
Abstract
Background: Workplace breastfeeding resources (e.g., break times and private spaces) help working mothers exclusively breastfeed for 6 months. However, not every employer offers lactation resources as specified in the Affordable Care Act. This study examined working mothers’ access to workplace breastfeeding resources, their barriers and facilitators to combining breastfeeding and work, and their recommendations to improve access to breastfeeding resources. Methods: Working mothers between the ages of 18 to 50 years who had given birth in the previous 2 years were recruited online to participate in the study. An online, cross-sectional survey collected qualitative and quantitative data from working mothers on their access to workplace breastfeeding resources and experiences with breastfeeding at work. Descriptive statistics were used to report the quantitative results from the survey, and the qualitative data were examined using the constant comparative method. Findings: Fifty-two participants met the inclusion criteria for the study and completed the survey. Most of the participants in the study were White, college-educated women who worked in clerical or administration support and education occupations. Approximately 78.8% of the participants reported access to private spaces and 65.4% reported access to break times for breastfeeding. Fewer participants reported access to breast pumps, lactation consultants, and support groups. Conclusions/Application to Practice: There are gaps in access to workplace breastfeeding resources, but occupational health nurses can inform and help employers implement lactation resources to reduce breastfeeding disparities.
Introduction
Breastfeeding has been shown to offer numerous health benefits for infants and mothers. Infants who were breastfed have been found to have a lower risk of developing type 2 diabetes, asthma, and ear and respiratory infections (Centers for Disease Control and Prevention [CDC], 2018b). Breastfeeding mothers had a lower risk of developing breast cancer, ovarian cancer, and type 2 diabetes (CDC, 2018b). In 2012, the American Academy of Pediatrics (AAP) recommended that infants be exclusively breastfed for the first 6 months of life and continue to be breastfed for 1 year (Eidelman, & Schanler, 2012). In 2015, approximately 83.2% of infants in the United States were breastfed at birth, but the proportion of infants who were breastfed decreased with increasing age, with 46.9% exclusively breastfed at 3 months, and 24.9% at 6 months (CDC, 2017a).
Studies have found that women stopped breastfeeding for multiple reasons including challenges with breastfeeding after returning to work and lack of workplace breastfeeding resources (Bonet et al., 2013; Kozhimannil et al., 2016; Mandal et al., 2010; Ogbuanu et al., 2011). Women who returned to work earlier than anticipated and returned to full-time jobs were less likely to continue breastfeeding (Mandal et al., 2010; Mirkovic et al., 2014). In addition, women who breastfed less than 4 months after returning to work reported not having flexible time or a private space to express breast milk (Lauer et al., 2019).
In 2010, the Affordable Care Act (ACA) mandated that employers provide reasonable break time and a private space, other than a restroom, to express breast milk (“Patient Protection and Affordable Care Act,” 2010). Some employers are not required to comply with the law, which leaves their employees without access to workplace breastfeeding resources (Hawkins et al., 2015). For instance, employers with less than 50 employees can receive a “undue hardship” exemption from providing break times or a private space to express breast milk (“Patient Protection and Affordable Care Act,” 2010). In addition, the ACA provisions only apply to employees who are not exempt from the Section 7 requirements of the Fair Labor Standards Act (FLSA) in the ACA (“Patient Protection and Affordable Care Act,” 2010). Employees covered by the FLSA include those who work hourly and are subject to receive overtime pay (“Patient Protection and Affordable Care Act,” 2010). However, salaried workers and employees who are exempt from the FLSA overtime requirements are not covered under the ACA (“Patient Protection and Affordable Care Act,” 2010). These employees may be covered under state laws or workplace breastfeeding policies implemented by their employers (U.S. Department of Labor, 2018).
