
Abstract
Background: Employee engagement, exemplified by positive perceptions of supervisors, workplace, and job, improves productivity and employee retention. We identified the extent of and barriers to employee engagement at Centers for Disease Control and Prevention’s (CDC) National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention (NCHHSTP). Methods: In 2015, NCHHSTP’s leadership collected baseline data through a centerwide Employee Engagement Pulse Survey (EEPS) from NCHHSTP’s full-time Civil Service employees, U.S. Public Health Service Commissioned Corps officers, and Title 42 service fellows. EEPS included six demographic questions; nine Likert-type scale questions measuring 26 perceptions related to immediate supervisors, the work environment, and job satisfaction; and four open-ended questions soliciting recommendations for improvement. Findings: Among 727 of 1,171 staff (response rate = 62%), positive perceptions of supervisors ranged from a high of 94% (supervisor conducts performance reviews) to a low of 63% (supervisor assists employees with career development). Perceptions of work experience ranged from 98% (respondents were willing to put in extra effort to get a job done) to 68% (respondents’ talents were used well in the workplace). Perceptions of job satisfaction ranged from 87% (support from their coworkers) to 69% (satisfaction with opportunities to learn or grow professionally). Conclusion/Application to Practice: Overall, NCHHSTP staff have positive perceptions of their work, their leaders, and the agency. Other public- and private-sector employers might be able to improve their employees’ engagement and retention by listening to their opinions and needs and frequently recognizing their individual achievements. NCHHSTP’s workforce development initiatives can be used as a model for assessing a baseline of their employees’ engagement.
Keywords
Background
Among both public- and private-sector employers, employee engagement is a principal factor in productivity, job satisfaction, higher employee retention, and lower absenteeism. Highly engaged employees are motivated to do their best, place organizational interests above their own, are innovative, and contribute to a collegial work environment (Marrelli, 2011); they often are the top contributors to their organization’s performance (Trahant, 2009).
In contrast, disengaged employees become focused on tasks rather than outcomes, do not have productive relationships with their managers or coworkers (Fernandez, 2007), have low or no vitality at work, resist change, and usually have a negative outlook (Marrelli, 2011). Disengagement results in high turnover, which costs time and resources spent in hiring replacements, slows productivity while new employees learn on the job, and causes loss of institutional memory (Fernandez, 2007; Fragoso et al., 2016; Liss-Levinson et al., 2015). The scientific literature has focused on job satisfaction as a key factor in employee turnover by examining demographic and economic variables (Liss-Levinson et al., 2015), but job satisfaction (i.e., liking the job but not necessarily feeling committed to the organization) is only one determinant in employee engagement (Fernandez, 2007; Fragoso et al., 2016).
Throughout 2010 to 2015, the Centers for Disease Control and Prevention’s (CDC) National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention (NCHHSTP) Employee Engagement Index score from the U.S. Office of Personnel Management’s (OPM) Federal Employee Viewpoint Survey remained at 69% to 70%. OPM’s Employee Engagement Index comprises three subfactors: Leaders Lead, Supervisors, and Intrinsic Work Experience (U.S. OPM, n.d.). The Leaders Lead subfactor reflects employees’ perceptions of the integrity of leadership and leadership behaviors (e.g., communication and workforce motivation); the Supervisors subfactor reflects the interpersonal relationship between worker and supervisor, including trust, respect, and support; and the Intrinsic Work Experience subfactor reflects the employee’s feelings of motivation and competency relating to his or her role in the workplace (U.S. OPM, n.d.). Although consistent with scores from across CDC for the Leaders Lead subfactor, NCHHSTP’s scores had been consistently lower than for the Supervisors and Intrinsic Work Experience subfactors. To explore reasons for the lower score, in 2015, NCHHSTP leadership collected baseline information through a centerwide Employee Engagement Pulse Survey (EEPS).
