
Abstract
The purpose of this study was to identify factors influencing hospital nurses’ dietary practices during their shifts. Semistructured interviews grounded in the Social Ecological Model focused on individual, interpersonal, organizational, and public policy factors affecting intake. Responses from 20 female nurses were qualitatively coded and categorized based on common themes. Four major themes emerged: occupational characteristics, hesitation to take breaks, influence of unhealthy food, and organizational and industry policies. Of note, nurses’ perceived inability to take breaks was due to patient load, unpredictability of patient needs, reluctance to burden other nurses, a tendency to prioritize patient care over self-care, and the repercussions of working longer hours to complete work. Other influential factors included the presence of unhealthy food options, regulations restricting nurses’ ability to eat and drink in the workplace, and the need for more staff. Multilevel interventions are necessary to ensure nurses take appropriate meal breaks and maintain satisfactory dietary habits.
Keywords
Nursing is the largest health care profession in the United States (Department of Professional Employees AFL-CIO, 2014). Over 3 million registered nurses are licensed nationwide (Health Resources and Services Administration [HRSA], 2010), more than 4 times the number of physicians (American Association of Colleges of Nursing, 2016). Nurses comprise 62.2% of health care staff in hospital settings (2008 National Sample Survey of Registered Nurses; HRSA, 2010), and national forecasts estimate that the industry will need to add more nursing jobs over the next decade due to an aging population, health care advancements, and increased access to health insurance (U.S. Bureau of Labor Statistics, 2015; Chan, Tam, Lung, Wong, & Chau, 2012).
Given the nature of their profession, nurses should be viewed by the public as healthy role models (Blake & Harrison, 2013; Kemppainen, Tossavainen, & Turunen, 2013). However, nursing tasks take a toll on both work performance and physical health. For example, the likelihood of making a health care error during shifts of 12.5 hours or longer has been found to be 3 times the rate of errors made during an 8.5-hour shift (Rogers, Hwang, Scott, et al., 2004). In addition, studies have shown that nurses who work 12 or more hours per day are more likely to experience musculoskeletal disorders (J. A. Lipscomb, Trinkoff, Geiger-Brown, & Brady, 2002) and needle stick injuries (Trinkoff, Le, Geiger-Brown, & Lipscomb, 2007). Although studies have found that periodic breaks can enhance short-term performance and reduce fatigue and physical discomfort (Faucett, Meyers, Miles, Janowitz, & Fathallah, 2007; Galinsky, Swanson, Sauter, Hurrell, & Schleifer, 2000; Rogers, Hwang, & Scott, 2004; Tucker, Folkard, & Macdonald, 2003), more than one third of nurses rarely or never take meal breaks during their shifts (American Nursing Association, 2009). As a result, many nurses do not maintain a regular eating schedule (Nahm, Warren, Zhu, An, & Brown, 2012) and often rely on high-fat, sugary foods rather than consuming the recommended amounts of fruits and vegetables each day (Malik, Blake, & Batt, 2011). These practices are contrary to what is considered healthy.
The practice of healthy lifestyle habits benefits both nurses and their patients (Zapka, Lemon, Magner, & Hale, 2009). Yet, much of the existing research on hospital nurses is focused on patient safety (Hughes, 2008; Lang, Hodge, Olson, Romano, & Kravitz, 2004; Stimpfel & Aiken, 2013), nursing workload and performance (Aiken, 2002; Hughes et al., 2008, Keijsers, Schaufeli, Le Blanc, Zwerts, & Miranda, 1995), and job satisfaction, nursing shortage, and staffing (Aiken, Clarke, & Sloane, 2002; Lang et al., 2004; Tam et al., 2013), with comparatively little on lifestyle and preventive health behaviors (Nahm et al., 2012; Zapka et al., 2009). The purpose of this study was to identify factors that affect the eating practices of hospital nurses during their shifts. Given that hospital nurses work in a dynamic and multidimensional environment, the Social Ecological Model (SEM) was used to provide a framework for describing the individual, interpersonal, organizational, and policy influences on nurses’ eating behaviors. With a better understanding, these influences can be used as leverage points for guiding health behavior interventions in future research and practice.
Method
To probe deeply into the factors influencing what, how, and when hospital nurses eat during their shifts, semistructured interviews were conducted with hospital nurses who work in New Jersey. Recruitment for study participants occurred through solicitations via email and telephone to local nurses and flyers to local nursing schools. To be eligible for this study, nurses were required to have been working for their current hospital employer for at least 1 year to ensure sufficient time to establish habits and form routines. Participants were restricted to women because the majority (90%) of nurses in New Jersey are female (Vaida, 2016). Participants were excluded if they did not work 12-hour shifts so that work hours would be constant, and because shifts of 12 to 13 hours are most common in hospitals (Witkoski-Stimpfel & Aiken, 2013). Recruitment continued until information saturation was reached. Because the last two interviews did not reveal new information, recruitment ended after interviewing 20 nurses. As for theoretical saturation, the SEM’s levels of influence can interact with each other in numerous permutations which in this study occurred enough to achieve theoretical saturation as well.