The workplace is an important setting for promoting health, and the recent Workplace Health in America Survey revealed that 46% of worksites offer programs to employees to improve their health (Linnan et al., 2019). Unfortunately, lactation support was only reported by 8% of worksites, and large gaps were reported between small and large worksites (59% of worksites with 500 or more employees offered lactation support programs compared with fewer than 5% of worksites with 10–24 employees) (Linnan et al., 2019). Kim et al. (2019) described various forms of lactation support at work that included but were not limited to maternity leave, workplace policies, education, flexible work schedules, lactation rooms, and adequate break times. Lactation programs at worksites have been shown to increase breastfeeding duration with a dose response such that breastfeeding duration increased with each additional worksite support for breastfeeding (Kim et al., 2019). Access to both a private space and break times at work has been associated with breastfeeding longer (Kozhimannil et al., 2016).
A recent systematic review concluded that workplace lactation programs increased duration and exclusive breastfeeding; however, these studies have been conducted in worksites with adequate resources to provide such programs (Kim et al., 2019). Data from the recent Workplace Health in America survey suggest that many worksites do not offer such programs (Linnan et al., 2019). Occupational health nurses play a critical role in the development and implementation of workplace lactation support programs and are a critical link between worksite benefits and employee health (Hilliard, 2017; Rietz & McCullagh, 2010). However, additional data are needed about who has access to lactation resources and how to overcome the barriers that women face in accessing resources at work to support their lactation goals.
The purposes of this study were to examine working mothers’ access to workplace breastfeeding resources, describe working mothers’ barriers and facilitators to breastfeeding at work, and describe their recommendations to improve access to workplace breastfeeding resources.
Methods
We conducted a mixed-methods study to examine working mothers’ access to workplace breastfeeding resources and their overall experience with combining breastfeeding and work. The University of Georgia Institutional Review Board approved the study protocol and deemed the study “exempt” (approval ID: STUDY00005924). The targeted population was working women between the ages of 18 and 50 years who had given birth in the past 2 years. The inclusion criteria for the study were mothers that had given birth within the previous 2 years, had at least one main job outside of Amazon Mechanical Turk (MTurk), and were between the ages of 18 and 50 years.
Study Population and Recruitment
Participants were recruited on MTurk, a crowdsourcing labor market that connects workers with tasks (i.e., surveys and transcription) (MTurk, n.d.). MTurk workers are required to be over 18 years of age. Additional qualifications were selected that required potential participants to have at least one main job outside of MTurk and be between the ages of 18 and 50 years. Only MTurk workers who met these qualifications had access to the posted survey. The survey was posted as a task in MTurk in April 2018. Participants voluntarily accepted the task and were further screened for eligibility by responding to the question “Have you given birth in the past 2 years?” Participants who answered “yes” proceeded to a consent letter. After reading the consent letter, participants consented to participation in the study by clicking the “Next” button on the page. Participants who completed the survey received an incentive of US$1.90. The survey was cross-sectional and administered using Qualtrics electronic survey platform. A total of 181 respondents completed the screener question. Fifty-two participants met the eligibility requirement and completed the survey.
Survey Instrument
The survey included questions on demographics, breastfeeding behaviors, employment characteristics, and access to workplace breastfeeding resources.
Participants reported their age in years. The participants reported their race/ethnicity by selecting from one or more of the following categories: “Black or African American,” “White or Caucasian,” “Hispanic or Latino,” “Asian,” “American Indian or Alaska Native,” and/or “Native Hawaiian or Pacific Islander.” Education level was measured using the following categories: “some high school,” “high school graduate or GED,” “some college or technical or vocational training,” “associate degree,” “bachelor’s degree,” “postgraduate work,” and “postgraduate degree.” The education levels were collapsed into the following categories for analyses: “high school diploma or GED,” “associate degree,” “bachelor’s degree,” and “postgraduate degree.” Individual income level was measured using the following categories: “US$0 to US$20,000,” “US$20,001 to US$40,000,” “US$40,001 to US$60,000,” “US$60,001 to US$80,000,” and “US$80,001 or more.” Marriage status was measured by asking participants if they were single or married/living with a partner.