The term employee engagement in the context of EEPS refers to the employees’ sense of purpose on the job, as evidenced by their expression of dedication, persistence, effort, and overall attachment to the organization and its mission and vision (Liss-Levinson, et al., 2015; Myler, 2013; Sorenson, 2013). Employers who are unaware of their employees’ level of engagement can survey their staff to determine their level of satisfaction with their supervisors and management, their day-to-day work experience, and the overall work environment, similar to the EEPS conducted by NCHHSTP.
For this project, we explored the quantitative and qualitative findings from the EEPS, presented employees’ recommendations for improvements, and provided examples of NCHHSTP workforce development initiatives used to ensure employee engagement and retention. These initiatives were designed to improve employees’ work experiences, opportunities for professional growth, vitality at work, and productivity. Moreover, the initiatives support national goals for improving federal employee performance for the 21st century workforce (Pon et al., 2018) and serve as examples for other public and private employers who wish to retain high-performing, engaged staff.
Methods
EEPS was administered electronically through SurveyMonkey® (Palo Alto, California) and offered to all full-time-equivalent NCHHSTP staff onboard as of April 2015, including Civil Service employees, U.S. Public Health Service Commissioned Corps officers, and Title 42 service fellows. All survey responses were anonymous (i.e., respondents’ answers were not linked to information in any other data collection system that identifies individual persons).
The survey comprised 19 questions, divided into three parts: background demographic information (six closed-ended questions); employment experience, including attitudes and opinions about the respondent’s experience in NCHHSTP (three Likert-type scale questions with multiple parts, plus six closed-ended questions); and the respondent’s recommendations about ways NCHHSTP could improve its work environment (four open-ended, free-text questions).
Three Likert-type scale questions (Questions 7–9) were used to measure employees’ reactions to statements in 26 specific areas measuring perceptions of their immediate supervisor, their work experience, and job satisfaction. Respondents answering Questions 7 and 8 could select Strongly disagree, Disagree, Agree, Strongly agree, or I prefer not to answer. Question 9 responses included Very dissatisfied, Dissatisfied, Satisfied, Very satisfied, and I prefer not to answer. To facilitate analysis, the four response options for Questions 7 and 8 were combined into two options, Agree or Disagree. For Question 9, the four response options were combined into Dissatisfied or Satisfied.
For the open-ended, free-text responses, a qualitative data analysis was conducted by using the QSR NVivo 11 (QSR International Pty Ltd., Doncaster, Victoria, Australia) software program. A thematic analysis was applied to identify and describe explicit ideas or themes. A structural codebook was developed based on survey questions and linked to identified themes. The analyst read each comment and assigned a code from the codebook (Guest et al., 2012). A descriptive analysis was then performed for all survey responses to determine the frequency distribution for each variable (survey available in the Supplemental Information). Ethics officials not involved in the work determined the survey to be public health practice that did not require approval by a CDC Institutional Review Board.
Findings
Of 1,171 NCHHSTP staff eligible to participate in the electronic EEPS, 771 (66%) accessed the survey. Of those, 44 did not complete one or more questions and were removed from the analysis, for a final response rate of 62% (727/1171).
Demographic Results
EEPS respondents varied by age group, General Schedule (GS) pay grade level, job series, years of NCHHSTP service, and physical location. Of 683 respondents providing their age group, 245 (35.9%) were in the 46 to 55 year age group, followed by 215 (31.5%) in the 34 to 45 year age group.
By grade category, among 675 respondents, 419 (62%) were in Grades 13 to 15. Of 663 respondents, the highest percentages indicated their job series as GS-0685, Public Health Program Specialist (n = 202; 30.5%) or GS-0601, General Health Science (n = 146; 22%). Other identified series included GS-0602, Medical Officer (n = 59; 8.9%); GS-0101, Social Science (n = 44; 6.6%); and GS-0403, Microbiology (n = 42; 6.3%). Fourteen other series were combined into one category, All other (n = 172; 26%), for statistical analysis because of limited numbers of employees in each series. Commissioned Corps officers could select the job series that most closely matched their billet (Table 1).
Summary of Demographic Characteristics of the NCHHSTP Workforce and the NCHHSTP Employee Engagement Pulse Survey Respondents, a by Percentage.