Interview Guide
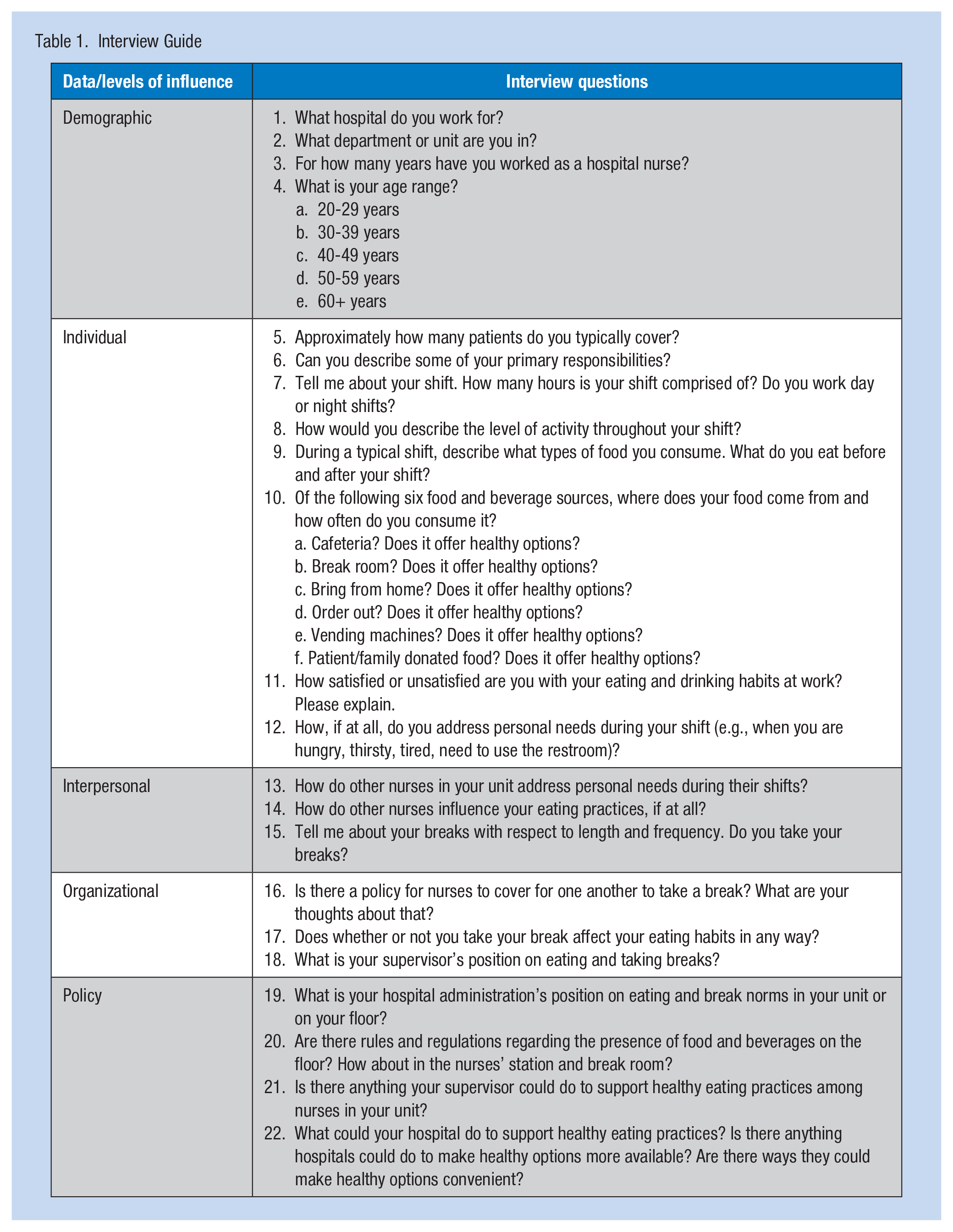
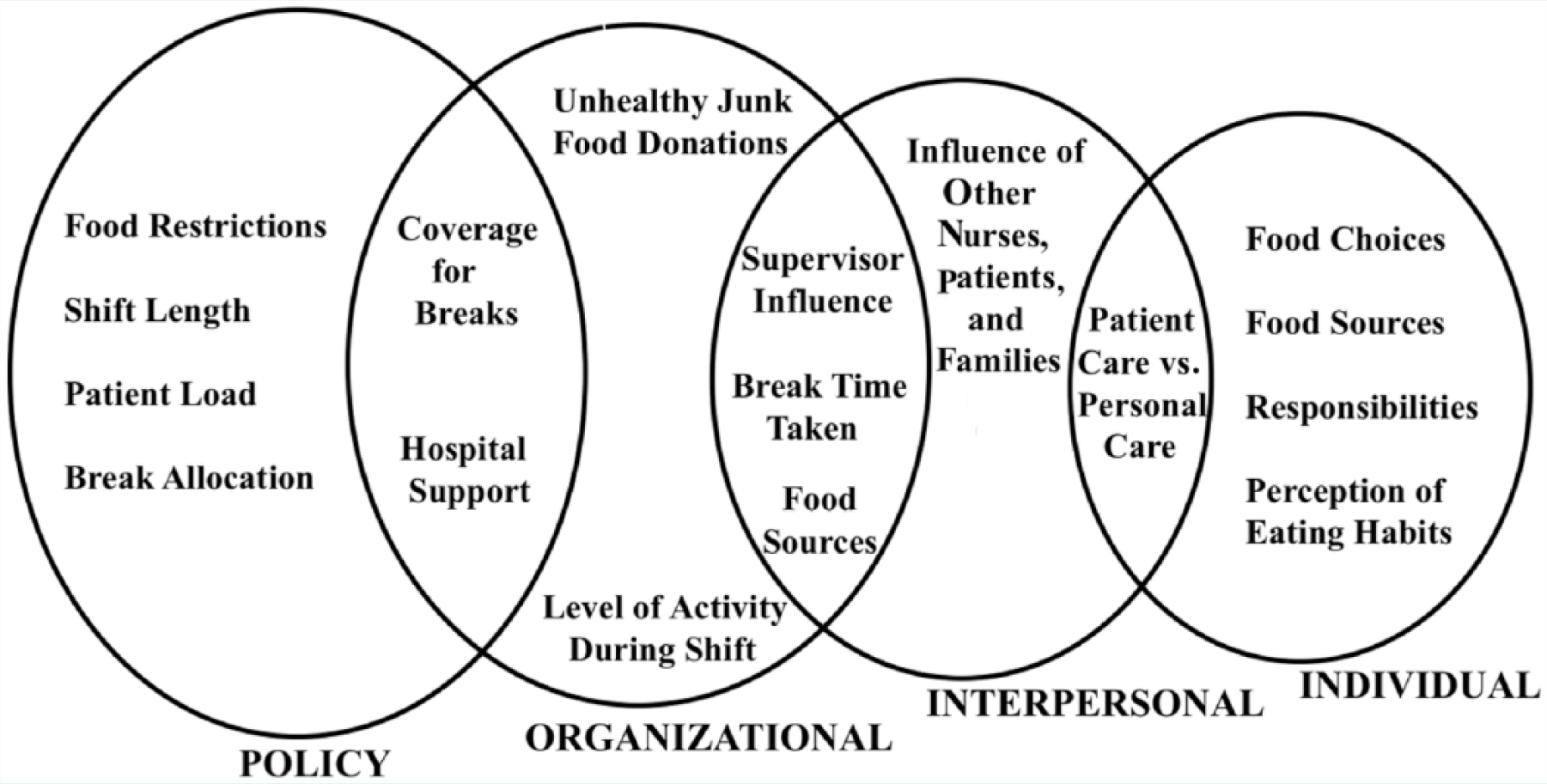
An interview guide of 22 semistructured questions (Table 1) was created to gather demographic information and probe participants about factors that influence their dietary habits at work. The interview questions were based on results from an unpublished pilot study of nurses’ eating habits. The pilot study had a smaller sample size (n = 8 vs. n = 20 for this study), yet it provided insight on how to structure the interview guide and research design. Interview guide questions were formulated using the SEM to evaluate factors within four levels of influence: individual, interpersonal, organizational, and policy (Figure 1). A core aspect of SEM is that the levels of influence interact with each other. Hence, some factors straddled two levels as illustrated in Figure 1. Because behaviors can be categorized in more than one level, understanding behavior change is more effective when considering multiple, interacting determinants of health behaviors (Glanz, Rimer, & Viswanath, 2008).