Breastfeeding Behavior
To measure breastfeeding exclusion, participants were asked to report how old their baby was when they introduced formula or any other food besides breast milk (responses ranging from “less than 1 month,” “1 to 2 months,” “3 to 4 months,” “5 to 6 months,” “7 to 9 months,” and “more than 9 months”). This question was modified from the Prenatal Questionnaire used in the Infant Feeding Practices Study II (CDC, 2017b).
Employment Characteristics
Participants were asked to select the job category that best described their main job outside of MTurk. Job categories included “executive, administrator, or senior manager”; “professional”; “technical support”; “sales”; “clerical and administrative support”; “service occupation”; “precision production and crafts worker”; “operator or laborer”; and “educator.” Participants were also asked to self-report their job titles. Participants were asked if they had flexible work arrangements (“yes” or “no”). If participants selected “yes,” they were asked to select one of more types of flexible work arrangements they had: “flextime,” “telecommuting,” “compressed work schedules,” and/or “job-sharing assignments.” The types of flexible work arrangements were definitions used in a guideline from the University of Kentucky (Flexible Work Arrangements Work Group, n.d.).
Access to Workplace Breastfeeding Resources
Participants were asked if they had the following workplace breastfeeding resources: breaks for expressing breast milk, breast pumps, breast pump accessories, spaces other than a restroom for expressing breast milk, lactation consultants, educational materials, support groups, worksite-based programs that promote expressing breast milk in the workplace, and written policies on expressing breast milk at work (National Business Group on Health, 2009). The response options for each resource are described below.
Participants were asked if they had breaks in their workday that allowed them to breastfeed/pump breast milk (responses ranging from “always,” “often,” “sometimes,” “rarely,” and “never”). Participants that selected responses “always,” “often,” or “sometimes” were counted as having breaks for expressing breast milk. Participants were asked if their employer provided breast pumps, breast pump accessories, spaces other than a restroom for expressing breast milk, lactation consultants, educational materials, support groups, or worksite-based programs by selecting “yes” or “no” to each item in the survey. Finally, participants were asked if their employer had a written policy on breastfeeding at work (responses ranging from “yes,” “no,” and “I don’t know”).
Open-Ended Questions
Participants were asked to provide qualitative data on their breastfeeding experiences at work by describing the workplace breastfeeding resources they found most helpful and the challenges they experienced when trying to express breast milk at work. Participants were also asked to provide recommendations to improve workplace breastfeeding support.
Data Analysis
Data were analyzed using IBM SPSS statistical software version 24 (IBM Corporation, 2016). Descriptive statistics were used to summarize the data from the survey. Responses to open-ended questions were reviewed, and themes were identified using the constant comparative method (Glaser, 1965).
Results
Participant Characteristics
A total of 52 respondents completed the survey. The mean age of the participants was 30.88 years (SD = 5.12) with a range from 21 to 42 years. The majority of the participants were married (78.8%), White (78.8%), and college-educated (90.4%). Nearly one fourth (21.2%) of participants reported they were single (Table 1). Approximately 32.7% of participants worked in clerical and administrative support occupations followed by education (17.3%). An estimated 71.2% of participants reported access to flexible work arrangements, with participants frequently reporting flextime (41.8%) and telecommuting (23.6%) as one or more of their arrangements.