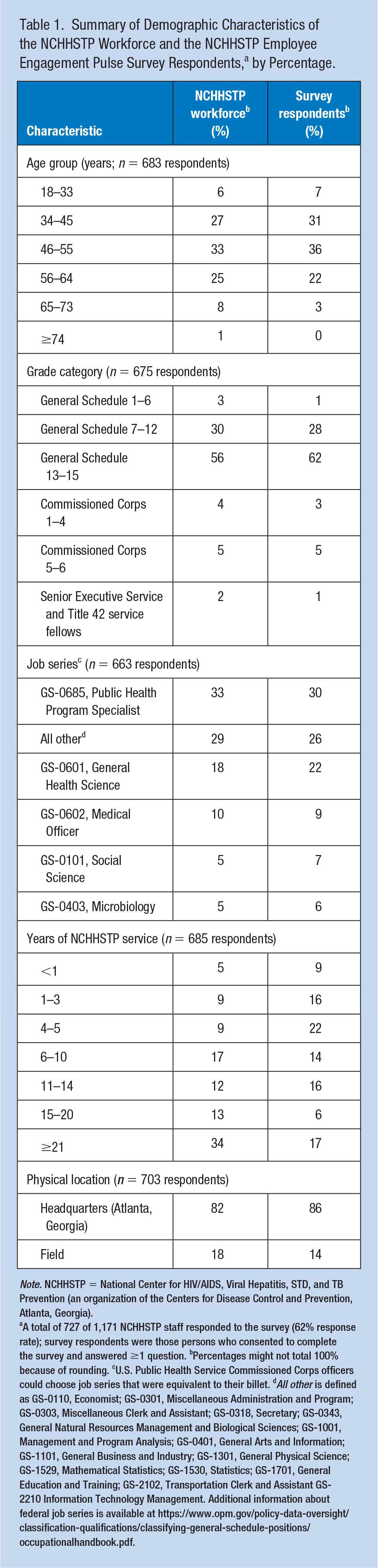
Note. NCHHSTP = National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention (an organization of the Centers for Disease Control and Prevention, Atlanta, Georgia).
A total of 727 of 1,171 NCHHSTP staff responded to the survey (62% response rate); survey respondents were those persons who consented to complete the survey and answered ≥1 question. bPercentages might not total 100% because of rounding. cU.S. Public Health Service Commissioned Corps officers could choose job series that were equivalent to their billet. dAll other is defined as GS-0110, Economist; GS-0301, Miscellaneous Administration and Program; GS-0303, Miscellaneous Clerk and Assistant; GS-0318, Secretary; GS-0343, General Natural Resources Management and Biological Sciences; GS-1001, Management and Program Analysis; GS-0401, General Arts and Information; GS-1101, General Business and Industry; GS-1301, General Physical Science; GS-1529, Mathematical Statistics; GS-1530, Statistics; GS-1701, General Education and Training; GS-2102, Transportation Clerk and Assistant GS-2210 Information Technology Management. Additional information about federal job series is available at https://www.opm.gov/policy-data-oversight/classification-qualifications/classifying-general-schedule-positions/occupationalhandbook.pdf.
The highest percentage of the 685 respondents had been with NCHHSTP for 4 to 5 years (n = 149 respondents; 21.8%), followed by ≥21 years (n = 117; 17.1%), 11 to 14 years (n = 109; 15.9%), and 1 to 3 years (n = 107; 15.6%). The lowest percentages were for employees who had been with NCHHSTP for 6 to 10 years (n = 98; 14.3%), followed by 15 to 20 years (n = 40; 5.8%). Eighty-six percent (n = 605) of 703 respondents reported working at CDC’s headquarters in Atlanta, Georgia; the other 14% (n = 98) were field staff (i.e., stationed in a state or local health department).
Quantitative Results
The EEPS quantitative results were divided into three broad categories for analysis: perception of supervisor, perception of work experience, and job satisfaction.