Interview Guide
Four levels of influence.
Data Collection
The primary researcher conducted all interviews either by telephone (80%), video call (5%), or in person at a local public library private study room (15%). All participants provided informed consent and agreed to be audio-recorded. Following each interview, the primary researcher transcribed the audio recording verbatim and then deleted the recording. To further ensure confidentiality, all transcriptions were identified by participant number. Nonverbal cues (e.g., laughter, pauses, and voice inflections) were detected over the telephone, captured on the audio-recordings, and noted on the transcripts. Interviews averaged 21 minutes, with a range of 11 to 40 minutes. As an incentive for participation, a gift bag containing healthy and convenient snacks and a food container was presented or sent in the mail (US$8 value). This study, Protocol Number 15-16-97, was approved by the Montclair State University Institutional Review Board prior to research commencement.
Data Analysis
Once completed, all interview transcripts were uploaded to ATLAS.ti, Version 1.0.45 (ATLAS.ti GmbH, Berlin, Germany), and coded by the primary researcher. A combination of phenomenological and grounded theory approaches was used in this study to develop the inquiry methods (Parahoo, 2014). Use of the phenomenological method began during the pilot study when hypotheses were in the formation stage and supported formulation of the interview guide. Responses from the 20 interviews were used to build a data set of themes. Grounded theory was applied when coding data to identify themes.
Through inductive data analysis, responses with conceptual similarity were uncovered and grouped under emergent themes. Codes were further sorted within each major theme to identify overlap and frequencies. Thematic analysis as a top-down approach was used at this stage to identify which of the remaining themes were major themes and subthemes (V. Clarke & Braun, 2013). To ensure reliability, a second researcher independently coded 25% of the interviews. A high degree of similarity between coding methods was found and any discrepancies were discussed and agreed upon. In addition, comments from a public online forum for nurses and nursing students around the country (http://www.allnurses.com) were consulted to provide triangulation of the research findings.
Results
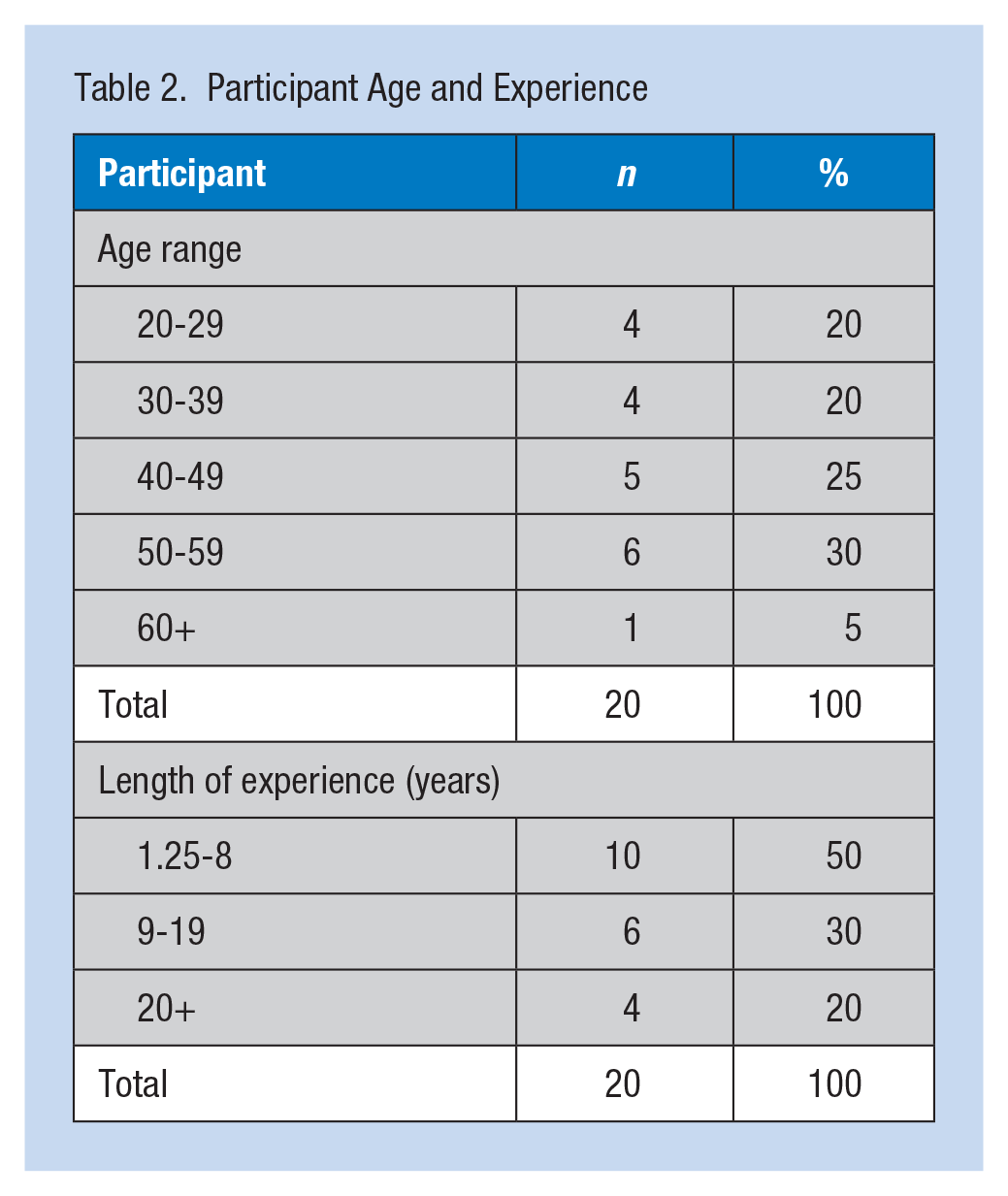
The average age range of the 20 participants was 40 to 49 years, and the average length of nursing experience was 10 years (range = 1.25-30 years). The range of shift length spanned from 12 to 15 hours, with an average length of 13 hours. Sixty percent of the participants were assigned to the day shift, 35% worked the night shift, and 5% rotated between night and day shifts. Because 90% of the nurses in New Jersey are female, variation in age and experience was calculated as illustrated in Table 2. Sampling via multiple recruitment outlets resulted in participants from a variety of public and private hospitals and medical centers as well as diverse patient care units across urban and suburban areas as illustrated in Table 3.