Participants’ Demographic Information, Employment Characteristics, and Workplace Resources for Breastfeeding
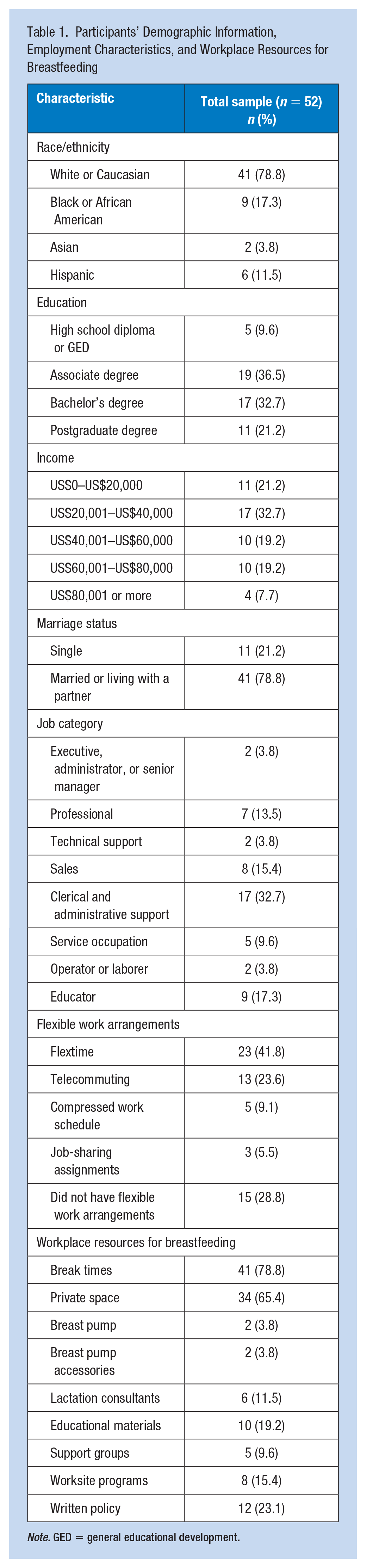
Note. GED = general educational development.
Breastfeeding Behavior and Workplace Resources
One fourth of participants (25.0%) introduced formula or other foods within the infant’s first month. Approximately 11.5% of participants introduced formula within the infants’ first and second month; 17.3% within the third and fourth month; 30.8% within the fifth and sixth month; and 13.5% within the seventh and ninth month.
Approximately 78.8% of participants reported access to break times for expressing breast milk, and 65.4% had access to spaces other than a restroom to express breast milk (Table 1). The least reported workplace resources were access to breast pumps (3.8%), breast pump accessories (3.8%), support groups (9.6%), and lactation consultants (11.5%). Only 23.1% of respondents reported that their employer had a written policy on expressing breast milk at work, whereas 40.4% did not and 36.5% did not know.
Barriers to Expressing Breast Milk at Work
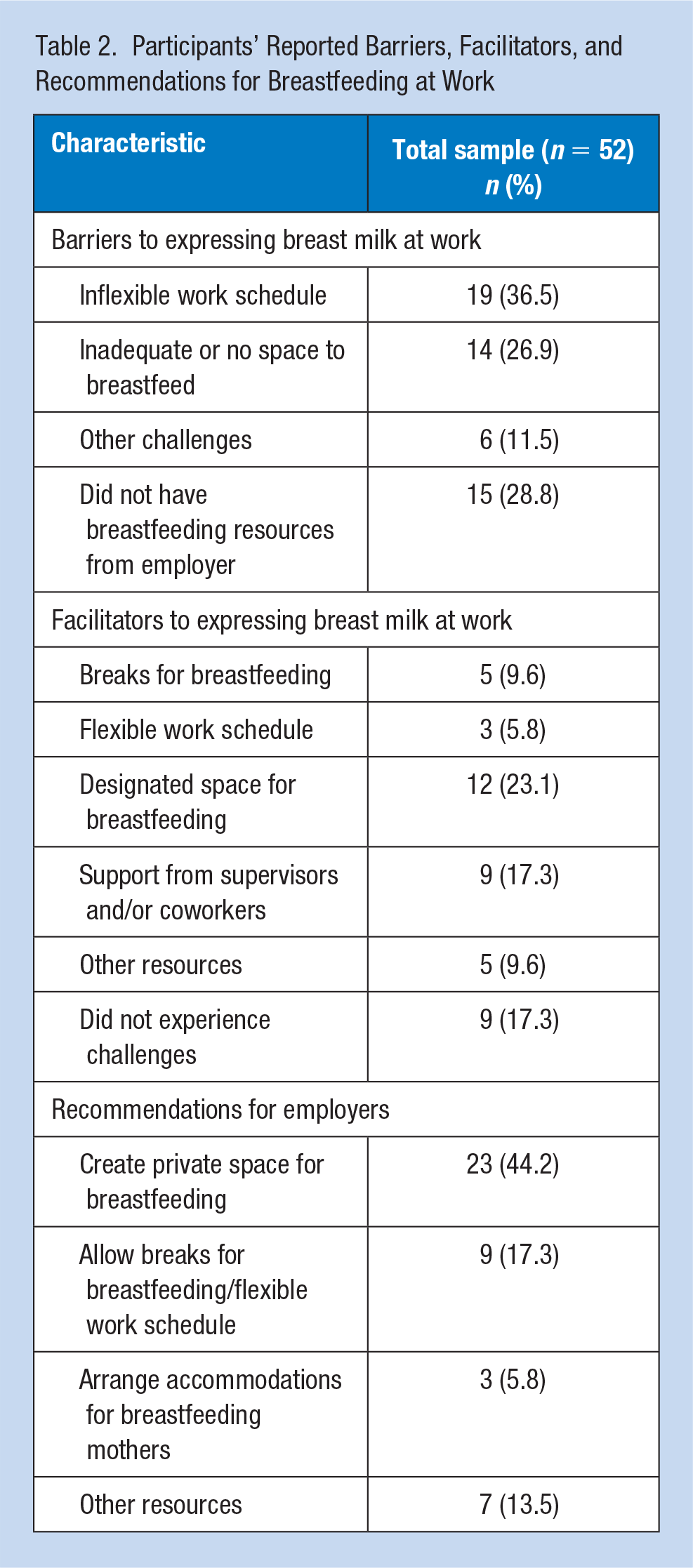
Nineteen participants (36.5%) reported that their work schedule was too demanding to take breaks for breastfeeding while fifteen (28.8%) did not have access to any workplace breastfeeding resources (Table 2). Fourteen participants (26.9%) reported that they did not have access to a designated space or that the designated space was dirty. Six participants (11.5%) reported other challenges such as difficulty finding breastfeeding information at the workplace, difficulty making arrangements at the workplace for breastfeeding, and difficulty feeling comfortable to express breast milk while at work. Workers expanded on these issues.
Participants’ Reported Barriers, Facilitators, and Recommendations for Breastfeeding at Work
A registered nurse (who exclusively breastfed for less than 1 month) indicated, I have a super busy schedule and would not be able to complete my work if I took the time to pump as I should have to sustain my milk supply. Another issue was that I work on the road a lot, and pumping in the car is awkward and draws unwanted attention.