Perception of Supervisor
Ninety-four percent (n = 625) of 665 respondents indicated that their immediate supervisor conducted midyear and annual performance reviews, treated them with respect (n = 601/675; 89%), supported a work–life balance (n = 602/676; 89%), listened to what they had to say (n = 599/673; 87%), cared about them as people (n = 563/655; 86%), and was trustworthy (n = 549/646; 85%). Seventy-seven percent (n = 517/671) reported that their immediate supervisor delivered meaningful feedback on their performance, provided them with opportunities to demonstrate leadership skills (n = 520/675), and effectively delegated work (n = 517/671). Sixty-six percent (n = 440/666) agreed that their immediate supervisor devoted sufficient time to coaching and development, and 63% (n = 417/662) agreed that their supervisor worked with them to develop an Individual Development Plan (i.e., an outline of training needs for achieving career goals).
Perception of Work Experience
Overall, 98% (n = 689/703) indicated that, when needed, they were willing to put in the extra effort to get a job done. Ninety-three percent (n = 654/703) reported both knowing how their work related to the agency’s goals and priorities and believing that their job was important to NCHHSTP’s mission and vision (n = 656/705). Respondents also indicated knowing what was expected of them on the job 88% (n = 620/704). Eighty-three percent (n = 581/700) agreed that their work gave them a feeling of personal accomplishment; 80% (n = 558/697) felt challenged in their job; and 77% (n = 530/688) stated that their job or position supported their career goal. Seventy-one percent (n = 497/699) believed that they had the necessary resources to complete their work successfully, and 68% (n = 474/697) believed that their talents were used well in the workplace.
Job Satisfaction
Respondents reported being satisfied with support from their coworkers (n = 576/662; 87%), opportunities for workplace flexibility (e.g., telework and flexible work schedules; n = 569/669; 85%), and support from their immediate supervisor (n = 535/661; 81%). A slightly lower percentage (n = 500/658; 76%) reported satisfaction with the overall NCHHSTP work environment, and 73% (n = 485/664) felt recognized for their accomplishments. Only 69% (n = 460/667) reported satisfaction with opportunities to learn or grow professionally at work.
Qualitative Results
Respondents also provided open-ended, free-text opinions, and recommendations in the survey relating to what additional support and resources they needed for conducting their work, what recommendations they had for improving the center as a best place to work at CDC, and what other questions they would have liked to have been asked. Three principal themes emerged from those responses:
Theme 1: Support for Career Development and Training Needs. respondents were most interested in having more support for participating in detail assignments (i.e., temporary assignments in other program offices intended to lead to job growth), mentoring and professional certification programs, and coaching and guidance in obtaining job promotions. They cited needing financial support for online and classroom college courses, national conferences related to their expertise, and professional training related to their specific job series. Supervisory approval and time away from regular duties were also mentioned as being needed for participating in career development activities. Staff working in the four laboratory branches requested more support for meeting their unique career development needs (e.g., tailored career ladders or transitioning into managerial positions). Similarly, field staff were interested in cross-training at a headquarters location to increase skills related to their individual interests. Improved guidance and policies from CDC and NCHHSTP leadership were cited as being necessary for eliminating barriers to career development opportunities.
Theme 2: Improving NCHHSTP as an Overall Best Place To Work. respondents noted fearing negative responses or retaliation from leaders when expressing new ideas about the organization’s mission and goals or when requesting information about priorities and strategic directions. They also wanted center-level leadership to be more proactive in supporting lower level staff and to be more transparent in decision-making. One respondent noted that leadership engagement directly correlates with employee engagement. Other staff expressed a desire for more two-way communication between leadership and staff, recognition of quality performance and swifter action for inadequate performance, intolerance of disparate treatment of staff by leaders, and exit interviews to determine ways to improve morale. Lack of an employee gym or dedicated walking trails, a desire for more telework or flexible schedules in support of a work–life balance, and better technology to support teleworking and virtual meetings were common responses. Respondents also requested more collaboration with partner organizations to increase interchanges of ideas and bridge-building with the public health community at large. Filling vacated positions to facilitate fairer work distribution improved administrative services at the team and branch levels, and software programs and electronic systems that were more user-friendly (e.g., less redundant, cumbersome, and time-consuming) also were mentioned.