Participant Age and Experience
Hospital Demographics by County
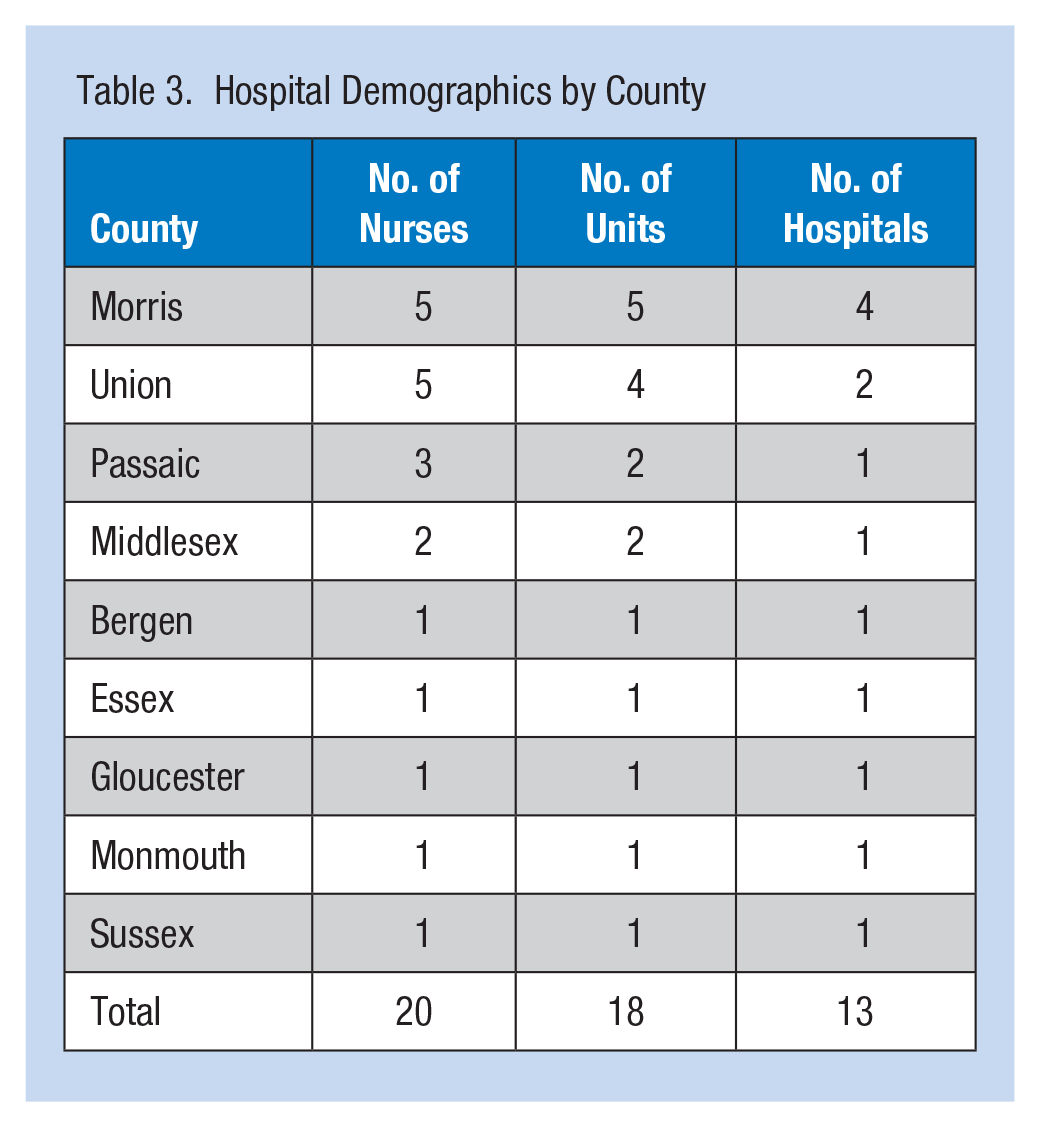
The 20 participants worked in 13 hospitals located in nine New Jersey counties, representing 11 hospital units, including Emergency, Medical-Surgical, Orthopedic Medical-Surgical, Psychiatry, Acute Inpatient Rehabilitation, Labor and Delivery, Maternity and Special Care, Cardiac Telemetry, Neonatal Intensive Care Unit (NICU), Cardio-Oncology, and Same Day Surgery. Sixty-nine percent of the hospitals were in suburban communities and 31% were in urban settings.