An engineer, who exclusively breastfed for 7 to 9 months, indicated, “We don’t have a designated room so sometimes it took a while to find a room I could lock and pump in,” as well as an office manager (who exclusively breastfed for 5–6 months) indicated, “I am the only worker who is pumping at work so it took some arranging to get a private room.”
A worker in fiduciary services (who exclusively breastfed for 1–2 months) indicated, [There was] no direct contact/information on who to contact to get more information on the pumping rooms at my work. I had to ask someone who was currently pumping in order to find out who I needed to talk to. It wasn’t readily available.
Facilitators to Expressing Breast Milk at Work
Nine (17.3%) participants reported that they did not experience any challenges or barriers while five (9.6%) had designated breaks, twelve (23.1%) had access to a space, other than a restroom, and nine (17.3%) reported that their supervisor and/or coworkers were supportive in helping participants combine breastfeeding and work (Table 2). Five (9.6%) participants reported access to additional lactation resources including breast pumps, breast pump accessories, and on-site lactation consultants. Some of the participants indicated the following: “There were not many challenges I faced. My company is extremely encouraging and supportive to new mothers” (Quality assurance, who exclusively breastfed for 5–6 months); “I have been able to change my schedule slightly for specific feeding times or pumping times” (Surgical technician, who exclusively breastfed for 1–2 months); “The designated space to breastfeed at my job is a comfortable, clean, and inviting room” (Quality assurance, who exclusively breastfed for 5–6 months); and “My coworkers and supervisor help me with breastfeeding questions [I have] because they have breastfed” (Food server, who exclusively breastfed for 5–6 months).