Theme 3: Questions That Should Have Been Asked. respondents believed that more questions should have been included on the survey about whether their leaders actively strived to improve the work environment, were open and innovative, and contributed to the organization’s success. They also wanted to be asked if senior leaders contributed to a less-than-favorable environment and low morale and if their leaders provided clear guidance about strategic priorities and expected deliverables. They wanted to be able to express opinions about work–life balance programs and what obstacles prevented employees from feeling engaged in their immediate organization (i.e., team, branch, or division), NCHHSTP, and CDC as a whole. Field staff again expressed interests related to organizational culture and their specific work environment.
Discussion
Overall, NCHHSTP’s employees were engaged in their work, the center, and the agency. OPM considers an approval rating for responses in the Federal Employee Viewpoint Survey of ≥65% to be a strength and ratings of ≤35% to represent challenges or barriers to success (U.S. OPM, n.d.). Notably, the NCHHSTP EEPS approval ratings for the majority of questions were ≥65%, and ratings of ≤64% were rare.
In EEPS, the highest ratings for supervisors were related to the immediate supervisor conducting midyear and annual performance reviews, which might be a reflection that these activities were mandatory; however, they also gave their immediate supervisor high ratings for management and personal skills, trustworthiness, and support. Such levels of respect and trust of leaders typically generate higher levels of motivation and commitment among employees (Marrelli, 2011).
Almost all respondents indicated that, when needed, they were willing to put in the extra effort to get a project done, which strongly correlated with CDC’s mission of saving lives and protecting populations from health threats, especially during exigent situations. High percentages of respondents reported that they knew the expectations of their job; they felt challenged, accomplished, and supported in their career goals; and they successfully completed their work. These positive responses reflected recommendations for engaging employees (Fernandez, 2007; Liss-Levinson et al., 2015; Myler, 2013; Trahant, 2009) and were in keeping with national goals and strategic priorities for the 21st century workforce (Pon et al., 2018).
Respondents across all job series and grade levels cited wanting more recognition for doing quality work, an attribute that is strongly correlated with engagement, vitality, and retention (Marrelli, 2011; Prince & Mihalicz, 2019). Receiving recognition from peers as well as leaders increased an employee’s feelings of dignity and respect, regardless if it was received in person, during a performance evaluation, or by e-mail (Landry et al., 2018).
Frequent survey responses involved having opportunities to learn or grow professionally, including being allowed to participate in such programs as CDC University’s formal mentoring program or NCHHSTP’s Speed Mentoring and Employee Shadowing programs. These desired improvements correlated with Trahant’s (2009) recommendation that managers energize their employees by using career development and enrichment discussions as an engagement tool and team-building strategy. Fernandez (2007) reports that the most important factor for employee engagement is leadership’s “interest in the employee’s well-being” (p. 525). Employees being satisfied with their position or knowing that their work might lead to a better position in the future has a direct correlation with their well-being (Fernandez, 2007; Wieneke et al., 2019). Responses from NCHHSTP’s EEPS reflected the importance the organization’s employees placed on learning and career development opportunities and their regard for the work environment, including opportunities for physical activity during the workday. Longevity with an organization also factored into satisfaction and well-being. With 40% of EEPS respondents reporting having been with the center only 1 to 10 years, NCHHSTP recognized the need for meeting employees’ expectations for career development and job growth to improve employee retention within the center, at the agency, and in public health practice.
Workforce Initiatives for Addressing Employees’ Expressed Needs
NCHHSTP has long promoted employee engagement through its workforce development and capacity-building programs (Dean et al., 2014). For example, NCHHSTP’s Coaching and Leadership Initiative (CaLI) worked to improve midlevel leader effectiveness, a key area for predicting employee engagement and retention (Prince & Mihalicz, 2019). Midlevel leaders participated in a 15- to 18-month process; completed a 360-degree leadership assessment; and were evaluated by their supervisor, staff, peers, and colleagues; they also completed six leadership coaching sessions and an in-depth interview. Since its inception in 2012, a total of 94 NCHHSTP midlevel leaders have completed the CaLI program (Dean et al., 2019).