Factors Influencing Eating Practices
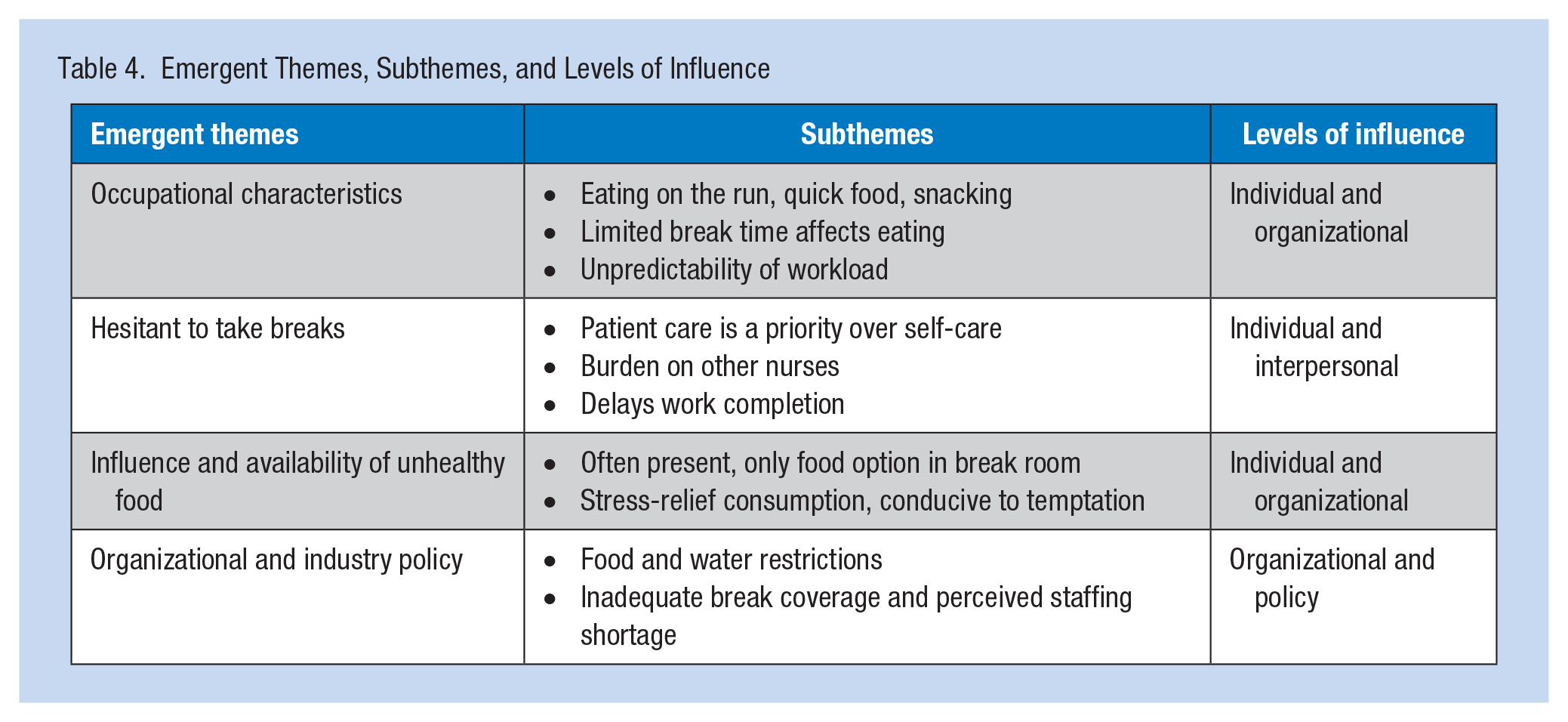
Table 4 highlights major themes and subthemes of main factors influencing the eating practices of hospital nurses during their shifts. These themes and subthemes are depicted at the SEM levels of individual, interpersonal, organizational, and public policy, and described in more detail below. Table 5 lists illustrative quotes that represent major findings from the study within the applicable SEM level of influence. However, as Figure 1 demonstrates, some of the themes that were initially categorized within a single SEM level could apply to multiple SEM levels of influence.
Emergent Themes, Subthemes, and Levels of Influence
Quoted Responses Based on SEM Level of Influence
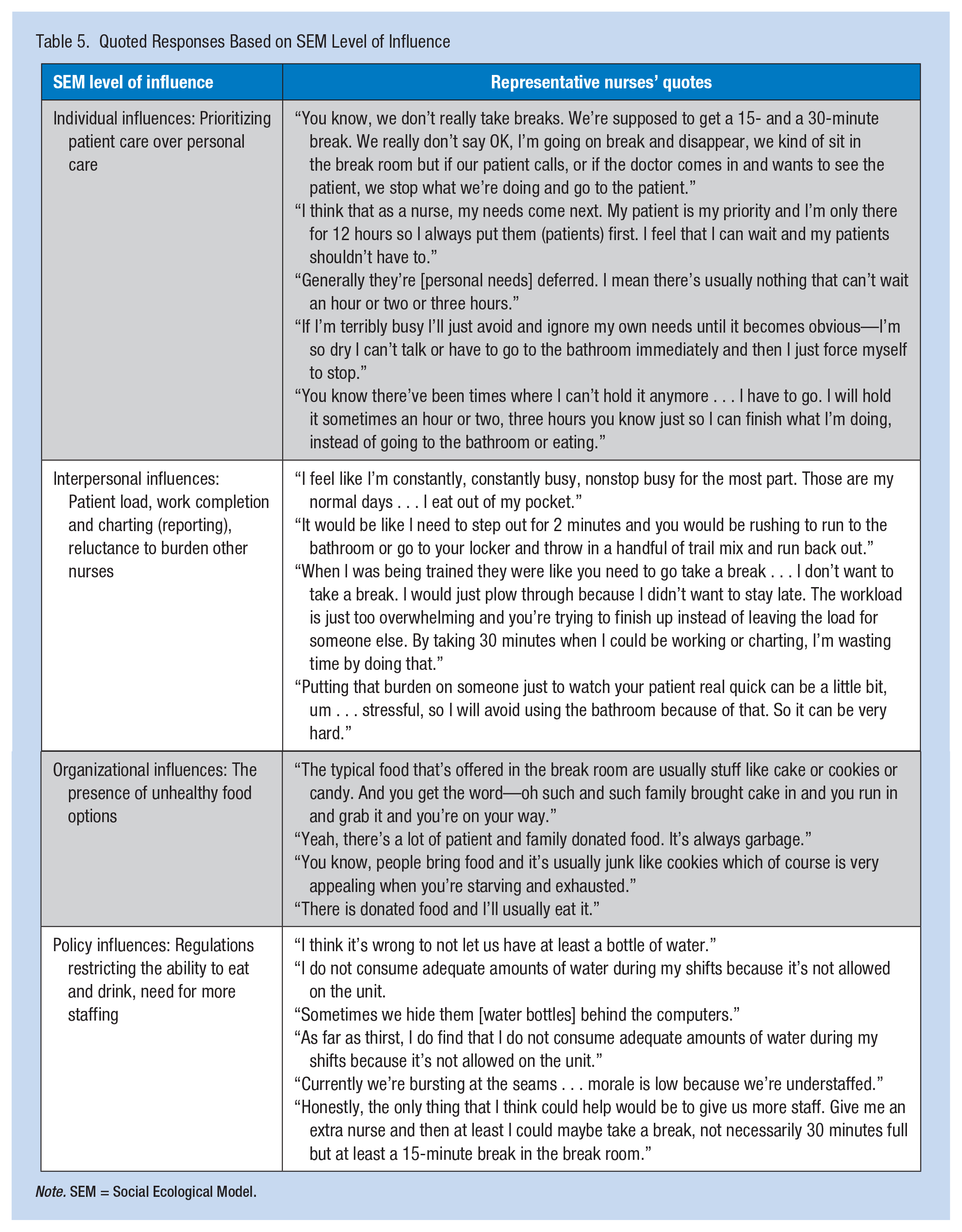
Note. SEM = Social Ecological Model.