Participants’ Recommendations for Employers
Twenty-three (44.2%) participants reported that they wanted access to a private space for breastfeeding or for their employer to update the current space for breastfeeding (Table 2), whereas nine participants (17.3%) indicated that they wanted more breaks and a flexible work schedule to arrange breaks for breastfeeding. Three (5.8%) participants suggested that their employers should play a more active role in arranging accommodations for breastfeeding while seven (13.5%) offered other recommendations such as access to lactation consultants, support groups, and educational materials. Participant quotes that capture recommendations are included below.
“Every company should have a private room for breastfeeding and there should be a policy in place that gives all pumping women enough breaks to maintain supply” (Teacher, who exclusively breastfed for less than 1 month). A mother who worked as a tutor and exclusively breastfed for 5 to 6 months indicated, I don’t expect a lot from my company since women can choose to formula feed rather than breastfeed. It would be nice for managers to try to be flexible with the schedules of women who are pumping so that they can pump at more convenient times or have more time in which to accomplish the pumping.
In addition, a mother who worked as a baker, and exclusively breastfed for 7 to 9 months, indicated, They don’t make their willingness to work with nursing mothers well known. I had to go out of my way to tell them what I needed and ask how to get it. They were accommodating, but they don’t offer up the information.
Discussion
Using quantitative and qualitative data, this study examined access to breastfeeding resources, facilitators and barriers to breastfeeding at work, and recommendations to support breastfeeding at work from mothers who recently gave birth. Despite the federal protections in the ACA, data collected in this study suggested that gaps exist in access to lactation support in workplaces in the United States.
Dagher et al. (2016) conducted a prospective cohort study among working mothers in the United States and found that women who initially breastfed their infant were more likely to be White, college-educated, and married compared with women who did not initially breastfeed their infant. Although our study population is similar in demographics and findings, our sample size and sampling methods are not generalizable with respect to making inferences across these groups.
Consistent with the provisions in the ACA, private spaces and break times for expressing breast milk were the most commonly reported breastfeeding resources. A small proportion of participants in this study did not have access to any breastfeeding resources at work. One explanation for this finding is that these participants’ employers may have been exempt from the ACA provisions. Employers with fewer than 50 employees can be exempt from the ACA due to financial hardship or difficulty in supplying breastfeeding resources (“Patient Protection and Affordable Care Act,” 2010). Alternatively, these employers may not see lactation support as a necessary benefit to employees. Bai et al. (2012) conducted telephone interviews with a sample of human resource (HR) managers and found HR managers reported concerns with providing breastfeeding accommodations. The HR managers indicated that providing these resources would be time-consuming, not cost-effective, and create challenges with scheduling and covering for employees who are breastfeeding (Bai et al., 2012).
In this study, working mothers’ experiences with expressing breast milk at work depended on their job characteristics. Some barriers were specific to job duties such as traveling for work while others represented challenges most working mothers may face such as no access to a private space for breastfeeding, while common facilitators were access to breaks for breastfeeding, private spaces to breastfeed, and social support from coworkers or supervisors. Previous studies have shown that the number of workplace resources working mothers received was positively associated with exclusively breastfeeding for the first 6 months (Balkam et al., 2011; Kim et al., 2019). To meet the 6-month recommendation, employers can provide additional resources (i.e., lactation consultants and support groups) to help mothers transition back to work and continue breastfeeding.
