizational policies to improve health and health behaviors among IDD-SS workers through health promotion activities so that they can provide better care and achieve optimal health outcomes for people with IDD.
Footnotes
Acknowledgements
We would especially like to extend our gratitude to all of the people who participated in the research project and provided invaluable information and feedback. The ongoing interest and support provided through our community academic partnership, including Dina Donohue-Chase, CEO at NorthPointe Resources, Inc., and Ed Kaul, President/Chief Executive Officer at ARCA, has been invaluable. The authors thank Rubia E. Magallanes, MEd, for her review of the manuscript.
Authors’ Note
This research study was approved through the University of Illinois Office for the Protection of Research Subjects (OPRS) Protocol no. 2004-0113.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported by funding from the U.S. Department of Education, Office of Special Education and Rehabilitative Services, National Institute on Disability and Rehabilitation Research (grant nos H133B080009 and H133B130007) and U.S. Department of Health and Human Services, Administration for Community Living (ACL), National Institute on Disability, Independent Living, and Rehabilitation Research (NIDILRR) (grant no. 90RT5020-03) to the Rehabilitation Research and Training Center on Developmental Disabilities, University of Illinois at Chicago, and The Retirement Research Foundation. The content does not necessarily represent the policy of the U.S. Department of Education, and endorsement by the Federal Government should not be assumed.
Author Biographies
Beth Marks, PhD, RN, FAAN, is a research associate professor in the Department of Disability and Human Development, at the University of Illinois at Chicago (UIC). She directs research programs related to the empowerment and advancement of people with disabilities through health promotion initiatives and primary health care. She has published numerous articles and books related to disability, health promotion, health advocacy, and primary health care and co-produced a documentary film entitled Open the Door, Get ‘Em a Locker: Educating Nursing Students with Disabilities.
Jasmina Sisirak, PhD, MPH, is a research assistant professor, in the Department of Disability and Human Development, at the University of Illinois at Chicago. She directs health promotion research projects related to nutrition and health promotion for persons with intellectual and developmental disabilities. She has published articles, chapters, and research briefs in the areas of disability, health, and nutrition, and has co-authored two books, Health Matters: The Exercise and Nutrition Health Education Curriculum for People with Developmental Disabilities and Health Matters for People with Developmental Disabilities: Creating a Sustainable Health Promotion Program.
Yen-Ching Chang is an assistant professor in the Department of Occupational Therapy, at National Cheng Kung University. Her research interests include recovery of people with psychiatric disabilities, occupational therapy, and health promotion for people with disabilities.
Ryan Murphy, MPH, is a statistician in the Trauma Quality Improvement Program at the American College of Surgeons. His primary professional interests include the aggregation and analysis of health data to improve quality of care—especially in under-served populations, as well as the promotion of preventative health initiatives.