Individual influences
Nurses were asked if they took breaks and could attend to personal needs like hunger, thirst, and using the restroom. All 20 nurses reported that they do not take their full breaks. Forty-five percent took approximately half of their allotted breaks, and 40% did not take their official breaks but took 5 minutes when there was an “open-window.” Fifteen percent took “some” of their allotted break time.
Sixty-five percent of the nurses indicated that the main reason they did not take breaks was prioritizing patient care over their personal needs. Consequently, “quick” foods and snacks were typical choices during work shifts. Five nurses used the terms “eat on-the-run” or “eat on-the-fly” when referring to norms regarding hunger and thirst. As one nurse explained, “I mean, eating is just done on the fly. You know, walk in, throw something in your mouth and chewing while you’re washing your hands and then walking to see another patient.”
When asked whether taking a break affected their eating habits, 85% of the respondents said yes; 75% attributed taking an allotted break to better eating habits. A cardiology nurse responded, “If I actually do take a break and sit down, then I’m more likely to eat something more substantial.” An orthopedic nurse shared that “If I don’t take a break, then I only eat once per day and it’s at dinner” (following 14 hours of work and commuting time).
Although not directly related to dietary habits, another unexpected yet common theme among 35% these nurses was a tendency to delay using the restroom. They refrained from drinking fluids to avoid the restroom. Two emergency room (ER) nurses reported that they routinely held off immediate needs for up to 3 hours or longer. Three nurses reported having “stretched” or distended bladders from delaying visits to the restroom and one reported numerous urinary tract infections (UTIs).
Interpersonal influences
Burdening other nurses as well as insufficient time to complete reports for physicians’ orders and prepare for shift change were the main interpersonal reasons nurses neglected breaks. An ER nurse summed up several of the major findings:
One nurse couldn’t take care of their five patients and then take care of another five patients so that someone could take a break. And that’s why no one does it, because you feel bad. I don’t want to put my five really sick patients on anyone else. It wouldn’t be safe. Then again, it’s not safe for nurses to work 12 hours and not eat and not drink.
The role of supervisory nurses appeared to be another interpersonal influence. Nearly all nurses perceived that their supervisors or managers were unable to provide break coverage due to supervisory responsibilities or patients of their own. Yet, 75% of respondents reported that management encouraged them to take breaks.
The nurses unanimously offered suggestions about how hospitals could provide more support. At the interpersonal level, two nurses who reported being satisfied with their eating habits described working closely with fellow nurses in the unit as a team and efficiently coordinated break times. Camaraderie was mentioned as playing a key role in break coordination. The coverage strategy of splitting a nurse’s patient assignment between two nurses to make the additional responsibility more manageable was also effective. Sufficient break time for rest and meals is an integral part of occupational health.
Hospitals could emphasize the value of break time as part of initial orientation and ongoing professional development for nurses. A buddy system approach to caring for patients (e.g., nurses care for one another’s patients for short periods) might be more acceptable to resistant nurses. One hospital in the study encouraged uninterrupted break time. Nurses were asked to respond to patient calls on behalf of the off-duty nurse for the full break duration.
Organizational influences
Seventy percent of nurses indicated that food donated by patients’ families was typically high in sugar and fat and readily available in the break room. These foods were reported as being “always there,” and often the only option. The influence of unhealthy foods such as cookies and brownies in the break room was described as a “go-to” food during stressful “bad shifts.” The most frequently mentioned donated foods were donuts, cookies, and cake.
A rehabilitation nurse cited why an ever-present supply of unhealthy food was a barrier to healthy eating practices:
Unfortunately, I do find myself subjected to the junk food that is brought in such as cookies, donuts. I know from my own self-reflection regarding my diet that when I’m hungry, tired, or stressed in that environment, or in pain for instance . . . because I worked 2 days in a row, I tend to go for, I’m more driven toward carbohydrates and sugar.
On the contrary, 85% of respondent nurses reported that their cafeterias offered healthy options, yet 60% said they did not eat in the cafeteria, primarily due to time constraints.
By adopting plans like Weight Watchers and Jenny Craig, three night shift nurses reported feeling significantly better physically and having more stamina. Night shift nurses especially struggled with what and when to eat during shifts with unconventional hours. Their work hours typically conflicted with their and their families’ eating habits on nonwork days. They reported that a disciplined program helped them identify regimented eating times and commit to nutrient dense foods. One of the nurses joined a weight management program that was promoted by the hospital for employees. Two of the nurses suggested that hospitals promote regimented diet and exercise programs to assist nurses in establishing and maintaining healthy dietary practices.
Two hospitals in the study promoted a biggest loser challenge initiative that was well received, regardless of whether weight loss was the goal. In both hospitals, nurses from both day and night shifts within a unit created teams and competed to lose the most combined weight. One hospital reportedly had a weigh-in day when healthy options dominated the cafeteria menu. Challenge contestants were awarded free healthy food that day each week. In another hospital, cafeteria staff brought a cart to each floor with nourishing snacks for the nursing staff once a week so that nutritious food was conveniently accessible.
Policy influences
All 20 nurses were aware of the policies restricting food at the nurses’ stations. They reported that food is not permitted at the nurses’ station, but four nurses (20%) were quick to add that water is permitted in three of the hospitals. Three nurses (15%) acknowledged concerns regarding food contamination at the nurses’ station. Four nurses (20%) cited distance to the break room as a barrier to eating, but the more significant issue was water restrictions. Night shift nurses explained that minimal staffing prevented them from taking meal breaks, and so an unofficial understanding that eating at their desks was consequently accommodated. When options were available (i.e., time, food choices, coverage) to hydrate and adequately consume nutrients, hospital nurses were apt to have the energy, focus, and stamina to provide better patient care and derive the personal benefit of long-term health as well.
Discussion
All 20 nurses reported that they did not take their full allotted break time. The major factors preventing them from taking breaks included attending to patient needs before their personal needs, a reluctance to burden other nurses, the availability of unhealthy foods versus less available healthier options, the inconvenience of accessing healthy food and water, inadequate staffing, and policies restricting foods and beverages on the hospital units.
Individual—Patient Care Over Personal Needs
Sixty-five percent of the nurses reported that patient needs were attended to before addressing their own needs, which were routinely delayed. Prioritizing patient care over their needs prevented nurses from taking breaks, leading to unsatisfactory eating habits. Several studies support this finding. A study in the United Kingdom revealed that nurses did not perceive their working environment as conducive to healthy eating due in large part to lack of breaks. Workload was a major detriment to breaks (Faugier, Lancaster, Pickles, & Dobson, 2001). Not only are nurses working longer hours, they are sacrificing break time to care for patients (Witkoski & Dickson, 2010).