Fernandez (2007) states that leaders should provide “good supervision, effective performance management and communication, and clarity about how employees contribute to results” (p. 526). Although these attributes were reflected in the high scores and respondents’ comments in the EEPS, NCHHSTP has since launched other activities designed to improve employee engagement and increase morale even further. For example, new staff were invited to have lunch with the center director in a small-group (≤10), casual setting. New employees brought their own lunch and frankly and openly discussed topics, such as the organizational culture and mission, new employee concerns, and recommendations for improvement, with the director.
In another effort, NCHHSTP encouraged its employees to stay healthy and active by taking the stairs instead of elevators. To make this form of exercise more attractive, the center decorated the stairwells throughout the campus with interesting and inspiring photographs taken by staff during their business or personal travel. An employee gym was also installed and includes a walking workstation (i.e., a treadmill with an attached network-connected computer) and other exercise equipment so that employees have a much-desired opportunity for exercise before, during, or after work.
NCHHSTP also enhanced employee communication. For example, each month, all employees received the Deputy Director’s Update, an electronic newsletter promoting and encouraging career-development opportunities and work–life balance activities. After the EEPS, the Deputy Director’s Update launched monthly recognition tips to encourage staff to frequently acknowledge their colleagues’ contributions in both small and substantial ways (e.g., from hand-written notes to employee recognition awards). Also included each month was an article voluntarily contributed by an employee sharing his or her recommendations for improving one’s physical health or emotional well-being.
To aid employees in improving their job skills and opportunities for advancement, NCHHSTP offered a monthly Learn@Lunch Career Development Series session. Staff throughout CDC were invited to attend, in person or through live, interactive broadcasts; these hour-long sessions focused on improving career-related skills. The sessions were conducted by subject matter experts from within or outside CDC who presented on such topics as effectively applying and interviewing for a new position, networking for success, proactive approaches to career advancement, and career paths for nonscientists. Participants were invited to complete an evaluation after the session, and data from the evaluations were used to improve future sessions.
To further improve employee satisfaction after the 2015 EEPS, NCHHSTP staff conducted data-driven reviews for monitoring employee engagement, satisfaction, recognition for achievements, and support for diversity in all organizational units. Tangible strategies gauged whether each indicator’s target goal had been achieved or exceeded. Results from these reviews and follow-up surveys to the Federal Employee Viewpoint Survey were routinely communicated with all NCHHSTP staff through, for example, senior staff briefings, all-hands meetings, staff newsletters, and electronic bulletin boards (i.e., large television screens located in common areas that display announcements about upcoming training opportunities, meetings, and employee awards and accomplishments).
Through these and other workforce development efforts, NCHHSTP’s leadership continued to implement activities previously rated highly (the Leaders Lead subfactor) and to initiate activities for increasing satisfaction in areas with slightly lower scores (the Supervisors and Intrinsic Work Experience subfactors). By implementing programs designed to improve career development opportunities, supervisory practices, performance management, communication from leaders, and recognition of employee contributions, NCHHSTP has improved its employee engagement. This can be observed in OPM’s latest Federal Employee Viewpoint Survey results for NCHHSTP, which revealed an increase from 60% in 2015 to 65% in 2018 in employees’ perception of recognition for high-quality work.
Limitations
This study was based on responses from employees in one national center within one federal agency; therefore, the responses might not reflect those of employees in CDC’s other centers, institute, or offices or of other federal or private-sector employees. As with other self-reported data, responses might reflect social desirability or be subject to recall bias. To assuage possible employee concerns regarding their responses being confidential, the survey invitation and all reminders to take the survey explained that it was not linked to any personally identifiable employee information and that the results would be used to improve the overall work environment.