The ACA was an important first step for establishing minimum resources to support breastfeeding mothers; however, it needs to be expanded to cover all employers and workers. Currently, there is no system in place to hold employers accountable to the ACA. This lack of accountability raises concerns that every working mother in the United States has differential access to lactation support. Unequal access to support creates breastfeeding disparities that some mothers and infants are not able to gain the health benefits from breastfeeding. For instance, Dagher et al. (2016) found that women in professional jobs (i.e., accountant and professor) were more likely to initiate breastfeeding than women in clerical jobs. One reason for this might be that women in professional jobs often have more flexibility in their work schedules (Murtagh & Moulton, 2011).
Future studies should conduct environmental assessments of worksites to measure which lactation resources are available. Some of the participants in this study reported that they did not know if their employer had a breastfeeding policy and may not have known about all the resources available through their employer. Future studies examining how lactation resources and policies are communicated in the workplace would be informative. Dabritz et al. (2009) found that working mothers were reluctant to discuss breastfeeding accommodations with their employer and lacked knowledge about their workplace’s breastfeeding policy. Working mothers may feel they are solely responsible for finding and securing lactation resources. Occupational health nurses can step in to alleviate the burden placed on employees by communicating to worksite leadership the importance of these accommodations and provide strategies into the best practices of adopting these resources. In addition, occupational health nurses can serve as a conduit between worksite policies and benefits to employees.
Several limitations may have influenced the findings from this study. First, the sample size was small and may not be generalizable to all working mothers in the United States because participants were only recruited through MTurk and the inclusion criteria were restrictive. Second, we were not able to determine the participants’ location in the United States because the survey did not ask for the participants’ specific state or city of residence. Third, the data were self-reported and could be subject to response and recall bias. Finally, the survey did not measure participants’ self-efficacy or internal motivation to continue breastfeeding upon their return to work, which could be important factors in breastfeeding outcomes.
Despite these limitations, the study has several strengths. The sample size is small, but it is comprised of working women that share the experience of combining breastfeeding and work. In addition, the study collected qualitative data to provide contextual information to the quantitative data collected. This study is one of the few studies to include and measure access to breastfeeding support such as breast pumps, worksite programs, educational materials, support groups, lactation consultants, and workplace policies. Finally, this study explored the impact of the ACA from the perspectives of working mothers in the United States and identifies the gaps in the ACA provisions where employers can address breastfeeding disparities.
Implications for Occupational Health Nurses
Occupational health nurses play a pivotal role in promoting breastfeeding in the workplace and advocating for lactation resources. Women can go to an occupational health nurse to seek lactation resources if they do not feel comfortable going to their supervisor. Occupational health nurses can work with breastfeeding mothers to increase their confidence to continue breastfeeding and fill communication gaps to link working mothers to lactation resources in the workplace. Occupational health nurses can communicate the benefits of breastfeeding to the employer and provide guidance on how to implement workplace breastfeeding resources. The National Business Group on Health and the CDC have toolkits available online to help occupational health nurses familiarize themselves with the benefits of lactation resources and best practices into implementing these resources within their worksites (CDC, 2018a; National Business Group on Health, 2009).
Applying Research to Occupational Health Practice
This study examined working mothers’ access to workplace breastfeeding resources, and their barriers and facilitators to expressing breast milk at work using an online, cross-sectional survey. Most working mothers in the study reported access to break times and private spaces for breastfeeding, but fewer mothers reported access to breast pumps, support groups and lactation consultants. The most common barriers to expressing breast milk at work were inflexible work schedules and lack of breastfeeding resources. The most common facilitators to breastfeeding were access to a private space and support from coworkers and/or supervisors. Occupational health nurses should advocate for employees’ health and well-being. Workplace breastfeeding resources play an important role in helping mothers continue breastfeeding and maintain work–life balance. The findings from this study demonstrate the need for occupational health nurses to work with employers to implement workplace breastfeeding resources and policies to support working mothers and their families.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Rachel E. McCardel is working to obtain her MPH and PhD in Health Promotion and Behavior in the Department of Health Promotion and Behavior at the University of Georgia.
Heather M. Padilla is an assistant professor in the Department of Health Promotion and Behavior at the University of Georgia.