Interpersonal—Resistance to Breaks Because of Additional Workload for Peers
Nurses were reluctant to take breaks and routinely failed to take allotted breaks in their entirety. Few U.S. research studies have focused on rest periods and meal breaks for hospital nurses (Witkoski & Dickson, 2010). According to an American Nursing Association Survey (2009), 35% of respondents reported rarely or never taking meal breaks. Forty percent of the nurses in this study reported taking 5-minute breaks or no breaks at all, despite working between 12 and 15 hours. A study that examined shift length as it pertains to safety and quality of care stated, “Many nurses do not regularly take breaks during the workday” (Witkoski-Stimpfel & Aiken, 2013, p. 127).
Organizational—The Influence of Unhealthy “Junk” Food and Staffing
The presence of unhealthy “junk” food was another adverse influence on the dietary habits of nurses in this study. Although research on nurses’ eating habits is limited (Zapka et al., 2009), hospital nurses reported regular consumption of foods high in sugar and fat (Cheung, 2003; Zapka et al., 2009). In a 2011 study of registered nurses’ lifestyle habits, 42.5% reported that they consumed high-fat and high-sugar foods daily (Malik et al., 2011). Patients’ families are known to bring unhealthy food donations to nurses in hospitals (Cheung, 2003). A similar environment exists in the United Kingdom. A recent National Health Service (NHS) initiative launched in England demonstrated the unwanted prevalence of unhealthy “junk” food in hospitals and the NHS quest to banish these foods from the workplace (Donnelly, 2015). Another reported barrier was a need for more staff. Fifty percent of study nurses responded that more staffing would provide adequate patient coverage during breaks and consequently improve eating habits.
Policy—Hospital Regulations That Prohibit Food and Water
All 20 nurses communicated a solid understanding of the food and water regulations in their hospital, yet four of the day shift nurses reported hiding water bottles in drawers or behind computers. Although the policy on water at the desk varied among hospitals, nurses generally preferred an accommodation for water.
Limitations
This qualitative study included a small sample of 20 women within the predominantly suburban areas of New Jersey, and thus, generalizability of the findings to other populations is limited. A quantitative study of a larger, broader sample of nurses could offer significant insight and account for differing state laws. The nurses interviewed were of one profession and therefore reflected a single perspective. Future study involving the viewpoints of other hospital professionals could determine whether perceived factors and corresponding levels of influence are valid and, if so, to what extent. Another limitation of this study was the possibility of social desirability bias during the interviews. The potential for social desirability was somewhat evident in reporting dietary intakes, but because this study did not involve nutritional content analysis, it did not affect the results. Although 90% of New Jersey nurses are female, the prospect of gender differences in eating practices is worth exploring.
Implications
Future Research
Further research on a broader population of nurses and hospitals could identify whether similar themes emerge. Specific questions about break-taking norms, workload, hospital support, variations among units, and differences between day and night shifts could be further explored. A study of how hospital administration oversees break time might explain the variation in break supervision among hospitals in this study. Clarification of food and water restrictions at nurses’ desks would be useful given the ambiguity of where those restrictions originated and the differential implementation of those restrictions.
Practice
Educating nurses on healthy eating practices is a means of staff support that could have positive outcomes. Addressing dietary habits and break times as part of nurses’ education and professional development could provide effective strategies to improving health. Structured eating programs were credited with improving dietary habits, especially among night shift nurses. Hospitals could engage nurses through direct nutrition programs within the hospital or by arranging discounts at local weight management and wellness programs.
A need for more staffing so that nurses could take sufficient break time was cited by half of the respondents. Nurses whose units furnished floater nurses mentioned that they were highly effective sources of break relief. In a recent arbitration decision filed by the Washington State Nurses Association (WSNA; 2016), Tacoma General Hospital was ordered to supply a float/relief registered nurse for the “precise assignment” of relieving nurses to take full uninterrupted breaks.
Policy
The issue of adequate staff to provide break time coverage straddles all four levels of influence: individual, interpersonal, organizational, and policy. The health care industry could enforce uninterrupted break time for nurses. Supervisors could oversee the practice of nurses covering for each other and ensure that breaks are taken. In some units, supervisors could possibly provide patient coverage themselves. From an individual perspective, perceptions of burdening other nurses and temporarily relinquishing patient care could be addressed through initial and continuing education.
More than half of the nurses reported they were encouraged and expected by management to take breaks, yet administration provided no support for this expectation. Providing nurses with opportunities for breaks is not a federal law. According to the U.S. Department of Labor, no federal laws require lunch or coffee breaks. New Jersey does not have laws to that effect either. Nevertheless, ensuring break time for nurses could mitigate negative nurse and patient outcomes. Several studies link long work hours to errors and occupational injuries (S. P. Clarke, 2007; H. J. Lipscomb, Epling, Pompeii, & Dement, 2007; Rogers, Hwang, & Scott, 2004; Trinkoff, Geiger-Brown, Brady, Lipscomb, & Muntaner, 2006).Trying to maintain a rigid schedule of breaks may not be realistic given the nature of hospital nursing, but reminders or direct coverage support where applicable could increase nurses’ likelihood of taking breaks. Furthermore, supervisors could benefit from professional development opportunities that provide strategies for organizing break structures, motivating nurses to use break time, and instigating a workplace culture shift.
In future hospital construction or renovations, a floor design that features a centralized break room and audible call bells rung by patients could enable healthier eating practices. One nurse described the proximity between the break room and patient rooms resulting in convenient access to water or fruit. Another nurse reported that call bells could be heard in the break room, enabling her to sit for what could be “as many as 20 minutes” until beckoned. The snack cart with fruit and water that one hospital delivered to each unit in the afternoon was very popular. To thwart the presence of unhealthy food, posting signs at nurses’ desks encouraging patients’ families to donate healthy rather than unhealthy food to nurses could be instrumental. However possible, healthy eating convenient for nurses during their shifts should be promoted.
Significant health outcomes (e.g., less stress and improved stamina) could result from occupational health training and supplemental break support. An intervention that encourages nurses to take meal breaks and maintain satisfactory dietary habits is recommended. Table 6 outlines a comprehensive program with action steps and leverage points mentioned above within the corresponding SEM levels of influence.