Conclusion
With approximately 25% of the public health workforce planning to retire in 2020 (Harper et al., 2018), employee engagement and retention is particularly vital for CDC. NCHHSTP’s EEPS can serve as a model for both public- and private-sector employers who want to improve their employees’ engagement, vitality, and retention. By listening to their employees’ opinions and expressions of need, employers can assess their employees’ engagement and intention to stay with the organization. By using the survey results, employers can tailor workforce development initiatives that address and improve employees’ work experiences, opportunities for professional growth, and productivity, thus improving employees’ engagement, satisfaction, attendance, and retention.
Application to Professional Practice
For any employer, employee engagement is a principal factor in productivity, job satisfaction, higher employee retention, and lower absenteeism. Highly engaged employees are motivated, place organizational interests above their own, are innovative, and are usually the top contributors to their organization’s performance. Employers might be unaware of the level of their employees’ engagement or, in contrast, their dissatisfaction and intention to leave the organization. Employee turnover costs the employer time and resources spent in hiring replacements, slows productivity, and causes loss of institutional memory. Employers can conduct an employee engagement pulse survey to measure their staff’s satisfaction with their immediate supervisors, the organization’s management, the day-to-day work experience, and the overall work environment. By using the survey results, employers can tailor workforce development initiatives that address and improve employees’ work experiences, opportunities for professional growth, and productivity, thus improving employees’ engagement, satisfaction, attendance, and retention.
Supplemental Material
Employee_Engagement-Supplemental_Content-Workplace_Hlth_and_Safety – Supplemental material for Supporting Public Health Employee Engagement and Retention: One U.S. National Center’s Analysis and Approach
Supplemental material, Employee_Engagement-Supplemental_Content-Workplace_Hlth_and_Safety for Supporting Public Health Employee Engagement and Retention: One U.S. National Center’s Analysis and Approach by C. Kay Smith, Crystal Spears-Jones, Carolyn Acker and Hazel D. Dean in Workplace Health & Safety
Footnotes
Acknowledgements
The authors gratefully acknowledge Beza E. Ayalew, a fellow of the Oak Ridge Institute for Science and Education, for her work during the development of the survey instrument.
Authors’ Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Author Contributions
Conceptualization was done by C.S.-J. and H.D.D.; data curation was done by C.S.-J. and C.A.; formal analysis was done by C.S.-J. and C.A.; investigation was done by C.S.-J., C.A., and H.D.D.; methodology was done by C.S.-J. and H.D.D.; project administration was done by H.D.D.; supervision was done by H.D.D.; writing—original draft was done by C.K.S.; and writing—review and editing was done by C.K.S., C.S.-J., C.A., and H.D.D.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
C. Kay Smith, MEd, is the Senior Technical Writer–Editor in the Office of the Associate Director for Science, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention, Centers for Disease Control and Prevention (CDC). She has been with CDC for 23 years and previously served for 6 years as an Environmental Protection Specialist with the Indian Health Service.
Crystal Spears-Jones, MPA, manages Workforce Development and Capacity Building initiatives at the Centers for Disease Control and Prevention’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. Crystal leads the Coaching and Leadership Initiative (CaLI)—a systematic development initiative to sustain effective leadership, management, and administration skills of government supervisors. She is the recipient of several awards and her work has been recognized as one of the Best Workforce Development Programs in government.
Carolyn Acker is with Emory University where she works on multisite evaluations, providing technical assistance to community-based organizations. Her interest in workforce development began when she provided technical assistance to clients at Advantage Consulting, LLC. This interest grew during her ORISE fellowship with NCHHSTP, where she implemented and evaluated workforce development programs. She has also implemented mentoring programs for the American Evaluation Association’s Graduate Students and New Evaluators TIG and the Atlanta-area Evaluation Association.
Hazel D. Dean, ScD, MPH, at the time this study was performed, was deputy director of CDC’s National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. She is currently the editor-in-chief of Public Health Reports, which is located in CDC’s Center for Epidemiology, Surveillance, and Laboratory Services. She has authored >130 scientific journal articles, policy reports, and other publications about infectious and chronic diseases, public health surveillance, applied epidemiologic methods, social and structural determinants of health, and public health workforce development.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.