Intervention for Hospital Nurses’ Eating Practices
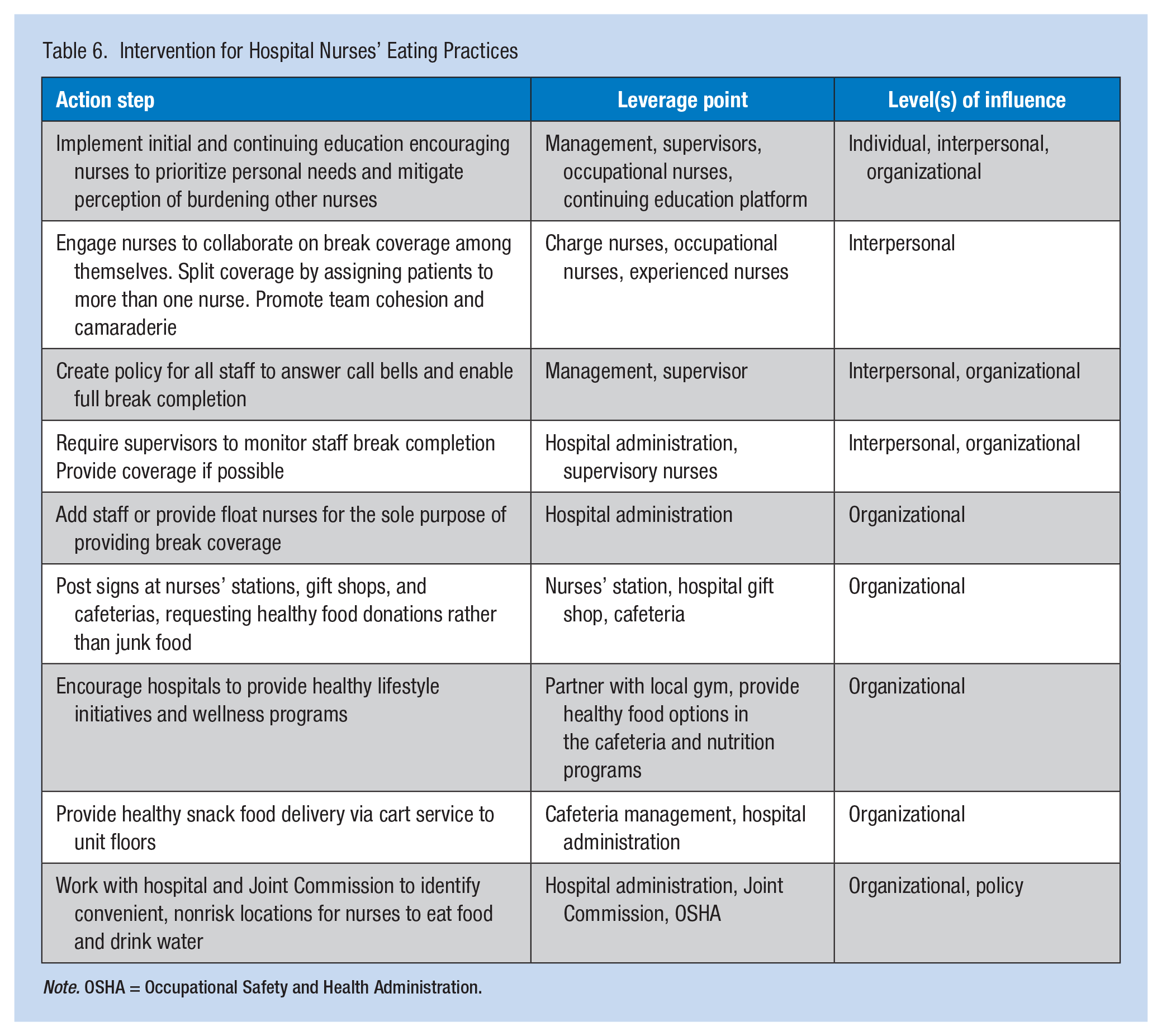
Note. OSHA = Occupational Safety and Health Administration.
Conclusion
As the largest health care profession in the United States, the nursing workforce is a relevant population, especially within the health care industry. Hospital nurses provide the essential service of assisting patients to prepare for critical procedures and recover from injury, disease, illness, and trauma. This study found that more support from hospital management through staffing, coverage, and education are needed so that nurses can eat a healthy diet while at work. Steps should be taken to address social norms, coverage policies, and supervisory involvement on hospital units to ensure that break opportunities are enjoyed. Efforts such as appropriate signage could be used to redirect patient food donations toward healthier offerings, thus improving the overall food environment for nurses. Policies and practices to support and promote nutritious dietary habits for hospital nurses are needed. Hospital health care providers should work in an environment that embodies the promotion of health for all, patients and employees alike.
Applying Research to Practice
Hospital nurses often face a challenge during their shift to address personal needs, specifically hunger and thirst due to patient load, unpredictability of patient needs, and reluctance to burden other nurses, among other perceived barriers. Hospitals and supervisors could provide various means of training and support:
Implement initial and continuing education encouraging nurses to prioritize personal needs
Enact policy that ensures sufficient break time
Engage nurses to collaborate on break coverage among themselves
Add staff or provide float nurses for the sole purpose of providing break coverage
Split coverage by assigning patients to more than one nurse
Create hospital wide programs to provide healthy lifestyle and wellness initiatives for employees.
Policies and practices to support and promote nutritious dietary habits for hospital nurses are needed. Hospital health care providers should work in an environment that embodies the promotion of health for all, patients and employees alike.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Tina Monaghan is a graduate of the Montclair State University College of Education and Human Services with a Master of Science degree in Nutrition and Food Studies. She does consulting work for wealth management professionals and fundraising for educational, healthcare, and performing arts organizations.
Lauren Dinour is an assistant professor of nutrition in the Department Nutrition and Food Studies at Montclair State University. Currently, her research interests focus on health-promoting policies and programs that improve nutrition, particularly in the areas of school food and breastfeeding. A registered dietitian (RD) and public health professional, she holds a DrPH with a focus on public health nutrition from the Graduate Center (City University of New York [CUNY]), an MPH with a focus on public health nutrition from Hunter College (CUNY), and a BS in nutritional sciences from Cornell University.
Doreen Liou is currently an associate professor at Montclair State University in the Department of Nutrition and Food Studies, where she teaches undergraduate and graduate courses in nutrition education and social marketing in nutrition. Her research interests include applications of social-psychological theories of dietary behaviors in prevention of chronic diseases.
Melanie Shefchik is a certified health education specialist (CHES) and an instructional specialist within the Department of Public Health at Montclair State University, where she teaches undergraduate courses focused on health education, human diseases, and population-based nutrition. Her professional interests and experience center around chronic disease prevention and management.